
Abstract
Objective:
To examine the two-year outcomes for depression, anxiety, cognitive and global social functioning after cognitive behavioural therapy (CBT) and metacognitive therapy (MCT) for depression.
Method:
Participants were 31 adults with a diagnosis of major depressive disorder in a randomised pilot study comparing MCT and CBT. Therapy modality differences in change in depression and anxiety symptoms, dysfunctional attitudes, metacognitions, rumination, worry and global social functioning were examined at the two-year follow-up for those who completed therapy.
Results:
Significant improvements, with large effect sizes, were evident for all outcome variables. There were no significant differences in outcome between CBT and MCT. The greatest change over time occurred for depression and anxiety. Large changes were evident for metacognitions, rumination, dysfunctional attitudes, worry and global social functioning. Sixty-seven percent had not experienced a major depression and had been well during all of the past year, prior to the follow-up assessment.
Conclusion:
The finding at end treatment, of no modality specific differences, was also evident at two-year follow-up. Although CBT and MCT targeted depression, improvements were much wider, and although CBT and MCT take different approaches, both therapies produced positive change over time across all cognitive variables. CBT and MCT provide treatment options, that not only improve the longer-term outcome of depression, but also result in improvements in anxiety, global social functioning and cognitive status.
Introduction
Depression is the second leading cause of health disability in the world (World Health Organization, 2004). Since the initial development of cognitive behavioural therapy (CBT), numerous studies and subsequent meta-analyses have repeatedly shown the efficacy of this approach for a variety of disorders, including depression (Cuijpers et al., 2013, 2019; Munder et al., 2019). As a consequence, CBT is recommended as one of the first-line treatments in a variety of depression treatment guidelines, for example, Royal Australian New Zealand Journal Psychiatry (Malhi et al., 2021), the National Institute for Health and Clinical Excellence (2009) and the American Psychological Association (2019). Despite the efficacy of CBT, it is also the case that only 40–58% of patients recover at the end of treatment (Dimidjian et al., 2006). Similar response rates are evident for other psychotherapies and medications (Cuijpers and Gentili, 2017). Unfortunately, around 50% of those who initially respond to treatment go on to relapse within a year, with most relapsing in the first 6 months posttreatment (Burcusa and Iacono, 2007; Fonagy et al., 2005). It also seems after each episode of depression there is a higher probability that subsequent episodes will be treatment resistant (Kendler et al., 2000; Kessing et al., 2004).
The limited outcome of psychological treatments such as traditional CBT has led researchers to investigate alternative psychotherapies for treating depression. Metacognitive therapy (MCT) is one such development, originally developed for the treatment of anxiety disorders. There are important fundamental differences in the underpinnings of MCT, as compared with CBT, that make the MCT model very applicable to depression (Wells et al., 2009). In the metacognitive model, psychological problems such as depression are maintained, not by the content of thinking per se, but by the activation of the cognitive-attentional syndrome (CAS). The CAS, an inflexible style of thinking, increases rumination and worry, which in turn maintains depression. According to Wells et al. (2009), an individual’s positive beliefs (metacognitions) that repetitive thinking (i.e. worry and rumination) is helpful and negative beliefs that the repetitive thinking is uncontrollable or harmful maintain the CAS and therefore subsequent rumination or worry. Considerable research supports the metacognitive model of depression, with studies finding that rumination not only increases the severity of the depressive episode but also the length of the episode and likelihood of relapse (Kovács et al., 2020; Nolen-Hoeksema et al., 1993; Watkins and Roberts, 2020).
A growing number of studies also support the effectiveness of MCT for depression. For example, in their open trial of group MCT, Dammen et al. (2015) reported all (n = 11) patients met recovery criteria at the end of treatment and 91% at the 6-month follow-up. Similar to CBT, MCT also appears to be as effective for severe, comorbid and treatment-resistant depression. In their open trial of treatment resistant depression, Wells et al. (2012) reported that 80% of patients at posttreatment and 70% at the 12-month follow-up were classified as recovered. In their open trial with severe depression and current comorbid disorders, Hjemdal et al. (2017) reported that all (n = 10) patients were deemed nondepressed at the end of MCT. At the 6-month follow-up, Hjemdal and colleagues reported that 70% were classified as recovered, 20% improved and 10% unchanged (Beck Depression Inventory [BDI]). Hjemdal et al. (2017) also reported significant improvements in the rate of comorbid disorders. Other studies of MCT for depression have also reported improvement in domains other than depressive symptoms. In their waitlist study of 39 patients with depression, Hagen et al. (2017) reported large effect sizes for both depressive (d = 2.51) and anxiety (d = 1.92) symptoms. Approximately 70–80% were classified as recovered at posttreatment and 6-month follow-up. Although not a specific target of MCT, a further study by this group found significant improvement in interpersonal functioning and depression (Strand et al., 2018). In their 2018 review of eight studies of MCT for depression, Normann and Morina (2018) reported that in their within-group analyses, the pre–posttreatment effect sizes were very large for depression (g = 1.72).
It also appears that MCT for depression is at least as effective as CBT. Jordan et al. (2014) conducted a pilot study to compare the relative speed and efficacy of MCT and CBT in adult outpatients with depression. At the end of treatment, both MCT and CBT resulted in similar clinically significant changes in depressive symptoms, with moderate to large effect sizes. Of note, there were no significant modality differences in the speed of change over therapy, and at the 6-month follow-up, the gains were maintained similarly for MCT and CBT. In the previously mentioned Normann and Morina (2018) review, the treatment modality meta-analyses comparing MCT with CBT evidenced slightly higher effect sizes for MCT. Normann et al. note, however, that the number of trials examining MCT for their review was low and most studies had small sample sizes.
The long-term effects of CBT and MCT are much less clear, as very few studies report outcome past 12-month follow-up, and most reporting only 6-month follow-up. One of the reasons longitudinal studies are scarce is because high attrition rates tend to occur as studies progress over time. In their review of largely 6- and 12-month follow-up studies, after acute-phase psychotherapy for depression, Karyotaki et al. (2016) reported that the effect of psychotherapy appeared to decrease as the follow-up duration increased. Given depression is a recurrent disorder with approximately 80% experiencing at least two episodes in their lifetime (Malhi et al., 2021), we need to continue to understand the effects of therapy, not only in the short term but also long after therapy has ended. By tracking depression over time, it is possible to better understand the true effectiveness of a given therapy. Long-term follow-up of depression, after different therapy modalities, would also enable examination of whether changes over time are dependent on the specific approach utilised. It is also not clear that the specific cognitive changes that are the focus of CBT (e.g. modifying thinking content) and in MCT (e.g. decreasing rumination) to ameliorate depression are uniquely modality specific. There is some evidence that both CBT and MCT may result in reductions in rumination and dysfunctional thinking (Spinhoven et al., 2018), at least in the short term. The possibility that CBT and MCT produce general rather than specific changes is further indicated by the research highlighted above, that is, although both CBT and MCT focus on depression, improvement in non-targeted areas, such as comorbid disorders and social and interpersonal functioning (i.e. quality-of-life indices), also occurs.
This paper reports on the 2-year follow-up of patients who received either CBT or MCT for depression in the Jordan et al. (2014) study. This study has a number of strengths that make this analysis important. Although a small pilot study, it is still one of the larger studies comparing MCT and CBT for depression to date. In addition to the assessment of depression status, anxiety, cognitive variables and global social functioning were also assessed at 2-year follow-up. Finally, this study had a good retention rate during therapy and at follow-up.
The specific aims of the current study were to examine the depression status of patients at a follow-up 2 years after they were randomised to CBT or MCT (22 months after the end of treatment). In addition, anxiety and social functioning outcomes in the two treatment groups were examined. Similarly, changes in cognitive variables specifically relevant to the mechanisms of action in CBT (dysfunctional cognitions) and in MCT (metacognitions, rumination and worry) were examined.
Methods
Participants
Participants were 48 men and women, aged 18–65 years, with a current primary Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) diagnosis of major depressive disorder or Bipolar II disorder depressed phase, who were able to converse and answer questionnaires in the English language and provide informed consent. Exclusion criteria were minimal and were Bipolar I disorder, schizophrenia, current severe substance abuse, psychotropic medication other than the occasional hypnotic, severe physical illness or a recent (past year) adequate course of CBT or MCT. Recruitment was primarily through referrals from health professionals, although included some self-referrals. This trial received ethical approval from the Upper South B Regional Ethics Committee, New Zealand, and participants provided written informed consent. The study was registered with the Australian and New Zealand Clinical trials Registry ACTRN12611000804987. CONSORT information has been reported in Jordan et al. (2014).
Procedure
After pretreatment assessment, participants were randomised to either MCT or CBT. Of the 48 patients, 23 were randomised to MCT and 25 were randomised to CBT. Duration of therapy was 8–15 sessions over 12 weeks. Eight was set as the minimum number of sessions to ensure an adequate dose of therapy. Twenty patients completed an adequate dose of MCT and 22 completed an adequate dose of CBT (87.5% total). Four therapists delivered both therapies. Therapist competence and treatment integrity were addressed by weekly group supervision and monthly ratings of randomly selected audio-taped sessions for each therapist. Further information about the treatment protocol, therapy integrity and the patient flow figure up until the 6-month follow-up can be found in Jordan et al. (2014).
At 2-year follow-up, 31 (13 CBT and 18 MCT) of the 42 (73.8%) participants who completed therapy completed self-report questionnaires relevant to the study aims here. At 2-year follow-up, eight participants who previously completed therapy were unable to be contacted, two participants were contacted but did not return questionnaires and one participant withdrew from follow-up assessments.
Therapy content
Therapy was based on the manuals of Judith Beck (1995) and Adrian Wells (2008; Wells et al., 2009). Key components of CBT included the CBT model/formulation, behavioural activation (activity scheduling, pleasant events), monitoring and challenging automatic thoughts, behavioural experiments and relapse prevention. Key components of MCT included the MCT model/formulation, identifying rumination and worry, challenging positive and negative metacognitions, addressing the CAS, the attention training task, attentional re-focussing, detached mindfulness, behavioural experiments and the therapy blueprint.
Measures
Measures of depression, anxiety, cognitive constructs and social functioning completed at pretreatment and repeated at 2-year follow-up are used in analyses here. Depression was assessed with the Montgomery–Åsberg Depression Rating Scale (Montgomery and Asberg, 1979) at baseline, the Quick Inventory of Depression Symptomatology–Self-Report Version (QIDS16-SR; Rush et al., 2003) and the depression subscale of the Hopkins Symptom Checklist (SCL-90; Derogatis et al., 1974). A cut-off score of 13 on the QIDS16-SR indicates a probable major depressive episode (Rush et al., 2003). General anxiety was assessed with the anxiety subscale of the SCL-90 and worry with the Penn State Worry Questionnaire (PSWQ; Meyer et al., 1990).
Cognitive measures included the Dysfunctional Attitudes Scale (DAS; Weissman and Beck, 1978) and the rumination subscale from the Response Styles Questionnaire (RSQ; Nolen-Hoeksema, 1991). Global social functioning was assessed with the Social Adjustment Scale (SAS; Weissman and Bothwell, 1976). Recurrent depression was defined as two or more lifetime episodes (American Psychiatric Association, 1994). A General Impression (GI) five-item scale developed for the study was used to assess overall functioning at the 2-year follow-up. The five items were collapsed into two categories: 1 = well during the past year and did not meet criteria for major depression and 2 = persistent symptoms of depression or meets criteria for depression for at least 50% of the past year.
Statistical analysis
All data were analysed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Macintosh). Independent t test, chi-square test and Fisher’s exact test were used to compare baseline variables. Repeated-measures analyses of variance (ANOVAs) (one within factor ‘time’ and one between factor ‘treatment type’) were used to examine for differences in outcome by treatment modality. In the absence of difference in the change between treatment types, paired t tests were used to examine outcome for each variable of interest. Percent change and pre–post effect sizes (Cohen’s d) were also calculated. Significance was set at p < 0.05.
Results
Mean age of the sample was 36 years, and 48% were male with the gender ratio the same in the CBT and MCT groups (see Table 1). Ethnicity was predominantly New Zealand Caucasian (74%), 4% were New Zealand Maori and 22% identified as other ethnicities (Australian, European, North and South American and African). Approximately half the sample were single. Seventy-one percent of the sample reported they were employed, 18% on a benefit, 8% were students and one person (2%) self-identified as a homemaker. No significant differences between therapy groups were found on any of the demographic variables. Over three-quarters of the sample had recurrent depression and the pretreatment assessment indicated that the sample was moderately depressed. Lifetime and current comorbidity were high and at a similar level in both therapy groups (Table 1).
Demographic information, clinical status, comorbidity and psychiatric history at pretreatment for MCT and CBT groups.
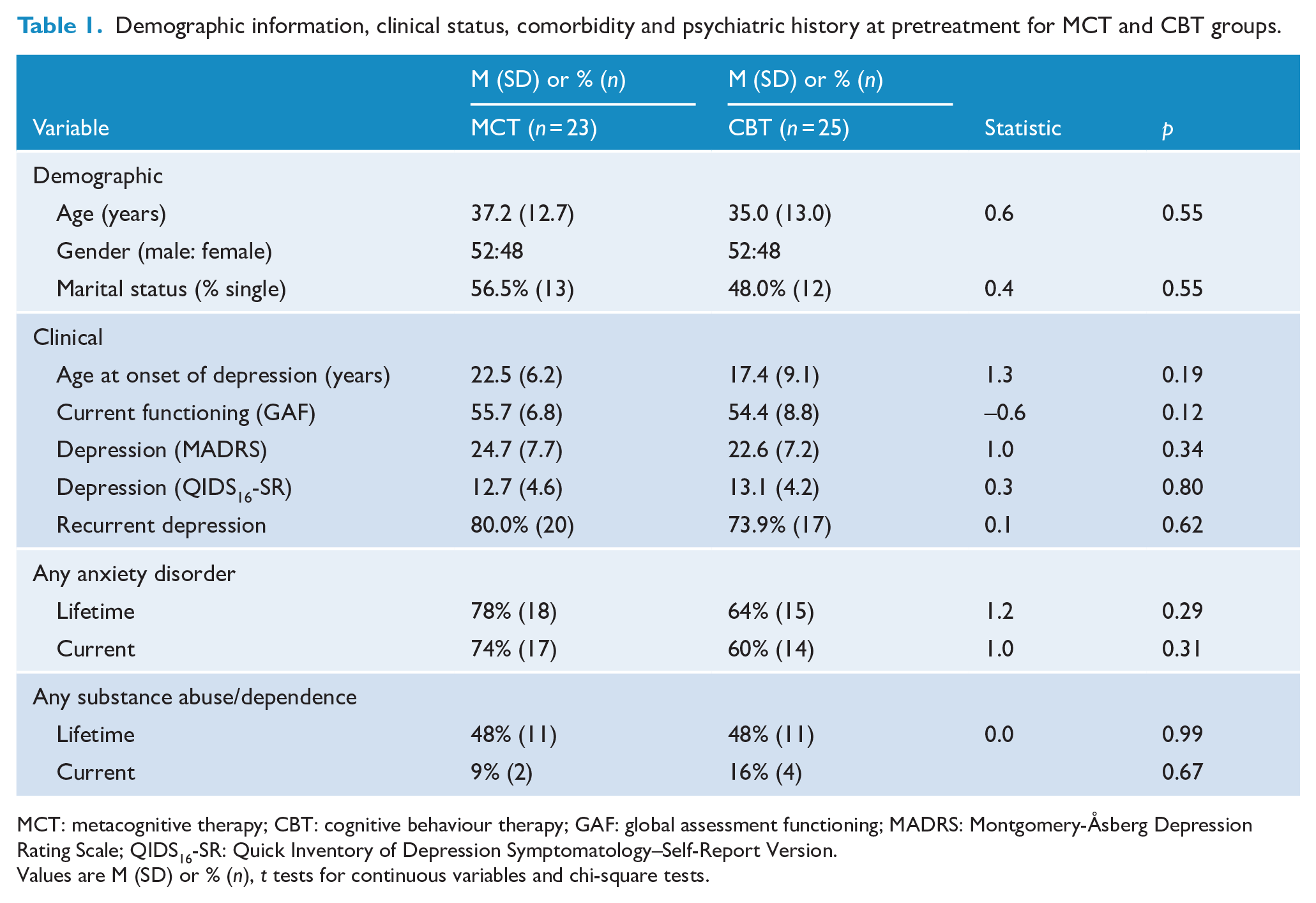
MCT: metacognitive therapy; CBT: cognitive behaviour therapy; GAF: global assessment functioning; MADRS: Montgomery-Åsberg Depression Rating Scale; QIDS16-SR: Quick Inventory of Depression Symptomatology–Self-Report Version.
Values are M (SD) or % (n), t tests for continuous variables and chi-square tests.
Analyses at baseline between those participants who subsequently completed therapy and returned follow-up questionnaires versus those who completed therapy and did not return questionnaires showed no significant differences except for anxiety. At baseline, the 31 participants who subsequently returned their 2-year follow-up questionnaires had lower anxiety than the 11 participants who did not return their questionnaires (see Table 2).
Comparison of therapy completers at pretreatment who returned and those who did not return 2-year FU questionnaires.
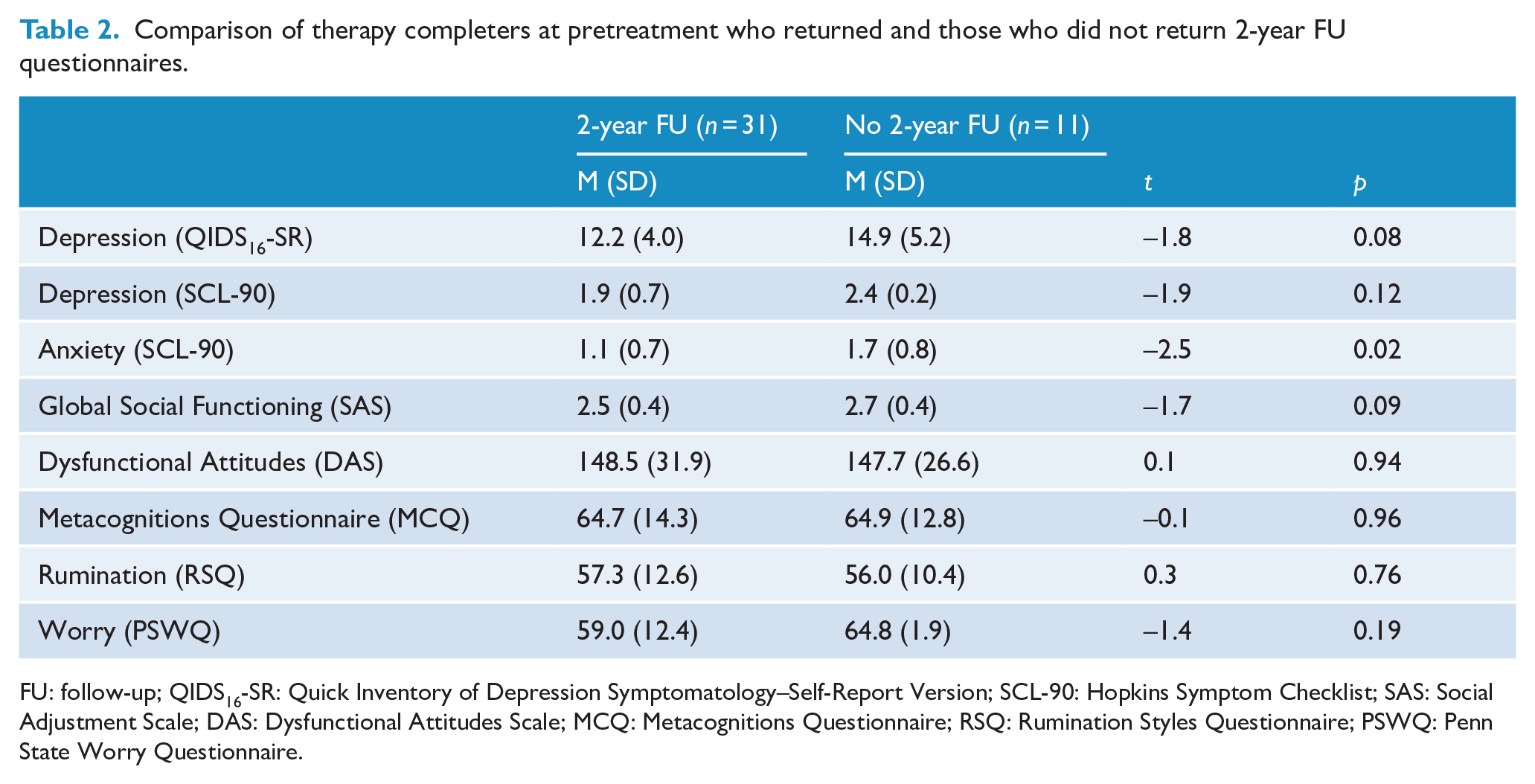
FU: follow-up; QIDS16-SR: Quick Inventory of Depression Symptomatology–Self-Report Version; SCL-90: Hopkins Symptom Checklist; SAS: Social Adjustment Scale; DAS: Dysfunctional Attitudes Scale; MCQ: Metacognitions Questionnaire; RSQ: Rumination Styles Questionnaire; PSWQ: Penn State Worry Questionnaire.
Repeated measures ANOVA for those who completed therapy indicated there were no significant therapy modality (MCT vs CBT) differences in depression or anxiety status from pretreatment to 2-year follow-up. Similarly, there were no significant therapy modality differences in the cognitive variables examined – dysfunctional attitudes, rumination, worry and metacognitions – from pretreatment to the 2-year follow-up. Finally, there were no significant therapy modality differences in social functioning from pretreatment to the 2-year follow-up. The effect sizes for the between-therapy modality differences in changes from baseline to follow-up were small (>0.35) for all variables.
Given the absence of treatment modality differences at the 2-year follow-up, paired t tests were used to examine change from pretreatment to follow-up for each variable of interest in the total sample. Percent change and pre–post effect sizes were also calculated. Overall, functioning at 2-year follow-up indicated significant improvements, with large effect sizes for all outcome variables (Table 3). The greatest change over time occurred for depression (QIDS16-SR: 44.1% change, d = 1.0; SCL depression: 50.6% change, d = 1.0) and anxiety (PSWQ: 44.4% change, d = 0.6). The percentage change on cognitive variables and clinical symptom changes were all significant with large effect sizes: metacognitions (25.2% change, d = 1.3), rumination (33.5% change, d = 1.3), dysfunctional attitudes (20.5% change, d = 0.9) and worry (19.5% change, d = 1.0). Large and statistically significant improvements were also evident for social functioning (25.2% change d = 1.3). At the 2-year follow-up, 67% (n = 20) of this group who completed therapy reported they had not experienced a major depressive episode and had been well during all of the past year prior to the 2-year assessment. Based on the cut-off 13 for the QIDS16-SR, 13% of the sample were classified as currently having a probable major depressive episode.
Change in symptomatology, cognitive and global social functioning from BL to 2-year FU for participants who completed therapy (n = 31).
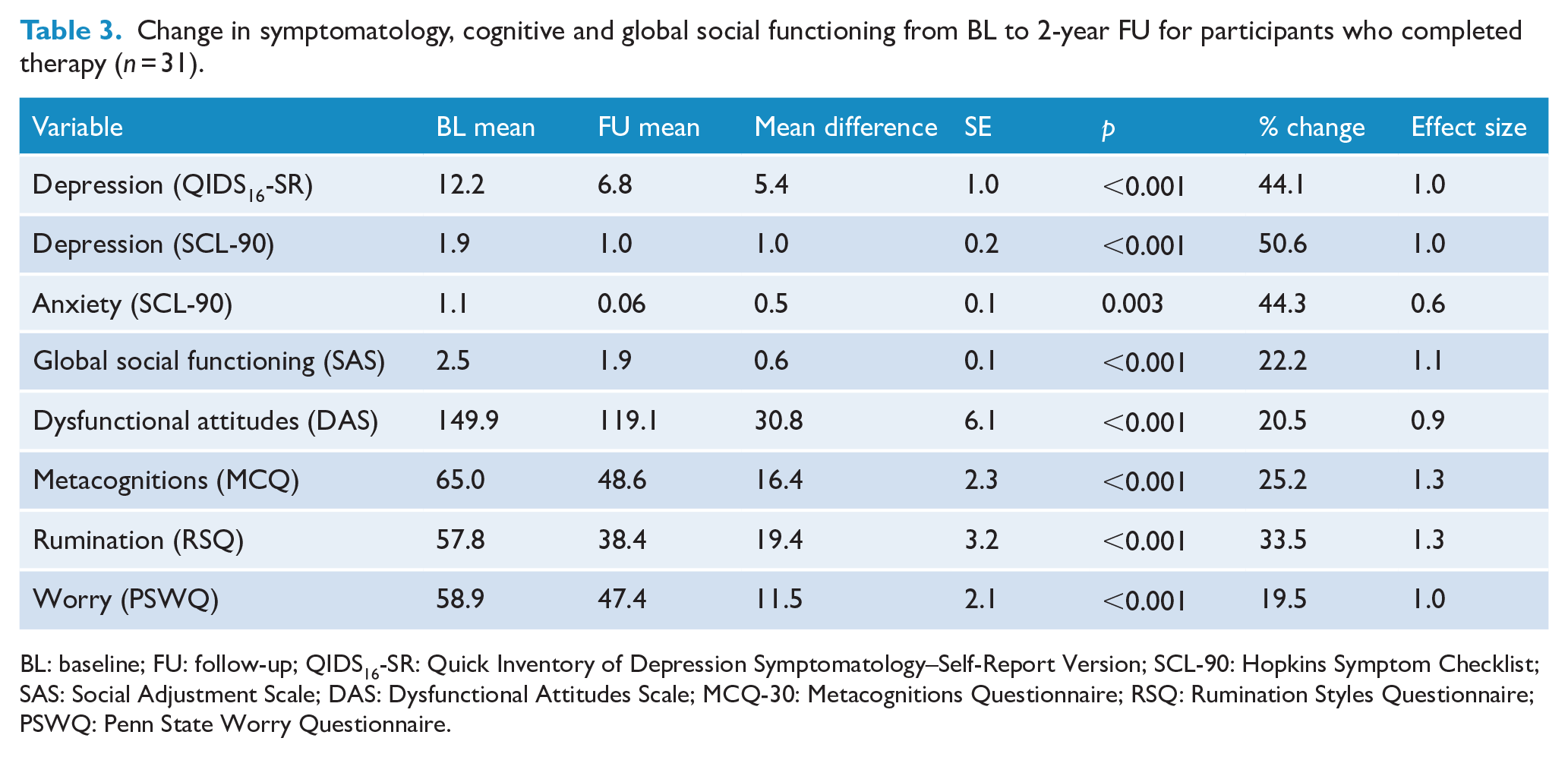
BL: baseline; FU: follow-up; QIDS16-SR: Quick Inventory of Depression Symptomatology–Self-Report Version; SCL-90: Hopkins Symptom Checklist; SAS: Social Adjustment Scale; DAS: Dysfunctional Attitudes Scale; MCQ-30: Metacognitions Questionnaire; RSQ: Rumination Styles Questionnaire; PSWQ: Penn State Worry Questionnaire.
Discussion
The aim of the current study was to examine the status of depression, anxiety and social functioning of patients 2 years (22 months after the end of treatment) after completing CBT or MCT. A secondary aim at this follow-up was to investigate whether any treatment modality differences existed in cognitive factors, specifically relevant to change in CBT and in MCT. Results of the current study indicated no significant modality differences in depression outcome for CBT and MCT. Rather, both therapies resulted in similar substantial changes in depression status, with the majority of participants not being depressed (87% based on QIDS16-SR cut-off) at 2-year follow-up.
The finding of no differences in outcome after MCT and CBT at the 2-year follow-up is consistent with the outcome findings at the end of the treatment and at the 6-month follow-up reported by Jordan et al. (2014). This result is consistent with a variety of studies and subsequent meta-analyses that do not find depression therapy modality differences in outcome, at least in the short term (Cuijpers and Gentili, 2017; Westen et al., 2004). Also consistent with some studies (Hagen et al., 2017; Hjemdal et al., 2017), all participants in the current study showed substantial positive change in anxiety status and social functioning at 2-year follow-up. This supports the notion that although therapy is targeted at depression, improvements tend to be much wider than only depression status for both CBT and MCT. Furthermore, although CBT and MCT theoretically target differing cognitive processes and take different approaches to therapy, both therapies produced positive change over time across all cognitive variables examined in the current study. Together, these findings suggest that psychotherapies such as CBT and MCT have similar general and broad, rather than specific, effects. The current study adds to a growing body of research suggesting that both CBT and MCT provide viable approaches that improve the long-term outcome of not only depression, but also anxiety, cognitive status and global social functioning (Hirschfeld et al., 2000; Lemmens et al., 2017). This latter finding is important, given problematic interpersonal functioning is strong predictor of depression relapse and greater ongoing emotional distress (Altenstein-Yamanaka et al., 2017).
While long-term follow-up research of depression therapy is important, it is not without inherent difficulties, including small sample sizes from participant attrition. The sample size for the current study was small, and although retention was good, the 2-year follow-up sample consisted of only 31 of the 42 participants who completed therapy. Long-term outcome for the 11 participants who completed therapy and did not return their 2-year follow-up questionnaires and those who dropped out early, prior to an adequate dose of therapy, other than higher levels of anxiety, remains unknown. Furthermore, the study is limited by the use of only self-report measures at the 2-year follow-up. With these caveats in mind, results suggest that CBT and MCT for depression not only significantly reduce depressive symptoms but also improve other symptomatology and cognitive and general functioning, and these improvements are evident for at least 2 years.
Poor long-term outcomes for depression are not only detrimental for the individual concerned but also lead to increased health care service utilisation and concomitant higher costs for the public health care system and the work environment. Given this, much more research needs to focus on long-term effects of psychotherapy and to compare this with pharmacotherapies. It is also important that depression treatment follow-up studies also investigate outcome over time in quality-of-life domains, not only depression status. Research on treatment modality predictors and moderators of long-term outcome would also contribute to better understanding maintenance of treatment gains or improvement over time.
Footnotes
Acknowledgements
Special thanks to the research team Professor Peter Joyce, Amanda Baird, Julia Martin, Robyn Abbott, Andrea Bartram, Yolanda Broerson, Barbara Malthus, Bridget Kimber and Megan Tucker.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article:: This work was supported by grants from the New Zealand Lottery Board Health fund and a University of Otago, New Zealand Research Fund grant.