
Abstract
Objectives:
Both antidepressant medications and psychological therapy are common treatments for depression in postpartum women. Antidepressant treatment may have a number of practical disadvantages, including a preference by women to avoid medication while breastfeeding. Consequently, more information about the relative benefits of the two modalities in the perinatal period is helpful. In the treatment of depressive disorders there is some evidence that combination therapies (pharmacological plus psychological treatment) may be more efficacious than either form of mono-therapy in isolation. However, in the treatment of postnatal depression, such evidence is limited.
Method:
Forty five postpartum women with a DSM-IV diagnosis of depression were randomised to receive either: 1) cognitive behavioural therapy (CBT); 2) sertraline, or 3) a combination of both treatment modalities. Psychometric measures were collected weekly for 12 weeks, with a follow-up at 24 weeks.
Results:
Symptoms of depression and anxiety were reduced to a significant degree following all three treatments. CBT mono-therapy was found to be superior to both sertraline mono-therapy and combination therapy after 12 weeks. The CBT mono-therapy group appeared to display the most rapid initial gains after treatment commencement.
Conclusions:
In this sample, a specialised CBT program for postnatal depression was found to be superior as a mono-therapy compared to sertraline, a commonly prescribed SSRI antidepressant. This is in contrast to previous studies which have found no detectable difference in the efficacies of drug and psychological treatment for postnatal depression. Unlike some previous work, this study allowed a statistically independent evaluation of CBT mono-therapy for postnatal depression compared to both antidepressant and combination therapy. In line with previous studies in postpartum women, there was no detectable advantage of combining pharmacological and psychological treatments in the short term.
Introduction
The best available meta-estimates suggest that postnatal depression (PND) affects approximately 13% of women at three months after childbirth (Gavin et al., 2005; O’Hara and Swain, 1996), with long-term consequences for women and their infants (Halligan et al., 2007; Murray et al., 2011). In general, meta-analyses of depression treatment trials conclude that antidepressant medication and psychological treatments both have clinical efficacy (Cuijpers et al., 2008). For PND, good evidence exists for the efficacy of psychological interventions (Dennis and Hodnett, 2007). By contrast, the evidence base relating to pharmacotherapy for PND has emerged only slowly, preventing clear conclusions being drawn (De Crescenzo et al., 2014; di Scalea and Wisner, 2009; Hoffbrand et al., 2001).
A handful of small, placebo-controlled randomised trials have confirmed clinical effects for specific serotonin reuptake inhibitors (SSRIs) including paroxetine and fluoxetine in postnatally depressed women (e.g. Appleby et al., 1997; Yonkers et al., 2008). There have also been a number of ‘open-label’ trials of various antidepressants in treating PND (e.g. Cohen et al., 2001; Nonacs et al., 2005; Suri et al., 2005; Suri et al., 2001) and trials evaluating SSRI antidepressants against active comparators from the older class of tricyclic medications (Wisner et al., 2006). It has been suggested that the SSRIs, and in particular sertraline, may be suitable where an antidepressant is required in the treatment of PND, due to reports of mild side effect profiles, and relatively low levels of excretion in breast milk (di Scalea and Wisner, 2009; Epperson et al., 2001; Weissman et al., 2004).
For depression in the general population, there is some support for the efficacy of combining antidepressant medications with psychological treatment (de Matt et al., 2007). However, while concomitant pharmacotherapy may confer some increase in efficacy over psychological treatment alone, it is unclear whether the differences found are clinically relevant and whether there is longer-term maintenance of the short-term gains (Cuijpers et al., 2009). Interestingly, where the psychological component of combination therapy is CBT, the addition of an antidepressant appears to make the smallest difference to outcomes (de Matt et al., 2007).
For PND, existing studies of combination therapy report no benefit of combining SSRIs with psychological therapy (Appleby et al., 1997; Bloch et al., 2012; Misri et al., 2004). Appleby et al. (1997) reported the results of a placebo-controlled study of fluoxetine and cognitive behavioural counselling in the treatment of PND. Fluoxetine, or six sessions of counselling, were found to be similarly effective treatments and no additive benefit of combining these treatments was found. Misri et al. (2004) reported paroxetene alone and in combination with CBT as comparable in efficacy. More recently, Bloch et al. (2012) found no benefit in combining sertraline with brief dynamic psychotherapy. No study of combination therapy for PND has thus far found any additive benefit in reducing depressive symptoms, in contrast to previous work in general adult populations (e.g. Keller et al., 2000). Given the preference of many (but not all) postnatal women for non-pharmacological treatment while breastfeeding (Boath et al., 2004; Dennis and Chung-Lee, 2006; O’Mahen and Flynn, 2008), further establishing both speed of recovery and the comparative efficacy of mono-therapy versus combined therapy is highly relevant in perinatal populations to allow a considered balancing of risks versus benefits. One larger pragmatic trial of psychological intervention versus medication (n = 254) suggested that antidepressants may act more rapidly than non-directive counselling for PND, a potentially important clinical advantage (Sharp et al., 2010). Recent reviews have pointed out that more research is needed in this area, especially randomised controlled trials with longer follow-up periods (De Crescenzo et al., 2014; O’Hara and McCabe, 2013).
The aim of this study was to compare the relative efficacy of mono-therapy with an SSRI (sertraline), CBT mono-therapy and combined treatment at reducing symptoms of depression and anxiety and to monitor the trajectory of depressive symptoms in each group weekly for the first 12 weeks of treatment. In addition, we measured the effect of the different treatments on parenting-related stress.
Our choice of psychological treatment draws on research that supports the effectiveness of cognitive behavioural therapy (CBT) for depression in general. About two-thirds of participants in CBT trials are no longer diagnosed with depressive disorders at follow-up and have a reduced risk of relapse (Gloaguen et al., 1998). Therapeutic benefit accrues particularly to individuals with mild to moderate depression (Clarke et al., 2005). While there are very few CBT interventions specifically adapted for postnatal depression, those that exist also support the effectiveness of CBT (Appleby et al., 1997; Cuijpers et al., 2008; Dennis and Hodnett, 2007). In previous randomised trials, we evaluated a structured 12-week group cognitive behavioural therapy (CBT) program designed specifically for women suffering PND and found our treatment was successful at lowering depressed mood in a sample of moderately depressed women (Meager and Milgrom, 1996; Milgrom et al., 2005). The program was both superior to a group counselling intervention and to routine care. Similarly, Cooper and colleagues reported improvement with CBT treatment for PND (Cooper et al., 2003). Findings with CBT treatment are consistent with psychological treatment trials of PND in general (not limited to CBT) (Cuijpers et al., 2008; Dennis and Hodnett, 2007). However, most research on PND to date has focused on maternal mood, despite evidence that PND is also accompanied by significant levels of stress related to the parenting role (Milgrom et al., 2006) that is largely unalleviated by identification and treatment of maternal depression (Myers et al., 2013).
Method
Design
The study was a parallel 3-group randomised controlled trial (RCT). To assess the timing of improvement in depressed mood, psychometric assessment of depression symptoms was repeated weekly for 12 weeks (the treatment period for the CBT therapy). Follow-up occurred at 24 weeks. The trial is registered at clinicaltrials.gov (trial number NCT02122393) and was approved by the Human Research Ethics Committee of Austin Health.
Participants
Women were assessed for possible PND through a community screening program in Maternal and Child Health Centres in Melbourne, Victoria. Most were attending a routine 12-week postnatal check-up, and all were screened with the Edinburgh Postnatal Depression Scale (EPDS: Cox and Holden, 2003). The EPDS is purposely designed as a screening instrument for depression in postnatal women. This brief self-report instrument has adequate sensitivity when tested against clinical interview and has good acceptability (Gemmill et al., 2006). The EPDS is the most widely used screening tool for postnatal depression and a cut-off score of ⩾ 13 is widely used to indicate possible depression (Gibson et al., 2009).
Procedure
Women with an EPDS score of ⩾ 13 were offered referral to the study and informed consent was obtained. Those who consented were assessed by a psychologist or by a psychiatry registrar using a standardised psychiatric interview to confirm a DSM-IV diagnosis of a depressive disorder – the Composite International Diagnostic Interview (CIDI: WHO, 1993). Demographic and Background Information was collected during the interview and included: age, occupation, marital situation, employment status, housing and language group.
Women receiving a DSM-IV diagnosis of depressive disorder received a full medical examination by a medical practitioner. This occurred for all potential participants prior to treatment allocation, in order to rule out any underlying or undiagnosed medical conditions and included a full physical exam and a serum pregnancy test.
Women were included if they: were between 19 and 40 years of age and had an infant > 2 months and < 8 months of age, born after a full-term pregnancy, with no congenital abnormalities; a screening EPDS score of ⩾ 13; DSM-IV diagnosis of a depressive disorder with postnatal onset. Women were excluded from the trial if they had: a positive serum pregnancy test; a concurrent psychiatric disorder (excepting co-morbid anxiety); a recent history of antidepressant usage (within the last month); a history of major allergy or drug allergy; a history of substance abuse; prior non-response to sertraline, or prior non-response to adequate trials of two SSRIs; a predisposition to headache, migraine or nausea; tobacco habit in excess of 10 cigarettes per day; caffeine consumption in excess of 6 cups of coffee/tea or cola-flavoured drinks per day; ongoing dental work; extreme levels of depression (psychotic); or suicidal intent. Women were also excluded if they had taken part in any medical trial within the previous three months; or if they were unwilling a priori to engage in either of the mono-therapies or in the combination therapy.
Outcome measures
Depression, anxiety and stress were assessed using the following measures at three major timepoints: prior to randomisation and again at 12 and 24 weeks (hereafter referred to as Baseline, Time 1 and Time 2, respectively).
The Beck Depression Inventory-II (BDI-II: Beck and Steer, 1987) is a widely used, well-validated, 21-item clinical instrument that measures cognitive, affective and physiological symptoms of depression. It has well-validated psychometric properties (Beck et al., 1996). A score of > 14 indicates presence of depression (14–19: mild, 20–28: moderate, 29–63: severe). In addition, as the BDI-II was the central clinical measure of depressive symptoms in this study, it was given weekly from Baseline to Time 1 to more closely monitor rate of progress.
The Beck Anxiety Inventory (BAI: Beck et al., 1988) consists of 21 descriptive statements of anxiety symptoms on a 4-point scale and yield a measure of overall anxiety (0–7: minimal level of anxiety, 8–15: mild anxiety, 16–25: moderate anxiety, 26–63: severe anxiety). The BAI was administered at Baseline, Time 1 and Time 2.
The Parenting Stress Index (PSI: Abidin, 1986) comprises 101 items measuring parent–child relationship functioning, level of dysfunctional parenting behaviour and child behaviour problems. Responses to items are totalled to produce seven ‘Child Domain’ and six ‘Parent Domain’ subscales, which are totalled to yield overall scores for each domain. Domain scores are summed to yield a total PSI score – scores > 260 reflect clinically significant levels of parenting dysfunction. The PSI was administered at Baseline, Time 1 and Time 2.
Randomisation
Consenting, eligible women were allocated to treatments at random in a 1:1:1 ratio. A variable-length permuted blocks randomisation schedule, generated and administered by an independent person, was prepared prior to commencement of the trial and operated via telephone.
Treatment conditions
CBT mono-therapy
The specialised CBT group treatment for postnatal depression followed a manualised, replicable treatment (Milgrom et al., 1999; Milgrom et al., 2005), conducted over 12 weeks at weekly intervals including 5–10 mothers per group. Nine sessions were provided for women and a further three ‘couple sessions’ (i.e. including the women’s partners). Sessions were supported by subsidised childcare to better enable attendance.
Sertraline mono-therapy
Women randomised to sertraline (Zoloft, Pfizer Inc) were commenced on the standard recommended initial dose (50mg) for two days. Further increases were at the discretion of the prescribing psychiatry registrars on an individual basis, up to 200mg/day.
CBT + sertraline (combination therapy)
Women randomised to this condition began medication as per the sertraline mono-therapy group, and also attended group CBT as per the CBT mono-therapy group.
Treatment compliance
Subsequent medical reviews occurred 1, 2, 4, 6, 8, 12 and 24 weeks after entry and included monitoring of symptoms as well as medication compliance for those participants allocated to sertraline mono-therapy or to combination therapy. Psychologists delivering CBT kept weekly compliance checklists throughout the 12-week treatment period.
Statistical analysis and power considerations
CONSORT standards were followed at all stages of the protocol (Moher et al., 2010) and the primary outcome analyses adhered to intention to treat principles.
The primary analysis of the three main outcome variables was based around two a priori comparisons, which were run separately at both Time 1 and Time 2. This approach was chosen in order to maximise power by focusing the analysis around single degree of freedom tests that addressed the main questions of interest. The first comparison focused on the combined therapy condition compared against the two single therapy conditions together. The second comparison involved the two single therapies, sertraline and CBT. Comparisons were run for each of the three main outcome variables. At Time 1, the two a priori comparisons were run incorporating the Baseline scores as a covariate and the Time 1 scores as the dependent outcome. These two comparisons were repeated at Time 2, with both Baseline and Time 1 scores serving as combined covariates. The effect size partial eta-squared, ηp2, was reported for all inferential outcomes. Each of these results was assessed against a per comparison α level of .017 in order to account for the inflation of the family-wise error rate from testing associated with the three dependent outcomes. A power analysis of this design using G*Power 3 (Faul et al., 2007) revealed that, with α = .017, and our randomised sample size of 45 participants, only very large effects (ηp2 > .14) had a reasonable probability of being reliably identified (i.e. power > .70).
Because depression was the primary outcome measure, a secondary inferential analysis that addressed different questions of the data was conducted on these outcomes. This analysis examined the pattern of change for the three groups across the 12 weeks of the protocol. The design was a 3 × 12 mixed factorial ANOVA with the three conditions forming the single between-subjects factor and the 12 time periods forming the single repeated measure. Post-hoc testing of the interaction test was conducted using simple main effects with Bonferroni-adjusted α levels. A power analysis of this design revealed that, with α = .05, and our randomised sample size of 45 participants, a large or moderate effect for the group by time interaction (ηp2 = .14 and .06, respectively) had an almost certain probability of being reliably identified (power > .99 in both cases). For the detection of small effects (ηp2 = .01) the design yields power = .40.
Clinical significance was assessed using an analysis of depression remission rates, as described below.
For the primary outcome analysis at the major assessment points (12 weeks and 24 weeks post-randomisation), inspection of the patterns of missing data and Little’s MCAR test found that the main outcome variables met the conditions for multiple imputation, which was the chosen implementation of intention to treat. All available data were used to model the multiple imputation outcomes for the main outcome variables, and pooled estimates of the imputed scores were used in all subsequent analyses. A secondary intention to treat analysis examined baseline data from those participants who provided complete data at the post-treatment phase against those who didn’t (completers versus non-completers). Both independent samples t-tests and χ2 analyses failed to find any systematic significant relationships between completion and any of the baseline clinical or demographic measures.
Data were examined for normality and homogeneity of variance. Normality was assessed using visual inspection of stem-and-leaf plots, histograms and normality plots, along with direct inferential tests of normality. Homogeneity of variance was assessed using Levene’s test. All dependent variables met the assumption of homogeneity of variance.
Computations were executed in IBM SPSS Statistics 19 & 20.
Results
Baseline characteristics
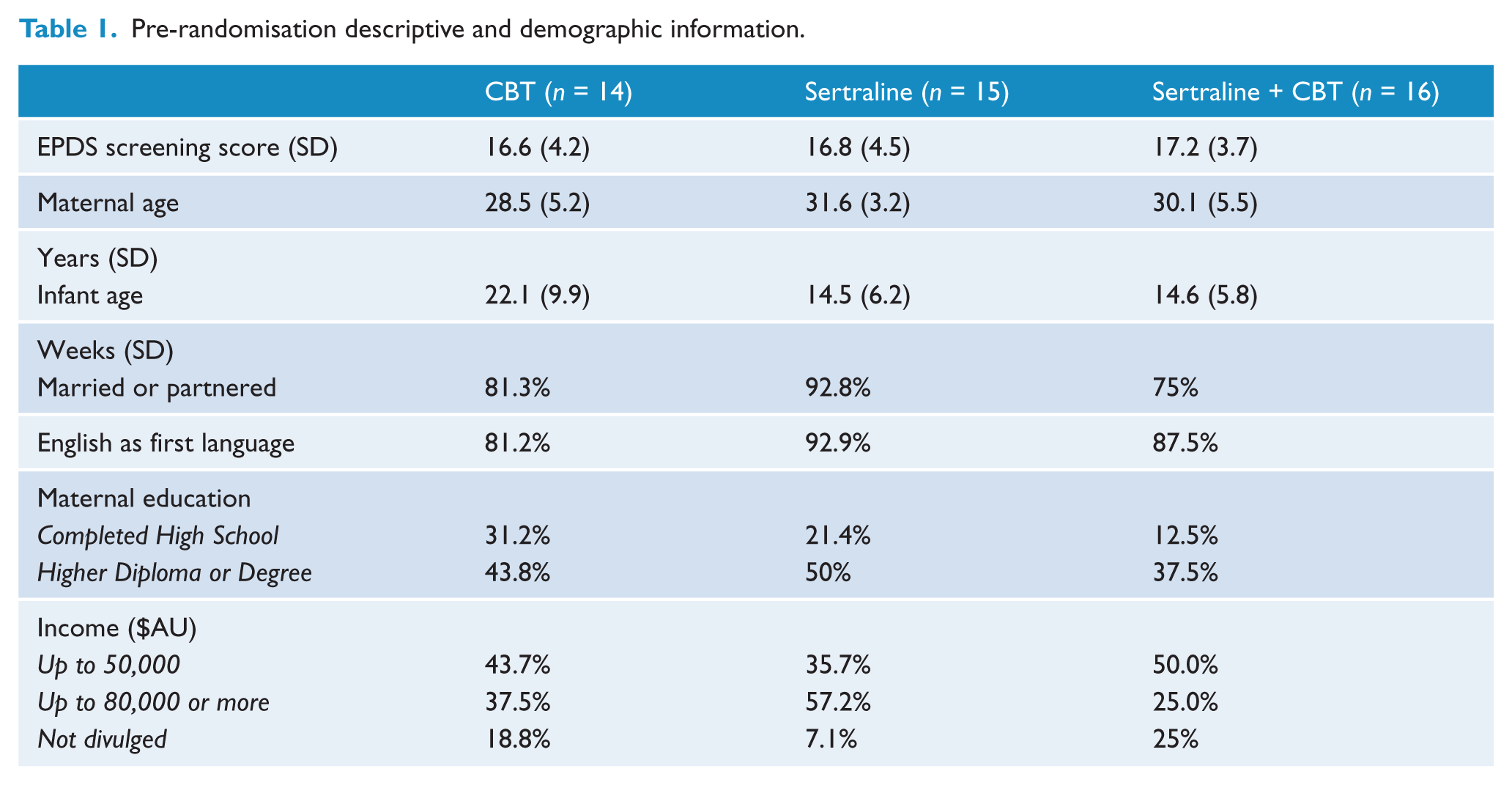
Over three years, a total of 6,500 women were screened at Maternal and Child Health Centres in Melbourne (Figure 1). Of the 915 women scoring ⩾ 13 on the EPDS, Maternal and Child Health Nurses referred 397. Of these referred women, 153 met all inclusion/exclusion criteria and a total of 45 women consented to be randomised (108 declined research participation). Baseline characteristics of women randomised to the three treatment groups are given in Table 1. Thirty nine women had a primary DSM-IV diagnosis of Major Depressive Disorder; three had a primary diagnosis of Mixed Anxiety/Depressive Disorder; two had Depressive Disorder N.O.S. and one woman had a primary diagnosis of Dysthymia.
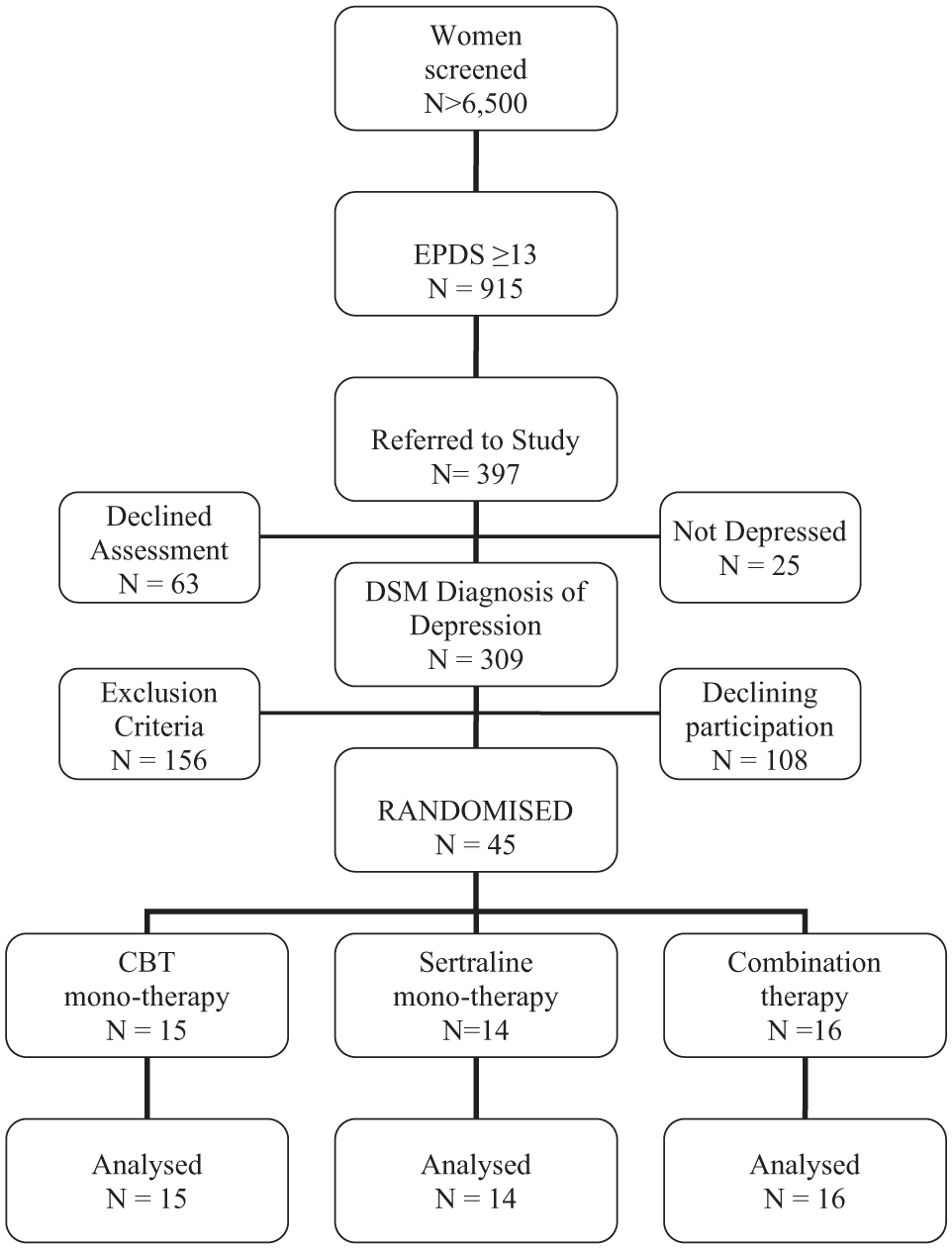
CONSORT diagram of recruitment, treatment, follow-up and analysis.
Pre-randomisation descriptive and demographic information.
Compliance
Women in the combined therapy discontinued medication after an average of 10.5 weeks, with five never starting and six still taking medication at 24 weeks. In the sertraline mono-therapy group women discontinued medication after an average of 12.9 weeks, with four women failing to commence medication and six complying with medication for the full 24 weeks. The rate of medication non-commencement did not differ statistically between the sertraline mono-therapy and combined therapy groups (p = .6) and neither did the average length of time on medication (p = .5). There were no adverse events recorded among those women prescribed sertraline.
In the combination therapy, women attended an average of 7.5 sessions out of a possible 12, with four women completing less than half the sessions. In CBT mono-therapy, women completed an average of 10.6 of the possible 12 sessions and all completed at least half of the sessions. The average number of CBT sessions attended did not differ significantly between the CBT mono-therapy and combined therapy groups (p = .058).
Primary efficacy analysis
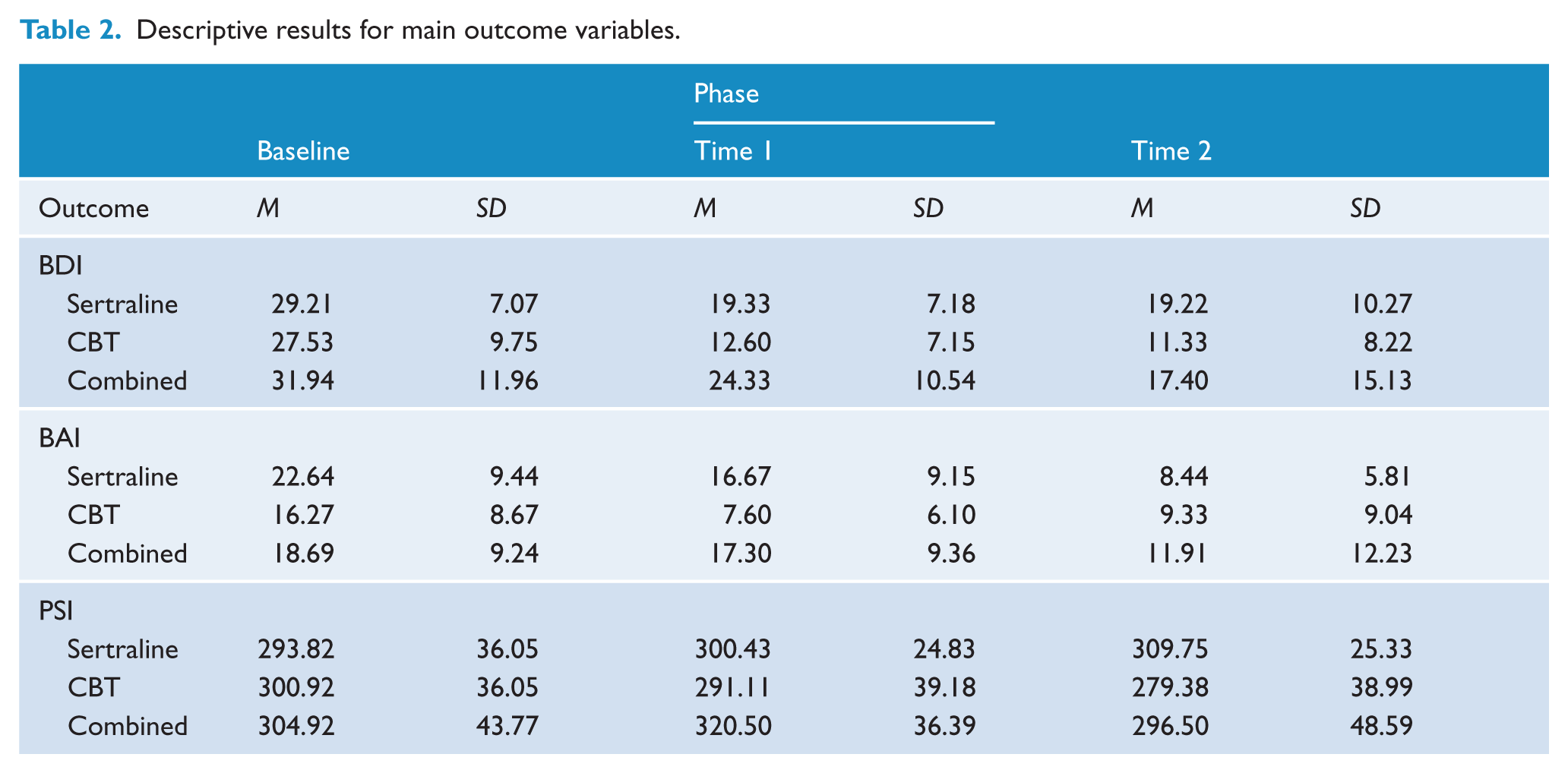
Descriptive statistics for the three main outcome variables are presented in Table 2. In relation to depression, with CBT mono-therapy (see also Figure 2), a notable decrease from Baseline to Time 1 is evident, followed by some levelling off at Time 2. A similar pattern is evident for participants receiving sertraline, although the Baseline to Time 1 effect is not as strong. The participants receiving combination therapy demonstrated a different change over time; specifically, a less pronounced Baseline to Time 1 change was followed by a more notable decrease from Time 1 to Time 2.
Descriptive results for main outcome variables.
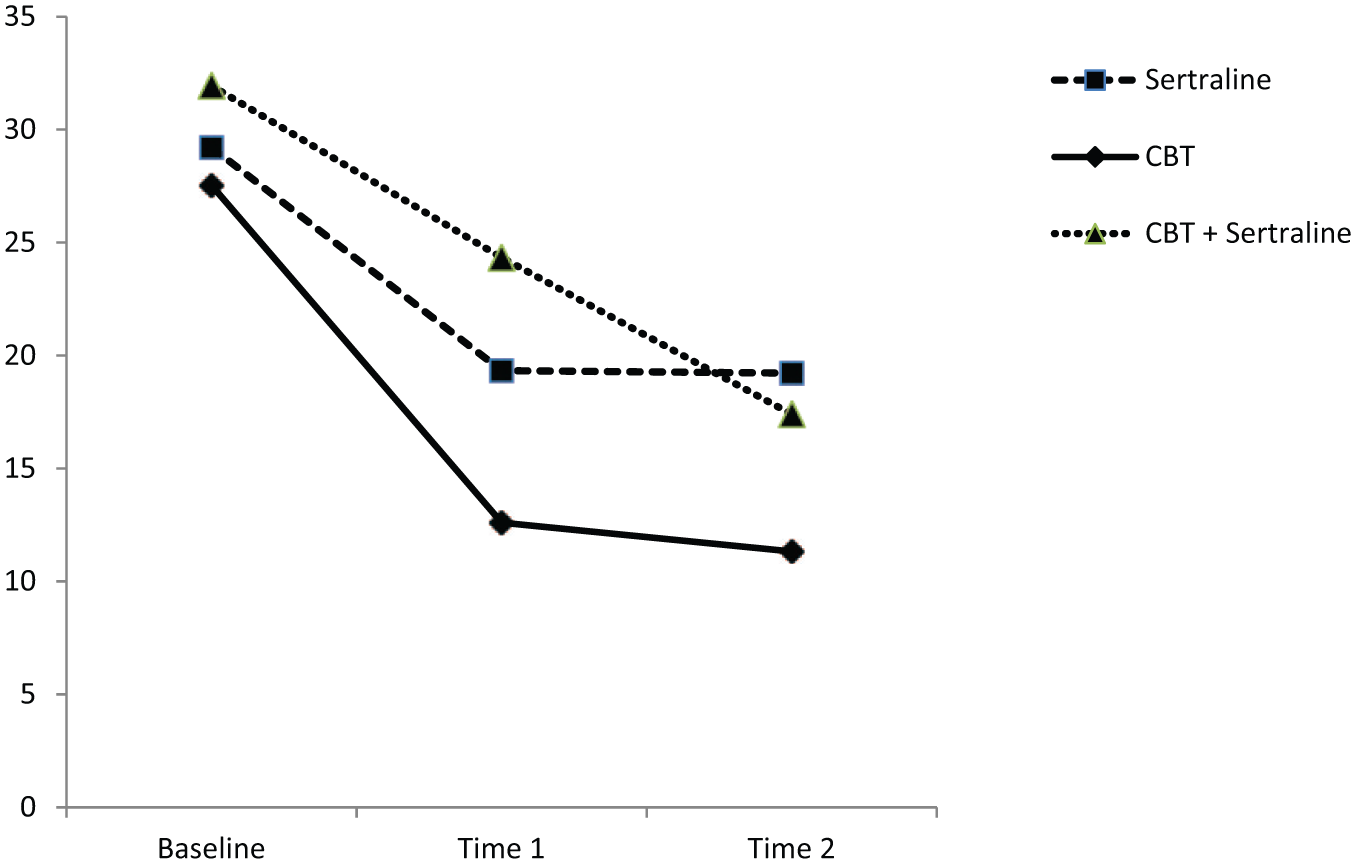
Depression severity (BDI-II) at Baseline and follow-up points (includes imputed values).
The pattern of results for anxiety was similar, with the notable exception being a sharp decrease in symptoms from Time 1 to Time 2 for those participants in the Sertraline group.
For parenting stress, the most obvious descriptive result was that only the participants receiving CBT mono-therapy exhibited any change in the desired direction.
Primary inferential test results for depression failed to reveal a clearly significant difference between the two single therapies (taken together) compared to the combination therapy at Time 1 after co-varying out baseline variance, F(1, 41) = 6.38, p = .02, ηp2 = .21. Despite this non-significant result at α < .017, it is worth noting that (a) the result was near significance, (b) the effect size, ηp2 = .21, was large, and (c) the descriptive findings clearly indicate an effect in the clinically desired direction. Taken together, we would contend that there is convincing evidence to ‘suspend judgement’ 1 on this result, rather than dismiss it outright as a non-significant finding. Finally, simulation analysis revealed that, had all other parameters remained consistent, the completion of three extra participants per group would have resulted in a clearly significant result. No significant difference was found between the Sertraline and CBT groups, and no significant differences were found for the equivalent Time 2 comparisons.
For anxiety, a significant difference was found at Time 1 for the first contrast, F(1, 41) = 8.65, p = .007, ηp2 = .26, with the single therapies demonstrating the stronger effect in the desired direction. Also, a significant Time 1 difference was found between CBT and Sertraline, F(1, 41) = 8.13, p = .009, ηp2 = .25, with CBT demonstrating the higher decrease in anxiety symptoms. No significant results were found at Time 2.
For the parenting stress index, no significant results were observed.
There was no evidence that any of these results were moderated by baseline levels of depression. Baseline to Time 1 and Baseline to Time 2 change scores were calculated for each of the three main outcome variables. These were analysed initially by correlating these change scores – separately for each group – with the baseline scores on the Hamilton Depression Inventory. No significant or indicative results emerged to warrant more formal moderation testing.
Secondary analysis of weekly depression scores
Figure 3 shows the weekly trajectory of BDI-II scores across the first 12 weeks of treatment. On visual inspection, the CBT mono-therapy group appears to have displayed the most rapid and largest gains in this initial treatment period. This was confirmed statistically by running a 3 × 12 mixed factorial ANOVA. The significant group by time interaction, Λ = .68, F(22, 64) = 4.88, p < .001, ηp2 = .63, was followed by group within time simple main effects analysis, which found significant differences among the three groups at week 2, p < .001, week 3, p = .02, week 4, p < .001, and week 5, p = .01. In each instance, the CBT group demonstrated the lowest depression score, which was significantly lower than at least one of the other two conditions.
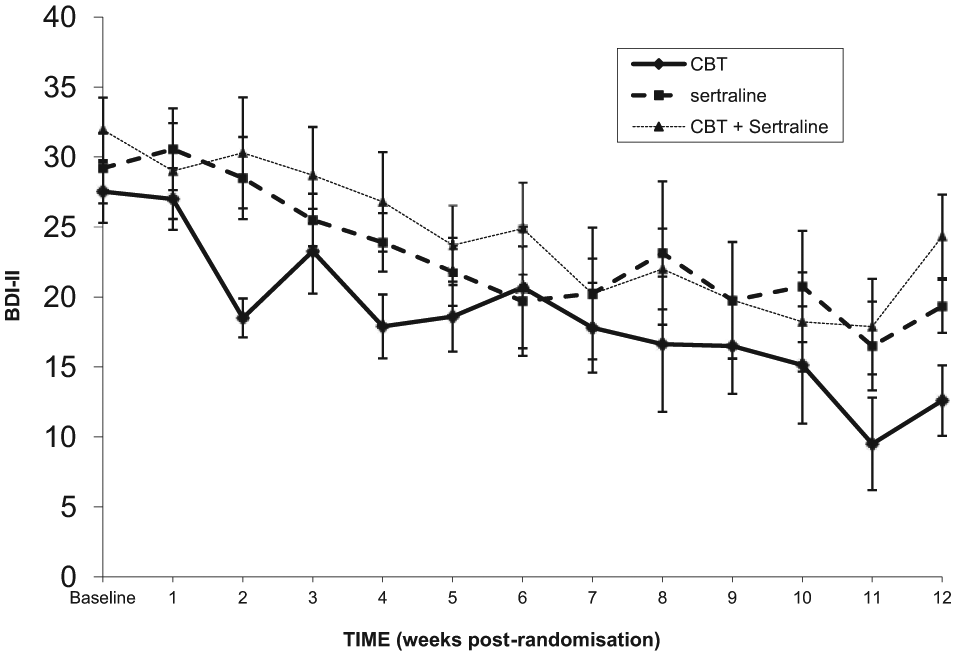
Weekly ratings of depression severity (observed cases only). Error bars are ±1 S.E.
Given the importance of analysing the pattern of change over time for each treatment condition, the time within group simple main effect was analysed using trend analysis, with an emphasis on linear and quadratic patterns; these analyses were Bonferroni adjusted. Strong and significant linear trends were found for all three conditions: Sertraline, F(1, 13) = 32.18, p < .001, ηp2 = .71; CBT, F(1, 14) = 16.36, p = .001, ηp2 = .54; and combination therapy, F(1, 15) = 44.50, p < .001, ηp2 = .75. Only the linear trend was found to be significant for any of the conditions; hence, all three conditions demonstrated a significant linear pattern of symptom reduction over the 12-week protocol.
Regarding these analyses, it should be noted that while a 3 × 12 mixed factorial ANOVA might be considered overly exploratory, the follow-up simple main effects tests were Bonferroni-corrected, which reduces capitalisation on chance.
Remission
Remission analysis was conducted on the BDI-II scores using a cut-off score of < 13 to indicate minimal depression.
The results for the percentage of participants reporting minimal levels of depression were analysed using a Cochrane’s Q test across the three time periods, where success from the point of view of the analysis was defined as falling within the minimal depression category. The percentage changes across the three time periods for the three groups are shown in Figure 4. No significant change was observed across the Sertraline group, p = .17, but significant changes in the proportion of participants falling within the minimal depression category were seen in both the CBT, p = .008, and Combined groups, p = .05. Pairwise post-hoc comparisons for these two findings revealed a significant difference between the Baseline and Time 2 phases for the CBT group, p = .007, but no significant post-hoc results for the Combined group. Adjusted asymptotic significance levels were used for these analyses.
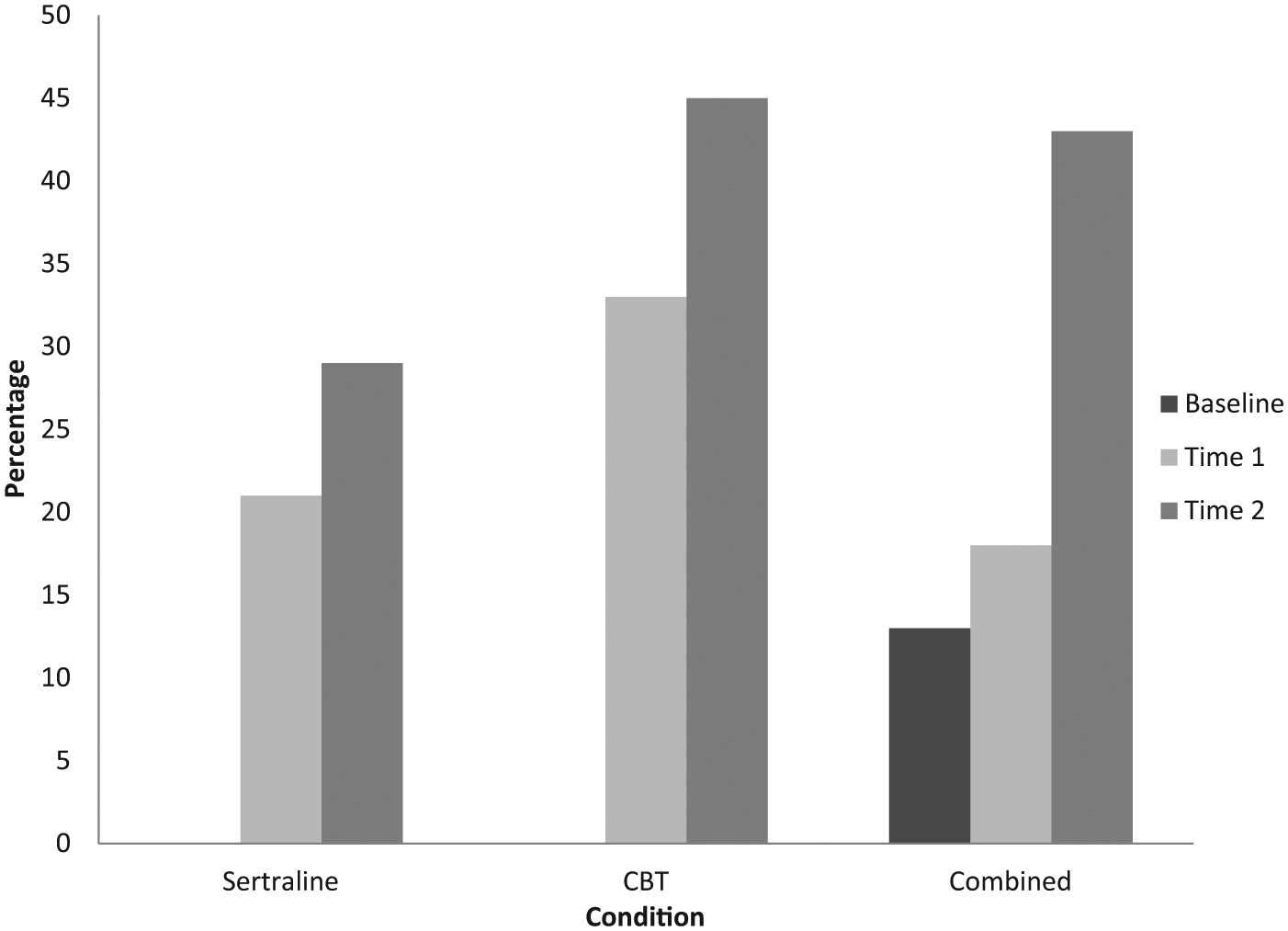
Percentage of participants reporting minimal levels of depression. In the Sertraline and CBT conditions, no participants reported minimal levels of depression at Baseline.
Discussion
There is good evidence that both antidepressant medication and cognitive behavioural therapy are effective in treating adult depressive disorders (Cuijpers et al., 2009). Our findings that women’s mood improved with CBT treatment are consistent with psychological treatment trials of PND in general (Cuijpers et al., 2008; Dennis and Hodnett, 2007). Unlike some previous work, our design allowed a statistically independent evaluation of specialised CBT for PND as a mono-therapy compared to both antidepressant and combination therapy. In line with previous studies of postpartum women, there was no detectable advantage of combining pharmacological and psychological treatments on the outcome of clinically diagnosed PND. However, these results are in contrast to the outcomes of a large and identically configured 3-arm RCT with nefazodone and CBT in the general adult population (Keller et al., 2000). In our sample, for the treatment of depression, mono-therapies per se (CBT or sertraline) were found to be superior in the short term to combination therapy. CBT mono-therapy was also more effective than either sertraline or combination therapy in short-term reduction of anxiety scores. At 24 week follow-up only CBT mono-therapy led to the average BDI-II score falling in the ‘minimal’ range immediately post-treatment. Consequently, at 24 week follow-up a higher percentage of women in this treatment condition had achieved remission, their scores falling below the threshold for minimal depression. A recent meta-analysis of 3-month, 6-month and 12-month remission rates in untreated major depression (Whiteford et al., 2013) estimated that around 32% of adults in primary care will experience remission of depression by 6 months. Consistent with this, our findings show improvement across time in all groups irrespective of treatment allocation. Interestingly, the remission rate seen in our sertraline mono-therapy group is similar to Whiteford et al.’s estimate, which raises the question of whether in this trial antidepressant treatment alone offered therapeutic benefit in the longer term.
Interestingly, in our study, those women in combination therapy showed a poorer amelioration of depression and anxiety than any other group. They also attended fewer CBT sessions compared to those in CBT mono-therapy and discontinued antidepressant medication more frequently and earlier than those in sertraline mono-therapy. Although these last differences were not statistically different, they may point to some unidentified factor which made combination therapy less acceptable or harder to comply with. Combined therapy did require the greatest time commitment by women who had to attend the CBT sessions and also medication review appointments. Their lack of compliance with both these aspects may reflect their limited physical and emotional resources as an obstacle to care in combination therapy.
When considering choice of treatment, the rapidity with which symptoms ameliorate after commencement of treatment may be relevant in clinical practice. In this study we found a suggestion that CBT may have resulted in the fastest initial improvements in mood.
Limitations
It should be noted that there are limitations to this study which may influence the results and the ability to apply these findings. First, one of the inclusion criteria was that women agreed to be willing to receive any of the three treatment conditions. There were a large number of eligible women who declined participation, which may suggest that obtaining their therapy of preference may be important in treatment initiation. Thus, as a group, the participants in our sample may not reflect the wider population of postnatal women. It may also suggest that one or more of the treatment conditions were particularly unattractive to prospective participants leading to them avoiding participation. Second, like most work in this area, the sample size was relatively small, again potentially hindering the generalisability of findings.
Of the women who were prescribed sertraline, around 30% never commenced medication. This may reflect women’s ambivalence about treatment with medication, which must surely be a major obstacle to treatment in general practice. Literature shows depressed individuals are more likely to pursue a treatment option that is in line with their health beliefs and that they feel will be beneficial (Kwan et al., 2010). Further research on woman-centred care and involving women in choosing treatment options they feel will be beneficial may help our understanding of how to improve treatment uptake.
For parenting stress, the change following treatment was non-significant and left women in this group well above the ‘dysfunctional threshold’ replicating similar findings that have been noted elsewhere (Milgrom et al., 2006; Myers et al., 2013). It may be that additional mother–infant therapy may be needed to repair the relationship (Milgrom et al., 2006).
Conclusions
Our results add to a small but expanding literature on the efficacy of antidepressant medication and the comparative benefits of CBT or combined therapy for women with postnatal depression. In a recent systematic review, De Crescenzo and colleagues (De Crescenzo et al., 2014) noted that such RCTs are required, with broader inclusion criteria with respect to depression severity and longer-term follow-up. By including a broad sample with respect to demographics and depression severity and by conducting a follow-up at six months, the present study adds necessary information to the existing evidence base.
Footnotes
Acknowledgements
We thank the women who took part. Thanks also to Dr Trevor Norman for useful advice and discussion.
Funding
The study was funded through a grant from Pfizer Inc. and by the Kinsman Fund. Neither funding body had any input into the study design, the analysis or interpretation of results, or the decision to publish the findings.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.