
Abstract
Objective:
Little work has examined Community Treatment Order processes, including mode of termination. This paper aimed to examine service utilisation and legal status following the Community Treatment Order termination by a review board, treating psychiatrist or expiry of order.
Method:
Data-linkage study following the service utilisation of those discharged from a Community Treatment Order of at least 3-month duration for the subsequent 2 years. We used the state-wide database of all contacts with state-funded mental health services in Victoria, Australia.
Results:
Of the 1478 patients who were discharged, 5% were discharged by the review board, 88% were discharged by the treating psychiatrist and in 7% the order expired. Logistic regression indicated that those discharged by the treating service were less likely to be subsequently placed under an involuntary order than those discharged by the Mental Health Review Board or those whose order had expired (odds ratio = 0.61).
Conclusion:
Poorly planned discharge as a result of expiry of the Community Treatment Order or abrupt discharge by the review board may be associated with a more severe relapse and subsequent need for compulsory treatment. The likelihood of being readmitted as an involuntary patient is greater for younger adults and those living in urban settings. In order to minimise the risk of major relapse, strong community engagement with treating services should be supported.
Introduction
Community Treatment Orders (CTOs), in which a person receives involuntary care in the community, have been the subject of considerable controversy, with conflicting evidence as to their effectiveness and utility (Kisely et al., 2011; Kisely and O’Reilly, 2015; Maughan et al., 2014). CTOs were introduced in Victoria through the Mental Health Act (MHA, 1986). Their introduction occurred concurrently with the closure of stand-alone long-stay mental health beds. Victoria has been recognised as having one of the highest rates of CTO utilisation compared with other jurisdictions with provision for involuntary treatment in the community (Dawson, 2005; Light et al., 2012). Arguments for CTOs include a reduction in the need for inpatient admission by better adherence to medication in the community and thus reduced risk of relapse and possibly better morbidity and mortality outcomes (Pinfold and Bindman, 2001). Recent work in the United Kingdom has contributed to the debate on the effectiveness or otherwise of CTOs (Burns et al., 2013; Burns and Molodynski, 2014; Curtis, 2014) with a systematic review of the effect of CTOs on service use concluding that other than medication adherence, there was little evidence that CTOs influenced hospitalisation and service outcomes (Maughan et al., 2014). CTOs of longer duration appeared to confer added benefit in terms of relapse (Swartz et al., 2010). The review concluded that studies of CTO effectiveness should consider the different aspects of process and outcome.
Until the commencement of a reformed MHA in 2014, external review of the decision to make a person subject to an involuntary order in Victoria, Australia, was made by the Mental Health Review Board (MHRB). The rate of discharge by the MHRB remained relatively static with less than 7% of reviews resulting in a ruling to discharge the patient from the CTO and terminate the involuntary order (MHRB, 2013). It is assumed that discharge ordered by the MHRB will be counter to the views of the treating team since the person must be discharged from the CTO if the treating psychiatrist believes the person no longer meets the criteria. (MHA, 1986: s14). Discharge from a CTO is mostly determined by the treating service in the context of discharge planning and provision of ongoing treatment. Some people actively evade mental health services such that the CTO expires, rather than finishing as part of treatment planning.
There has been limited research on whether the mode of discharge results in different outcomes for the person being treated. A study of 124 persons (inpatients) discharged by the Mental Health Review Tribunal under the English 1983 MHA found no difference in subsequent survival period in the community or readmission rate when compared to those not discharged by the Tribunal (Myers, 1997). CTOs were not available in England at the time of that study. The purpose of our study was to examine service use following discharge from a CTO, making comparisons between those discharged by the MHRB, by the treating psychiatrist or by the expiration of their CTO.
Methods
Study design
In this retrospective cohort study, we identified all individuals in Victoria, Australia, who had been on a CTO for at least 3 months and were then discharged between 1 January 2008 and 31 December 2008 (n = 1520). We followed these individuals for 24 months to identify their service use. This period was chosen to facilitate a later comparison between two legislative frameworks. We excluded the records of 24 individuals whose reason for discharge was death and 18 individuals where no information on the reason for discharge was available, giving a sample of 1478 participants.
We used a 3-month period on a CTO as the inclusion criterion because in our clinical experience, this corresponded to those with severe mental illness with associated disability and need for treatment. We considered service utilisation as a proxy measure of whether the person had experienced a relapse (need for inpatient admission), the severity of the relapse (return to involuntary status) and whether the person remained engaged with services following discharge from a CTO (ongoing community contacts). Ethical approval was obtained from the Melbourne Health Human Research Ethics Committee (No. 2013.109).
Data sources
The Department of Health Victoria administers the Client Management Interface/Operational Data Store (CMI/ODS) data system that records all registrations and contacts with state-funded mental health services. The CMI/ODS records basic demographic information about patients as well as detailed information about the use of mental health services. The Department provided us with baseline data on the 1478 individuals who met the inclusion criteria along with follow-up data on any inpatient admissions (n = 2407 records), any community mental health contacts (n = 7078 records) and information on changes in their mental health legal status (n = 8652 records). The data set included mental health diagnosis. As this sometimes changed between episodes, we used the primary diagnosis prior to discharge, or if this was unavailable, we used the primary diagnosis immediately following discharge. Using a unique identifier, we converted these administrative records to a person-level data set, constructing outcome variables that represented whether the individual went back onto an involuntary order of any type in the subsequent 24 months (yes or no), went onto a CTO (yes or no) or had an inpatient admission (yes or no). We also constructed predictor variables based on the patient’s status at discharge. These were as follows: method of discharge (discharge by the MHRB, discharge by the treating psychiatrist or expiration of order), sex, age (16–24 years, 25–65 years, >65 years), location (urban, rural) and days on order prior to discharge (⩽180 days, 181–364 days, >364 days).
Statistical analysis
We report descriptive statistics of the sample. In order to assess whether there were systematic differences between patient’s method of discharge and the other predictors, we calculated two-way cross-tabulations between method of discharge and sex, age location and days on order prior to discharge. Using logistic regression, we examined the association between method of discharge and each of the outcome variables (involuntary order of any type, CTO, inpatient admission). As we were interested in the outcomes of those whose CTO was terminated by the MHRB compared to the other modes, we made this our reference category. Our models adjusted for sex, age, location, days on order prior to discharge and diagnosis. All analyses were undertaken in Stata 13.1.
Results
Sample characteristics
The characteristics of the sample are shown in Table 1. The majority were male (60%), aged between 25 and 65 years (85%), living in urban location (77%) and had been on a CTO for more than a year at discharge (80%). The most common diagnosis was schizophrenia and related disorders (72%). We were unable to provide a diagnosis in 12% of cases.
2008 Sample characteristics.
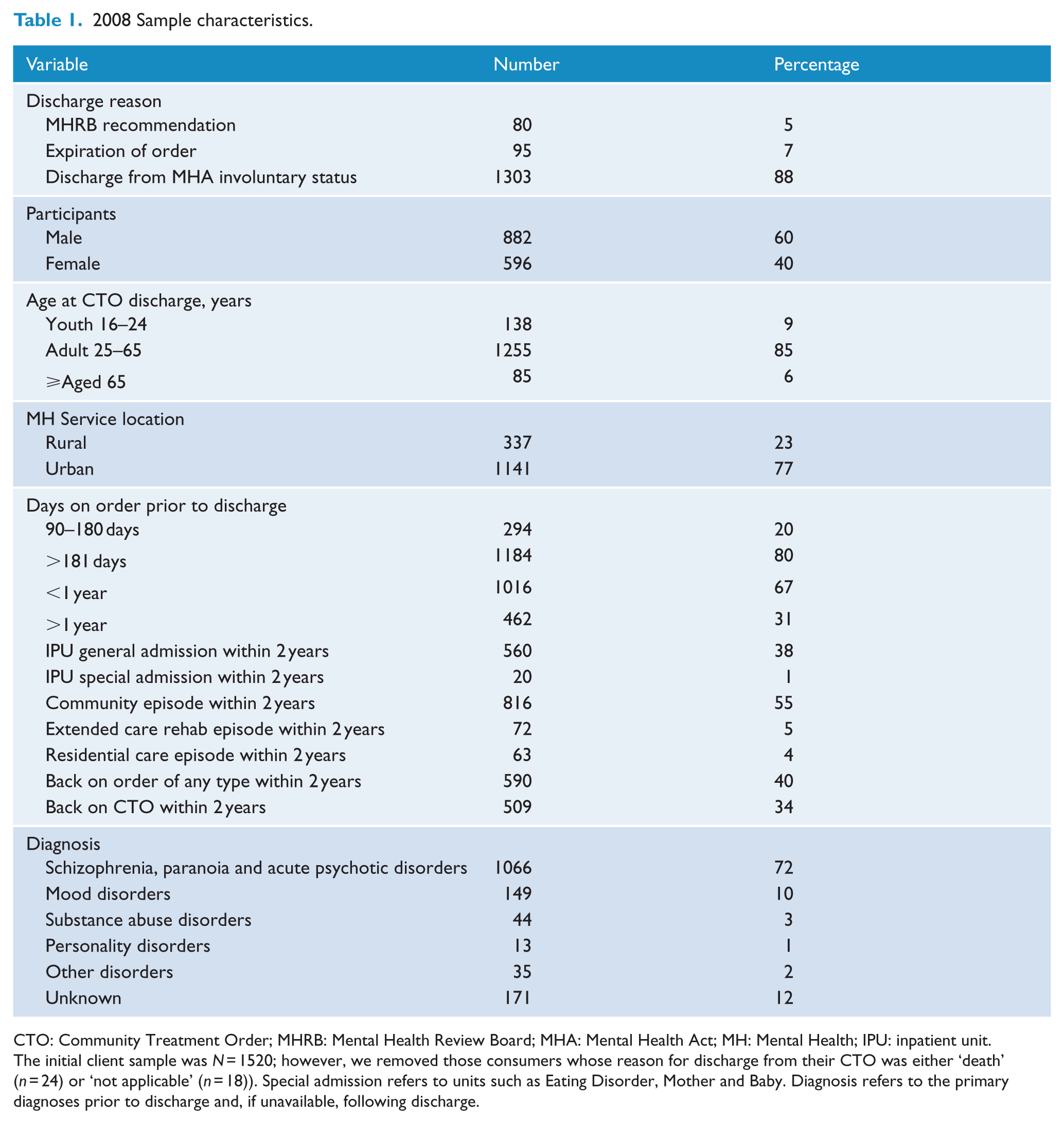
CTO: Community Treatment Order; MHRB: Mental Health Review Board; MHA: Mental Health Act; MH: Mental Health; IPU: inpatient unit.
The initial client sample was N = 1520; however, we removed those consumers whose reason for discharge from their CTO was either ‘death’ (n = 24) or ‘not applicable’ (n = 18)). Special admission refers to units such as Eating Disorder, Mother and Baby. Diagnosis refers to the primary diagnoses prior to discharge and, if unavailable, following discharge.
A total of 80 individuals (5%) were discharged from the CTO by the MHRB, 1303 individuals (88%) were taken off the CTO by the treating service and orders expired for 96 individuals (7%). Of the sample, 590 (39%) went back on an involuntary order (inpatient or CTO) within the following 2 years and 509 (34%) went back onto a CTO at least once. For those who went back on an order of any type, the mean time between coming off the CTO and going back onto any type of order was 262 days. The mean time for going back onto a CTO was 304 days. There was no significant difference between discharge by the service and discharge by the MHRB in days to next contact or days to next admission. Of those discharged by the MHRB, 34 (43%) experienced another inpatient admission within the subsequent 2 years while 495 (33%) of those discharged by the service were admitted. Of the total number, 560 (38%) were admitted during the following 2 years. There was no significant difference in age or gender in those who were discharged by the service or MHRB or whose order expired. There appeared to be a greater likelihood that those in a rural setting would be lost to follow-up resulting in expiry of their CTO (Table 2). The diagnosis did not differ significantly between the modes of CTO termination.
Mode of discharge.
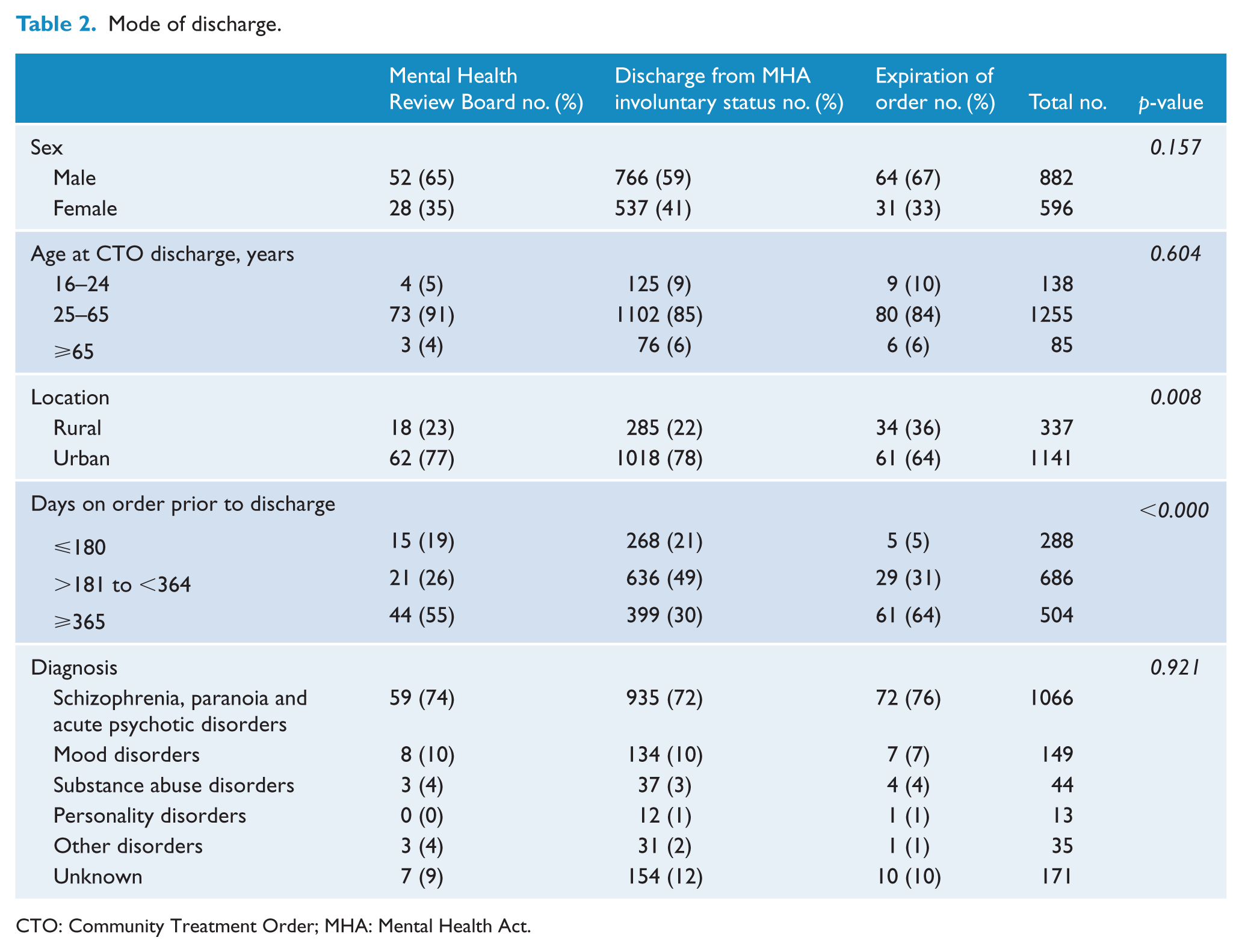
CTO: Community Treatment Order; MHA: Mental Health Act.
The logistic regression analysis showed that the odds of going back onto an order of any type within 2 years of release differed by the mode of discharge (Table 3). In comparison with those released by the MHRB (the reference category), and independent of the other covariates in the model, those released because their order had expired had approximately the same odds of returning to a new order of any kind (inpatient or CTO) (odds ratio [OR] = 1.02) and those discharged from the order by the treating psychiatrist had lower odds of returning to a new order (OR = 0.61). Similarly, those discharged from the CTO by the MHRB had about the same odds of returning to a CTO as those whose order had expired (OR = 1.2), while those who were discharged from the MHA involuntary status by the treating psychiatrist had lower odds (OR = 0.63).
Unadjusted and adjusted logistic regression results predicting going back on an involuntary order of any type, a CTO and general inpatient admission.
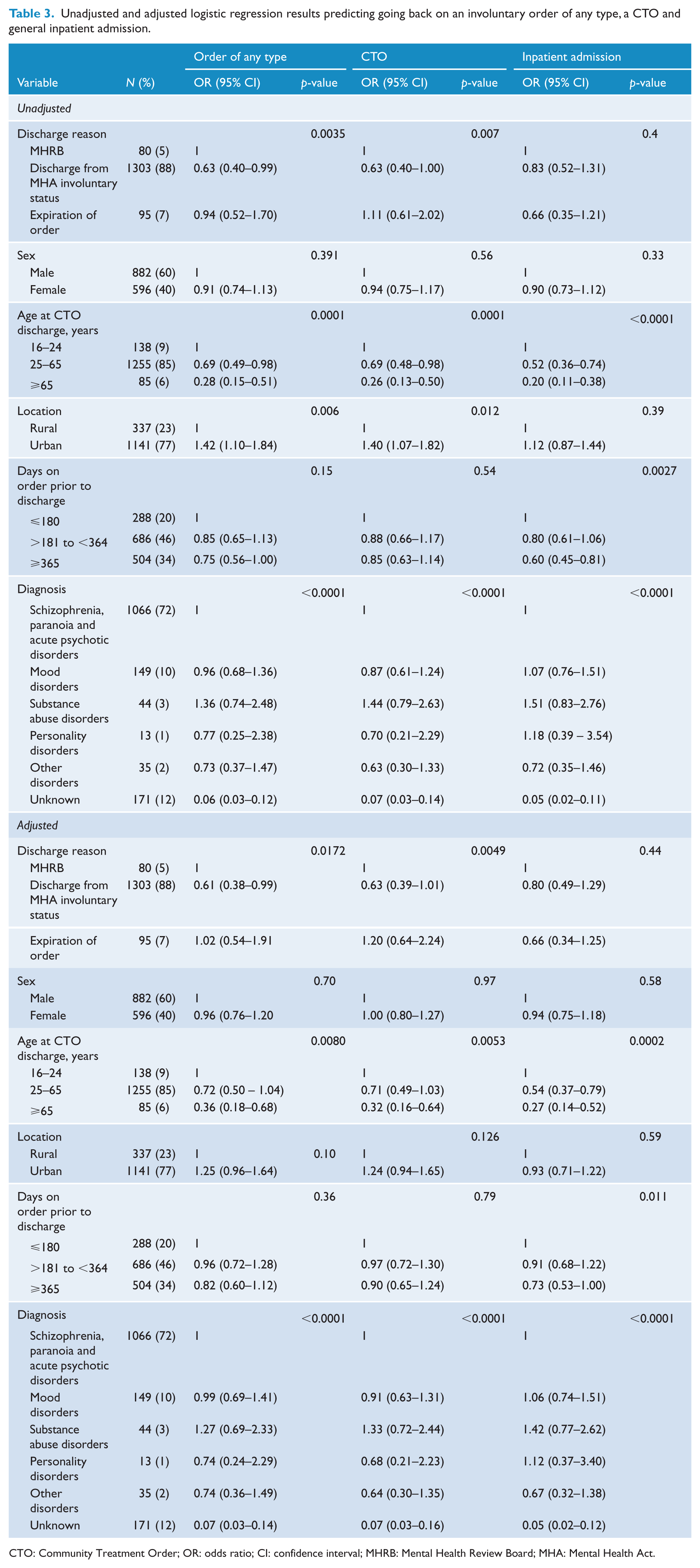
CTO: Community Treatment Order; OR: odds ratio; CI: confidence interval; MHRB: Mental Health Review Board; MHA: Mental Health Act.
In addition, the odds of returning to an order of any type, a CTO or having an inpatient admission were related to age. Youth had the highest odds of returning to a new order, and this declined with age. Similarly, those living in urban locations had higher odds of returning to an order of any type or a CTO than those living in rural locations, although this finding did not hold for inpatient admissions. Finally, sex and the number of days on order prior to discharge were unrelated to returning to an order.
Discussion
There are a number of tensions in where and how we provide services to those with severe mental illness. There is general support for policy and practice that encourages consumer choice, provision of care in the least restrictive way and respect for the rights of individuals. But there is also increasing recognition and concern regarding poor physical health and disability outcomes of those who suffer from severe mental illness and concerns regarding violence in mental health clinical settings and community safety (Szmuckler, 2004; Zipursky et al., 2013). There is also concern that for some people disengagement with services and non-adherence with treatment lead to increased risk of relapse and progressive deterioration related to the mental illness (Weiden, 2006). Maintaining engagement and treatment adherence in illnesses such as schizophrenia is challenging where there is episodic treatment by mental health services, fragmented funding and a dearth of strong community health and support services (Fleischhacker et al., 2014).
Mental health legislation reflects the tension between individual autonomy and clinical care in that it provides for treatment and detention as an involuntary patient where the person is deemed by clinical staff to meet strict criteria, but also places limits on this by empowering an external non-clinical body to reverse those decisions. In general, involuntary treatment can only be provided where the person has a diagnosed mental illness that is believed to be associated with increased risk of harm, and they have refused or are unable to comply with recommended treatment.
Under the 1986 Victorian Act, the decision to place a person on a CTO was made by the Authorised Psychiatrist (AP) and subject to review by the MHRB. With the introduction of a new MHA in 2014, there has been a significant shift in that the decision to place a person on a CTO, and the duration, is now made by the Mental Health Tribunal (MHA, 2014).
In most cases, CTOs are made in regard to persons who suffer from severe and often relapsing mental illness such as schizophrenia and schizoaffective disorder. In our sample and more generally in Victoria, these two diagnoses account for three-quarters of people who appear before the MHRB (MHRB, 2014). Although there is now agreement that the outlook for people with schizophrenia is better than was believed in the past, long-term studies show that a significant number of people will experience clinical and social deficits (Van Os and Kapur, 2009). The best outcomes are associated with ongoing medication and psychosocial support. It is also likely that with each relapse, there is further deterioration in social and occupational functioning (Zipursky et al., 2014; Zygmunt et al., 2002). Relapse is strongly associated with non-adherence to treatment (Gitlin et al., 2001). Non-adherence has also been associated with poorer functional outcomes including increased likelihood of readmission, violence, substance abuse and victimisation (Ascher-Svanum et al., 2006). CTOs are primarily aimed at improving treatment adherence and facilitating engagement along with improved understanding and acceptance of treatment.
In this study, we were interested in whether there was any difference in subsequent service contact where the MHRB made a decision counter to the treating team. While there were few differences in subsequent contact, we found that there was a greater likelihood of going back onto an involuntary order if the discharge was made by the MHRB or if the CTO expired – most likely because the person had disengaged with services. It is plausible that discharge planning was less advanced in these cases. We were not able to consider whether there was a different pattern of diagnosis associated with termination of the CTO by the service, the MHRB or because of expiry.
An additional finding of this study is that the risk of needing further treatment as an involuntary patient was greater for young people and for those living in urban settings. It seems likely that younger people have less understanding of their illness and are thus more likely to drop out of treatment. Urban services carry a greater proportion of those who are homeless and who have co-morbid substance use, which may contribute to the increased risk of relapse and readmission as an involuntary patient.
There is good evidence that the best outcome for those who suffer severe mental illness is to minimise the number and severity of relapses and that the best way to achieve this is through medication alongside good psychosocial support (Fleischhacker et al., 2014; Zipursky et al., 2013). Adherence to prescribed treatment is more likely when patients are well informed, when their choice regarding treatment can be supported and where there is good clinical engagement. CTOs have a primary function of endeavouring to improve treatment adherence. Ideally, this adherence means that a person remains well while he or she learns more about the illness such that they will continue with treatment in the absence of compulsion. While recognising that more than 50% of those who were discharged by the MHRB did not have an admission over the next 2 years, our findings suggest that those discharged by the MHRB, or those who dropped out of treatment because they were lost to follow-up and the CTO expired, were at increased risk of having a relapse of a severity that required readmission under the MHA. While perhaps little can be done to address those who actively seek to avoid services, our findings suggest that we should be working with the external review body and those who develop mental health policy to allow a period of discharge planning rather than abrupt cessation of the CTO. This study does not purport to provide evidence of support for CTOs per se, but does suggest that engagement and discharge planning associated with appropriate use of a CTO may lessen the severity and therefore the negative impact of future illness episodes. Where discharge occurs as a result of the decision of the MHRB, the service and patient should be given time and encouragement to put in place supports for ongoing treatment and engagement.
This study has a number of limitations. We have only included service utilisation in the 2 years after termination of the CTO and so cannot comment on admissions over a longer period. We were not able to include comorbidity as a variable of interest as this is not reliably entered into the database. We were not able to determine whether the persons discharged by the MHRB were more or less likely to have legal representation. It is also acknowledged that the data only cover contact with mental health services funded by the State and thus exclude those services provided through private specialist and primary care services. In Victoria, all involuntary or compulsory care is provided only in state-funded services. In addition, a number of psychosocial factors that may impact the decisions made by the MHRB, or the service, such as family support, vocational or educational achievements, were not able to be included. Despite this, this study has a number of advantages over previous studies in this area, including the use of a state-wide data collection and a long follow-up time. Our finding of less likelihood of returning to involuntary care if discharge was planned and implemented by the treating service supports the aims and intention of better engagement by treating services with people who experience severe mental illness.
Footnotes
Acknowledgements
The data set was provided by the Department of Health and Human Services, Victoria, with the kind assistance of Mr Lachlan Rimes. Ruth Vine was primarily responsible for this study and drafted the initial manuscript. Matthew Spittal and Suzanne Turner provided assistance with the statistical analysis. Jane Pirkis and Fiona Judd provided oversight and critical comment. All authors contributed to writing the manuscript and approved the final version.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.