
Abstract
Objective:
While incidence rates of depression and anxiety disorders in the elderly have been comprehensively investigated, the incidence rates of other mental disorders have rarely been researched. The incidence rate and predictors of various mental disorders in the elderly were evaluated in different European and associated countries.
Methods:
A cross-sectional and longitudinal multi-centre survey of Diagnostic and Statistical Manual of Mental Disorders (4th ed.) diagnoses was conducted in different European and associated countries (Germany, Italy, Spain, Switzerland, the United Kingdom and Israel) to collect data on the prevalence and incidence of mental disorders in the elderly. The sample size of the longitudinal wave was N = 2592 elderly.
Results:
The overall 1-year incidence rate for any mental disorder in the elderly is 8.65%. At 5.18%, any anxiety disorder had the highest incidence rate across all diagnostic groups. The incidence rate for any affective disorder was 2.97%. The lowest incidence rates were found for agoraphobia (1.37%) and panic disorder (1.30%). Risk factors for the development of any mental disorder were never having been married, no religious affiliation, a higher number of physical illnesses and a lower quality of life.
Conclusion:
In comparison to other studies, lower incidence rates for any affective disorder and middle-range incidence for any anxiety disorder were found. To the authors’ knowledge, no prior studies have reported 1-year incidence rates for somatoform disorder, bipolar disorder and substance misuse in community-dwelling elderly. These findings indicate the need to raise awareness of psychosocial problems in the elderly and to ensure adequate availability of mental health services.
Introduction
The percentage of people aged 65 years or over in the European population was 18.0% in 2019 and is expected to rise to 26.1% by 2050 (United Nations Department of Economic and Social Affairs, 2019). Due to the predicted life expectancy increases, physical and mental health in old age is of the utmost importance (Karel et al., 2012). The MentDis_ICF65+ study found lifetime diagnoses of a mental disorder in one of two individuals aged 65–84 years (47.0%) (Andreas et al., 2017). The 12-month prevalence rate in this sample was 35.2%, and the current prevalence rate showed that nearly a quarter of the sample was diagnosed with any mental disorder at the time of the study (23.3%). Anxiety disorders (25.6%) were the most prevalent mental disorders, followed by substance misuse (18.2%) and affective disorders (14.3%) over the course of the lifetime. The 12-month rates (17.2%) and current prevalence rates (11.4%) were also highest for anxiety disorders. In contrast, affective disorders were more prevalent than substance-related disorders in the 12 months (13.7% vs 8.9%) and current prevalence (8.0% vs 4.6%) rate analyses (Andreas et al., 2017). The MentDis_ICF65+ study showed that the burden of mental illness in the European elderly was previously underestimated. To adequately adapt mental health services in Europe, more specific parameters are needed in addition to prevalence rates. In particular, these parameters are incidence rates and the identification of risk factors for all mental diseases in community-dwelling elderly.
Among mental disorders in elderly people, incidence rates have been comprehensively reported for depression (Büchtemann et al., 2012; Chang-Quan et al., 2010; Cole and Dendukuri, 2003; Conde-Sala et al., 2019; Luppa et al., 2012; Weyerer et al., 2013). A number of reviews of studies on the incidence of depression in the elderly agree on the variation in reported rates. A review examining the incidence rates of depressive disorders in persons aged ⩾70 years reports incidence rates of major depression (MD) of 0.2–14.1/100 person-years (Büchtemann et al., 2012), and another review reports frequencies of incident depression from 1.8% to 24.1% (median = 12.0%) for studies including persons aged ⩾50 years (Cole and Dendukuri, 2003). Büchtemann et al. (2012) also reported the incidence of clinically relevant depressive symptoms (6.8/100 person-years), and a very similar rate was reported in another review that included studies with persons aged ⩾55 years (Chang-Quan et al., 2010). Recent studies support these findings (Conde-Sala et al., 2019; Luppa et al., 2012; Weyerer et al., 2013). A review on anxiety disorders in older adults suggests that the probability of the onset of anxiety disorders in late life is low (Wolitzky-Taylor et al., 2010).
Given the heterogeneous designs of prior studies regarding the use of different instruments and diagnostic systems, it is hardly possible to compare the incidence rates of mental disorders. A study examining the 1-year incidence of mental disorders for community-dwelling elderly aged ⩾65 years with an overall 1-year incidence rate of 6.2% reported higher incidence rates for depression (3.4%) than for anxiety disorders (2.4%) (Préville et al., 2010). Currently, incidence rates in the elderly are mostly available for depression and anxiety disorders. There is still a great need to collect data with age-sensitive instruments and to collect further information on the incidence rates of other mental disorders in the elderly. Furthermore, the choice of applied instruments has to be taken into account. In addition to the age-sensitiveness of instruments, the format has an impact on the identified rates. For example, studies on the incidence of depression in old age using a standardized interview have a tendency to report lower incidence rates than studies using self-report scales for diagnosis (Büchtemann et al., 2012; Chang-Quan et al., 2010).
To examine whether mental disorders in the elderly are related to specific risk factors such as old age, living conditions in retirement and health conditions, and whether these risk factors are the same throughout various mental disorders, we addressed this issue in a large sample of elderly from the general population. The scope of studies reporting risk factors for mental disorders in the elderly has primarily focused on depression and rarely on any other mental disorder (Vink et al., 2008). Risk factors that are frequently reported as significant for the incidence of late-life depression are the baseline depression score (Cole and Dendukuri, 2003; Harris et al., 2006), physical chronic diseases (Beekman et al., 2001; Chang-Quan et al., 2010; Vink et al., 2008), female gender (Beekman et al., 2001; Büchtemann et al., 2012; Cole and Dendukuri, 2003; Conde-Sala et al., 2019; Luppa et al., 2012; Pálsson et al., 2001; Weyerer et al., 2013), poor physical health (Cole and Dendukuri, 2003; Harris et al., 2006; Vink et al., 2008; Weyerer et al., 2013), poor self-rated health status (Chang-Quan et al., 2010; Conde-Sala et al., 2019; Luppa et al., 2012; Vink et al., 2008), poor social network and loneliness (Cole and Dendukuri, 2003; Conde-Sala et al., 2019; Harris et al., 2006; Luppa et al., 2012; Vink et al., 2008) and age (Pálsson et al., 2001; Weyerer et al., 2013). Except for chronic diseases, those risk factors coincide mostly with predictors that are also reported as significant for anxiety disorders (Vink et al., 2008). Despite the similarities, there are differences in the prediction of the onset of anxiety disorders versus depression in the elderly. While being lonely or in grief is more likely to be associated with the onset of late-life depression, direct threats and traumatic events more likely to determine the onset of anxiety disorders in the elderly. Moreover, while increasing age is a predictor of the incidence of late-life depression, it appears to be protective against the onset of anxiety disorders (Vink et al., 2008). Studies examining predictors of incidence for more than one mental disorder in old age indicate similar risk factors, e.g. female gender, physical health status and low income (Préville et al., 2010; Samuelsson et al., 2005).
The objective of this study was to assess the 1-year incidence rate of the most frequent mental disorders (e.g. depression, anxiety, somatoform disorder, bipolar disorder) across six different European and associated countries and to identify predictors of the 1-year incidence of any mental disorder in community-dwelling elderly aged 65–84 years.
Methods
Design
Data were collected within the European project MentDis_ICF65+ study (Andreas et al., 2017), which is a cross-sectional and longitudinal multi-centre survey that aims to collect data on the prevalence, incidence and correlations of mental disorders in the elderly. The protocol of the study has been reported elsewhere (Andreas et al., 2013; Volkert et al., 2017). A random sample of N = 3142 older men and women (65–84 years) living in selected catchment community areas of each participating country (at least 500 subjects from each country), stratified by age and gender, was drawn from the population registries in Hamburg (Germany) and Ferrara (Italy) and from the postal addresses of market research units in Madrid (Spain), Geneva (Switzerland), London (the United Kingdom) and Jerusalem (Israel). Inclusion criteria for the participants were the ability to provide informed consent, living in the predefined catchment area at the beginning of the study and being at least 65 and less than 85 years old. Exclusion criteria were moderate cognitive impairment as assessed with the MMSE (Mini-Mental State Examination, cut-off score > 18) (Folstein et al., 1975) and insufficient level of corresponding language. Household residents were interviewed face to face by trained lay interviewers using the CIDI65+ (Wittchen et al., 2015) between January and October 2011 (Andreas et al., 2017).
Measures
The Composite International Diagnostic Interview for the elderly (CIDI65+)
Mental disorders were diagnosed with an adapted, age-sensitive version of the CIDI, the CIDI65+ (Wittchen et al., 2015). This fully structured lay interview generates diagnoses according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria. The process of adapting the test to the unique conditions of the elderly cover several components, including the addition of words, alternative questions and detailed section introductions, breaking down long questions into less complicated questions, sensitizing scales upfront (introductory sentences were included to make subjects aware of the following questions/items at the beginning) and embedding a fuller spectrum of syndromes. The English paper–pencil version was translated into German, Spanish, Hebrew, Italian and French with a back-translation and then computerized (Volkert et al., 2017). Questions were administered by trained lay interviewers using a computer-assisted personal interview (CAPI) version of the CIDI65+. The interviewers completed a 2-day workshop, and the reliability of ratings was approved by the authors of the CIDI65+. The assessment of the test–retest reliability of the newly adopted CIDI65+ showed good results for any mental disorder (k = 0.63), MD (k = 0.55), anxiety (k = 0.62), substance use disorders (k = 0.77) and obsessive-compulsive disorder (k = 1.00). Intraclass correlation coefficients (ICC) for age of onset, recency, quantity, frequency and duration questions ranged between k = 0.60 and 0.90. Further details of the CIDI65+ psychometric properties are reported elsewhere (Wittchen et al., 2015).
The Health of the Nation Outcome Scales 65+
The Health of the Nation Outcome Scales for older people (HoNOS65+) (Burns et al., 1999; Wing et al., 1998) is a 12-item clinician-rated instrument to assess the severity level of 12 problem areas of mental health in older people (e.g. item 2: self-harm; item 7: depressive mood). Items are scored on a scale from 0 (no problem) to 4 (severe or very severe problems).
The HoNOS65+ has a comprehensive glossary with anchor examples for scoring. The instrument is one of the most commonly used scales for older people in psychiatric services and has mostly satisfactory psychometric properties (Pirkis et al., 2005; Reilly et al., 2004).
World Health Organization’s QOL measure
The 26-item version of the WHO Quality of Life questionnaire (The WHOQOL Group, 1998a) was used to measure quality of life. The World Health Organization’s QOL measure (WHOQoL-BREF; The WHOQOL Group, 1998a) was developed by the World Health Organization from the WHOQoL-100 item version. The self-report questionnaire assesses an individual’s quality of life, including physical and psychological well-being, environmental factors and social support, while also taking into account the context of culture and value systems, personal goals, standards and concerns. The psychometric properties are satisfactory (The WHOQOL Group, 1998b), and there is evidence that the WHOQOL-BREF is appropriate for older people (Naumann and Byrne, 2004).
World Health Organization Disability Assessment Schedule II
To assess activities and participation according to the International Classification of Functioning, Disability and Health (ICF) (World Health Organization, 2001), the 12-item self-report version of the World Health Organization Disability Assessment Schedule II (WHODAS II; World Health Organization, 2000) was used. The WHODAS II measures functional impairment of daily activities in six different areas (including communication and self-supply). Satisfactory psychometric scores for patients with affective disorders are reported regarding reliability and validity (Pösl, 2004), and there is initial evidence that the WHODAS II is an adequate instrument for assessment in old age (Kim et al., 2005).
Statistical analyses
We calculated adjusted 1-year incidence rates as a percentage. Incidence rate analysis included cases where no lifetime prevalence was present in wave 1. This is true for the analysis of individual diagnoses as well as for the analysis of diagnostic groups. Incidence estimates and 95% confidence intervals resulting from logistic regression models with adjustment for centre, sex and 5-year age groups, allowing for an interaction between sex and age (if significant), were calculated. The reported estimates are the marginal means resulting from the logistic models. In a re-examination, we first combined incidence rates with recurrence rates by including cases with lifetime prevalence in wave 1 analysis and by including cases that already have one of the cumulated diagnoses in wave 1. To identify sociodemographic and illness-related characteristics of participants in the first wave that were associated with drop-out, i.e. non-participation in the second wave (1 year later), logistic regression analyses with backward elimination were conducted (based on non-significant p-values of F-tests), taking into account the survey structure of the data.
Furthermore, we examined risk factors for the development of any mental disorder. Logistic regression analyses with backward elimination were conducted to identify sociodemographic and illness-related characteristics associated with the incidence of any mental disorder over the course of 1 year. The analysis included all participants who did not fulfil diagnostic criteria for a mental disorder at the initial interview but were suffering from a mental disorder at the 1-year follow-up.
To identify predictors of the persistence of any mental disorders at the second wave, logistic regression analyses were conducted. The analysis included all participants who fulfilled diagnostic criteria for a mental disorder at the initial interview and who still suffered from the disorder 1 year later.
Based on the study by Chen et al. (2010), we used the following ranges to interpret the odds ratio (OR) as an effect size: OR < 1.5 = small effect; OR = 1.5–4.9 medium effect and OR > 5 = large effect. All analyses were computed using Stata 12.1 (StataCorp, 2011).
Results
Participant and non-participant analyses
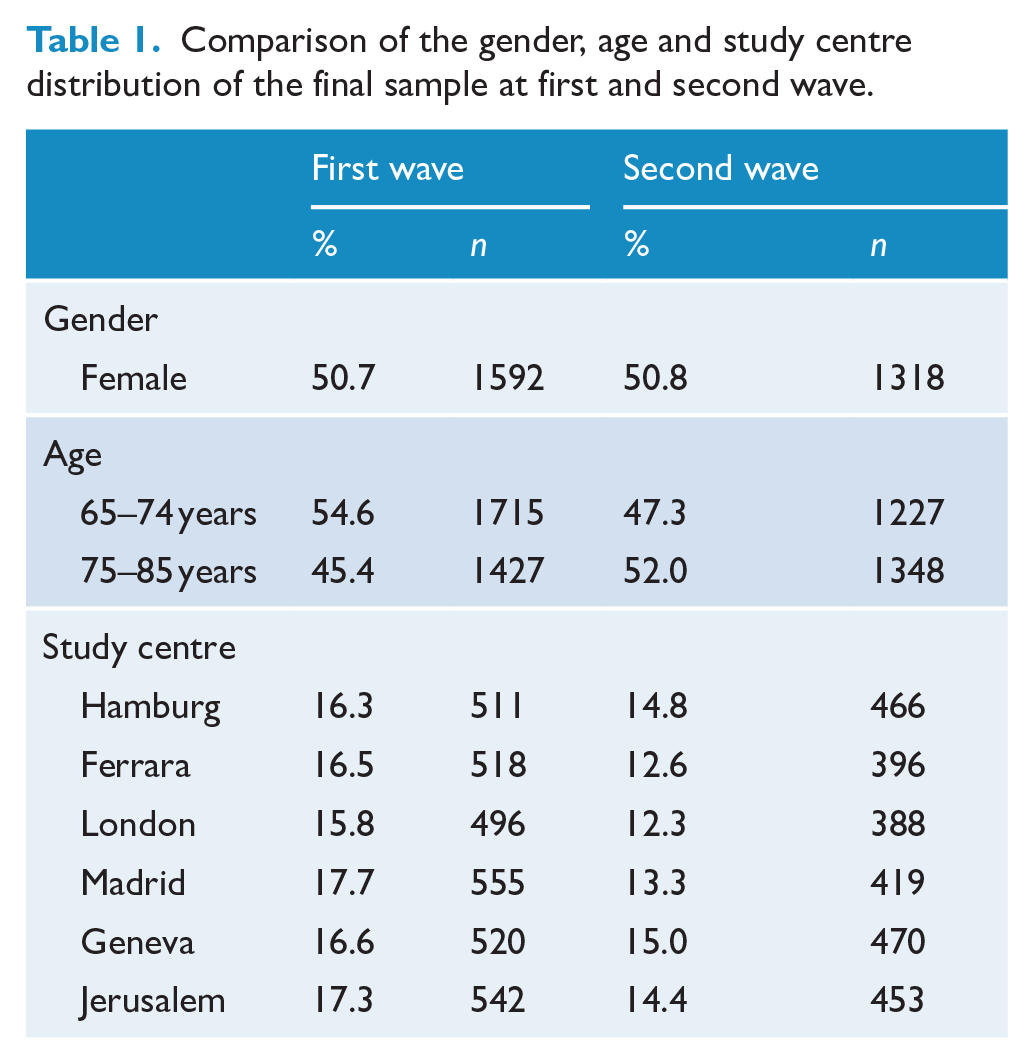
The total number of participants in the second wave of the survey was N = 2592. The gender distribution was equally divided at both waves, and more than half (52.01%) of the participants were between 75 and 85 years old (due to the stratification of the data). The sample sizes were equally distributed across study centres (Table 1).
Comparison of the gender, age and study centre distribution of the final sample at first and second wave.
The total drop-out rate between the first interview and the follow-up 1 year later was 17.5%. The most frequent reason was refusal to take part again (39.9%), followed by ‘not reached’ (18.0%), currently ill/unwell (11.1%), died (6.6%) and other reasons (22.1%) (Figure 1). In only 2.3% of the cases, the contact details were incorrect. Characteristics significantly associated with non-participation in the follow-up were study centre, education, socio-economic status, number of children and number of physical illnesses. Non-participation rates in Ferrara (22.9%), London (21.3%) and Madrid (21.4%) were significantly higher than in Hamburg (10.2%), Geneva (10.9%) and Jerusalem (13.9%). A higher drop-out rate was also found for participants with lower education (i.e. fewer years of schooling), poorer financial situation, a larger number of children and a larger number of physical illnesses (see also online supplement).
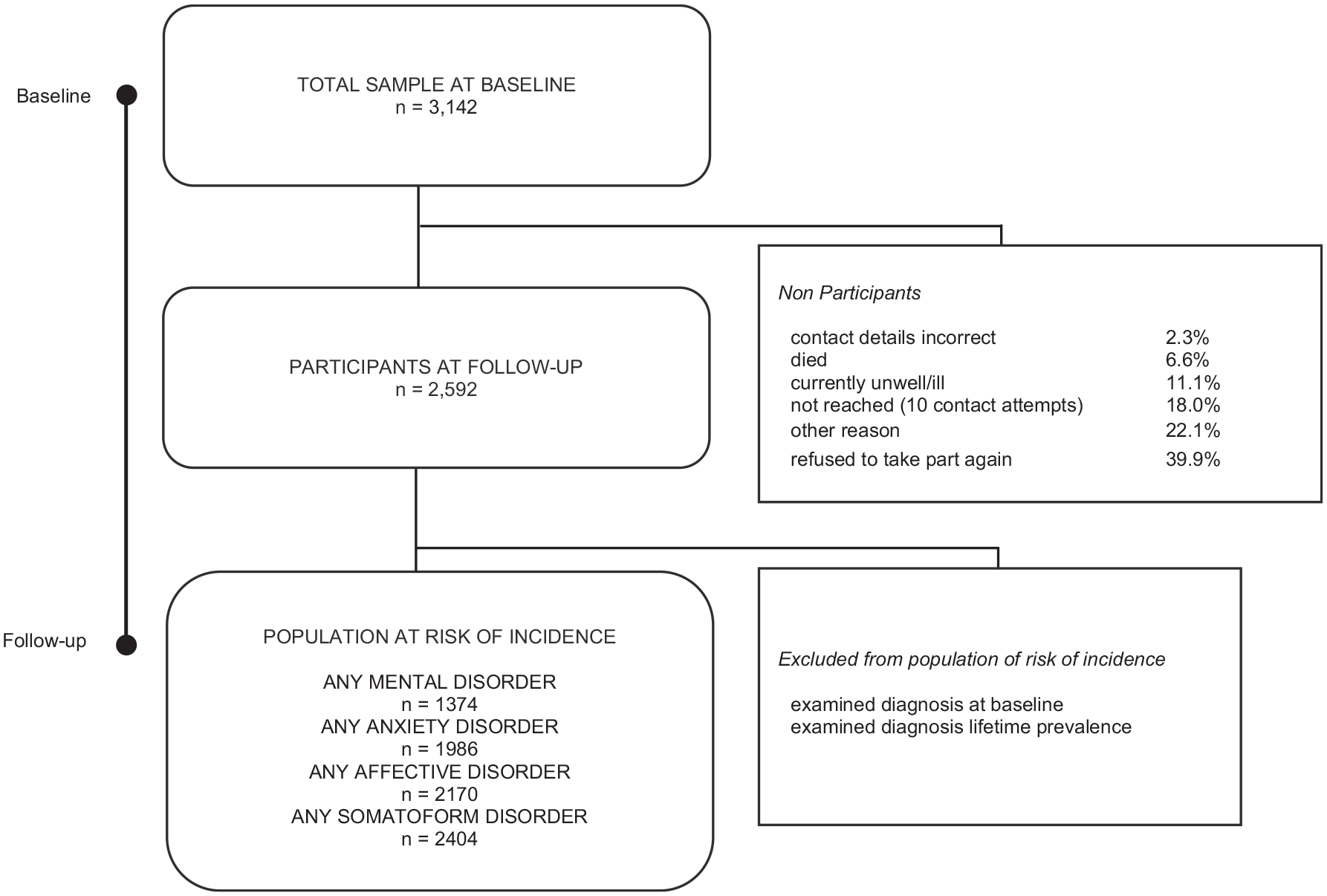
Sampling flowchart.
Sample
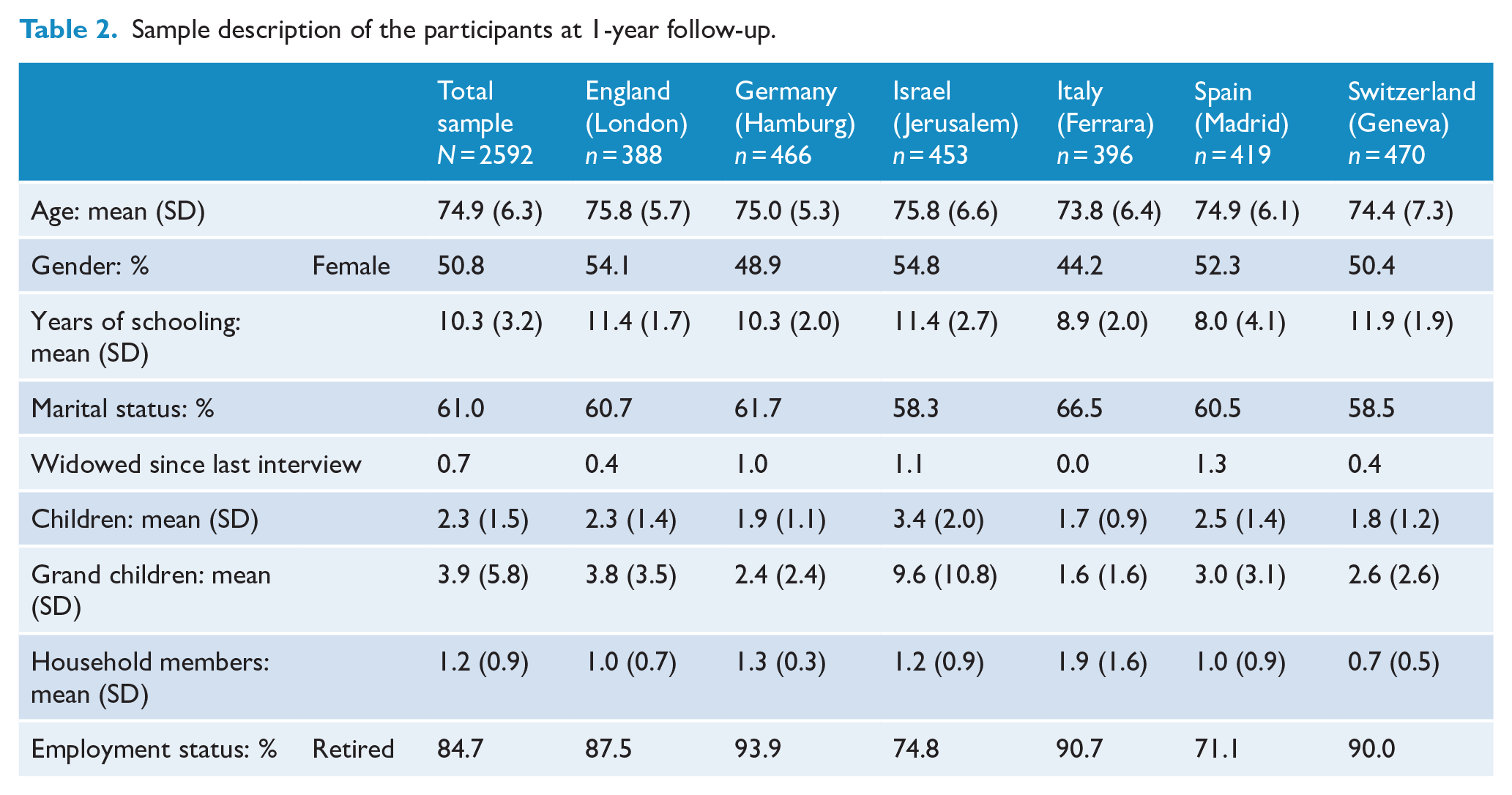
The sample characteristics of the 1-year follow-up participants are depicted in Table 2. The mean age of the elderly was 74.9 years (SD = 6.3 years). Most of the participants were born in the country of the interview with the exception of Israel, where only 200 of the 453 elderly were born in their country of residence. On average, most of the elderly had 10 years of schooling. Thus, the sample can be considered higher educated. Nearly 1 percent had been widowed since the last interview, and more than 60% were still married at the follow-up of the study. Most of the participants were retired on the date of the interview (84.7%).
Sample description of the participants at 1-year follow-up.
Incidence rates of mental disorders
Adjusted and weighted incidence rates for common DSM-IV mental disorders are displayed in Table 3.
One-year incidence rates of frequent mental disorder (%).
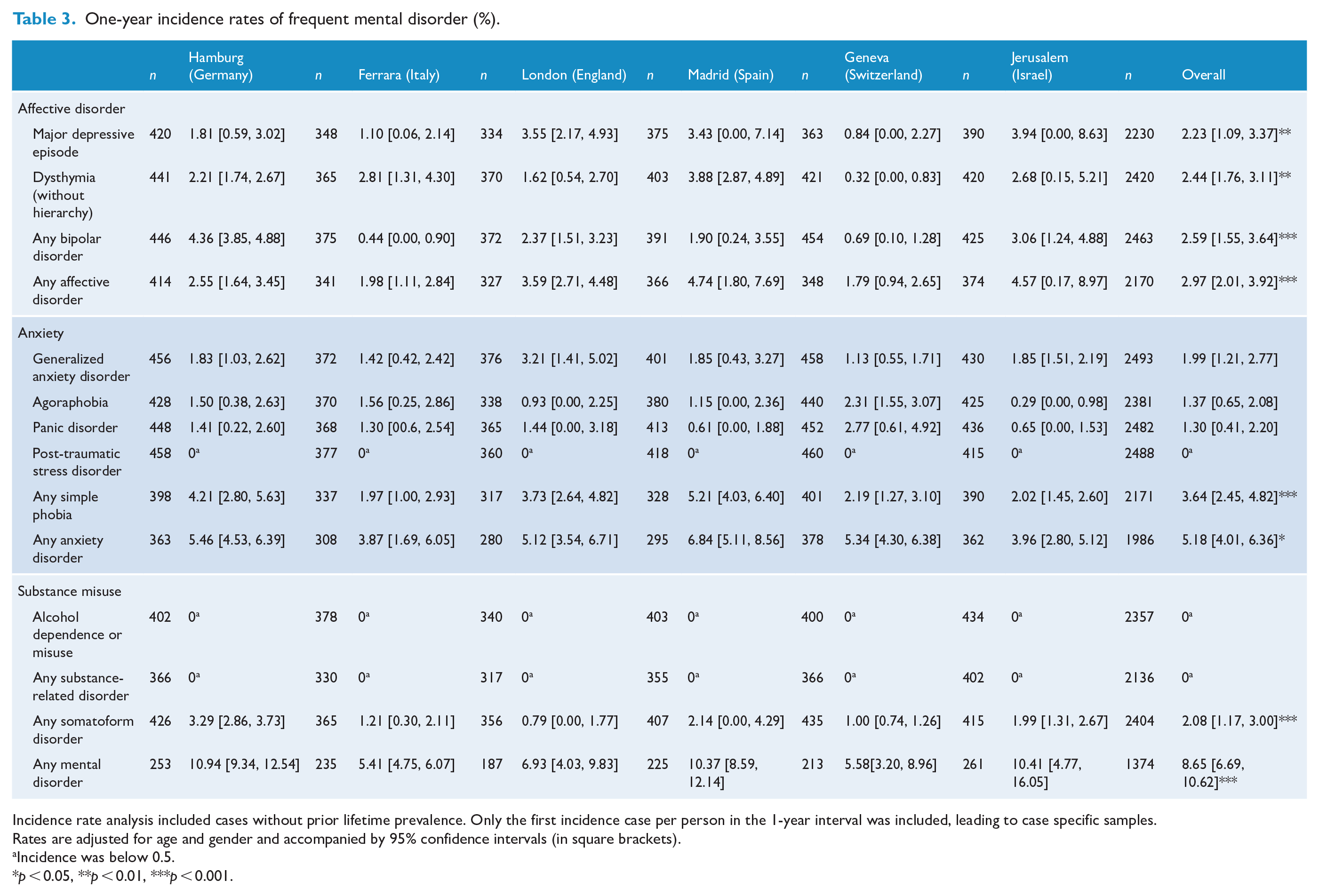
Incidence rate analysis included cases without prior lifetime prevalence. Only the first incidence case per person in the 1-year interval was included, leading to case specific samples.
Rates are adjusted for age and gender and accompanied by 95% confidence intervals (in square brackets).
Incidence was below 0.5.
p < 0.05, **p < 0.01, ***p < 0.001.
We found an incidence rate for any mental disorder of 8.65% in our sample. The highest incidence rate was found for any anxiety disorder (5.18%), wherein any simple phobia (covering animal type, natural environment type, blood-injection-injury type, situational type and other type phobia) was the most frequent anxiety disorder (3.64%). The incidence rates for any affective disorders were 2.97%, 2.23% for major depressive episodes, 2.44% for dysthymia and 2.59% for any bipolar disorder. Lower incidence rates were found for agoraphobia, generalized anxiety disorder, panic disorder and somatoform disorder. The incidence rates for substance-related disorders and post-traumatic stress disorder (PTSD) were below 0.5%. Moreover, we found a significant gender effect for affective disorders, in particular for dysthymic disorder and major depressive episode. Therefore, the incidence rates for females were more than twice as high as those for males. Furthermore, we found a significant age effect for any affective disorder and major depressive episode. Incidence rates also varied across study centres: overall, the highest incidence rate for any mental disorder was found in Hamburg (10.94%; 95% confidence interval [CI]: [9.34, 12.54]), and a much lower rate was found in Ferrara (5.41%; 95% CI: [4.75-6.07]). High incidence rates of affective disorders were found in Madrid (4.74%; 95% CI: [1.80, 7.69]) and Jerusalem (4.57%; 95% CI: [0.17, 8.97]), and high rates for anxiety disorders were found in Madrid (6.84%; 95% CI: [5.11, 8.56]) and Hamburg (5.46%; 95% CI: [4.53, 6.39]) (see Table 3). Combining incidence rates with recurrence rates resulted in slightly higher rates (rate for any mental disorder: 10.47%; see also online supplement). Rates were higher if the analysis included cases that already had one of the cumulated diagnoses in wave 1. The incidence rate for any mental disorder would thus be calculated at 11.42% and the combined rate of incidence and recurrence at 13.19%.
Risk factors of the 1-year incidence of any mental disorder in the elderly
The risk for developing any mental illness after 1 year was almost four times higher if the person was widowed at the follow-up (OR = 4.74; 95% CI: [1.46, 15.40]) and almost two times higher if the person had never been married (OR = 2.18; 95% CI: [1.15, 4.11]) and rated their religious affiliation as not very important (OR = 1.66; 95% CI: [1.19, 2.31]). We found a small but significant effect for developing any mental disorder at the follow-up for number of physical illnesses (OR = 1.15; 95% CI: [1.03, 1.29]) and quality of life (OR = 0.99; 95% CI: [0.98, 1.00]). The ORs of significant predictors included in the final model are displayed in the online supplement.
Discussion
Incidence rates of mental disorders
The primary objective of this study was to assess the 1-year incidence rate of frequent mental disorders across six different European and associated countries, including but not limited to depression, as this disorder has been comprehensively examined in the past.
The response rate for our incidence study was 82.5% (n = 2592) at the follow-up interview 1 year after baseline assessment. Due to the 1-year time interval, this response rate is in the upper range compared to prior incident studies on late-life mental disorders (Beekman et al., 2001; Conde-Sala et al., 2019; Harris et al., 2006; Luppa et al., 2012; Newman and Bland, 1998; Pálsson et al., 2001; Préville et al., 2010; Prince et al., 1998; Weyerer et al., 2013). Prior studies also reported similar reasons for non-participation (Beekman et al., 2001; Conde-Sala et al., 2019; Prince et al., 1998).
The overall 1-year incidence rate of 8.65% for any mental disorder in elderly persons across European countries is higher than the overall 1-year incidence rate for the presence of a probable DSM-IV disorder reported by Préville et al. (2010) using a Canadian representative sample of community-dwelling elderly (6.2%, SE = 0.70). At 2.97%, the incidence rate for any affective disorder is in the lower range of reported incidence rates for this mental disorder group in the elderly (Büchtemann et al., 2012; Cole and Dendukuri, 2003; Luppa et al., 2012; Weyerer et al., 2013). The overall incidence of any anxiety disorder was 5.18%, which is higher than the rate reported by Préville et al. (2010), but within the middle range of variation across analogous studies (Wolitzky-Taylor et al., 2010). The scope of studies reporting incidence rates for mental disorders in old age is weighted strongly towards the examination of depression and sometimes anxiety disorders. This is true for studies conducted in Europe as well as in North America and Oceania (Büchtemann et al., 2012; Préville et al., 2010; Trollor et al., 2007). To our knowledge, this is the first study to report 1-year incidence rates for somatoform disorder, bipolar disorder and substance misuse in community-dwelling elderly worldwide.
Risk factors of the 1-year incidence of any mental disorder in the elderly
The secondary objective was to assess relevant risk factors for 1-year incidence of any mental disorder in the elderly. In line with other incidence studies on mental disorders in old age, female gender was a risk factor for 1-year incidence (Beekman et al., 2001; Büchtemann et al., 2012; Cole and Dendukuri, 2003; Conde-Sala et al., 2019; Luppa et al., 2012; Pálsson et al., 2001; Weyerer et al., 2013). Other risk factors that have been previously reported are loneliness and widowhood (Cole and Dendukuri, 2003; Conde-Sala et al., 2019), poor physical health (Cole and Dendukuri, 2003; Harris et al., 2006; Vink et al., 2008; Weyerer et al., 2013), low quality of life (Chang-Quan et al., 2010; Conde-Sala et al., 2019; Luppa et al., 2012; Vink et al., 2008) and symptom severity (Cole and Dendukuri, 2003; Harris et al., 2006). Increasing age seems to be a protective factor, not only for any anxiety disorder as reported by Vink et al. (2008) but also for any simple phobia, any somatoform disorder and any mental disorder. Another previously unreported protective factor was religious affiliation. Explanations for this association must be explored in future research. The risk factors female gender, physical burden and symptom severity were largely identical to risk factors for younger age (Leach et al., 2008; Villamil et al., 2006). Only loneliness and widowhood seem to emerge as more age-specific risk factors.
Limitations, strengths and outlook
This study provides a unique and important database on incidence rates of mental disorders in the elderly in European and associated countries, based on a strong methodical basis thanks to the use of age-sensitive instruments and the sampling size and procedure. An additional strength is the low drop-out rate at the second wave. The findings indicate and support the urgent need to raise awareness of mental health problems in the elderly and to support the adequate availability of mental health services across Europe. All of the results of the MentDis_ICF65+ study present starting points for required structural changes at the level of mental health policy.
An additional inspection regarding the incidence and prevalence rates across the MentDis_ICF65+ study centres shows that the distribution of the occurrence and the risk for the development of a mental disorder in old age vary within and between study centres. For example, the highest prevalence rate was found in the same study centre that also had the lowest incidence rate. Further analyses are necessary for precise interpretations.
As we noted in previous publications (Andreas et al., 2017), this study has some limitations. Slightly different sampling approaches were applied across the study centres, the qualifications and number of interviewers differed, and the generalizability of findings to other countries is limited. We discussed these limitations of the MentDis_ICF65+ study in previous publications (Andreas et al., 2017). In addition, not all follow-up assessments took place, given that participants moved, did not appear, passed away or withdrew informed consent. Thus, the true 1-year incidence rates might be even higher, assuming mental disorders are the reason for absenteeism. In addition, the follow-up assessment in the Italian study centre (Ferrara) was affected by an earthquake during the study period. Our strict inclusion criteria for the analysis of diagnostic groups also had a diminishing impact on incidence rates. We have not recorded all mental disorders. Furthermore, no statement about connections with dementia is possible, and we describe only predictors for ‘any mental disorder’ and not for individual mental disorders. Despite these limitations, the findings remain representative.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211025711 – Supplemental material for Incidence and risk factors of mental disorders in the elderly: The European MentDis_ICF65+ study
Supplemental material, sj-docx-1-anp-10.1177_00048674211025711 for Incidence and risk factors of mental disorders in the elderly: The European MentDis_ICF65+ study by Sylke Andreas, Holger Schulz, Jana Volkert, Jonas Lüdemann, Maria Dehoust, Susanne Sehner, Anna Suling, Karl Wegscheider, Berta Ausín, Alessandra Canuto, Michael J Crawford, Chiara Da Ronch, Luigi Grassi, Yael Hershkovitz, Manuel Muñoz, Alan Quirk, Ora Rotenstein, Ana Belén Santos-Olmo, Arieh Shalev, Kerstin Weber, Hans-Ulrich Wittchen and Martin Härter in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The study was approved by research ethics committees in all six countries (Germany: Hamburg Ethics committee of the Medical Association No. 2895, Italy: Ferrara No. 0096637 5/11/2009, Israel: Jerusalem No. 0376-09-HMO, Spain: Madrid No. 22032010, Switzerland: University Hospitals of Geneva ethics committee, Protocol No 09-121 and UK: National Research Ethics Service No. 10/H0715/21).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by a grant from the European Commission within the 7th Framework Research Program of the EU (grant number 223105).
Research data
The clinical data were collected and analysed under consideration of privacy guidelines after all participants had given written informed consent and will be treated strictly confidential according to this condition. Consequently, data are available on request from the lead author only (S.A.).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.