
Abstract
Much has been made of the implications of ageing on the impact of common neuropsychiatric disorders such as the dementias [1]. The rapid rise in the elderly population may have implications for other common psychiatric disorders such as the affective and anxiety disorders, but national surveys that include older individuals are uncommon. The first such major survey, the Epidemiological Catchment Area Study [2], showed a decline in prevalence of mental disorders in the elderly. These data began a debate that has continued for two decades. The debate can be simplified into two mutually exclusive propositions: there are those who consider that there is an age-dependent decline in mental disorder [3–6], and those who view the reported reduction in mental disorder with age as an artefact [7–9]. The Australian National Mental Health and Well-being Survey (NMHWS) is a unique resource because it is the only population-based survey that included a broad range of older individuals. Our previously published NMHWS data showed that those individuals aged ≥65 years were at lower risk of mental disorder compared with those aged 18–24 years [10]. These data have been mirrored in the recent publication of the results from the New Zealand Mental Health Survey (NZMHS), which showed an age-dependent decline in prevalence of mental disorders as a whole and for diagnosis of any anxiety or mood disorder [11]. However, detailed analysis pertaining to the elderly was not undertaken in either NMHWS or NZMHS and the particular demographic correlates of mental disorder in the elderly were not explored. In revisiting the NMHWS data, we set out to perform a comparison between community-dwelling middle-aged and elderly participants. We aimed to determine whether the prevalence rates for mental disorder differed between these groups after controlling for cognitive impairment. Furthermore, we sought to discern the predictors of mental disorder unique to the elderly while controlling for the potential confounding influence of other variables.
Methods
The Australian NMHWS was conducted in 1997 by the Australian Bureau of Statistics (ABS). Detailed methodology has been published elsewhere [10]. A national probability sample of private dwellings was obtained from urban and rural areas across Australia. A total of 13 624 dwellings were selected, from which one adult member aged ≥18 years was randomly selected as the possible respondent. After refusals (n = 1477), non-contact with respondent (n = 558) and dropouts due to inability to communicate, death, illness in the household, or premature termination of interview (n = 948), there was a total of 10 641 respondents. Of these, 3111 respondents were aged between 45 and 64 years of age and 1792 respondents were aged ≥65 years. Individuals in hospitals, nursing homes, or jails were not approached for participation in the survey.
The Composite International Diagnostic Interview (CIDI) version 2.1 [12, 13] was administered by trained ABS personnel to determine the presence of reported symptoms of a number of mental disorders, using ICD-10 [14] and DSM-IV diagnostic criteria. We examined the CIDI items for three ICD-10 affective disorders (major depression, dysthymia, bipolar disorder) and six ICD-10 anxiety disorders (panic disorder, agoraphobia, social phobia, generalised anxiety disorder, post-traumatic stress disorder, obsessive–compulsive disorder). The presence of cognitive impairment was examined using the Mini-Mental State Examination (MMSE) [15]. Psychological distress was measured using the Kessler Psychological Distress Scale (K10) [16]. The prevalence of health consultations and the use of medications for mental health problems were also assessed. Survey respondents reported if they had consulted with any health professional for a mental health problem in the past 12 months. Those who had consulted were then asked to provide information regarding what type of intervention they received, including medication.
Data analysis
Routine data analysis procedures were conducted using the SUDAAN software package [17]. Due to the complex sample design of the NMHWS, special software was required to estimate standard errors (SE). The SE of estimated prevalence rates and confidence intervals around odds ratios (ORs; derived from logistic regression models) were estimated using delete-one jackknife repeated replication in 30 design-based subsamples [18].
All prevalence data reported are weighted to reflect the age and sex stratification of the Australian population (as estimated by the 1996 census data) and to control for the probability of being sampled. In order to examine for statistically significant differences in prevalence rates for mental disorders and number of health consultations we adopted χ2 analysis. A comparison of psychological distress was made using a t-test to compare the mean scores on the K10 in each group. Logistic regressions were used to calculate the adjusted ORs and examine the association between affective/anxious mental disorders (criterion variable) and sociodemographic factors (independent variables). The multivariate approach ensures that the contribution of each independent variable is calculated while controlling for the other independent variables. Each model examined the effects of sex, age, marital status, education, employment, and presence of physical disorder (and interactions between these variables) in either the middle-aged group, elderly group, or all participants aged >45 years. All models were run using the RLOGIST command in SUDAAN [17].
In anticipation that cognitive impairment associated with ageing may compromise the validity of reports of symptoms of mental disorder, health consultations and medication use, all analyses were initially run excluding data from elderly participants who scored <24 points on the MMSE (n = 141). In order to ensure that exclusion of these individuals did not bias the results, we re-ran all analyses while including the data from participants with low MMSE. This reanalysis confirmed that the pattern of the results was the same whether participants with low MMSE were included in the analyses or not. The tables presented throughout this article reflect the statistics generated while excluding participants with low MMSE.
Results
Response rates
The response rate for the survey as a whole was 78.1%. Data relating to response rates by age was not available from the ABS for this survey.
Sociodemographic characteristics
The sociodemographic characteristics of all middle-aged and elderly participants are shown in Table 1. Because age bands were not available for individuals >75 years of age, these individuals were grouped together. The slight excess of women in the elderly cohort reflected the sex distribution in the population. The household composition and employment status reflect the transition to retirement, relinquishing of care for younger dependents and past loss or separation from spouse in the elderly group.
Demographic characteristics of the NMHWS participants
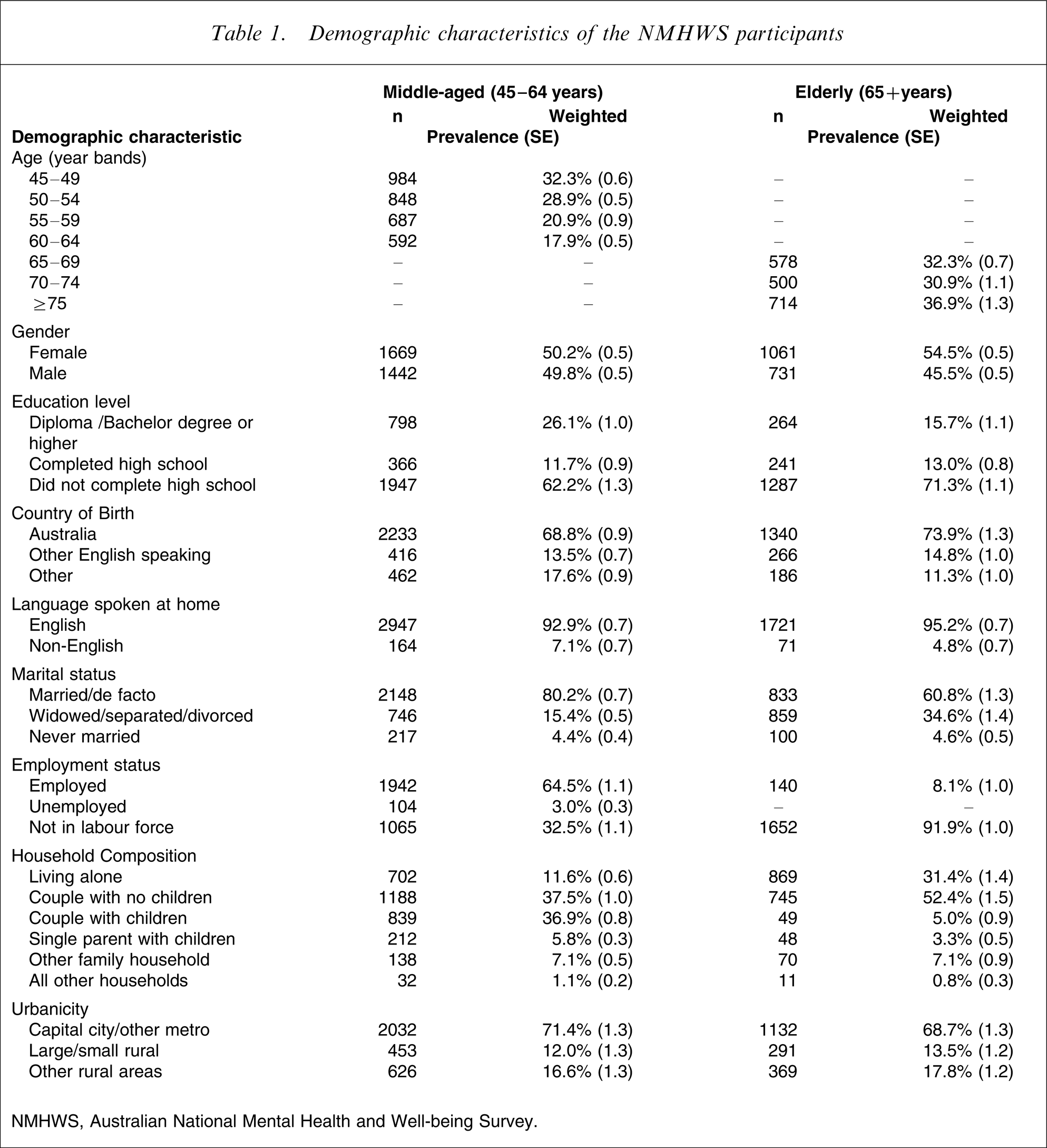
NMHWS, Australian National Mental Health and Well-being Survey.
Prevalence of psychiatric disorders
The 12 month prevalence for ICD-10 affective and anxiety disorders in the middle-aged and the elderly groups were compared (Table 2). Elderly participants were less likely to report symptoms consistent with any ICD-10 affective or anxiety disorder in the preceding 12 months (OR = 0.4, χ2=40.0, p < 0.001). Elderly participants were less likely to report symptoms consistent with any affective disorder (OR = 0.3, χ2=41.2, p < 0.001). Elderly participants were less likely than those in middle age to report symptoms consistent with any anxiety disorder (OR = 0.3, χ2=29.3, p < 0.001). The differences in the individual disorders were also significant, except for bipolar and obsessive–compulsive disorder, for which the numbers were very small.
Comparison of population prevalence of ICD-10 affective and anxiety disorders
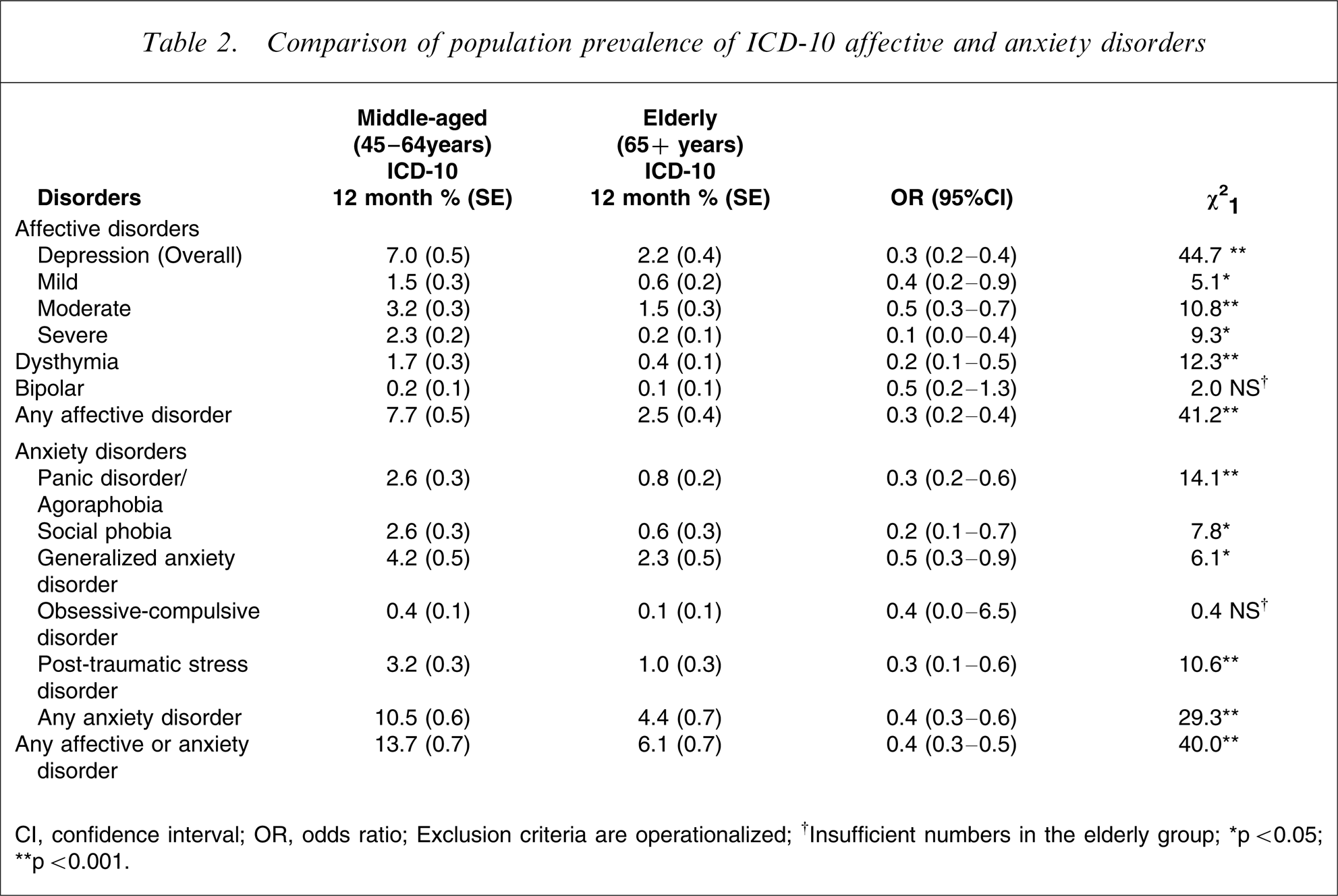
CI, confidence interval; OR, odds ratio
Exclusion criteria are operationalized.
†Insufficient numbers in the elderly group
∗p < 0.05; ∗∗p < 0.001.
Psychological distress, consultation rates and medication use
Elderly participants had lower levels of psychological distress as measured by the K10 (mean score = 13.3, SE = 0.1) compared with middle-aged participants (mean score = 14.1, SE = 0.1) and this difference was statistically significant (t (30) = 5, p < 0.001). Elderly participants were less likely to report having seen any health professional for a mental health problem in the past 12 months (weighted prevalence = 28.8%, SE = 4.6) compared to those in middle age (weighted prevalence = 39.9%, SE = 2.3), the difference being statistically significance (OR = 0.4, χ2=29.2, p < 0.001). Among those who reported receiving help for a mental health problem, medication was prescribed more often in the elderly (75.9%, SE = 5.7) compared with middle-aged participants (61.9%, SE = 2.7). This difference, however, was not statistically significant (OR = 1.9, χ2=3.5, p > 0.05).
Correlates of mental disorders
In the NMHWS demographic factors (sex, marital status, education, employment status and presence of a physical disorder) were correlates of mental disorder [10]. To explore whether these differed in the two age groups, logistic regression modelling was performed and is presented in Table 3 as multivariate ORs and corresponding χ2 estimates.
Demographic correlates of any 12 month ICD-10 affective or anxiety disorders for the middle-aged group (45–64 years; n = 3111) and the elderly group (65+ years; n = 1792)
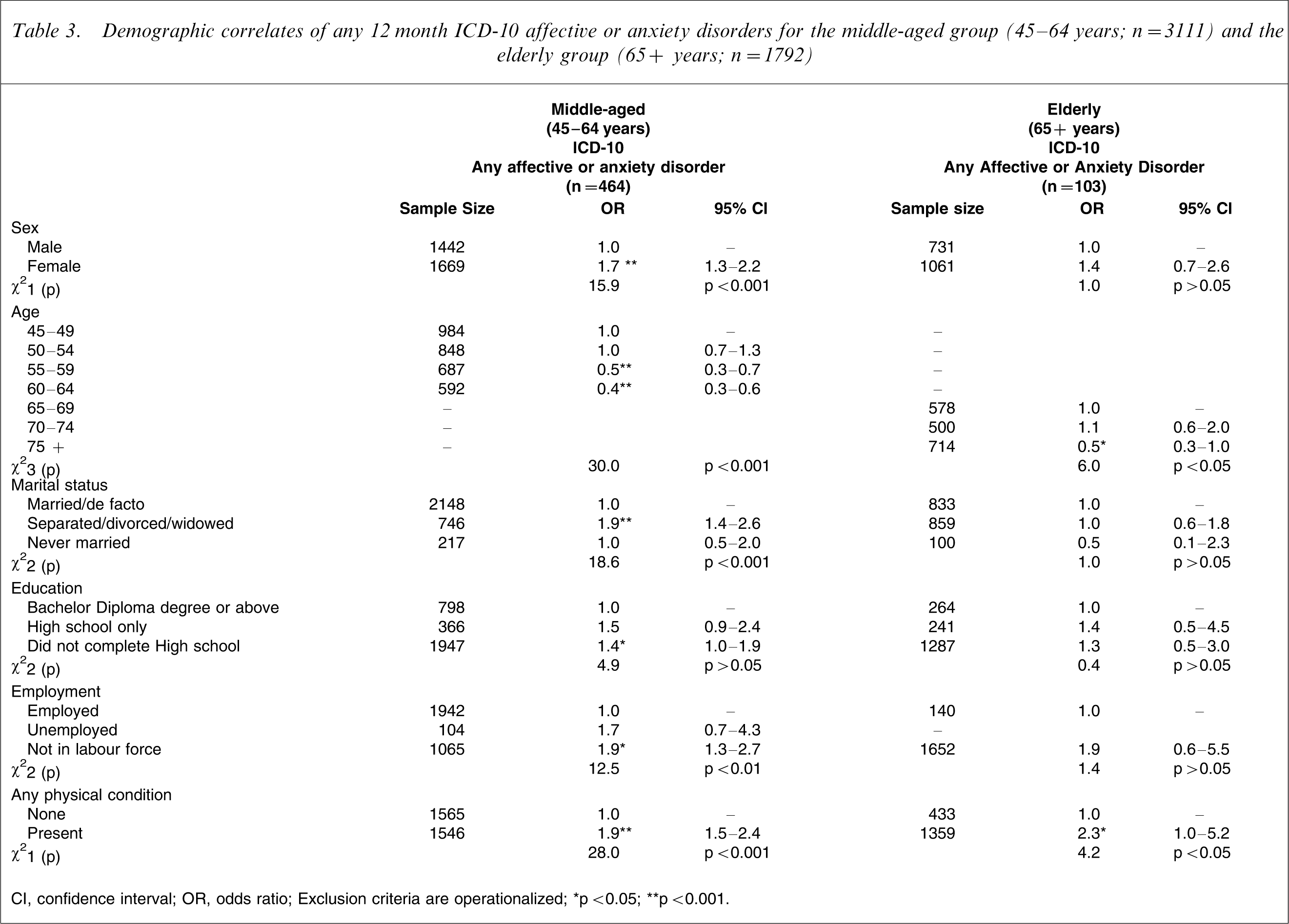
CI, confidence interval; OR, odds ratio.
Exclusion criteria are operationalized.
∗p < 0.05; ∗∗p < 0.001.
The impact of the sociodemographic variables on mental disorders for the middle-aged participants was similar to that published for the survey as a whole [10]. However, few of these demographic predictors were significant in the elderly participants. Detailed results are as follows.
Sex
For middle-aged participants, but not for elderly participants, being female emerged as a significant predictor of the presence of any affective or anxiety disorder. The groups differed significantly.
Age
Age emerged as a significant predictor of the presence of mental disorder, with increasing age being associated with lower likelihood of having experienced symptoms of an anxiety or affective disorder in the preceding 12 months in both middle-aged and elderly participants. For example, compared to the youngest age band (45–49 years) within the middle-aged group, a significant reduction in risk was apparent for those aged 55–59 years (OR = 0.5, p < 0.001) and for those aged 60–64 years (OR = 0.4, p < 0.001). With regard to the elderly, Table 3 shows that those over the age of 75 had a reduced risk of mental disorder (OR = 0.5, p < 0.05) compared to the youngest age-band (65–69 years) within that group. The overall pattern supported an age-dependent decline in risk for mental disorder.
Marital status
Marital status emerged as a significant predictor of mental disorder in the middle-aged group only. Those middle-aged participants who had experienced separation, divorce or death of a partner were significantly more likely to have experienced mental disorder in the preceding 12 months (OR = 1.9, p < 0.001). The age groups differed in this regard.
Education and employment
Education was not a significant predictor of mental disorder in either group. Employment status was a significant overall predictor of mental disorder for the middle-aged only. For this group, those out of the labour force were significantly more likely than employed individuals to have experienced mental disorder in the preceding 12 months (OR = 1.9, p < 0.05). In the elderly group employment was not related to mental health. The age groups differed in this regard.
Physical health
Self-reported presence of a physical disorder was significantly associated with the presence of mental disorder for both middle-aged and elderly groups.
In order to examine the interaction between age and other demographic variables, we re-ran the regressions in the sample (age ≥45 years) as a whole, entering interactions between age and each of sex, marital status, education, employment and physical disorder, while controlling for the presence of all the other independent variables. The only significant interaction between age and any other independent variable was that with marital status (χ2=11.2, p < 0.01). Examination of ORs showed that age was protective against mental disorder irrespective of marital status. Compared to elderly married or de facto participants, those in middle age were more likely to experience a mental disorder (OR = 2.8, 95% confidence interval [CI] = 1.9–4.2, p < 0.001); compared to elderly separated, divorced or widowed participants, those in middle age were more likely to experience a mental disorder (OR = 6.2, 95%CI = 4.2–9.2, p < 0.001); and compared to elderly never-married participants those in middle age were more likely to experience a mental disorder (OR = 7.3, 95%CI = 1.6–33.2, p < 0.05). A key difference emerged between groups in the way in which being separated, divorced or widowed influenced the prevalence of mental disorder. Compared to middle-aged participants who were married, those who were separated, divorced or widowed were significantly more likely to experience mental disorder (OR = 1.8, 95%CI = 1.3–2.4, p < 0.05). There was no such effect in the elderly group (OR = 1.2, 95%CI = 0.7–2.0, p > 0.05).
Discussion
We present the first detailed comparison of rates of mental disorder between middle-aged and elderly groups from a population-based survey. The 12 month prevalence of ICD-10 affective disorders in individuals aged ≥65 years was substantially below the rate for those aged 45–64 years (2.5% vs 7.7%). A similar pattern was observed for 12 month prevalence of ‘any anxiety disorder’ (4.4% vs 10.5%). The present data therefore support the notion that community-dwelling individuals >65 years of age have lower rates of affective and anxiety disorders compared to those in middle age. These data are consistent with those from the NZMHS, which demonstrated a highly significant effect of age on prevalence of mental disorder as a whole, and comparable rates for DSM-IV diagnosis of any mood disorder in individuals aged ≥65 years (2.0%) and those aged 45–64 years (6.8%) [10]. The rates for DSM-IV diagnosis of any anxiety disorder in the NZMHS demonstrated a similar age-dependent decline but were higher than those from NMHWS, most likely due to exclusion of the diagnosis of simple phobia and the use of ICD-10 criteria in the latter.
Whether population-based surveys accurately determine rates of mental disorders in the elderly has been a source of heated debate between clinicians and epidemiologists [4, 5, 9, 19, 20]. Several key criticisms of such surveys have been forthcoming. The first concerns sampling error [19, 21]. It has been proposed that unwell and unwilling elderly individuals may be under-sampled, artificially lowering the ascertainment of cases. Data relating to this phenomenon are almost impossible to obtain from population surveys because nothing is known of those individuals who fail to respond to an invitation to participate. Although data were not available for response rates by age in NMHWS, response rates have been documented in other similar ABS surveys. For example in the 2001 compulsory National Health survey participation rates among elderly individuals exceeded those of the middle-aged individuals (response rates 97.8% for age 45–54 years, 97.9% for age 55–64 years, 99.0% for age 65–74 years, 99.3% for age 75–84 years and 98.0% for subjects >85 years of age) (ABS: National Health Survey, unpublished data, 2001). This would suggest that unwell elderly individuals living in the community in Australia are not likely to be underrepresented in the NMHWS data.
Another criticism of population surveys is that they underestimate the prevalence of mental disorder in the aged by failing to take into account the high burden of mental disorder in age-specific residential care settings. We believe that the impact of non-inclusion of the institutionalised elderly on prevalence rates of mental disorder has been overstated. In Australia in 2001, only 2.0% of the population >65 years resided in a nursing home and a further 1.6% resided in other age-specific cared accommodation [22]. Although the proportion of those in residential aged care facilities increases dramatically as a function of age, this is offset by the dramatic decrease in the proportion of the elderly population accounted for by the oldest old. Therefore it is unlikely that exclusion of the institutionalised elderly would have a significant impact on the overall prevalence of mental disorders in the over-65 age group. To explore this issue further, we used our data and those published previously [23, 24] to extrapolate the influence of inclusion of residential aged care facilities on the prevalence of major depression in those over 65 years of age in Australia. For consistency with those within nursing homes, we reassessed our data without exclusion of those with lower MMSE scores. Using age-stratified data from the 2001 ABS Population Census [22] pertaining to the number of individuals in all residential aged care facilities and assuming a prevalence of major depression of 10% within those facilities [23, 24], we projected that the overall prevalence rate for major depression in those aged ≥65 years would increase negligibly from 2.2% to 2.5% on inclusion of residential aged care facilities. For those >75 years of age our calculations indicated a projected increase in the prevalence rate of major depression from 0.8% to 1.5%. These rates were well below the prevalence estimates for major depression in the middle-aged sample (7.0%).
There has hitherto been a one-sided debate relating to factors that may artificially lower prevalence rates of mental disorder in the elderly. We propose that the opposite phenomenon may also be at play, in that well individuals may be unavailable to participate in such surveys. Courtesy of good health some individuals may be enjoying a rich but nomadic lifestyle in retirement, thus escaping inclusion in population surveys. To evaluate this issue, we obtained customised data from the ABS 2001 Population Census (ABS: Population Census, unpublished data, 2001) relating to those individuals who on Census night were enumerated out of their statistical local area and who were aged 45–64 years and ≥65 years. Because we were interested in those individuals whose travel outside their local area may have related to favourable circumstances, we excluded those individuals who were institutionalised (e.g. those in age-specific cared accommodation, hospitals, gaols etc.), and expressed those remaining as a percentage of the total number in that age range. Congruent with the notion that active enjoyment of life through travel outside of one's residential area is a phenomenon seen in lives of healthy older Australians, we found that slightly more individuals in the age group ≥65 years were assessed as being remote to their statistical local area (4.5%) compared with individuals in the 45–64 year age group (4.26%). The unavailability of the elderly for the purposes of population surveys may have in fact created a small elevation of prevalence rates for mental disorder reported in the NMHWS.
The discordant pattern of demographic correlates for middle-aged and elderly individuals suggests that the determinants of mental disorder in these populations may be dissimilar. Some of these differences, such as employment status, may relate to life-stage issues and role. But because the sample size in the elderly group was relatively small, the possibility of a type II error was considered. As a second possibility, we considered that the difference may be real and explained by the interaction between age and other demographic variables. Secondary regression analysis demonstrated a significant interaction between age and marital status, but not with other demographic variables. These data suggest that loss experiences such as divorce, separation or death of a partner have greater impact on the presence of mental disorder in the middle-aged. While divorce or separation would be more common in middle age, death of a partner is more likely in later life. From our data it is uncertain whether each specific loss experience is associated with different propensity to mental illness. Loss of a partner in middle age may well be poorly anticipated, less easily assimilated and more likely to be a trigger for mental disorder. In comparison, loss and particularly death of a loved one is often considered an inevitable albeit painful consequence of growing old.
A third criticism of population surveys relates to the applicability of the diagnostic instruments in older persons. This arises from two key propositions: (i) the possible differential expression of depression as somatic complaints in the elderly [25] so that some instruments underestimate prevalence; and (ii) the default attribution of somatic symptoms to physical rather than psychiatric disorder, leading to a potential underreporting in the elderly. Owing to time constraints, population surveys are unlikely to include comparison diagnostic instruments in order to test the first proposition. Whether there is a robust qualitative difference in the nature of depression in the elderly [7] remains to be convincingly proven. Our finding of a reduced prevalence of mental disorder in the elderly could arguably relate to such a difference. However, the additional finding of reduced psychological distress in the elderly suggests that the reduced prevalence figures represent a true decline rather than differential expression or attribution of symptoms. Furthermore, our data confirm a clear relationship between the presence of a physical disorder and mental disorder in both the middle-aged and the elderly, but there was no interaction between physical disorder and age. This implies that the relationship between mental disorder and physical conditions is equally pertinent in both middle-aged and elderly groups, dispelling physical disorder as a particular source of bias in the elderly.
The paucity of demographic correlates of mental disorder in the elderly in our data suggests that we must explore further to understand mental disorder in later life. Henderson et al. have proposed that exposure to adverse experiences gradually creates resistance to the psychological effects of such experiences (so-called psychological immunisation), which becomes apparent in old age [4]. An age-dependent reduction in neuroticism has been proposed by Jorm to assist in understanding the reduction in prevalence in later life [5]. Both these factors are compatible with the present observed poverty of association with traditional life stressors. The present data are also compatible with the notion that the natural history of mental disorder in the community-dwelling elderly is one of remission with time. Clearly, until longitudinal data are available, this proposition remains speculative. A final possibility is of differential attrition so that those with mental disorders have a higher mortality [26] and are therefore underrepresented in the elderly.
The world mental health surveys have included elderly individuals [27]. We await detailed analysis of these surveys with interest. The data presented here highlight some important issues for population surveys. First, the present data underscore the importance of sampling across the lifespan, an omission that is a major shortcoming of many surveys and which should be corrected. Detailed information from these surveys relating to correlates of mental disorders in the community-dwelling elderly is virtually non-existent. Inclusion of large numbers of elderly individuals in population surveys is necessary because the prevalence of mental disorder is lower than in other age groups, complicating statistical analysis. This is seen as a necessary step in teasing out the similarities and differences in mental disorders in different stages of life. The issue of whether an age-sensitive bias in either the diagnostic instrument or diagnostic criteria exists is not likely to be addressed in future population studies because to do so requires the application of several parallel instruments in order to test whether the elderly endorse different symptoms of depression or other mental disorder.
The present data support the notion that the community-dwelling elderly enjoy a relative absence of affective and anxiety disorder in comparison to their middle-aged counterparts. We have argued that the lower prevalence of mental disorder in the community-dwelling elderly appears unlikely to be accounted for by sample bias. The differential pattern of demographic correlates of mental disorder in the middle-aged and the elderly suggests that either psychological response to adversity differs between the groups or that other factors hitherto unmeasured are more relevant in determining rates of mental disorder in older individuals.
Footnotes
Acknowledgements
This paper was supported by NHMRC programme grant no. 350833.