
Abstract
Objective:
Metacognitive therapy (MCT) is one of the newer developments within cognitive therapy. This randomized controlled pilot study compared independently applied MCT with cognitive behavioural therapy (CBT) in outpatients with depression to explore the relative speed and efficacy of MCT, ahead of a planned randomized controlled trial.
Method:
A total of 48 participants referred for outpatient therapy were randomized to up to 12 weeks of MCT or CBT. Key outcomes were reduction in depressive symptoms at week 4 and week 12, measured using the independent-clinician-rated Quick Inventory of Depressive Symptomatology16. Intention-to-treat and completer analyses as well as additional methods of reporting outcome of depression are presented.
Results:
Both therapies were effective in producing clinically significant change in depressive symptoms, with moderate-to-large effect sizes obtained. No differences were detected between therapies in overall outcome or early change on clinician-rated or self-reported measures. Post-hoc analyses suggest that MCT may have been adversely affected by greater comorbidity.
Conclusions:
In this large pilot study conducted independently of MCT’s developers, MCT was an effective treatment for outpatients with depression, with similar results overall to CBT. Insufficient power and imbalanced comorbidity limit conclusions regarding comparative efficacy so further studies of MCT and CBT are required.
Introduction
Depression is a common and debilitating condition and is a leading contributor to disease burden (World Health Organization, 2004). As the best evaluated psychotherapy for unipolar depression, cognitive behavioural therapy (CBT) is recommended in treatment guidelines for depression of mild-to-moderate severity (Goldberg, 2006; Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Depression, 2004). Despite consistently demonstrated efficacy, only around half of those receiving CBT achieve remission, and relapse is common (Butler et al., 2006).
Metacognitive therapy (MCT) is one of the newer developments within CBT attempting to improve acute treatment outcomes by focussing on a different approach to cognitive processes contributing to depression. Rather than challenging the content of thoughts, as is the focus of CBT, MCT addresses factors maintaining psychological distress: metacognitions (thoughts about cognitive processes) and specific unhelpful cognitive processes called the cognitive attentional syndrome. This includes rumination, worry, threat monitoring, thought suppression, and the use of problematic affect regulation strategies such as behavioural avoidance, substance use, or binge eating.
Wells and colleagues have outlined the theory and principles of MCT (Wells, 2008b, 2009). Empirical evaluation of key theoretical elements underpinning MCT provides evidence of the importance of a ruminative thinking style in depression (Nolen-Hoeksema and Morrow, 1991; Papageorgiou, 2009; Papageorgiou and Wells, 2003; Watkins et al., 2007), the importance of positive and negative metacognitive beliefs in predicting both state and trait depression (Papageorgiou and Wells, 2001, 2003, 2009), and that an inability to take a metacognitive perspective is associated with relapse (Fresco et al., 2007; Teasdale et al., 2002).
The research evidence for efficacy of MCT for depression is promising but more studies are required to fully establish the relative effectiveness of MCT (Churchill et al., 2013). In a recent study, Wells and colleagues reported an open trial/multiple baseline study of MCT for 12 participants with recurrent depression (Wells et al., 2012). MCT achieved large effect sizes, and change was well maintained. A previous multiple baseline study (n=4) also reported that MCT was effective in treating severe and recurrent depression (Wells et al., 2009). A recent case series of four Danish patients with depression also reported clinically significant changes, maintained at follow up (Callesen et al., 2013).
Nordahl (2009) compared MCT (n=15) with CBT (n=13) in an outpatient sample with mixed psychiatric diagnoses (primarily anxiety and depression). Both therapies were effective with no difference in reduction of depressive severity scores although MCT had a superior effect in reducing anxiety symptoms and rumination.
Papageorgiou and Wells (2000) reported a single case series using their attention training technique, a key component of MCT, for four participants with moderate-to-severe depression. All were in the “not-depressed” range after very brief treatment.
Siegle et al. (2007) published a randomized controlled trial of cognitive control training (n=19) compared to treatment as usual (n=10). Cognitive control training included computerized versions of Wells and colleagues’ attention training technique as well as another cognitive strategy (Adaptive PASAT). After only six 35-min sessions over 2 weeks, participants achieved clinically significant change in depressive symptoms, greater than that achieved in the comprehensive treatment-as-usual arm over 6 weeks.
Increasingly, clinicians are using MCT after attending workshops and utilizing published treatment resources (Wells, 2009) but to date, published studies of MCT for depression include the originators or key collaborators within the research teams. This pilot study compared the speed and efficacy of independently applied MCT and CBT in outpatients with depression to inform power calculations and determine potential effect sizes for a proposed randomized controlled trial. Exploratory questions were: (1) Is MCT more effective than CBT in reducing depressive symptoms at end of treatment (12 weeks); and (2) does MCT work more quickly than CBT (change by 4 weeks)?
Methods
Recruitment was primarily through referrals from health professionals although included some self-referrals. No advertising for patients was involved. Recruitment took place between September 2009 and January 2011. This study was conducted in the Clinical Research Unit, Department of Psychological Medicine, University of Otago, Christchurch, in collaboration with the Canterbury District Health Board. This pilot study received ethical approval from the Upper South B Regional Ethics Committee, New Zealand and was registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12611000804987).
Participants
Participants were 48 men and women aged 18–65 years with a current primary DSM-IV diagnosis of major depressive disorder, bipolar II, or bipolar not-otherwise-specified-depressed who were able to converse and answer questionnaires in the English language and provide informed consent. Exclusion criteria included bipolar I disorder, schizophrenia, current severe substance abuse, use of psychotropic medication (other than the occasional hypnotic), severe physical illness, or an adequate course of CBT or MCT in the past year.
A research nurse screened referrals for inclusion/exclusion criteria and, if potentially eligible, the participant was contacted by the next available therapist and booked for a clinical interview. If eligible, informed consent was obtained.
Assessment
A comprehensive pretreatment assessment included demographic information, clinician-rated diagnostic assessments; Diagnostic and Statistical Manual of Mental Disorders-IV mood, anxiety, substance use diagnoses, and Global Assessment of Functioning (American Psychiatric Association, 2000). Clinician ratings of mood severity were made using the 16-item Quick Inventory of Depressive Symptomatology (QIDS16-C; Rush et al., 2003). QIDS16 assesses symptom domains for DSM-IV major depressive disorder. Both clinician-rated and self-report versions of QIDS16 (QIDS16-SR) were used at key time points. The Montgomery Asberg Depression Rating Scale (MADRS; Montgomery and Asberg, 1979) is a more widely used measure of depressive severity and was included for comparability with other samples. Key assessment points reported were week 0 (pretreatment), week 4, and week 12 (end of treatment). Six-month follow-up data are also reported. The final 2-year follow up is underway. Pre- and post-treatment Penn State Worry Questionnaire scores are reported to provide a measure of anxiety.
Randomization
This is a parallel trial design with equal allocation to each therapy. Computerized permuted block randomization to determine therapy allocation was undertaken by the team’s biostatistician (CF) prior to the commencement of the pilot study. Sequentially numbered envelopes were stored in a locked cabinet by an independent research coordinator and given to therapists after the pretreatment assessment was completed.
Therapy phase
The therapy was 12 sessions (permitted range 8–15) over 12 weeks. Eight sessions was set as the minimum adequate dose of therapy. Sessions were conducted twice weekly for 2 weeks, to achieve six sessions within 4 weeks to maximize early change. All four therapists (clinical psychologists) delivered both therapies. Mood and risk status were monitored weekly. If a patient deteriorated in mood or risk status or failed to improve, he or she was referred for other treatment, usually antidepressant medication, and was removed from the assessment protocol.
Therapy content
CBT was based on the manuals of Aaron T Beck (Beck et al., 1978) and Judith Beck (Beck, 1995). The key target in CBT was the specific content of negative thoughts leading to depressed feelings and to unhelpful behaviours seen in depression such as social or behavioural avoidance. Key components included orientation to the CBT model, behavioural activation (activity scheduling, pleasant event scheduling), training in the identification, self-monitoring, and challenging of negative automatic thoughts with behavioural experiments to test the validity of thoughts and provide evidence for alternative appraisals. Other skills such as problem solving were taught if necessary.
MCT followed treatment manuals by Wells (2008a, 2009) and Papageorgiou and Wells (2004). The key target in MCT was unhelpful cognitive patterns. Strategies included case conceptualization and socialization to the MCT model using key questions to explore a recent dip in mood; use of Socratic questions and behavioural experiments to challenge positive metacognitive beliefs driving selection of cognitive strategies (e.g. rumination) to serve a particular function (e.g. I need to keep focussing on my thoughts so I can understand what is wrong with me); and negative metacognitions regarding dangerousness or uncontrollability of specific thinking processes (e.g. I have lost control of my thoughts); addressing the cognitive attentional syndrome (extended conceptual processing through worry and rumination, threat monitoring, all types of avoidance – cognitive, emotional, and behavioural, including unhelpful coping behaviours e.g. substance use); the attention training task to enhance flexible control of attention; attentional refocussing away from threat monitoring (excessive scanning of mood symptoms to determine coping ability), detached mindfulness (being aware of thoughts as internal events, without engaging with them by judging, trying to control, suppress, or avoid), behavioural experiments (e.g. rumination modulation experiments, rumination postponement); and the therapy blueprint (an individualized summary contrasting old patterns of responses to triggers, with new adaptive processing plans (e.g. new metacognitive beliefs, thinking style, behaviours, attentional focus). Residual symptoms were targeted.
Therapist competence
Supervisors rated complete sets of audiotaped CBT sessions, and therapists were required to exceed the competence threshold on the Cognitive Therapy Scale for at least two cases prior to commencing protocol therapy. Although there was no competence rating scale available for MCT during the pilot study, the MCT supervisor (JC) applied a similar level of scrutiny to complete sets of audiotaped MCT sessions until a satisfactory level of competent delivery was achieved for at least two cases per therapist. During the pilot study, therapist competence and treatment integrity were addressed by weekly group supervision and monthly supervisor reviews of randomly selected audiotaped sessions for each therapist for each modality.
Treatment fidelity ratings
Independent ratings of fidelity were conducted after the pilot study was completed. Raters were two clinical psychologists and an honours year psychology student. Raters were trained using didactic lectures and read key treatment resources for both therapies. They were trained on use of an observer rating scale and rating manuals and co-rated audiotapes with the supervisor until a satisfactory level of agreement was reached (routinely scoring within 2 points on each item). The Collaborative Study Psychotherapy Rating Scale (CSPRS) was adapted by adding an MCT subscale to capture key MCT strategies and the metacognitive focus of cognitive challenges. Preliminary data were available for 115/184 tapes (63%). The therapies were able to be distinguished by trained raters blind to therapy modality. The MCT subscale was higher for those randomized to MCT (MCT 48.6±10.8 vs. CBT 22.6±1.4, t=13.6, p<0.001) and the CBT subscale was higher for those randomized to CBT (CBT 66.3±16.0 vs. MCT 34.6±4.4, t=−14.7, p<0.001).
Statistical analysis
All data were analysed using Statistical Package for the Social Sciences version 19 for Windows. Student’s t-tests were used to compare normally distributed continuous variables. For dichotomous variables, the chi-squared test was used or Fisher’s exact test where expected cell numbers were small. Paired t-tests were used to calculate pre–post effect sizes within each therapy. A general linear model was utilized to establish the effect size for the between-therapy comparisons at 4 weeks and end of treatment (week 12). Effect sizes are Cohen’s d. Outcome data are reported for intention-to-treat (ITT) using last observation carried forward (LOCF), and completer analyses. ITT analyses are based on numbers in the originally assigned groups. For completer analyses, effect sizes were based on paired t-tests so included only those with data at both respective time points. Power calculations were not made for this pilot study which was intended to establish effect sizes for the planned larger study.
The QIDS16-C was completed weekly for 4 weeks, then fortnightly. The QIDS16-SR was completed weekly. The LOCF data point came from the last available assessment completed before the participant discontinued treatment.
The primary outcome variable was reduction in depressive symptoms measured by change in QIDS16-C. Where blind ratings were unavailable, independent (nontreating clinician) ratings were used. In two cases, at end of treatment, two therapist (nonblind) ratings were used as no other raters were available. At week 0, all ratings were blind ratings and at week 12, blind ratings were available for 35/37 participants. At week 4, 12/48 ratings were blind and 32 were independent ratings.
Reliability of clinician ratings
To establish reliability for the primary outcome measure, the QIDS16, both blind rater and treating therapists separately conducted QIDS16-C interviews with each patient at baseline and at week 12. An intraclass correlation (ICC) analysis was calculated to provide an index of the reliability of the blind rater in relation to the nonblind raters. The ICC indicated a high level of agreement between raters (ICC 0.86 (95% CI 0.78 to 0.91, F 13.9, df 81, p<.001). A paired t-test indicated a consistent difference between the blind and nonblind raters of around one QIDS16 point with the blind rater scoring higher (i.e. worse depression) at both week 0 and week 12. Interrater reliability for SCID I diagnoses were not undertaken for this study; however, a previous study by this group demonstrated satisfactory reliability, with an overall kappa for lifetime Axis I diagnoses of 0.85 (overall concordance 93%, range 83–100%; Jordan et al., 2008).
Other outcome analyses
Different methods of reporting outcome status are presented to allow comparison with other studies. These include remitted status (in the nondepressed range) using the QIDS16-C and responder status using the MADRS, defined as greater than 60% reduction in severity from pre- to post-treatment. The 60% reduction threshold has previously been found to offer an optimum balance of specificity and sensitivity in defining responder status (Mulder et al., 2003).
Results
Patient flow
Patient flow is presented in Figure 1. The final sample included 48 participants (MCT n=23, CBT n=25). Dropout rate did not differ between therapies; two participants within each therapy withdrew before the minimum eight sessions (completer status threshold). A total of 37 participants (MCT n=18, CBT n=19) completed at least part of the week-12 end assessment. Between session eight and the end assessment at week 12, seven participants dropped out or were withdrawn for the following reasons; started antidepressants (n=2), psychiatric admission after a suicide attempt (n=1), unilateral withdrawal (n=2), and earthquake disruption (n=2). The median number of sessions was 11.5 (range 3–15) and did not differ between therapies. Six-month follow-up assessments were completed by 19 in the MCT group (83%) and 21 in the CBT group (84%).
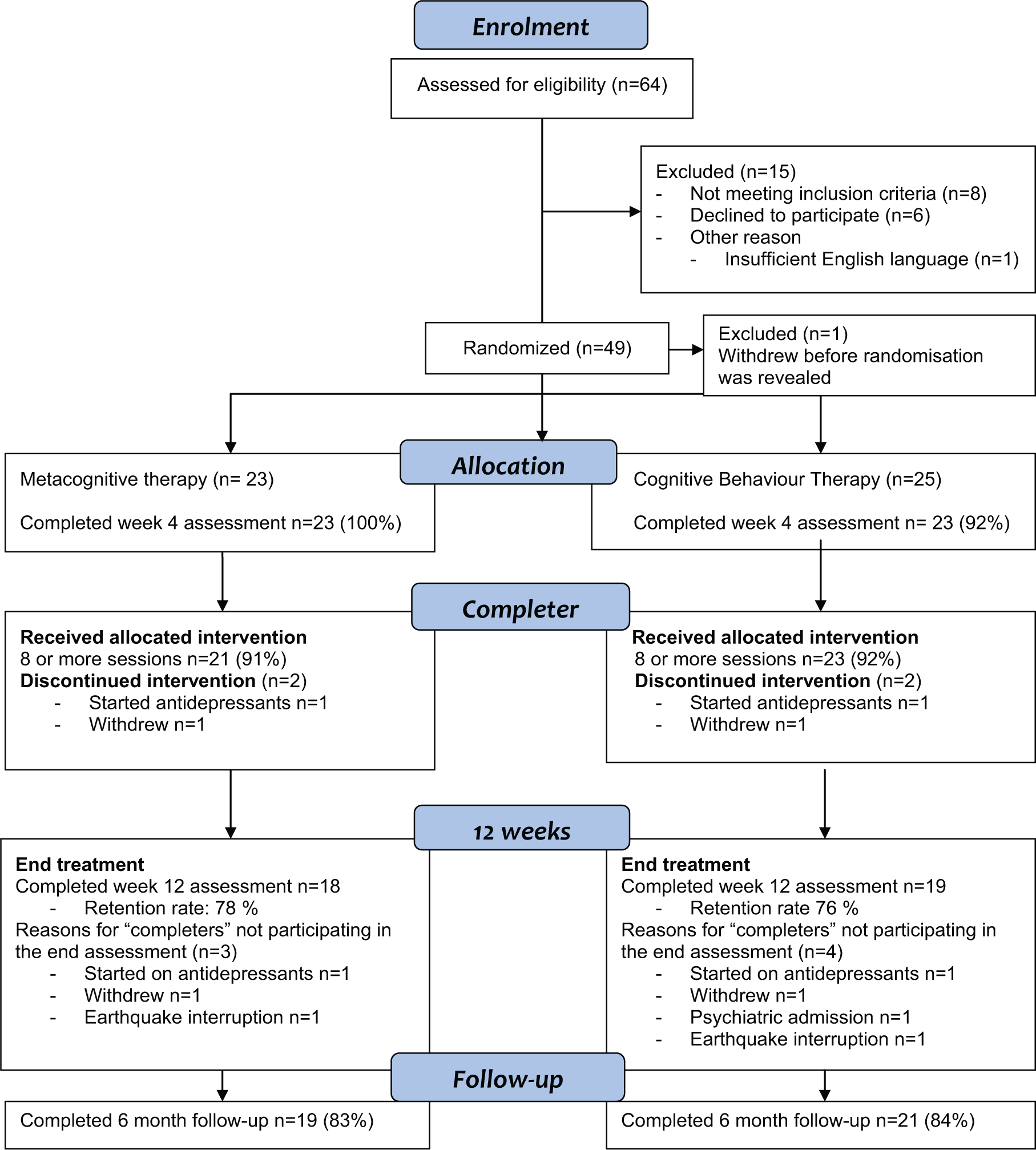
Patient flow in the pilot study for depression.
Table 1 presents pretreatment characteristics of the sample. The age of the sample was (mean±SD) 36±12.8 years (range 18–68 years) and the gender ratio was almost equal (males 52%, females 48%). Ethnicity was predominantly New Zealand Caucasian (67%), with 10% New Zealand Maori. A significant minority of participants were born outside New Zealand (23%), including participants from Australia, Europe, North and South America, and Africa, and 48% were married or in a stable de facto relationship, 44% had never married, 6% were separated, and 2% divorced. The number of education years was 14.5±2.6 years, and 71% were employed, 18% received a social welfare benefit, 8% were students, and one person (2%) self-identified as a housewife. There were no statistically or clinically significant differences between groups for any demographic variables. The sample was moderately depressed at the initial assessment, had on average three prior depressive episodes, and most participants reported chronic symptoms over the past 5 years.
Pretreatment functioning and psychiatric comorbidity in metacognitive therapy and cognitive behavioural therapy groups.
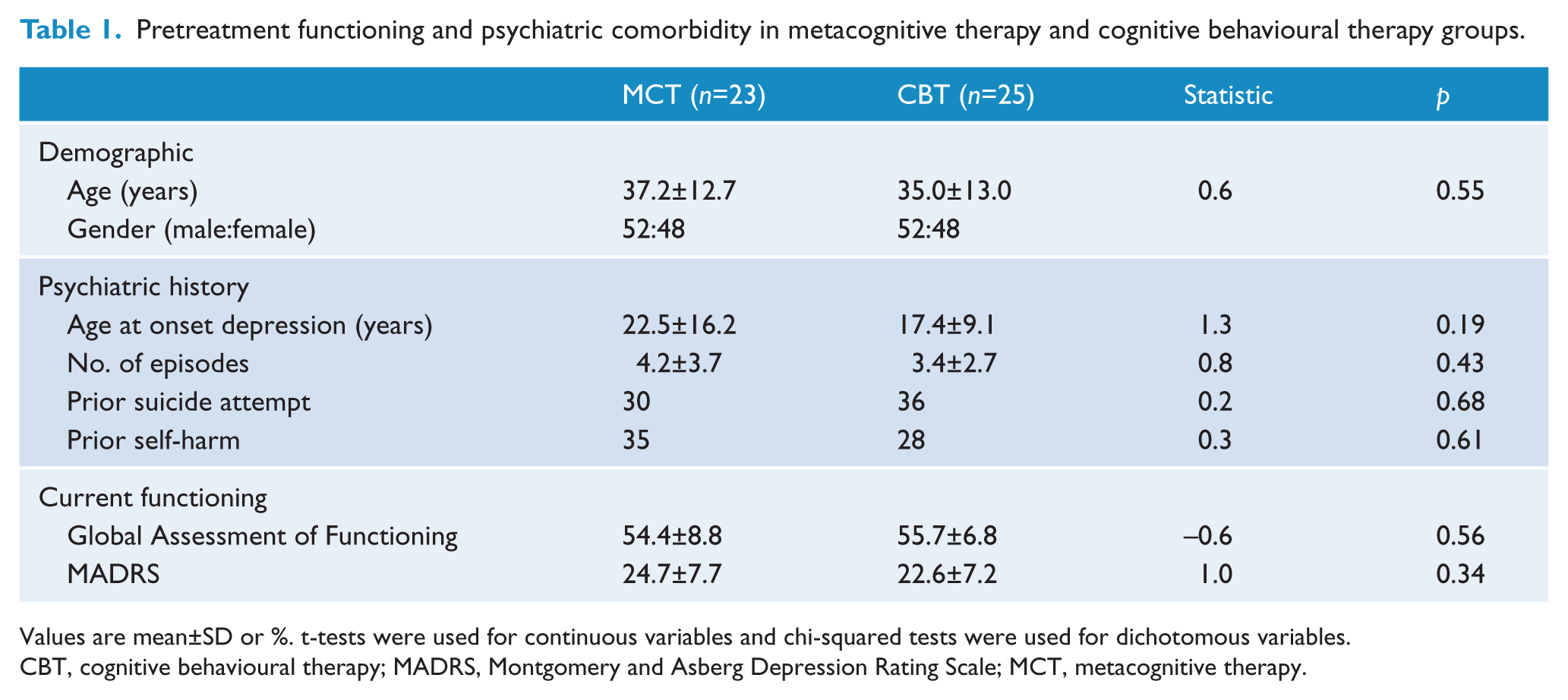
Values are mean±SD or %. t-tests were used for continuous variables and chi-squared tests were used for dichotomous variables.
CBT, cognitive behavioural therapy; MADRS, Montgomery and Asberg Depression Rating Scale; MCT, metacognitive therapy.
Table 2 presents comorbid psychiatric diagnoses. Comorbidity was highly prevalent in both groups. Although the MCT prevalence for social phobia was much higher (48%) than for CBT (28%), there were no statistically significant differences between groups for this or any current or lifetime comorbid disorder.
Psychiatric comorbidity in metacognitive therapy and cognitive behavioural therapy groups.
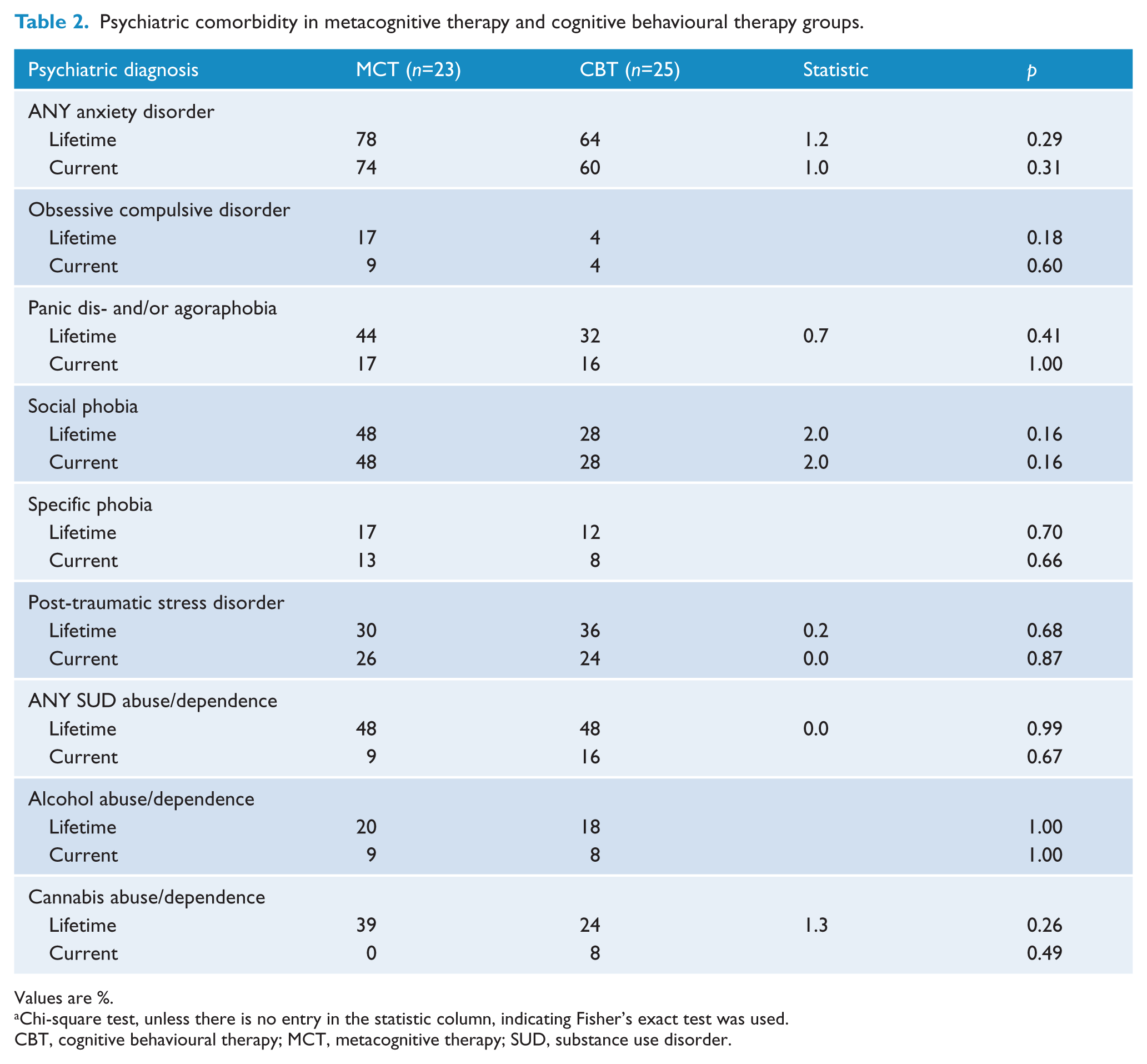
Values are %.
Chi-square test, unless there is no entry in the statistic column, indicating Fisher’s exact test was used.
CBT, cognitive behavioural therapy; MCT, metacognitive therapy; SUD, substance use disorder.
Changes in depressive scores over treatment are illustrated for both blind clinician-rated (Figure 2) and self-report (Figure 3) depression scores (ITT analyses). Outcome data are reported in Table 3 for ITT and completer analyses for both clinician-rated and self-report versions of the QIDS16. Using ITT, participants in both therapies demonstrated clinically significant improvements on the primary outcome variable, QIDS16-C, at week 4 (MCT d=0.74, 95% CI 0.30 to 1.17; CBT d=0.73, 95% CI 0.31 to 1.14) and at end of treatment (MCT d=1.03, 95% CI 0.60 to 1.46; CBT d=1.03, 95% CI 0.61 to 1.44). There were no significant differences between therapies for the ITT analyses at either week 4 (d=0.06, 95% CI −0.65 to 0.52) or end of treatment (d=0.04, 95% CI −0.62 to 0.54) (Table 3).
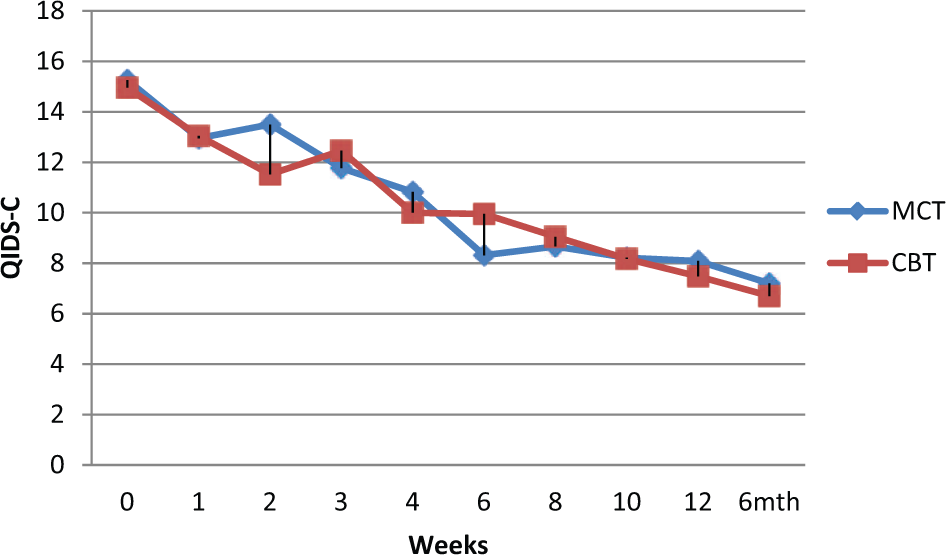
Clinician-rated QIDS16 depression severity scores over treatment and at 6-month follow up.
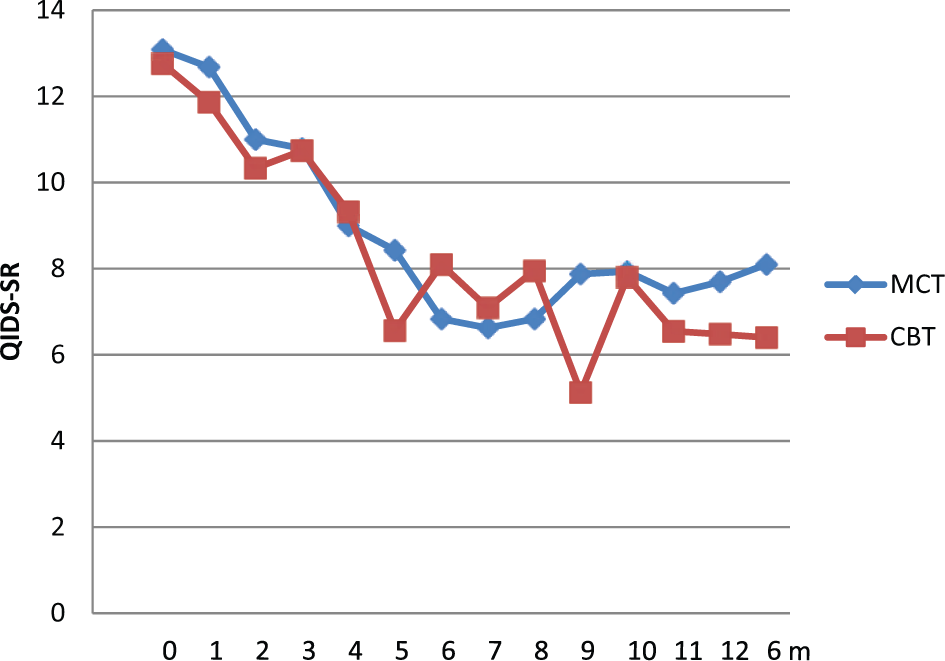
Self-rated QIDS16 depressive severity scores over treatment and at 6-month follow up.
Treatment outcome for metacognitive therapy and cognitive behavioural therapy groups.
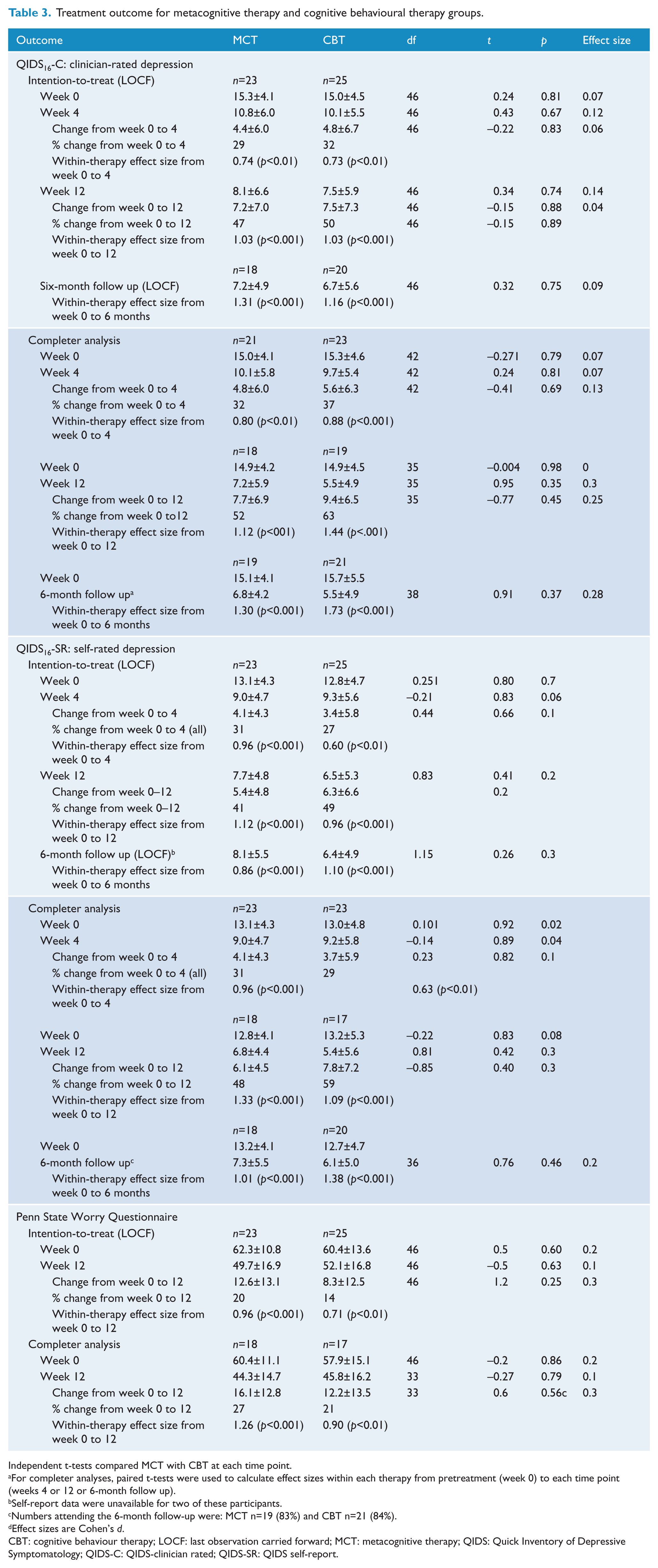
Independent t-tests compared MCT with CBT at each time point.
For completer analyses, paired t-tests were used to calculate effect sizes within each therapy from pretreatment (week 0) to each time point (weeks 4 or 12 or 6-month follow up).
Self-report data were unavailable for two of these participants.
Numbers attending the 6-month follow-up were: MCT n=19 (83%) and CBT n=21 (84%).
Effect sizes are Cohen’s d.
CBT: cognitive behaviour therapy; LOCF: last observation carried forward; MCT: metacognitive therapy; QIDS: Quick Inventory of Depressive Symptomatology; QIDS-C: QIDS-clinician rated; QIDS-SR: QIDS self-report.
The same pattern of results of clinically significant changes within each treatment but negligible differences between treatments at each time point was found for completer analyses for QIDS16-C scores and for each set of analyses for QIDS16-SR scores (Table 3). Effect sizes for completer analyses for QIDS16-C at week 4 were MCT d=0.80 (95% CI 0.34 to 1.25) and CBT d=0.88 (95% CI 0.45 to 1.31) and at end of treatment were MCT d=1.12 (95% CI 0.62 to 1.61) and CBT d=1.44 (95% CI 0.96 to 1.93). Effect sizes for ITT analyses for QIDS16-SR at week 4 were MCT d=0.96 (95% CI 0.52 to 1.39) and CBT d=0.60 (95% CI 0.18 to 1.00) and at end of treatment were MCT d=1.12 (95% CI 0.69 to 1.55) and CBT d=0.96 (95% CI 0.54 to 1.37). Effect sizes for completer analyses for QIDS16-SR at week 4 were MCT d=0.96 (95% CI 0.52 to 1.39) and CBT d=0.63 (95% CI 0.20 to 1.07) and at end of treatment were MCT d=1.33 (95% CI 0.84 to 1.83) and CBT d=1.09 (95% CI 0.57 to 1.60) (Table 3).
At end of treatment, there were no significant differences between therapy groups using the additional methods of examining outcome. Similar numbers of participants were in the nondepressed range on the QIDS16-C (MCT 43.5%, CBT 44%, chi-squared 0.001, p=0.97). A further measure of treatment response was a greater than 60% reduction on the MADRS. Those meeting this response criterion for each therapy were MCT (52%) and CBT (44%) (chi-squared 0.32, p=0.57).
Six-month follow-up data indicated that changes were maintained but again there were no statistically significant differences between therapies for any of the analyses.
Pre–post results for anxiety measured by the Penn State Worry Questionnaire are presented in Table 3. Anxiety levels reduced in both therapies over treatment but there were no statistical differences between therapies at any time point. Within-treatment effect sizes indicated large effect sizes for MCT, especially for the completer analyses (ITT d=0.96, completer analysis d=1.26).
Post-hoc subgroup analyses
Exploratory post-hoc analyses were undertaken to better understand the sizable difference in within-therapy effect sizes (MCT d=0.96, CBT d=0.60) at week 4 for the QIDS16-SR, despite the lack of significant differences between treatments at pretreatment or week 4. This was explained by greater variability in the change scores within the CBT group by week 4: 32% in the CBT group had worse scores (any change in the wrong direction) on the QIDS16-SR (ITT) compared with 4% in the MCT group (Fisher’s exact test, p<0.02).
The three participants with a bipolar diagnosis (two with bipolar II and one with bipolar not-otherwise-specified were all in the MCT group. The primary outcome analyses were re-run with those participants excluded. There were small positive changes in the MCT means, but there were still no statistically significant differences between therapy modalities on any of the primary outcome analyses at any time point. For example, for the primary outcome, the ITT QIDS16-C analyses, the data (mean±SD) with bipolar II/not-otherwise-specified excluded were as follows: week 0: MCT 15.6±4.1 vs. CBT 15.0±4.5 (t=0.49, p=0.83); week 4 MCT 10.7±5.8 vs. CBT 10.1±5.5 (t=0.31, p=0.76); week 12 MCT 7.2±5.9 vs. CBT 7.5±5.9 (t=−0.16, p=0.88). The pre–post percentage change was MCT 51% vs. CBT 47%. This difference was not statistically significant (t=0.13, p=0.90).
The disproportionate prevalence of social phobia in the MCT group (48% vs. CBT 28%) was a potential confounder. Key analyses were rerun with all those with current social phobia excluded from both groups. This substantially reduced the power to detect differences as the groups (particularly MCT) were much smaller (MCT n=12/23, CBT n=18/25). There were no significant differences for the QIDS16 clinician-rated or self-report measures at weeks 0, 4, or 12; however, the outcomes were better in both therapies. Using the MADRS responder outcome measure (>60% improvement), the percentage classified as responding in MCT improved from 52% in the original analyses to 83% in analyses excluding those with social phobia, while the CBT group did not change (44%). This result was statistically significant (chi-squared 4.54, p=0.03). A similar pattern was observed on the other outcome measure, nondepressed status on the QIDS16: the MCT group changed to 66.7% remitted and the CBT to 44.4%; however, this was not statistically significant (chi-squared 1.43, p=0.23).
Discussion
The aim of this pilot study was to compare MCT with CBT for outpatients with depression to establish effect sizes for power calculations for a proposed randomized controlled trial. Exploratory research questions concerned speed and efficacy of MCT in relation to CBT. Large effect sizes were achieved for both therapies. On the primary analyses, MCT was not more effective than CBT at end of treatment on any clinician-rated or self-report depression outcome measure and was not faster in reducing depression severity by week 4. However, the pilot study was underpowered to detect differences, and the disproportionate prevalence of social phobia in the MCT group is likely to have impacted on these results.
Notwithstanding the power issue noted above, the failure to find a difference in effectiveness between MCT and CBT for depression is consistent with results of one previous study of those with mixed diagnoses (Nordahl, 2009). In that study, both therapies were effective in reducing depression severity, although MCT was better at reducing anxiety in those with comorbid anxiety symptoms. Although the impact on anxiety levels was not significantly different between therapies in the present study due to insufficient power, the pattern of results was similar, suggesting that MCT may have added benefit for those with anxiety.
The large pre–post effect sizes achieved in the current study for CBT (clinician-rated d=1.03; self-report d=0.96) fall within the ranges reported in other published studies of CBT for depression (Beck and Dozois, 2011; Butler et al., 2006; Cuijpers et al., 2008; Dobson, 1989; Lambert and Ogles, 2004). Effect sizes reported for MCT for depression by Wells and colleagues are larger (1.83; Wells et al., 2012) than the effect sizes reported here (1.03 for clinician-rated, 1.12 for self-report). It has been suggested that therapy developers achieve larger effect sizes than independent investigators typically achieve in effectiveness studies (Cuijpers et al., 2010; Kliem et al., 2010). Failure to replicate those large effects in MCT here may relate to therapist competence and/or allegiance, as well as sample composition.
Participants in the current study were similar in age and extent of comorbidity to previous outpatient samples treated in our clinical research unit (e.g. Luty et al., 2007) although there was a higher prevalence of post-traumatic stress disorder in the current study. The latter finding was almost certainly related to the Christchurch earthquakes of 2010–2011 which occurred during this study. Participants in previous MCT studies for depression have had chronic, usually moderate, depressive symptoms and were taking antidepressants and/or other psychotropic medications (Nordahl, 2009; Siegle et al., 2007; Wells et al., 2009, 2012) whereas participants in the current study were medication free. Previous studies of MCT (Nordahl, 2009; Wells et al., 2009, 2012) excluded those with substance addiction, whereas participants were included in the current study provided the substance use disorder was not severe or the primary diagnosis. These factors may have contributed to the relatively smaller effect sizes.
Limitations
The current study has a number of limitations. This pilot study was not expected to have sufficient power to detect statistically significant differences for the therapy comparison but was intended to provide valuable data regarding treatment effect sizes for power calculations of the sample size needed for a larger randomized controlled trial. Failure to find a significant difference is not evidence of equal efficacy, which can only be determined by an equivalence design with typically a very large sample size.
Although therapists and supervisors involved in this pilot study attended at least one training workshop by Wells, were closely supervised, and followed the MCT therapy manual, these therapists did not have the opportunity to attend intensive training such as that now offered by the Metacognitive Institute, and the therapy was not supervised by Wells, Papageorgiou, or their colleagues. As such, MCT in this pilot study may not have been exactly as the originators would deliver. It is likely, however, to represent the way that clinicians across the world would implement a therapy such as MCT after attending training courses offered by therapy originators. Independent application of a therapy is an important step in establishing real-world effectiveness.
Formal competence ratings were not made during the pilot study and no competence measures for MCT were available. However, competence ratings in other trials by this group indicate that our therapists (some of whom overlap with this study) maintained scores above the competence threshold for CBT throughout those trials (Carter et al., 2013; McIntosh et al., 2013).
All therapists delivered both therapies. Although this controls to some extent for nonspecific therapist factors, there is also potential for reduced fidelity. Therapists had been trained originally in CBT and had learned MCT subsequently. As such, it could be argued that they may have had a greater therapeutic allegiance to and competence in CBT relative to MCT; however, these results do not support that argument. It has been suggested the mechanism of change in CBT might be due to adopting a metacognitive stance after having challenged common negative automatic thoughts, rather than thought challenging per se being the primary mechanism of change (Teasdale et al., 2002). It is also possible that delivery of MCT might have primed therapists to assist CBT patients in adopting a metacognitive approach. A more in-depth analysis of therapist fidelity and competence, as well as other therapy process factors, is underway.
MCT is reported to work rapidly, with the number of sessions in MCT for depression being typically 5–7 sessions. No difference between therapies was detected here for speed of change or the number of sessions attended; however, presetting minimum and maximum treatment parameters to match our standard treatment length for CBT may have influenced the number of sessions in MCT.
The sample was not stratified for variables such as comorbidity or prior depressive history at baseline. Although most variables did not differ between groups, the disproportionate burden of comorbidity in the MCT group, particularly for social phobia may have adversely affected the MCT results, posing a methodological issue.
The current study has a number of strengths. With a sample size of 48, this is a large pilot study collecting comprehensive pretreatment data using standardized well-validated measures, with reliability data reported for the primary outcome measure and fidelity data indicating therapy distinctiveness. ITT and completer analyses are reported along with several alternative outcome measures (responder and nondepressed status). Reporting multiple measures of outcome allows comparison with existing studies (Hiller et al., 2011).
Conclusions
This is the largest study of MCT for depression and, to our knowledge, the only randomized pilot study to date of MCT with CBT for those with depression as the primary presenting problem. Both therapies were effective in reducing depressive (and anxiety) symptoms by end of treatment. This finding is noteworthy as MCT was applied here independently of the originators, and the MCT group suffered from a greater burden of comorbidity. These preliminary data suggest that MCT may offer another useful therapy option. Further comparative studies of MCT and CBT are required with sufficiently large sample sizes to answer questions of relative efficacy and to allow for stratification of potentially confounding variables associated with severity. Future research should also examine possible differential predictors of response in MCT and CBT such as the level of rumination, specific anxiety symptoms, treatment acceptability, therapy process, and mechanisms of change.
Footnotes
Acknowledgements
We thank Amanda Baird and Joanna Vallance, therapists on this study, and Julia Martin, Robyn Abbott, Andrea Bartram, Yolanda Broerson, Barbara Malthus, Bridget Kimber, and Megan Tucker for their invaluable assistance.
Funding
This work was supported by the New Zealand Lottery Board Health Fund (grant no. 279032) and the University of Otago Research Fund (grant no. ORG0109-0310).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.