
Abstract
Objective:
Existing evidence on factors associated with community treatment order placement is largely restricted to administrative data. We utilised the data from a large nationally representative sample to compare the demographic, clinical, social functioning, substance use and service utilisation profiles of people living with psychosis under community treatment orders with those who were not.
Methods:
Participants were grouped based on whether they had been subject to a community treatment order in the past 12 months or not. We conducted logistic regressions to examine demographic, clinical, social functioning, substance use and service utilisation profiles associated with the two groups.
Results:
People who had recently been subject to community treatment orders were more likely to be treated with long-acting injectable antipsychotics and lacked insight but were less likely to report suicidal ideation. They also had higher psychiatric inpatient admission rates but a lower frequency of general practitioner visits.
Conclusion:
People on community treatment orders in Australia may differ from those who are not under a community treatment order in their treatment needs. Resources and care provision must match the needs of this particularly vulnerable group.
Introduction
Community treatment orders (CTOs) authorise the involuntary mental health treatment of a person living in the community. The rates of CTO use in Australia are high compared to other parts of the world but show a wide variation by jurisdiction (Light, 2019; Light et al., 2012; O’Donoghue et al., 2016; Rugkasa, 2016). For instance, the proportion of people in contact with state-run mental health services on CTOs ranges from 3.1% in Western Australia to 22.3% in Queensland (Kisely et al., 2020a, 2020b). A recent systematic review of CTO use across Australian and New Zealand found that CTO placement was associated with being male, single, a lack of vocational engagement, migrant background, primary diagnosis of non-affective psychosis, comorbid substance use and past contact with the criminal justice system (Kisely et al., 2020b). CTO placement was also associated with reduced mortality and increased community mental health service contacts, but there was no clear association with hospital admission or readmission rates (Kisely et al., 2020b).
The current understanding of CTO use across Australia relies on state-based administrative datasets (Kisely et al., 2020b). This approach limits the ability to generalise findings across jurisdictions and restricts the range of variables available for analysis. For example, while several studies have examined ‘hard’ outcomes such as admission rates (Harris et al., 2019; Kisely et al., 2020a; Segal et al., 2017; Vine et al., 2016), there has been limited exploration of factors such as symptom profiles and psychosocial functioning in people placed on CTOs.
The 2010 Survey of High Impact Psychosis (SHIP) (Morgan et al., 2012) provides a unique opportunity to explore characteristics of people under CTOs with psychotic disorders in Australia. Unlike state-based administrative datasets, the SHIP dataset provides detailed clinical and psychosocial information on over 1800 individuals living with psychosis in multiple jurisdictions in Australia at one given time. Using the data from the SHIP, we investigated the similarities and differences in the demographic features, clinical symptoms, social functioning, substance use and service use patterns of people under CTOs compared to those who were not.
Methods
SHIP data
SHIP was the second national survey of people living with psychosis in Australia. Data collection took place between April 2010 and April 2011, with the survey covering five Australian states and a population of approximately 1.5 million adults (18–64 years, around 10% of the population in this age range). A two-phase design was employed. In Phase 1, screening for people likely to fulfil formal criteria for psychotic disorder occurred in public inpatient and community mental health services, as well as non-government organisations supporting people with mental illness in the census month (March 2010) (Morgan et al., 2012). Additionally, people with a recorded diagnosis of psychosis in contact with public specialised mental health services in the 11 months prior to, but not in, the census month were identified through administrative records. A total of 7955 people screened positive for psychosis. In Phase 2, 1825 of the total sample that screened positive were randomly selected, stratified by catchment site and age group (18–34 years and 35–64 years) and interviewed. The interview was administered by trained mental health professionals and covered a broad range of areas including demographic characteristics, social functioning, physical health and activity, medication use, service utilisation and psychopathology. For the current study, all participants with a diagnosis of either an affective or non-affective psychosis who responded to the question regarding their CTO status were included (N = 1612). The research protocol for the SHIP study was approved by all relevant institutional ethics committees at each catchment site and all participants gave written informed consent.
CTO status
The use of CTOs in the previous 12 months was assessed using the question: ‘In the last 12 months when you were not in hospital, have you been under a legal obligation to obtain treatment, for example through a community treatment order?’ (response categories: [1] current, [2] not current but in last 12 months, [3] no). For the current study, the responses were dichotomised into either yes (combined responses [1] and [2]) or no (response [3]).
Demographic characteristics
Demographic data collected from participants included age, sex, marital status (categorised as (1) separated, divorced or widowed; (2) single, never married, or (3) partnered [married or de facto]), Aboriginal or Torres Strait Islander heritage, country of birth (dichotomised into either born in Australia or not born in Australia) and language spoken at home (dichotomised into either English or non-English). Post-school qualifications, any employment in the 12 months before the interview and any period of homelessness (primary, secondary and tertiary) over the past 12 months were coded yes or no. Self-reported criminal activity over the past 12 months such as break and enter, shoplifting, dealing drugs, forging cheques, armed robbery or assault was also coded yes or no.
Clinical characteristics
The Diagnostic Interview for Psychoses (DIP) (Castle et al., 2006), a semi-structured clinical interview for classifying psychotic illness according to various criteria, including International Classification of Diseases, 10th Revision (ICD-10), was administered. It uses prompts adapted from the Schedules for Clinical Assessment in Neuropsychiatry (SCAN) (World Health Organization, Division of Mental Health, 1994) to elicit signs and symptoms and then applies the Operational Criteria Checklist for Psychosis (OPCRIT) (McGuffin et al., 1991) algorithm embedded into a software package to generate diagnoses according to several classification systems. For the current study, ICD-10 diagnoses were divided into either non-affective psychosis (including schizophrenia, delusional disorder and other non-organic psychosis) or affective psychosis (including schizoaffective disorder, bipolar disorder with psychotic features and depression with psychosis). Individual DIP items examined included age of illness onset determined by the interviewer and based on responses to prompts such as: ‘When did you first experience mental health problems?’, ‘When were you first admitted to hospital with a mental health problem?’ and ‘When did others first say that they thought you had a psychiatric problem?’; duration of illness, which was derived from the age of onset; and course of illness, which captures the number of lifetime episodes of mental illness experienced and the degree of recovery between episodes. Course of illness was dichotomised into non-chronic (single episode with good recovery or multiple episodes with good or partial recover between) or chronic (continuous chronic illness with or without deterioration). We examined binary ratings (present or not present) for lifetime suicidal thoughts according to the DIP and past-year negative symptoms using items of the Carpenter deficits syndrome, rated but without including aetiological attribution (Kirkpatrick et al., 1989). As rated in the DIP, Insight was determined to be absent if the participant was unable to recognise that their experiences were abnormal, denied being currently or ever mentally unwell, or recognised that his or her experiences are abnormal but gave a delusional explanation. Medication use in the previous 4 weeks was based on participants being asked to bring their medication or medication list to the interview or a review of medication charts (Waterreus et al., 2012).
Social functioning measures
Loneliness was categorised based on participants’ response to the question: ‘In the last 12 months have you felt lonely?’ as follows: (1) I have felt socially isolated and lonely (categorised as ‘Severe’), (2) I have some friends but have been lonely for company (categorised as ‘Moderate’), (3) Although I have friends, I have been lonely occasionally (categorised as ‘Mild’) or (4) I have plenty of friends and have not been lonely (categorised as ‘None’). Life satisfaction was based on a response to the question: ‘During the last 12 months how have you been feeling about your life as a whole taking into account what has happened in the last 12 months and what you expect to happen in the future?’. The responses were categorised into: (1) mostly satisfied or better, (2) mixed or (3) mostly dissatisfied or worse. The Personal and Social Performance (PSP) Scale was used to estimate the personal and social functioning over the last 12 months. The interviewer makes a rating based on the degree of disability in four domains of socially useful activities, personal and social relationships, self-care and disturbing and aggressive behaviours (Morosini et al., 2000).
Substance use characteristics
Participants were asked to self-report lifetime use of alcohol, cannabis and amphetamines. The responses were dichotomised into either any or no use. The Fagerström test for nicotine dependence was used to categorise current smoking into either very low/low or moderate/high/very high (Heatherton et al., 1991).
Service utilisation patterns
Use of health services including hospital admission for mental and physical health reasons, any emergency department presentation and mental health outpatient attendance were determined by self-report. The utilisation of general practice (GP) services was based on response to the question: ‘In the last 12 months, have you seen a GP for any reason? If yes, in the last 12 months how many times in total have you seen a GP?’ For the current study, the responses were categorised into the following groups: (1) Frequent (12 or more visits), (2) Low (1–11 visits) or (3) Nil.
Data analysis
A series of logistic regressions were conducted to examine demographic, clinical, social functioning, substance use and service utilisation profiles associated with the CTO and non-CTO groups. Two models were considered. In Model 1, we calculated the odds ratios (ORs) with 95% confidence intervals (CIs) adjusted for age, sex and duration of illness to estimate the likelihood of participants being in the CTO group. In Model 2, we conducted multivariate analyses, calculating ORs with 95% CIs adjusted for additional variables that demonstrated statistically significant association with CTO in Model 1. For Model 2, the Holm method was used to reduce the risk of multiplicity (Holm, 1979). All analyses were done in R (version 4.0.4) (R Core Team, 2020) using packages tidyr (Wickham and Henry, 2020) and dplyr (Wickham et al., 2020).
Results
Of the 1612 participants included in the study, 342 (21.2%) had been under a CTO in the 12 months before the interview. Of those on a CTO, 133 people (38.9%) had previously been under CTOs but were not currently, and 209 people (61.1%) were currently under CTOs. The two groups did not differ in terms of age, sex and duration of illness. The comparison between the two groups is presented in Supplementary Table 1.
Demographic characteristics
Demographic characteristics of people under CTOs compared to people not under a CTO are presented in Table 1. Participants under CTOs were younger (t = 3.06, df = 571.43, p < 0.01) and more likely to be male (OR = 1.51, 95% CI: [1.17, 1.96]) and to be single/never married compared to being partnered (OR = 1.60, 95% CI: [1.11, 2.37]). They were also more likely to have been homeless (OR = 1.95, 95% CI: [1.41, 2.69]), and to have engaged in criminal activities in the past 12 months (OR = 1.53, 95% CI: [1.06, 2.18]), as well as being less likely to be in paid employment for the past 12 months (OR = 0.72, 95% CI: [0.55, 0.94]). There were no differences between the two groups in the following variables: country of birth, Aboriginal or Torres Strait Islander descent, language spoken at home and post-school qualification.
Demographic characteristics of people under CTO in the past 12 months compared to people not on CTO.
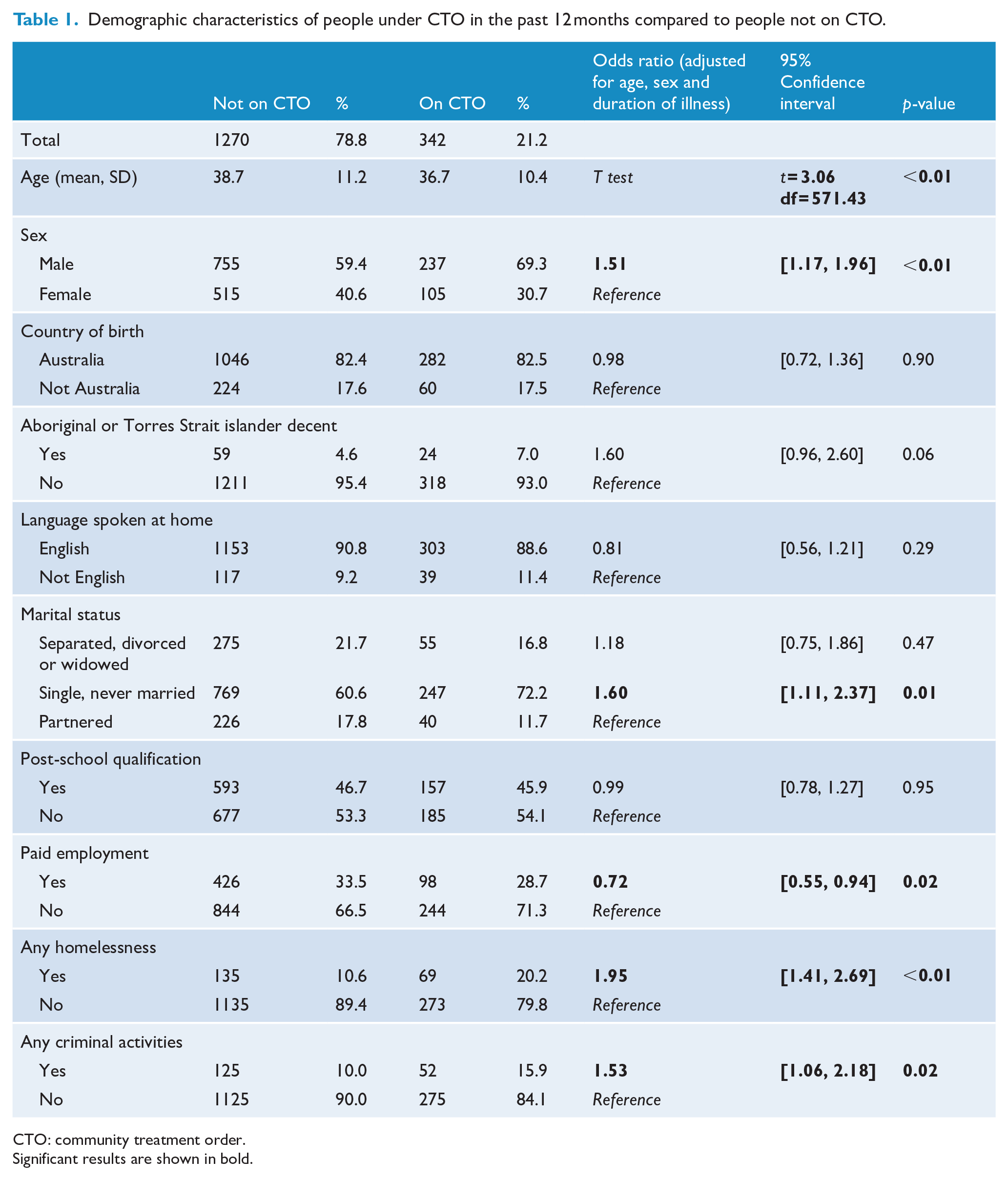
CTO: community treatment order.
Significant results are shown in bold.
Clinical characteristics
The clinical characteristics of people under CTOs compared to people not under a CTO are summarised in Table 2. Compared to the non-CTO group, the CTO group were more likely to have a longer duration of illness (t = 3.00, df = 591.44, p < 0.01), a non-affective psychosis diagnosis rather than an affective psychosis diagnosis (OR = 1.55, 95% CI: [1.20, 2.02]) and a more chronic course of illness (OR = 1.61, 95% CI: [1.25, 2.08]). Participants under CTOs were also more likely to be on any antipsychotic medication (OR = 3.67, 95% CI: [2.26, 6.35]), including long-acting injectable (OR = 4.70, 95% CI: [3.63, 6.10]), as well as lacking insight into their illness (OR = 2.70, 95% CI: [2.08, 3.49]). At the same time, participants under CTOs were less likely to have experienced lifetime suicidal thoughts (OR = 0.55, 95% CI: [0.44, 0.71]). There were no differences between the two groups in the following variables: age of onset and presence of any negative symptoms.
Clinical characteristics of people on CTO in the past 12 months compared to people not on CTO.
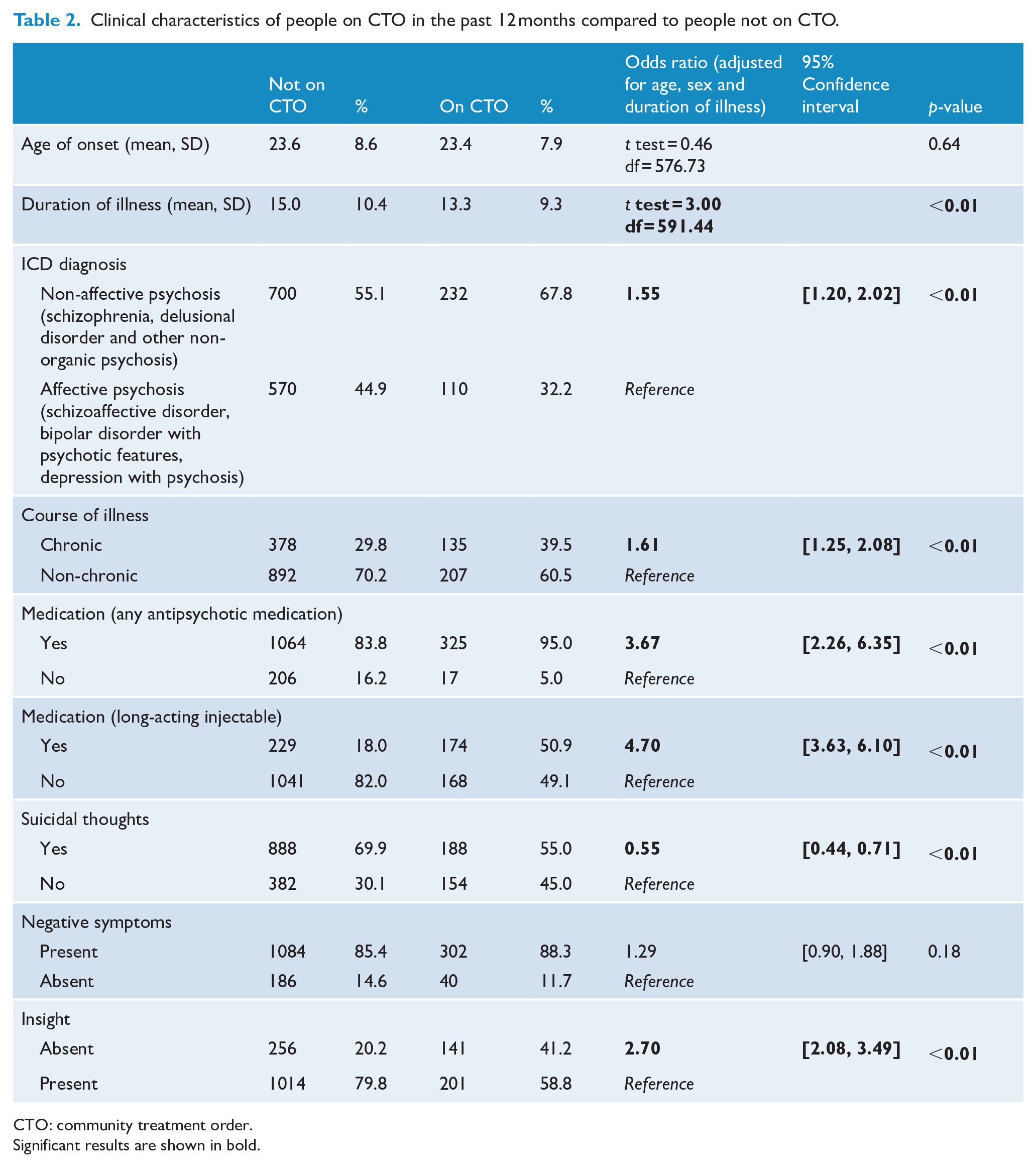
CTO: community treatment order.
Significant results are shown in bold.
Social functioning
Social functioning measures of people under CTOs compared to people not under a CTO are shown in Table 3. Compared to the non-CTO group, the CTO group were more likely to show poorer functioning on the PSP scale (i.e. less likely to be in the ‘absence of disability or only mild difficulties’ group; OR = 0.25, 95% CI: [0.14, 0.45] or in ‘Varying degrees of disability’; OR = 0.52, 95% CI: [0.32, 0.86]). There were no differences in loneliness or satisfaction with life between the two groups.
Social functioning measures of people on CTO in the past 12 months compared to people not on CTO.
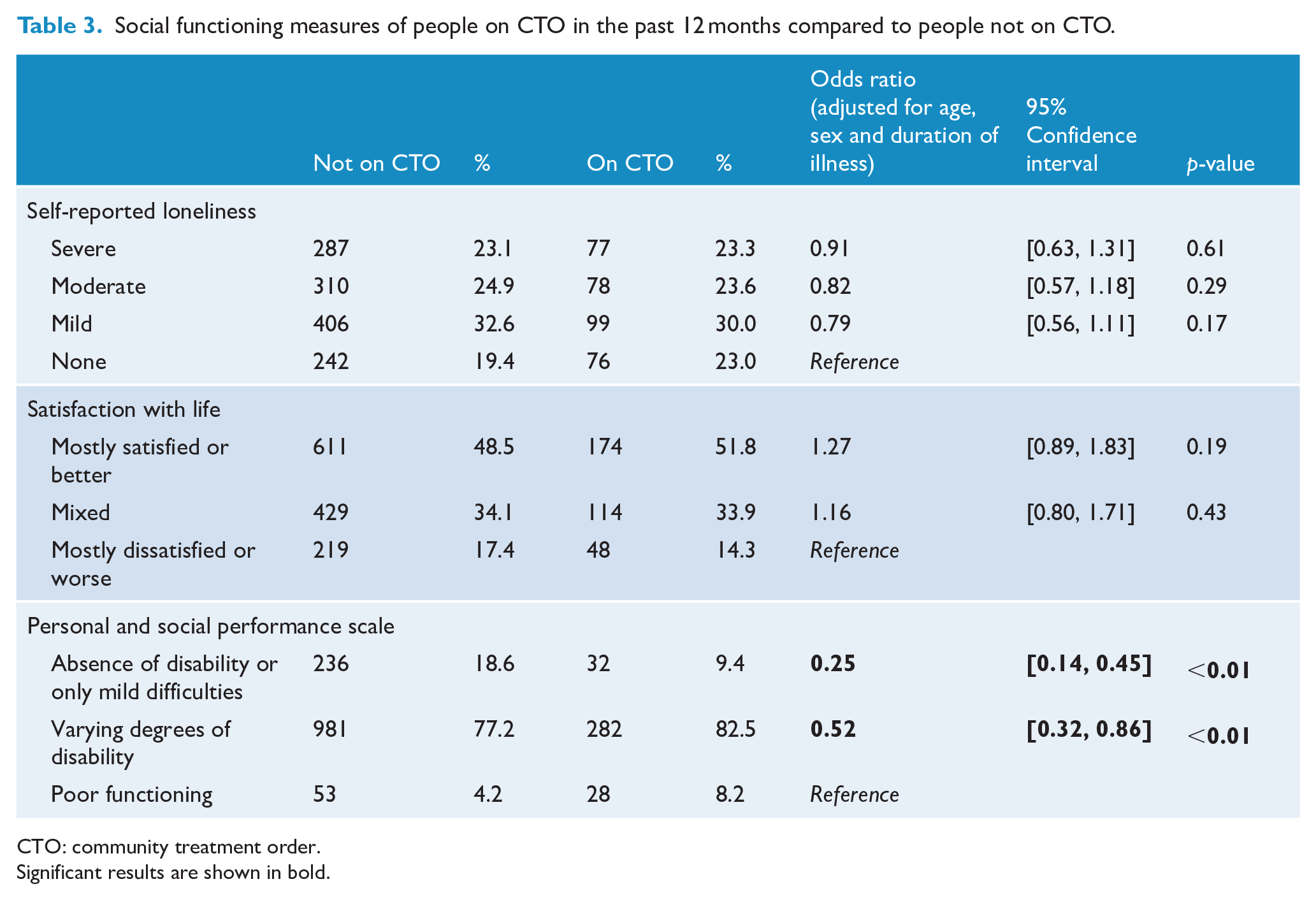
CTO: community treatment order.
Significant results are shown in bold.
Substance use characteristics
Substance use characteristics of people under CTOs compared to people not under a CTO are shown in Table 4. Compared to the non-CTO group, the CTO group were more likely to have moderate/high/very high nicotine dependence (OR = 1.53, 95% CI: [1.20, 1.96]) compared to very low/low dependence. There were no differences between the two groups in the following lifetime variables: alcohol use, cannabis use and amphetamine use.
Substance use characteristics of people on CTO in the past 12 months compared to people not on CTO.
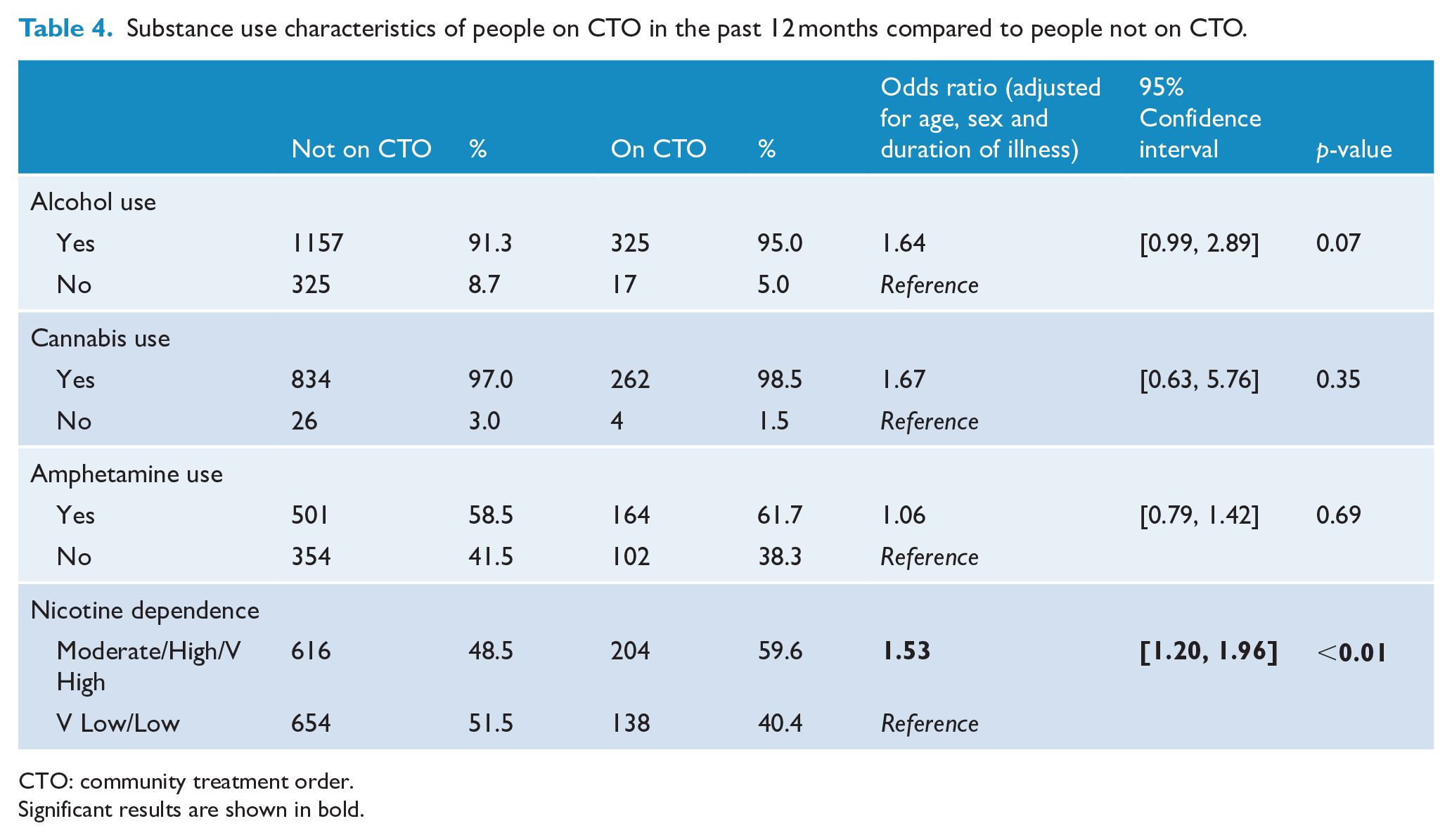
CTO: community treatment order.
Significant results are shown in bold.
Service utilisation patterns
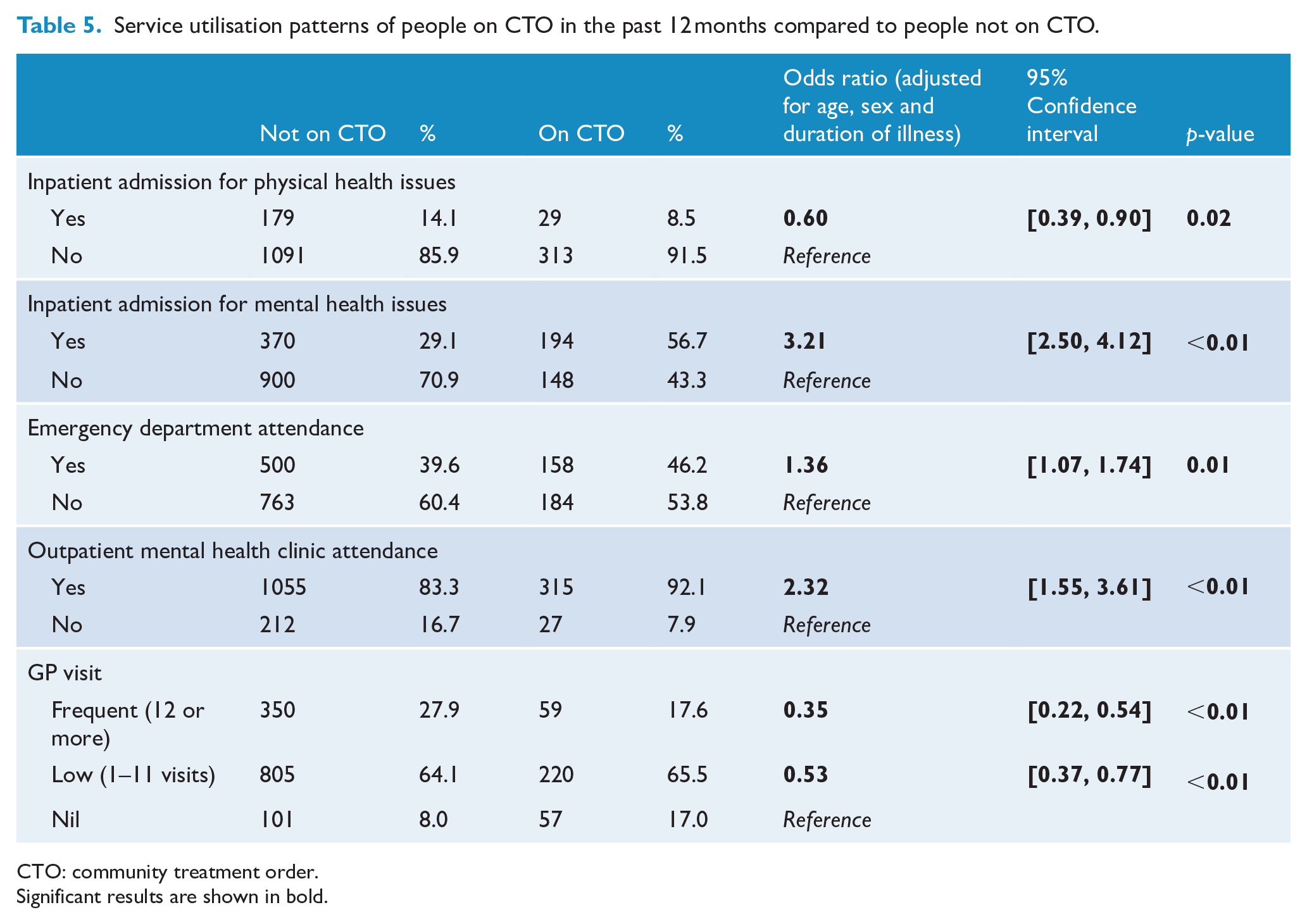
Service utilisation patterns of people under CTOs compared to people not under a CTO are presented in Table 5. Compared to the non-CTO group, the CTO group were more likely to utilise emergency departments in the past 12 months (OR = 1.36, 95% CI: [1.07, 1.74]) and were also more likely to have a hospital admission for mental health issues (OR = 3.21, 95% CI: [2.50, 4.12]) but less likely to be admitted for physical health issues (OR = 0.60, 95% CI: [0.39, 0.90]). Similarly, people under CTOs were more likely to have attended a mental health clinic (OR = 2.32, 95% CI: [1.55, 3.61]) but not a GP in the past 12 months (GP visit – frequent, OR = 0.35, 95% CI: [0.22, 0.54], and GP visit – low, OR = 0.53, 95% CI: [0.37, 0.77], both compared to nil GP visit).
Service utilisation patterns of people on CTO in the past 12 months compared to people not on CTO.
CTO: community treatment order.
Significant results are shown in bold.
Multivariate analyses
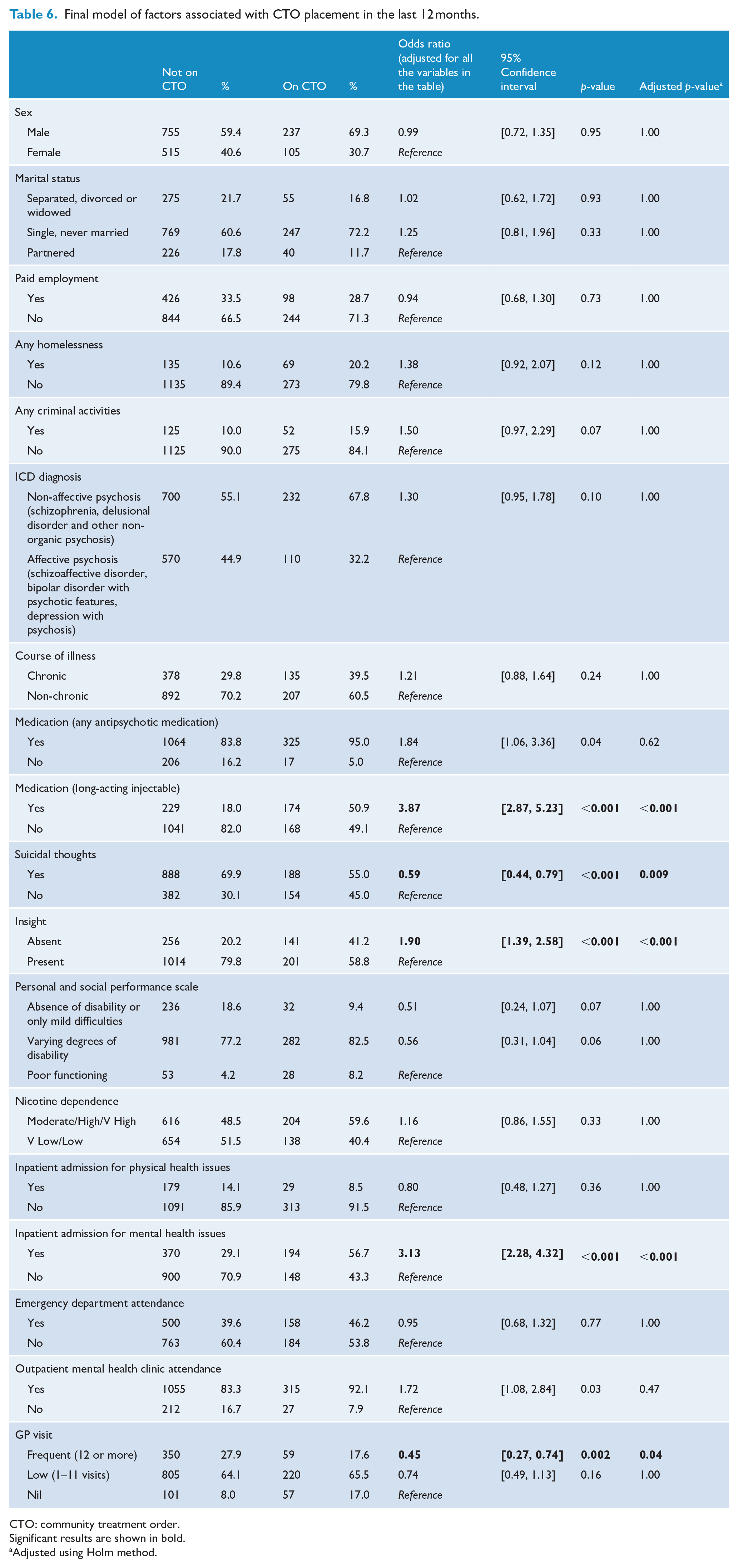
In Model 2, we included variables that were found to be significant in Model 1 (Table 6). Applying the Holm method to adjust for multiple comparisons, we identified that people under CTO were more likely to be on long-acting injectable medication (OR = 3.87, 95% CI: [2.87, 5.23]), lack insight into their illness (OR = 1.90, 95% CI: [1.39, 2.58]) and have been admitted to hospital for mental health issues in the past 12 months (OR = 3.13, 95% CI: [2.28, 4.32]). They were less likely to report suicidal thoughts (OR = 0.59, 95% CI: [0.44, 0.79]) and visited their GP less frequently (OR = 0.45, 95% CI: [0.27, 0.74]). The other variables included in the model were not significant, including sex, marital status, paid employment status, homelessness, past criminal activities, ICD diagnosis, course of illness, medication (any antipsychotic), personal and social functioning, nicotine dependence, inpatient admission for physical health issues, emergency department attendance and outpatient mental health clinic attendance.
Final model of factors associated with CTO placement in the last 12 months.
CTO: community treatment order.
Significant results are shown in bold.
Adjusted using Holm method.
Discussion
Using a large cross-sectional national dataset, our findings showed that people under CTOs were more likely to lack insight and be treated with long-acting injectable antipsychotics but were less likely to report suicidal ideation. People under CTOs also had higher rates of psychiatric inpatient admissions but a lower frequency of GP visits.
Almost a fifth of people with psychosis had been treated under a CTO in the past 12 months. In Model 1, we found that people under CTOs were more likely to be young, single, male, unemployed, homeless and have been involved in criminal activities. In terms of clinical characteristics, people under CTOs were more likely to have a shorter duration but a more chronic course of illness, non-affective psychosis as opposed to affective psychosis, as well as lacking insight. Many of these demographic and clinical variables have also been identified as associated with CTO use in previous studies of administrative data (Kisely et al., 2020a, 2020b). People on CTOs were also more likely to be on antipsychotic medication, including long-acting injectable medication. In addition, they were less likely than the non-CTO group to have experienced suicidal ideation. People under CTOs were also more likely to have poorer personal and social functioning and to use nicotine heavily. Finally, in examining service utilisation patterns, people under CTOs had increased emergency department attendance rates in the past 12 months. The increase is likely to be driven by psychiatric issues as they were significantly more likely to be admitted under psychiatry and significantly less likely to be admitted for physical health issues than the non-CTO group. In the community, people under CTOs had higher rates of outpatient mental health clinic attendance but reduced frequency of visits to GPs compared to those who were not under CTO. In contrast to other existing studies, we did not find that being born outside of Australia or speaking a language at home other than English were associated with CTO placement. This finding should be interpreted with caution. Unlike studies utilising service-level administrative data (where cultural and language differences are not a barrier to be included in the study), this particular group of people may have been systematically under-represented in the current sample as inclusion criteria required participants to speak English and be able to undertake the assessments without the need for an interpreter. Similarly, we did not find a significant association between CTO placement and being of Aboriginal or Torres Strait Islander descent. It is unclear whether this is because of insufficient power, or if it represents a true finding. There have been mixed results from studies of administrative data with two from Victoria and Western Australia finding no association (Kisely et al., 2015; Segal et al., 2017) while one from Queensland reported a greater likelihood (Kisely et al., 2020a). The reasons for these contradictory findings are unclear especially given that Indigenous Australians are more likely to experience involuntary psychiatric admissions (Nagel, 2003). One possibility is the limited availability of appropriate services to administer a CTO in non-urban areas where Indigenous Australians may be more likely to live (Kisely et al., 2015).
In Model 2, we included all variables found to be significant in Model 1. In this adjusted model, we found that people under CTO were more likely to be on long-acting injectable medication, lack insight to illness and be admitted to hospital for mental health issues. They were less likely to experience suicidal thoughts and visit GP less. Other variables were no longer significant in this Model. A major strength of this study was that we were able to investigate clinical characteristics associated with CTO placement in greater, more granular, detail. For instance, we found in our study that people on CTOs were more likely to display a lack of insight but experience less suicidal ideation.
Of particular note, they were approximately four times more likely to be on long-acting injectable medication compared to the non-CTO group. This strong association between CTO placement and long-acting injectable requires further exploration in future studies. Despite its potential to improve the illness course among people with psychosis (Correll et al., 2016), the rate of uptake of long-acting injectable antipsychotic medication remains relatively low (e.g. only 30% of people in SHIP were on long-acting injectables; Suetani et al., 2021). There is an ongoing debate about how early we should consider long-acting injectable antipsychotic medications for people with psychotic disorders (Catts and O’Toole, 2016; Siskind and Dark, 2017). It is important to recognise that in clinical practice, the use of long-acting injectables under CTO is a ‘clinical double-edged sword’. On one hand, treatment under CTO may allow clinicians to discuss the pros and cons of long-acting injectables long term, thus improving the likelihood of informed decision making regarding antipsychotic medication use. On the other hand, patients may associate long-acting injectables with coercion represented by CTO, making them more likely to discontinue the injections once the treatment order expires (Suetani et al., 2014). Given the cross-sectional design of our dataset, we were unable to examine the onset/offset effect of CTOs on long-acting injectable use and related outcomes over time. Interestingly, people on CTOs were less likely than the non-CTO group to experience suicidal ideation. They were also no more likely to report loneliness or dissatisfaction with life compared to those who were not under a CTO. Similarly, there was no difference between the two groups in terms of substance use patterns. One possible explanation for these findings is that the increased clinical contact enforced upon via CTO conditions may positively impact social connectedness for people with psychosis under CTOs. This may lead to the reduced suicidal ideation and substance use and reported social well-being at rates similar to the non-CTO group. Further research is required to examine these somewhat unexpected relationships.
In examining service utilisation patterns, we found that people under CTOs had higher rates of mental health input through increased hospital admission (but not through outpatient mental health clinic attendance). This may represent a process measure due to CTOs mandating engagement with mental health services (Kisely et al., 2020b) or that people under CTOs require increased inpatient admissions due to their illness severity. At the same time, we found that people in the CTO group were significantly less likely to see their GPs. This is concerning given that people with psychosis are more likely to have poor physical health status than people without psychosis (Firth et al., 2019). A previous study using the SHIP dataset demonstrated that over 90% of people living with psychosis were engaged with GPs, and most GPs believed that they had responsibilities to care for the physical and psychological needs of people with psychosis (Waterreus and Morgan, 2018). The reduced GP engagement rate in the CTO group suggests that people subject to CTOs may be particularly vulnerable. One way to strengthen the relationship between primary care and community mental health services may be to increase the inter-sectorial collaboration via co-location (Crompton et al., 2010). For example, GPs may work in community mental health services to target the more vulnerable groups of patients under psychiatry (e.g. people under CTO) while psychiatrists may work within GP clinics to target those who may require intense care for physical health issues but lower intensity input from psychiatry (e.g. people on long-term clozapine therapy with stable mental state). There may also be some implications for future research. While many of the CTO placement predictors in this study are also captured by administrative data, others are missing, such as psychotropic prescription and GP visits. However, these are available through either the Prescription Benefits Schedule (PBS) or Medical Benefits Schedule (MBS). Future research should therefore investigate the possibility of linking state-based administrative data to these Commonwealth databases.
Limitations
The cross-sectional nature of the data prevented us from drawing causal inferences between CTO use and the variables examined. This meant we were unable to explore clinical questions such as the association between insight and how it may impact the subsequent CTO duration and patient prognosis, or the impact of being on then off CTOs and patient medication choices, especially long-acting injectables. The national dataset allowed us to capture a broader cross-sectional picture of people living with psychosis than had been previously available. However, we were unable to differentiate participants by their state of residence. As such, the differences in the use of CTOs across jurisdictions could not be considered in the current study. Furthermore, since 2010, mental health legislation has been updated across multiple states. In particular, there has been an increased emphasis on the salience of whether or not a person has decision-making capacity for the relevant treatment decisions (Callaghan and Ryan, 2016). This is especially relevant given our finding related to the degree of insight and CTO placement. Under new legislation, insight, by definition, may not be congruent with, but related to, decision-making capacity. Thus, future studies under new legislation may find a stronger association between the lack of insight and CTO placement. Specific contextual issues, such as service accessibility and resource availability, are also likely to impact the implementation of CTOs in practice in different places at different times (Vine and Judd, 2019). These factors impact the generalisability of our findings. However, given findings from administrative datasets that show reasonably consistent predictors of CTO placement by both jurisdiction and time, this may be less of a limitation for our results (Kisely et al., 2020b). Additionally, although some key variables such as diagnosis and personal and social functioning were based on interviewer ratings, many variables were based on participant self-report, including CTO status, making them vulnerable to recall bias. It is also likely that some people in the non-CTO group may have been on a CTO beyond the 12 months covered in the questionnaire. However, this would have led to an underestimate of the differences between the two groups.
Conclusion
Our findings suggest that people on CTOs in Australia differ from those who are not under a CTO in their treatment needs. Even though they have increased use of both long-acting injectables and inpatient admissions, they have reduced engagement with their GPs than those who are not under CTOs. It is important that resources and care provision match the needs of this particularly vulnerable group.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211036032 – Supplemental material for Characteristics of people on community treatment orders in Australia: Data from the 2010 National Survey of High Impact Psychosis
Supplemental material, sj-docx-1-anp-10.1177_00048674211036032 for Characteristics of people on community treatment orders in Australia: Data from the 2010 National Survey of High Impact Psychosis by Shuichi Suetani, Steve Kisely, Stephen Parker, Anna Waterreus, Vera A Morgan and Dan Siskind in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group at the time of the survey were V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw and H. Stain. Ethical approval for the study was obtained from relevant institutional human research ethics committees.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.S. has received honoraria from Seqirus.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Australian Government Department of Health and Ageing. This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.