
Abstract
Objectives:
Effective prevention and intervention of Internet gaming disorder require the identification of risk and protective factors. This study aims to exhaustively review the risk and protective factors of Internet gaming disorder among Chinese people.
Method:
We searched for articles published from database inception to February 2020 in MEDLINE, PsycINFO, Embase, PubMed, Web of Science and two Chinese databases, CNKI and Wanfang Data. Studies were included in the meta-analysis if they addressed Internet gaming disorder, sampled people in China, presented correlational factors of Internet gaming disorder and reported the effect sizes for correlations. Reviewers independently selected the studies, assessed their validity and extracted the data. Pooled Pearson’s correlations were calculated using the random effects model.
Result:
In the meta-analysis, 153 studies covering 115,975 subjects were included. We identified 56 risk factors and 28 protective factors. Most risk factors strongly correlated with Internet gaming disorder fell into the category of maladaptive cognitions and motivations. Other factors that showed high effect sizes fell into various categories, including psychopathological characteristics, personality traits, cognition emotion regulation style and gaming-related factors. The only protective factor strongly correlated with Internet gaming disorder was self-control. We found that the factors related to the ‘environments’ show modest effect sizes compared to those related to the individual. The pooled effect sizes for most factors were not influenced by outliers and publication bias.
Conclusion:
Factors strongly correlated with Internet gaming disorder, especially maladaptive cognitions and motivations, are more likely to be proximal correlates of Internet gaming disorder and may be considered the focus of interventions. We encourage further empirical and experimental studies to examine the causal pathway and the treatment efficacy.
Keywords
Introduction
Video gaming is now an immensely popular entertainment form in the world. But with the development of Internet technologies and the video game industry, societies need to confront the challenge of individuals who ignore reality and are heavily immersed in the virtual gaming world. In 2013, the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) introduced Internet gaming disorder (IGD) and stated it requires ‘deep further studies’ (American Psychiatric Association, 2013). It was defined as the persistent and recurrent use of the Internet for gaming (often with other players) that leads to clinically significant impairment or distress, with nine proposed criteria for diagnosis: preoccupation, withdrawal, tolerance, unsuccessful attempts to control, loss of interest, continued despite problems, deception, escape and functional impairment (American Psychiatric Association, 2013). In 2018, gaming disorder was included in the 11th edition of the International Classification of Diseases (ICD-11) (World Health Organization, 2018). The definitions of IGD and gaming disorder are similar in many ways.
Many controversies about IGD still persist. First is the appropriateness of using the interpretive framework of substance use disorders and gambling disorder to understand problematic gaming. IGD was constructed as a non-substance behavioural addiction in DSM-5 (Petry and O’Brien, 2013). The proposed criteria of IGD were ‘chosen and worded to parallel some substance use and gambling disorder criteria’ (Petry et al., 2014). Some scholars challenged the conceptualisation of IGD as behaviour addiction. For example, Starcevic (2016) argued that the addiction framework is only one approach to behavioural disturbances like problematic gaming, and the framework of impulsive control disorders is another approach. Billieux et al. (2015) argued if the atheoretical and confirmatory approach is used (three steps: the behaviour is a priori considered addictive based on anecdotal observations, substance abuse criteria are used to develop assessment tools and risk factors are determined), an unlimited list of ‘new’ behavioural addictions would be identified. Moreover, some scholars concerned constructing IGD as an ‘addiction’ might pathologise normal gaming behaviour and stigmatise people who highly engaged in games (Aarseth et al., 2017; Zastrow, 2017).
However, there is increasing evidence to explore the neurobiological homology of IGD with substance abuse. IGD and substance addiction share in the following neurobiological aspects: the impaired prefrontal cortex functions in particular executive control function, the stimulation of mesolimbic dopamine system by cues, the deficiency in the overall neuronal reward system and the more inferior decision-making capabilities weighing the pros and cons of addictive behaviour (Brand et al., 2014; Dong and Potenza, 2014; Hellman et al., 2013; Kuss et al., 2018; Kuss and Griffiths, 2012). Therefore, the evidence may provide a biological base to support the justification of conceptualising IGD as a behavioural addiction.
Corresponding to the conceptualisation, the validity and wording of IGD criteria in DSM-5 were also contentious (Griffiths et al., 2016). Some studies assessed the validity of these criteria using clinician’s diagnosis as reference; criteria like ‘escape’ and ‘deception’ did not show adequate diagnostic accuracy. At the same time, most criteria showed acceptable to good diagnostic accuracy (Ko et al., 2014; Müller et al., 2019).
Second is the heterogeneity of the IGD measurements. There have been numerous instruments to assess IGD. The instruments developed before the publication of DSM-5 paralleled substance use disorder criteria, pathological gambling criteria, impulse control or other criteria (Petry and O’Brien, 2013). King et al. (2013b) reviewed 18 instruments developed to assess pathological gaming by that time. The instruments showed excellent internal consistency and convergent validity but were inconsistent in the coverage of core addiction indicators. After 2013, several new instruments have been constructed according to the proposed IGD criteria of DSM-5 (Kiraly et al., 2017; Lemmens et al., 2015; Pontes et al., 2014; Pontes and Griffiths, 2015). But until now, there has been no broad consensus on a unified approach to assessing IGD.
The third controversy is the advantages and disadvantages of including gaming disorder as an official condition in ICD-11. Some scholars believed the formalisation of this disorder would have negative medical, scientific, public health, social and human rights consequences due to the inappropriate operationalisation of IGD and lack of consensus towards symptomology and measurement (Aarseth et al., 2017). In contrast, some scholars argued gaming disorder consisted of less controversial criteria, and the formalisation of this disorder would help to clarify and popularise the difference between healthy game enthusiasm and gaming disorder, thus reducing the stigmatisation (Király and Demetrovics, 2017).
In conclusion, these controversies indicate a lack of a consensus about the conceptualization and assessment of IGD. Therefore, there is a need to conduct a review that can systematically examine and clarify the controversies surrounding the concept and measurement of IGD. Despite the controversies, IGD has emerged as a severe mental health issue. A meta-analysis reported a pooled prevalence of 3.1% among youth and young adults (Ferguson et al., 2011). Another meta-analysis reported a higher prevalence of 4.6% among adolescents (Fam, 2018). Moreover, the prevalence of IGD seems to be highest among people in Asian countries (American Psychiatric Association, 2013).
It is worth noting that IGD may lead to severe heath, psychological and social consequences. IGD can cause school failure, job loss or marriage failure due to excessive and compulsive gaming behaviours that interfere with regular school, vocational and social activities (American Psychiatric Association, 2013). In addition, much evidence indicates that IGD can cause harmful psychological and behavioural consequences, including depression, anxiety, social phobia, substance abuse and aggressive behaviours (Anderson et al., 2010; Mihara and Higuchi, 2017). IGD may also induce neurological impairments. IGD patients can have structural neural alterations, lower working memory and decision-making capabilities, decreased visual and auditory functioning and cognitive functional constriction in various domains (Kuss et al., 2018; Kuss and Griffiths, 2012; Yao et al., 2017).
Therefore, developing effective strategies to prevent and intervene in IGD is urgently needed. Moreover, it is necessary to develop a theoretical model that comprehensively includes risk and protective factors, mediating processes and pathological behaviours to conceptualise IGD prevention and intervention (Koo and Kwon, 2014). Potentially malleable risk factors, as well as protective factors that may reduce the risk, should be the central focus of intervention (Fraser et al., 2009).
The researchers identified risk and protective factors for mental illness in both cross-sectional and longitudinal studies (Cairns et al., 2014; Davies et al., 2020; Dowling et al., 2017). For the cross-sectional studies, risk factors were defined as conditions associated with a higher chance of negative outcomes (problem behaviour), and protective factors were conditions that decrease the probability of engaging in problem behaviour (Deković, 1999). For the longitudinal studies, risk (protective) factors were conceptualised as antecedent conditions that precede and are associated with a higher (lower) chance of negative outcomes (Kraemer et al., 1997). The advantage of this definition is that the contaminants and consequences can be excluded from the identification of risk and protective factors.
In the field of IGD, not too many longitudinal studies identified the risk and protective factors. It has been reported that people with aggression, social withdrawal, depression, anxiety and attention deficit hyperactivity disorder (ADHD) are more likely to immerse in online gaming (Cho et al., 2013; Ha et al., 2007; Ko et al., 2007, 2009a, 2009b; Young and Rogers, 1998). Certain types of personality also play a role in the development of IGD. People with high impulsivity, psychoticism, identity problem and low self-esteem are more likely to become pathological gamers (Dong et al., 2013; Gentile et al., 2011; Niemz et al., 2005; Stieger and Burger, 2010). By contrast, behavioural control over gaming and high-level social competence prevent people from developing IGD (Gentile, 2009; Lemmens et al., 2011).
Several environmental factors have also been explored. The conflict between the parent and the child and not living with the mother have been identified as risk factors of IGD (Ko et al., 2009a; van Den Eijnden et al., 2008). Conversely, quality communication between parents and children, social integration, school-related well-being and teacher autonomy support are protective factors (Haagsma et al., 2013; Jia et al., 2009; Rehbein and Baier, 2013; van Den Eijnden et al., 2010). Furthermore, much time spent on gaming, positive attitude towards gaming and the intention to play games predict a greater tendency to develop IGD (Gentile, 2009; Haagsma et al., 2013; King et al., 2013a; Mihara and Higuchi, 2017). At the same time, there are many more cross-sectional studies of IGD than longitudinal studies.
Although the previous studies have explored many risk and protective factors of IGD, we have identified two significant gaps. First, a lack of study that exhaustively reviews the risk and protective factors of IGD has made it difficult to compile a comprehensive list of them. This is not conducive to a thorough understanding of IGD. Second, the magnitude of the association between those factors and IGD is unexplored. It is therefore difficult to determine the central focus of the prevention of and intervention in IGD. The two gaps can be bridged by systematic review and meta-analysis.
Very few studies have systematically reviewed the risk and protective factors of IGD. Long et al. (2018) reviewed 21 articles published in Chinese. Mihara and Higuchi (2017) reviewed 28 cross-sectional and 13 longitudinal studies worldwide. Both studies explored risk and protective factors including demographic characteristics (e.g. male gender), game-related factors (e.g. time spent on games), psychological factors (e.g. depression and anxiety) and familial and scholastic factors (e.g. parenting styles). However, because the two studies did not explore the magnitude of those correlations and make quantitative syntheses for comparison, it remained difficult to determine which factors were more critical to IGD development.
In addition, we only found one meta-analysis that compared the magnitude of the correlations. Koo and Kwon (2014) reviewed 41 Korean articles on IGD and synthesised the correlated effect sizes of each factor. They found that intrapersonal factors were more strongly correlated with IGD than interpersonal factors, and that emotion was the strongest risk factor while control/regulation was the strongest protective factor. However, this study is inadequate in certain areas. First, it did not include studies with factors of maladaptive cognitions and motivations, which showed strong correlations in many Chinese studies (Huang et al., 2006; Wang, 2009; Wang et al., 2015; Zhen et al., 2016; Zhong and Yao, 2013; Zhou and Leung, 2012). The study also did not report the pooled effect sizes of the specific correlational factors under each category (e.g. depression under the category of emotion), which might hinder our understanding of the results. And methodologically, the study did not describe the method used to assess the risk of bias in individual studies and across studies. Including biased studies may lead to inappropriate interpretation and render the conclusion misleading. For these reasons, a new meta-analysis that follows a standard guideline is needed to bridge the gaps above.
To conclude, while previous empirical studies and reviews have explored various risk and protective factors of IGD, there is still a lack of qualified studies comparing the magnitude of the correlations between these factors and IGD. Therefore, the objectives of this study are (a) to review the risk and protective correlational factors of IGD and (b) to explore and compare the magnitude of the correlations between these factors and IGD. Considering the limited number of longitudinal studies for IGD and the need to control the bias from research design, we mainly reviewed available studies that had a cross-sectional design in nature. And to minimise cultural bias, we reviewed studies that sampled Chinese people. The problem of IGD in China is worthy of attention. In 2017, the number of online games in China reached 603 million (iResearch Consulting Group, 2018). A survey with a national representative sample reported the prevalence of IGD as 3.2% among adolescents and young adults (Zuo and Ma, 2010). IGD has therefore become a severe mental health issue in China.
Method
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines throughout this review (Moher et al., 2009) (Supporting Information, S1). This review has been registered at PROSPERO under the registration number of CRD42020161251.
Search procedure
We reviewed articles on IGD from seven databases, two of which are Chinese databases (i.e. MEDLINE, PsycINFO, Embase, PubMed, Web of Science and the two Chinese databases: CNKI and Wanfang Data). We searched for studies published between the first available year and 15 July 2019, using the terms ‘gam* disorder’, ‘gam* addiction’, ‘gam* dependenc*’, ‘problematic * gam*’ and ‘pathological * gam*’, combined with the terms ‘Chin*’, ‘Taiwan’, ‘Hong Kong’ and ‘Macao’. We also excluded ‘gamb*’. The articles were included if their title, subject headings or abstract matched these search phrases. When searching in Chinese databases, the corresponding Chinese terms were used. In addition, we reran the searches on 8 February 2020, to identify further studies for inclusion before the final analyses.
Study selection
We included studies that (a) address IGD and have employed the psychometrically standard IGD scale for assessment; (b) have sampled people in mainland China, Hong Kong, Macao or Taiwan; (c) have presented at least one factor correlated with IGD; and (d) have reported the effect sizes of correlation using Pearson correlation coefficient or other types of data that could be converted to Pearson’s r (e.g. means and standard deviations and t test).
We excluded studies that meet the following criteria: (a) the study is a review, case study, comment or editorial; (b) all correlational factors in the study are ineligible for synthesis; (c) the sample and the correlational factors completely overlap with those of another included study; and (d) the full text of the study is unavailable.
Two authors (Y.J. and M.X.C.Y.) have independently applied the eligibility criteria and selected studies to include in the meta-analysis. Disagreements between individual judgements were resolved through discussion. After removing duplicate studies, we first screened the title and abstracts of each study to determine whether the studies addressed IGD, sampled Chinese people and reported correlational factors with IGD, and were not a review, case study, comment or editorial. Subsequently, we retrieved the full text of the studies to examine whether they reported eligible data of effect sizes for correlations.
Validity assessment
The quality of each study was assessed by the Newcastle-Ottawa Scale (NOS) adapted for cross-sectional studies (Herzog et al., 2013). This scale contains eight items: representativeness of the sample, sample size, non-respondents, ascertainment of exposure, comparability, assessment of outcome and statistical test. Each item has different weights and could be assigned up to 1 or 2 scores. The maximum score of the scale is 10. Two authors (Y.J. and M.X.C.Y.) independently assigned the scores, and the interrater reliability was calculated using Cohen’s kappa (Cohen, 1960). Disagreements between the two author’s judgements were resolved by decision of a third author (A.Y.Z.).
Data extraction and coding
For each study, two authors (Y.J. and M.X.C.Y.) independently extracted the data. The following information was collected from each study: study name and the author, publication year, region of the sample, sample size, age range, percentage of male participants, sampling and survey method, scales for assessment, the correlational factor and the reported Pearson correlation coefficient or other data that could be converted to Pearson’s r. When the Pearson’s r was not directly presented, we followed the formulae given by Lipsey and Wilson (2001) to calculate Pearson’s r from a range of statistical data (e.g. means, standard deviation and sample size). An online effect size calculator that helps to run the formulae was used. Disagreements between authors’ judgements were resolved through discussion. For the included longitudinal studies, their baseline data was extracted. If the baseline data were unavailable, follow-up data were extracted.
We also classified each factor according to their psychosocial dimension through discussion. All factors were further classified as either risk or protective factors, based on their positive or negative correlations with IGD.
Quantitative data synthesis
All analyses were completed by using software R (R Core Team, 2013) with various packages involving ‘meta’, ‘metafor’ and ‘dmetar’ (Balduzzi et al., 2019; Harrer et al., 2019a; Viechtbauer, 2010). Pearson’s correlation coefficient (range = −1.0 to 1.0) and its 95% confidence interval were used to calculate the effect sizes for correlations. To interpret the magnitude of correlation coefficients, we followed the guidelines proposed by Hemphill (2003) for psychological literature. Weak, moderate and strong correlation coefficients are defined as r < 0.2, 0.2 < r < 0.3 and r > 0.3, respectively.
For the data synthesis, we employed a random effects model that assumes the true effects are normally distributed. Because the studies included were not identical, the effect sizes could be influenced by various covariates (Borenstein et al., 2011). In addition, the random effects meta-analysis was based on Fisher’s z transformation of the correlations (Cooper et al., 2009). This method allows correlations based on lager samples to gain greater weight compared with those based on smaller samples.
For the heterogeneity analysis, we calculated the Q statistic and I2 index to quantify the heterogeneity. The Q statistic is a measure to estimate the between-study variance (i.e. the heterogeneity across all studies), and the I2 index measures the proportion of excess heterogeneity from the total heterogeneity. According to Higgins et al. (2003), I 2 value of 25%, 50% and 75% could be roughly considered low, moderate and high heterogeneity.
Sensitivity analysis
We used multiple methods to examine the robustness of the result of quantitative synthesis. At first, outliers may exist in the dataset and heavily influence the result. We defined outliers as data points which confidence intervals do not overlap with the confidence interval of the pooled correlation coefficients (Harrer et al., 2019b). We removed the outliers of the correlation coefficient dataset and reran the quantitative synthesis to see whether the result would change substantially.
Second, there is some evidence that studies reporting large effect sizes have a better chance to be published than studies that report smaller effect sizes (Borenstein et al., 2011). The studies included in the analysis may be a biased sample, which would cause the pooled correlation coefficients to reflect the bias. To assess publication bias, we computed the fail-safe N (Rosenthal, 1979) of each correlation coefficient. It was suggested that if fail-safe N exceeds 5K + 10, the publication bias would be negligible.
The funnel plot was also used to determine whether small studies with small effect sizes were missing. We used Egger’s test (Egger et al., 1997) to quantify the funnel plot asymmetry and examine the significance. Sterne et al. (2011) recommend that the test for funnel plot asymmetry should only be conducted if the number of studies is larger than 10. Therefore, we only conducted Egger’s test for risk and protective factors that are contained in more than 10 studies.
Moderator analysis
For the pooled effect sizes with heterogeneity beyond a moderate level (i.e. I2 > 50%), we conducted moderator analysis to examine whether the extra heterogeneity can be explained by the moderators. Missing values were omitted in the analysis. The following variables were determined as moderators between the identified correlational factors and IGD: study quality, types of the sample, region of the samples, percentage of male participants and mean sample age. We assumed these moderators might affect the effect sizes. Meta-regression analysis was used to examine the moderator effects. It is also recommended that for meta-regression, each moderator should contain at least 10 studies (Borenstein et al., 2011). Therefore, we only conducted the moderator analysis for risk and protective factors with more than 10 studies.
Result
Study selection
Our study selection process is shown in Figure 1. Our search algorithm initially identified 1767 unique studies. Among them, 1546 articles were excluded after screening their titles and abstracts. We retrieved 221 studies for their full text and assessed for eligibility. Among them, 68 studies were excluded. Specifically, 2 could not be found in their entirety, 3 were case studies or reviews, 8 did not employ psychometrically standard IGD scales for assessment, 11 showed no correlational factor with IGD, 16 did not show Pearson’s r or other convertible data for effect sizes, 23 did not show the eligible correlational factors for synthesis and 5 showed data that completely overlapped with other included studies. As a result, 153 studies were included in the meta-analysis (Supporting Information, S2).
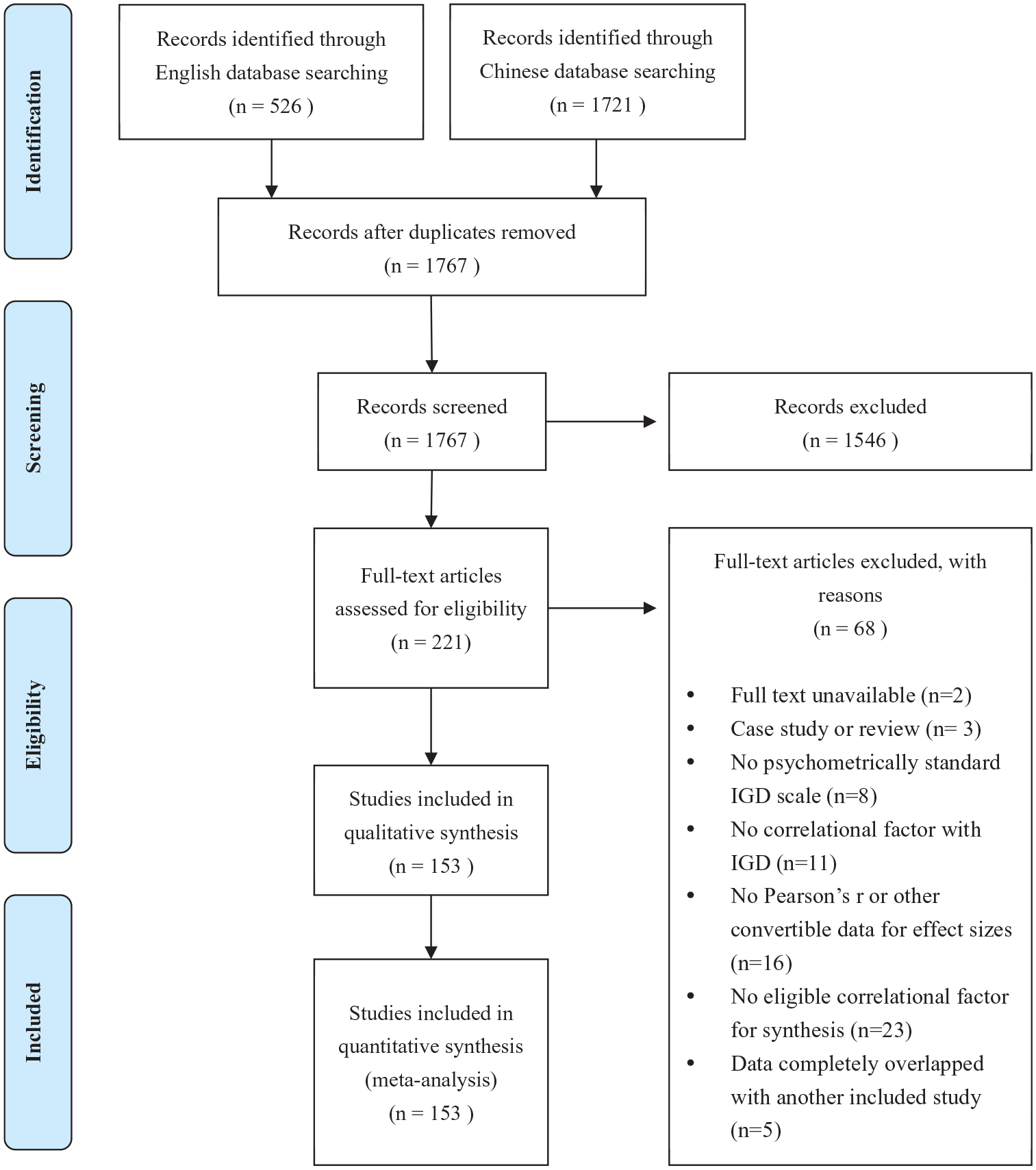
PRISMA flow diagram of study selection.
Study characteristics
Almost all 153 studies were cross-sectional design in nature, except 8 longitudinal studies. The sample size of each study ranged from 40 to 4105 (mean sample size = 758), and the aggregated number of included individuals was 115,975. The studies mainly sampled four different types of population: IGD patients and healthy controls (n = 7); primary school and high school students (n = 73); college students (n = 64); and people of all ages (n = 8). One study sampled high school students and college students. Most of the studies (n = 135) used paper-and-pencil questionnaires to collect responses.
As for the assessment, various instruments were employed to evaluate IGD, such as adapted DSM-IV criteria for pathological gambling (n = 6), DSM-5 criteria for IGD (n = 16), Pathological Video Game Use Questionnaire (n = 30), Young’s Diagnostic Questionnaire (n = 19), Chinese Internet Addiction Scale (n = 10), and others. All instruments used were in the Chinese language, and for those instruments originally assessing Internet addiction or other behavioural addiction, the included studies usually modified the terms to IGD. The quality score of the included studies ranged from 5 to 9 (M = 7.2, SD = 1) (Supporting Information, S3). And the Cohen’s kappa interrater reliability of the reviewers was 0.884.
Quantitative data synthesis
Risk factors
Figure 2 shows the summary plot of the pooled effect size of each risk factor. Sixty-four factors were identified. The dashed line in the figure separates factors that are strongly correlated with IGD and factors with moderate and weak correlations.
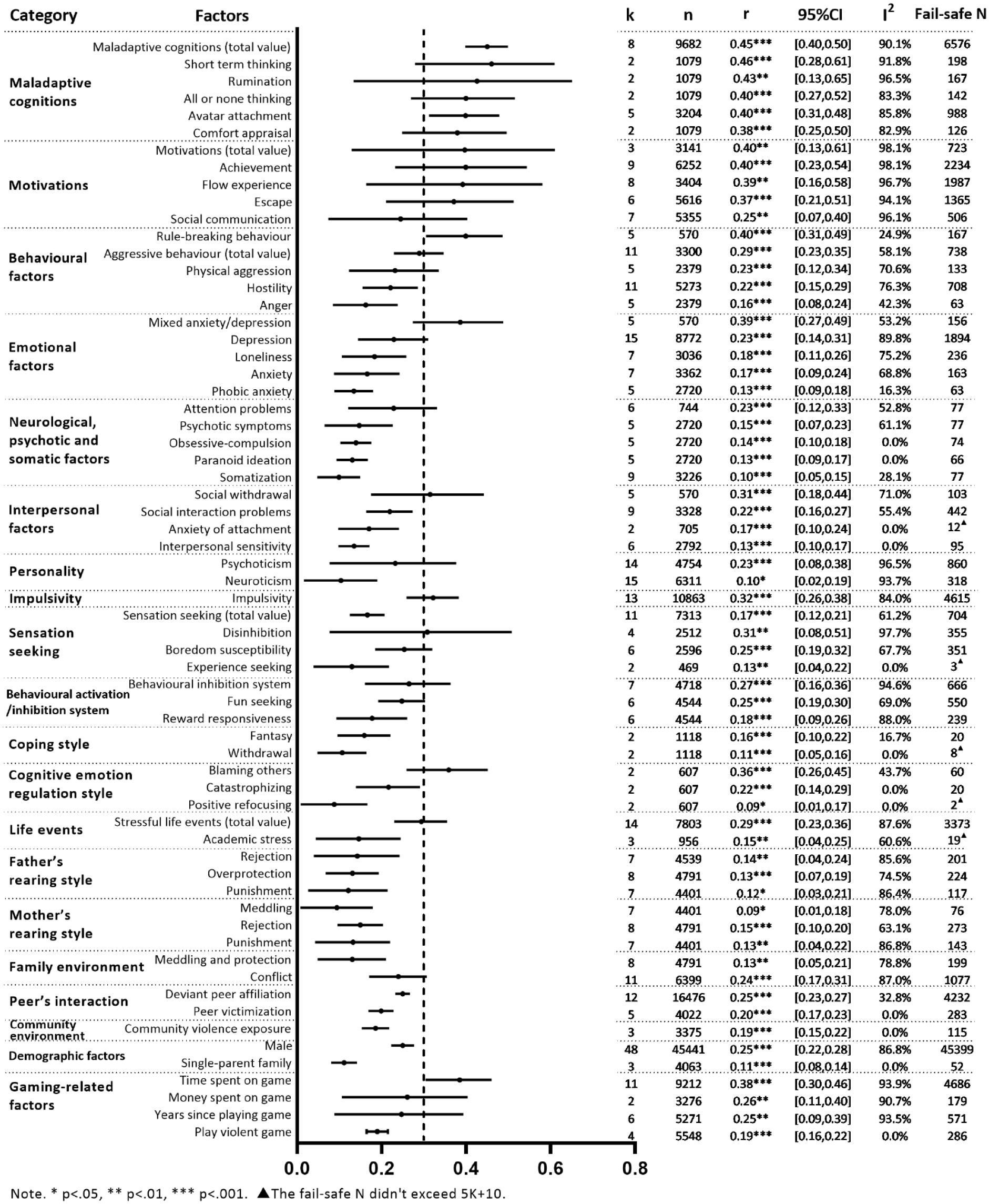
Summary plot of the pooled effect sizes of risk factors.
Most risk factors strongly correlated with IGD fell into the category of maladaptive cognitions and motivations. First, maladaptive cognitions generally showed the strongest correlations to IGD, and the effect size for the total value was 0.46. The maladaptive cognitions that showed large effect sizes were short-term thinking (r = 0.46), rumination (r = 0.43), all-or-none thinking (r = 0.40), avatar attachment (r = 0.40) and comfort appraisal (r = 0.38). Second, strong correlations were found between IGD and various motivational factors, involving achievement (r = 0.40), flow experience (r = 0.39) and escape (r = 0.37). The between-study variance for the above effect sizes was high.
Except for maladaptive cognition and motivation, other factors with large effect sizes fell into four categories: psychopathological characteristics, personality traits, cognition emotion regulation style and gaming-related factors. Psychopathological factors included rule-breaking behaviour (r = 0.4), mixed anxiety/depression (r = 0.39) and social withdrawal (r = 0.31); personality traits involved impulsivity (r = 0.33) and disinhibition (r = 0.31); cognition emotion regulation style involved blaming others (r = 0.36); and gaming-related factors involved time spent on game (r = 0.38). In addition, the effect sizes of aggressive behaviour (r = 0.29) and stressful life events (r = 0.29) were almost large. It is also noteworthy that being male (r = 0.25) was moderately correlated with IGD.
Generally, the factors related to the ‘environments’ (e.g. family, school, community) showed modest effect sizes comparing to the factors related to the ‘individual’. Several familial and scholastic factors showed moderate correlations with IGD. They were conflictual family environment (r = 0.24), deviant peer affiliation (r = 0.25) and peer victimisation (r = 0.20).
Protective factors
Figure 3 shows a summary of protective factors. Thirty-seven factors were identified, and the dashed line in the figure highlights the factors strongly correlated with IGD. We also found only one protective factor to have a strong correlation with IGD: self-control (r = −0.31).
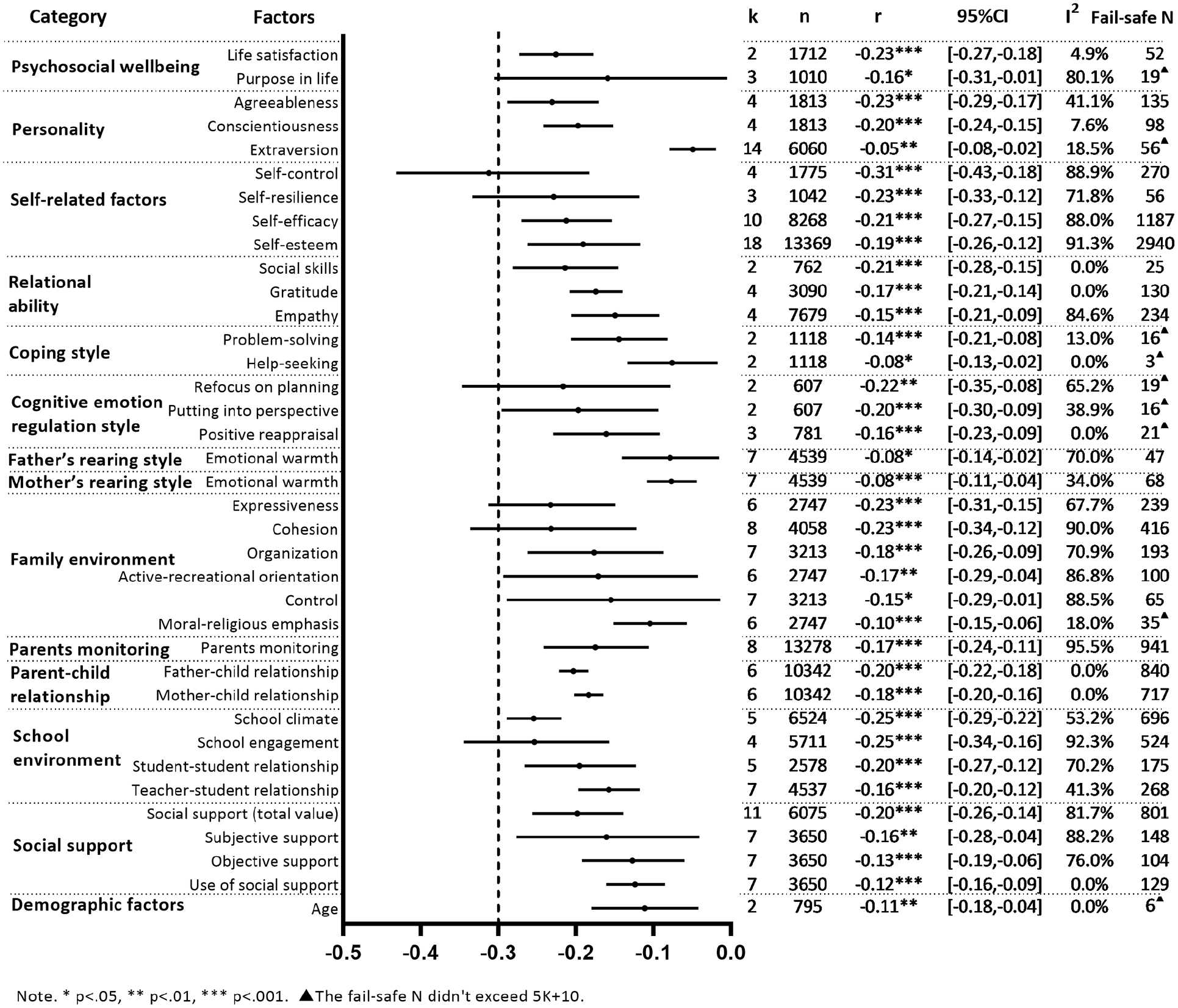
Summary plot of the pooled effect sizes of protective factors.
Various factors showed moderate correlation with IGD, involving psychosocial well-being: life satisfaction (r = −0.23); personality: agreeableness (r = −0.23) and conscientiousness (r = −0.20); self-related factors: self-resilience (−0.23) and self-efficacy (r = −0.21); relational ability: social skills (r = −0.21); and cognitive emotion regulation style: refocus on planning (r = −0.22) and putting into perspective (r = −0.20).
Several familial and scholastic factors showed moderate correlations with IGD. The familial factors were the family environment of expressiveness (r = −0.23) and cohesion (r = −0.23), and positive father–child relationships (−0.20). The scholastic factors were school engagement (r = −0.25), positive school climate (r = −0.25) and positive student–student relationship (r = −0.20). In addition, social support (r = −0.20) also showed a moderate correlation with IGD.
Sensitivity analysis
The effect of outliers
After removing the outlier, the average I2 of all factors has dropped from 56.3% to 45.9%. We checked if any significant correlation became non-significant and vice versa, and if the effect sizes changed considerably (i.e. the value changes of Pearson’s r exceeded 0.05). Table 1 shows the factors that effect sizes changed greatly after removing outliers, and their I2 also dropped clearly.
Factors significantly affected by the outliers.
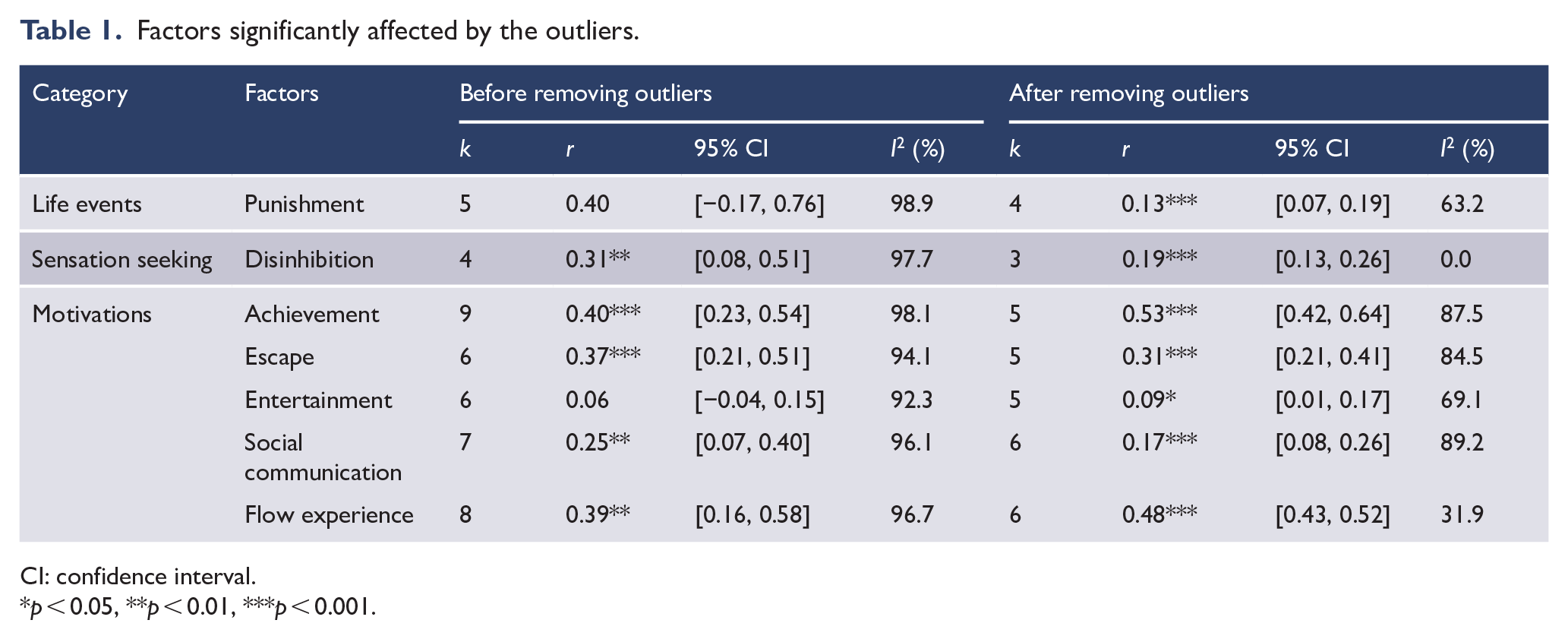
CI: confidence interval.
p < 0.05, **p < 0.01, ***p < 0.001.
The life events (punishment) (r = 0.13) became significantly correlated with IGD after removing the outliers, and the I2 dropped to 63.2%. The effect size value of disinhibition decreased to 0.19, and I2 dropped to 0%. Several motivation factors also changed: the effect size values of achievement and flow experience increased to 0.53 and 0.48; escape and social communication decreased to 0.31 and 0.27; and entertainment became significantly correlated to IGD with a small effect size.
We excluded life events (punishment) and entertainment from the correlational factors of IGD since their effect size values changed significantly in the opposite direction after removing the outliers. We also excluded disinhibition from the strong correlational factors of IGD as its effect size value decreased to a moderate level.
Fail-safe N
The fail-safe N of 92.2% (59/64) of the risk factors exceeded 5K + 10, and those of 76.3% (29/38) of the protective factors exceeded 5K + 10. Therefore, we considered the effect sizes for most identified factors were robust, and there were more protective factors than risk factors which were probably biased. The results of the fail-safe Ns are presented in Figures 2 and 3. The factors with fail-safe N less than 5K + 10 are marked, and we exclude them from correlational factors of IGD since the results may be influenced by publication bias.
Egger’s test
Seventeen factors were eligible for Egger’s test. The result suggested that all of them were unbiased except aggressive behaviour (total value). As a result, the effect sizes of this factor might be biased since small studies with small effect sizes were missing. And we also excluded this factor from the correctional factors of IGD.
Moderator analysis
Thirteen factors were needed and eligible for moderator analysis. We detected that heterogeneity could be reduced to a low level (i.e. I2 < 50%) for only one factor. With the percentage of male participants as the moderator, the value of I2 for aggressive behaviour (total value) could be reduced to 28.1%. If the percentage of male participants were to be increased, the effect size of the correlation between aggressive behaviour and IGD would increase as well. However, this finding may not be robust since the sensitivity analysis showed this factor to be biased.
Discussion
To effectively prevent and intervene in IGD, proper identification of risk and protective factors is needed. This study intends to exhaustively review the risk and protective factors of IGD and compare the magnitude of correlations. We examined 153 studies with 115,975 subjects and identified 64 risk factors and 37 protective factors. After a sensitivity analysis, 56 risk factors and 28 protective factors were retained. Finally, 16 risk factors and 1 protective factor were identified to be strongly correlated with IGD.
The factors with the strongest correlation were maladaptive cognitions, which included short-term thinking, rumination, all-or-none thinking, avatar attachment and comfort appraisal. These cognitive processes are automatically invoked when online games are available and lead directly to problematic gaming. Scholars have noticed the importance of cognitions in IGD development. Davis (2001) proposed a cognitive behavioural model to explain the causal mechanism of Internet addiction. In his model, specific maladaptive cognitions about the self and the world are considered proximal factors for Internet addiction. For example, people who tend to continually think about their problems of online gaming (rumination) will experience more severe IGD, since rumination will recall more reinforced memories about gaming, thus maintaining the vicious cycle of IGD.
People with IGD may have maladaptive cognitions about the self (e.g. ‘I am worthless offline, but when playing online games, I am someone’.), which incentivise them to play online games to have more positive responses from others and gain a sense of personal competence and pride. Meanwhile, maladaptive cognitions about the world (e.g. ‘The gaming world is the only place I feel safe and respected’.) drive them to play games to gain a sense of safety, and they may feel depressed and irritated when they quit playing games. To alleviate negative emotions, they are likely to return to play games.
There are more underlying cognitions that contribute to IGD. King and Delfabbro (2014) have identified four cognitive factors of IGD through a systematic review, including ‘(a) beliefs about game reward value and tangibility, (b) maladaptive and inflexible rules about gaming behaviour, (c) over-reliance on gaming to meet self-esteem needs, and (d) gaming as a method of gaining social acceptance’. Challenging these maladaptive cognitions might be useful to reduce IGD symptoms.
Generally, motivations showed the second-strongest correlations with IGD. The motivational factors involve flow experience, achievement, escapism and social communication. This result is partially consistent with previous studies. Young and Brand (2017) have summarised the most relevant motivations for playing games as achievement (or performance), social interactions and escapism/discovery. Our study found that social interactions were not as meaningful as achievement and escapism and that flow experience was another critical intrinsic motivation.
Achievement and escapism are salient extrinsic motivations for online gaming among IGD people. People with IGD would pursue achievement satisfaction in gaming because they inherently prefer activities with mission rewards and high competition. And they may face poor academic achievement or career achievement in the real world, thus use online gaming to compensate for deficits (Huang et al., 2006). They would also pursue Internet gaming to escape from reality because they may be trapped in anxious and depressed mood in real life. As a result, they play online games for mood modification (Li et al., 2011). Flow experience is a state in which people get completely immersed in an activity, and the experience itself is so gratifying that people will do it even at a high cost (Csikszentmihalyi, 2013). When playing online games, players get gratification by achieving goals (e.g. beating other players, defeating the boss and advancing the characteristics). For those players who are ‘in the zone’, they concentrate so much on their tasks, enjoy their performances and get great pleasure and a diminished sense of time and space. Therefore, they will spend excessive time on playing and not stop even they miss out on other important activities.
Except for cognitions and motivations, factors which showed strong correlations also fell in other categories. First, psychopathological factors involving rule-breaking behaviour, mixed anxiety/depression and social withdrawal were strongly correlated with IGD. As mentioned before, they were demonstrated by longitudinal studies to have predictive power for IGD. Rule-breaking behaviour played a part in IGD development. It is plausible that online gaming has provided a space where rule-breaking and aggressive behaviour prohibited in the real world could be expressed without restrictions. People with mixed anxiety/depression also have higher chances to develop IGD because those with emotional difficulties may escape to a virtual world to avoid facing stress and gain temporal comfort (Cho et al., 2013). As for people with social withdrawal, online games offer an excellent place for them to achieve social interactions. It allows players to express themselves in the ways that may be uncomfortable in reality because of their appearance, gender, sexuality and age (Cole and Griffiths, 2007).
Second, we found a personality trait, impulsivity, also contributed to IGD greatly. Exhibiting impulsivity suggests a breakdown in the process underlying cognitive inhibitory control (Ding et al., 2014). Therefore, impulsivity may link to the impaired cognitive function of executive control to play and diminished ability to defer gratification gained from playing games. On the contrary, we found self-control strongly prevented people from IGD. Self-control is an ability to resist an impulse, drive or temptation to perform an action (Kim et al., 2008). It is not surprising that people with strong self-control abilities may be good at inhibiting the impulse to play online games immoderately.
In addition, we found a cognitive emotion regulation style, blaming others, had a strong correlation with IGD. Among people experiencing stress or threatening events, blaming others has an association with poor emotional well-being (Garnefski et al., 2001). Therefore, people with style of blaming others may have a high probability to experience depression and anxiety, thus play games to escape. The last factor we found, which has a strong correlation with IGD, was time spent on gaming. In some instruments, time spent on gaming was considered a significant indicator to predict or even diagnose IGD (King et al., 2013b).
It is noteworthy that we found environmental factors probably were not as crucial as the abovementioned individual factors. They had low to moderate correlations with IGD. The results were partially consistent with Koo and Kwon’s (2014) research, which found the magnitude of the correlation between intrapersonal factors and IGD was significantly higher than that of interpersonal variables factors. We assume that environmental factors do play an important role in IGD development, but what matters more is individuals’ ways of processing information which comes from the external environment. Family, school and social factors contribute to IGD because either they increase individuals’ motivations to play online games or they implicitly shape individuals’ maladaptive cognitions of themselves, the real world and the gaming world.
For the familial factors, we found that the conflictual family environment had a moderate positive correlation with IGD, while expressiveness and cohesion family had negative correlations with IGD. The escapist explanation (Bonnaire and Phan, 2017) can explain the relationship between family environment and problematic gaming. Adolescents exposed to parental conflict may have feelings of depression, anxiety and divided loyalty between parents. As a consequence, they may flee into the gaming world to avoid negative emotions and gain support from online friends.
Long et al. (2018) reported in a systematic review that family economic status and parental educational background were correlated with IGD. However, this study found family income (k = 6, p = 0.57), mother’s education level (k = 4, p = 0.35) and father’s educational level (k = 4, p = 0.20) have no significant correlation with IGD. The inconsistency may be because the study of Long et al. only included two articles reporting family economic status and one article reporting parental educational background. In contrast, this study included more articles, and some articles reported opposite results to their findings. After conducting a quantitative synthesis, we had the overall values of effect sizes, which indicated the insignificant correlations.
School and community factors also play a role in IGD development. Deviant peer affiliation and peer victimisation had moderate correlations with IGD. Peer contagion could explain the association between deviant peer affiliation and IGD. Deviant friends may provide opportunities to play online games, offer positive or negative reinforcement for game behaviour, model and normalise IGD (Li et al., 2016). As for peer victimisation, it is understandable that when children and adolescents are bullied at school, they may turn to the virtual world to seek comfort and confidence and escape from their painful real-life problems (Hsieh et al., 2019). On the contrary, harmonious school climate, high level of school engagement and positive relationship between students could reduce the risk of being in these situations. Understandably, a good school climate would reduce deviant peer affiliation and enhance school discipline to prevent adolescents from IGD (Li et al., 2016). Similarly, adolescents with high school engagement levels are more likely to learn and to meet conventional expectations and keep themselves away from deviant peers (Zhu et al., 2015). In addition, a positive student–student relationship would support students when they face difficulties and prevent them from deviant peers, thus decreasing the risk of IGD.
We intend to highlight that the magnitude of the correlations may help to distinguish the proximal and distal factors in IGD development. The proximal risk factors are those ‘risk factor(s) in the causal chain that actually precipitate disease, as distinguished from predisposing or distal risk factors’; the distal risk factors are behavioural or environmental factors ‘that has a remote or indirect causal influence on a specific disease outcome’ (Last, 2007). The factors with large correlational effect sizes have higher chances to be proximal in the chain of events leading to pathological gaming. In contrast, those with small correlation effect sizes are more likely to be distal. The results of this study suggest that the maladaptive cognitions and motivations have higher chances to be the proximal correlates of IGD, which may represent an immediate vulnerability for IGD. And factors like psychopathology, personality traits, stressful life events and familial and scholastic factors could be distal correlates, which may represent an underlying vulnerability for IGD and contribute to IGD through intermediary factors.
Several studies have highlighted the mediating effects of the proximal correlates between distal correlates and IGD. Xiong (2018) found depression contributes to IGD through maladaptive cognitions. People with depression are easy to generate maladaptive cognitions (e.g. short-term thinking, all-or-none thinking) to exaggerate the benefit of online gaming and lose the balance between gaming and other activities. In addition, Bányai et al. (2019) found escapism motives mediated psychiatric distress and IGD. People with psychiatric symptoms are more likely to escape in gaming to avoid real-life problems and develop IGD later. It has reported that motivations also mediated the relationship between behavioural inhibition system and IGD (Xie et al., 2016). Individuals with higher scores of behavioural inhibition system are more likely to get a sense of achievement from online games and escape the anxiety of reality. To conclude, there is some evidence to support the assumption that maladaptive cognitions and motivations were more proximal to IGD.
A new theoretical model: the motivation–cognition–behaviour model
Based on the findings of this study, we propose a theoretical model named motivation–cognition–behaviour model to explain the IGD mechanism. The model highlighted the role of maladaptive cognitions and motivations in the development of IGD.
In this model (as Figure 4 shows), the most proximal factor of pathological gaming is maladaptive cognition, which includes short-term thinking, rumination, all-or-none thinking, comfort appraisal and avatar attachment. The maladaptive cognitions could be automatically enacted when online games are available, then directly lead to pathological gaming. Another proximal factor is motivation, which includes flow experience, achievement and escapism. Motivations have important connections with maladaptive cognitions. For example, the cognitive reasoning process can be influenced by motivations (i.e. motivated reasoning). People can use reasoning strategies to confirm their preferred conclusions. People with IGD may tend to overvalue the gaming rewards and ignore the negative consequence for excessive gaming because they want to play games to have a sense of achievement, escapism and pure pleasure.
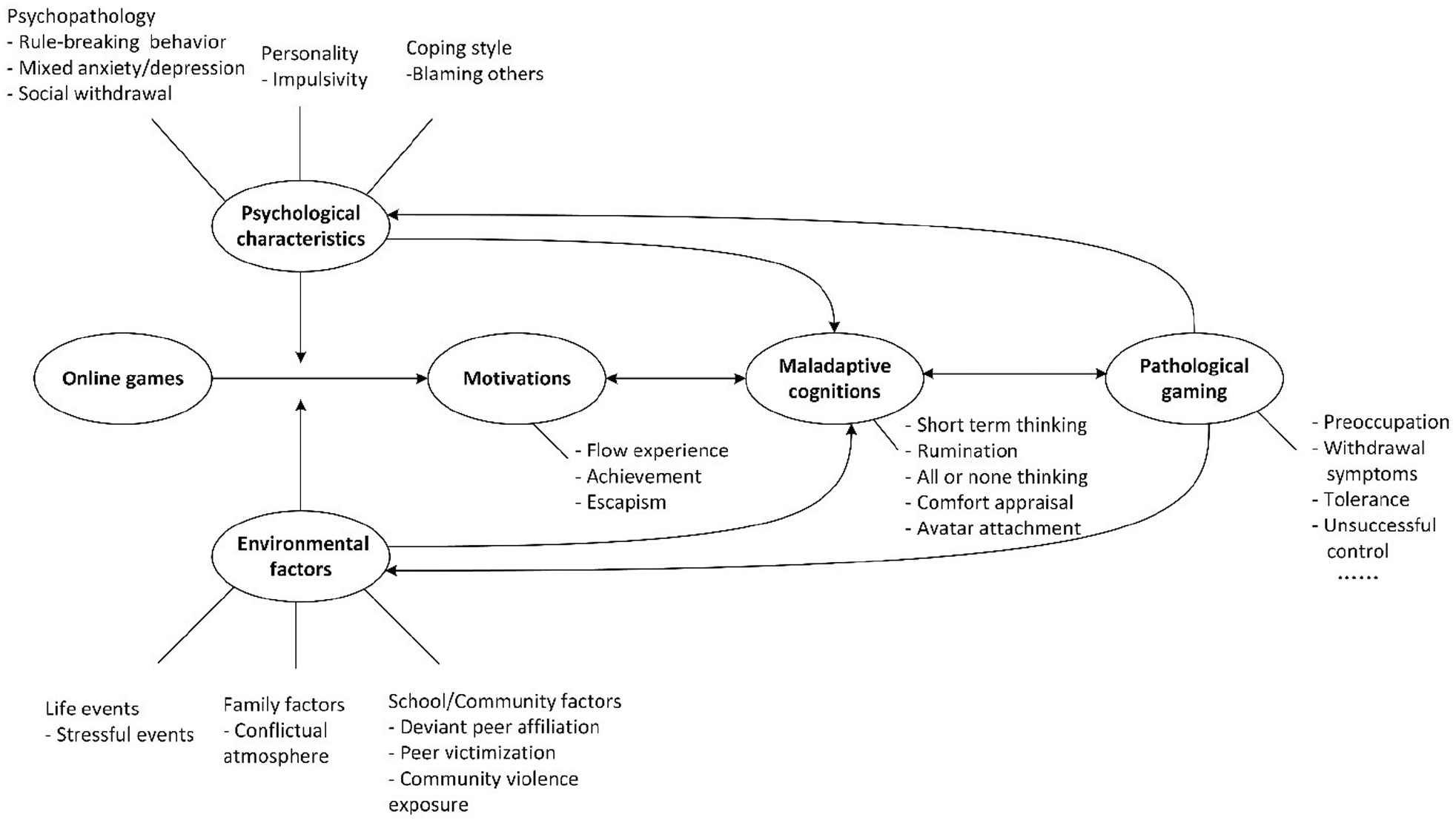
The motivation–cognition–behaviour model of IGD.
The person’s psychological characteristics and environmental factors are considered distal factors, while the environmental factors may be less important as other factors. The psychological characteristics involve psychopathology, personality and coping style. Environmental factors involve life events, family factors and school/community factors. They can trigger motivations or maladaptive cognitions to excessively playing video games. Pathological gaming is the consequence of the above pathway, which includes excessive time spent on gaming, craving, withdrawal symptoms preoccupation, tolerance, etc. And pathological gaming will reinforce the proximal factors and distal factors in turn. A vicious loop generates in the process of driving people compulsively and continuously playing.
An example can be given to explain the mechanism. People who experience stressful life events have emotions of depression and anxiety. They may think they are incapable of handling the problem in real life. As a result, they are motivated to play online games to escape from the bad mood and self-blame thoughts. When playing games, they can forget the trouble and stress in real life. After that, they believe ‘Online world is much more comfortable and safer than the real world’ and ‘I feel being online the most comfortable because I do not have to worry about the troubles’. As a consequence, they will spend a much longer time than originally expected. Playing video games relieves their bad mood temporarily, but once games are not available, their depression and anxiety will increase. Finally, a vicious cycle is developed to drive them to compulsively and continuously play online games. We encourage more empirical studies to examine the pathways highlighted in this model.
This study has three major limitations. At first, almost all the included studies were cross-sectional design. For the longitudinal studies, we only extracted the baseline or follow-up data. Cross-sectional studies do have strengths for analysing risk and protective factors. They allow the investigators to examine a large number of variables at the same time, and they are flexible and efficient to characterise the risk and protective factors in a particular population (Coran et al., 2012; Laake et al., 2015). However, the weakness of the cross-sectional design is apparent. Because cross-sectional studies have no dimension of time, it is impossible to determine if exposure to a risk factor occurred before, during or after the disease emerged (Arnett and Claas, 2017). As a result, the relationship examined in this study is the association between risk or protective factors and IGD but not the causal relationship. Correspondingly, the new model is also constructed on the base of the correlational findings. This limitation may hinder our interpretation of the results.
The second limitation is the small number of the included studies for each factor. This study reviewed 153 studies, identified 56 risk factors and 28 protective factors. The syntheses of effect sizes for most factors were based on less than 10 studies. Due to the small number, some of the analysis was not applicable to conduct for all the factors, especially the moderator analysis. We were not certain for many of the factors if the moderators could influence the correlations and if the high heterogeneity could be explained by the moderators. The third limitation is that the vast majority of the participants of the included studies are adolescents and young adults; therefore, the findings of this meta-analysis are restricted to the interpretation for this age group. It should be done with caution when generalising the findings to other age groups.
Notwithstanding the methodological limitations, this study demonstrated several novel findings and practical and theoretical implications. To our knowledge, this is the first study that comprehensively reviewed the specific risk and protective correlational factors of IGD and compared the magnitude of the effect sizes for correlations. We innovatively detected that maladaptive cognitions and motivations were the strong correlational factors of IGD, while the previous systematic reviews barely included these factors and specifically identified their importance to IGD (Koo and Kwon, 2014; Long et al., 2018; Mihara and Higuchi, 2017). Therefore, we suggest that the strong correlational factors, especially maladaptive cognitions and motivations, should be given higher priority to consider when conducting interventions. Following psychotherapies are suggested for further clinical interventions: therapies to change people’s cognitions such as cognitive behavioural therapy, mindfulness-based cognitive therapy and cognitive enhancement therapy, and therapies that focus on people’s motivations such as motivational interviewing and motivational enhancement therapy. More intervention studies are encouraged to examine the efficacy of these therapies.
Second, we build a theoretical model to understand IGD deeply, which is based on the identification of proximal and distal factors by their magnitude of correlations to IGD. The model highlights the motivations and maladaptive cognitions as proximal causes to pathological gaming and other individual and environmental factors as distal causes. The model illustrates the hypothetical causal chain. More empirical studies are encouraged to test the pathway demonstrated in this model.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211025703 – Supplemental material for Risk and protective factors of Internet gaming disorder among Chinese people: A meta-analysis
Supplemental material, sj-docx-1-anp-10.1177_00048674211025703 for Risk and protective factors of Internet gaming disorder among Chinese people: A meta-analysis by Yinan Ji, Margaret Xi Can Yin, Anna Yan Zhang and Daniel Fu Keung Wong in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.