
Abstract
Objective:
Only a small proportion of individuals with an eating disorder will receive targeted treatment for their illness. The aim of this study was to examine the length of delay to treatment-seeking and determine the barriers preventing earlier access and utilisation of eating disorder treatment for each diagnostic group – anorexia nervosa, bulimia nervosa, binge eating disorder and other specified feeding or eating disorder.
Method:
Participants were recruited as part of the TrEAT multi-phase consortium study. One hundred and nineteen Australians (13–60 years; 96.9% female) with eating disorders currently accessing outpatient treatment for their illness completed an online survey comprised of self-report measures of eating disorder severity, treatment delay and perceived barriers to treatment-seeking. The treating clinician for each participant also provided additional information (e.g. body mass index and diagnosis).
Results:
Overall, the average length of delay between onset of eating disorder symptoms and treatment-seeking was 5.28 years. Controlling for age, latency to treatment-seeking was significantly longer for individuals with bulimia nervosa and binge eating disorder compared to anorexia nervosa. However, when perceived barriers to treatment-seeking were investigated, there were no significant differences between the diagnostic groups in regard to the perceived barriers they experienced. Stigma was rated as the most impactful barrier for each diagnostic group.
Conclusion:
Findings suggest that individuals with eating disorders face substantial delays in accessing appropriate treatment and that latency to treatment-seeking is often magnified for counter-stereotypical eating disorder presentations. Further research is required to investigate other factors contributing to this delay.
Eating disorders (EDs) are severe and often chronic psychological illnesses that are associated with long-term mental and physical complications and poor quality of life (Hoek, 2016; Klump et al., 2009; Van Hoeken & Hoek, 2020). Individuals with EDs have significantly higher mortality rates compared to the general population, and anorexia nervosa (AN) in particular has the highest lifetime mortality rate of any non-substance use psychiatric disorder (Arcelus et al., 2011; Steinhausen, 2002). In Australia, the estimated prevalence of any Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) ED in adults is approximately 16% (Hay et al., 2015, 2017). EDs have been associated with significantly impaired health-related quality of life when compared with both the general population (Agh et al., 2016; Van Hoeken & Hoek, 2020) and other psychiatric illnesses (Jenkins et al., 2011). And the economic burden of EDs is also substantial due to high rates of emergency department visits, hospitalisation and outpatient care (Agh et al., 2016).
Despite the severity of EDs, they often go undetected and subsequently untreated in the community (Hudson et al., 2007). It is estimated that only 19–36% of individuals with an ED will receive treatment (Hart et al., 2011), and of the individuals who do receive treatment, only 35–40% will receive targeted treatment for their ED (Mond et al., 2007; Noordenbos et al., 2002). Mond et al. (2007) found that women with bulimia nervosa (BN) rarely received treatment for their ED; instead, they commonly received treatment for weight loss or a general mental health problem. Furthermore, there is often a substantial delay between the onset of symptoms and eventual treatment access. For EDs, the average delay is estimated to be approximately 2.5 years for individuals with AN, 4.4 years for individuals with BN and 5.6 years for individuals with binge eating disorder (BED; Austin et al., 2020). Understanding the cause of this delay could result in earlier intervention and more positive treatment outcomes (e.g. reduced illness duration, less need for intensive treatments) and inevitably reduce costs to the individual and the community. A recent systematic review by Ali et al. (2017) identified a scarcity of quantitative research investigating perceived barriers and facilitators to help-seeking for EDs. Of the 13 studies that were found to address this issue, stigma and shame were identified as key barriers in 11 of the studies, followed by denial or failure to perceive the severity of the ED symptoms (9 studies), practical barriers (8 studies) and negative attitudes towards treatment (7 studies). A similar systematic review by Innes et al. (2017) endorsed the same barriers to treatment, and both reviews highlighted the distinct lack of high-quality research conducted in this area and significant heterogeneity in terms of study design, participant samples and operationalisation of variables.
The majority of research investigating barriers to treatment-seeking has focussed on EDs as a whole, yet there are meaningful distinctions between ED diagnoses. For example, AN is associated with severe and often visible physical health impairments (e.g. emaciation) and is the only ED characterised by an underweight status, and BN is unique in requiring both recurrent binge eating and compensatory behaviours for a diagnosis (American Psychiatric Association [APA], 2013). Both BN and BED are often associated with a high body mass index (BMI), adding to the complexity of differential diagnosis. It is therefore possible that the individuals suffering from these distinct diagnoses may face different as well as similar barriers when seeking treatment.
A review of initial treatment-seeking for EDs found that several ED-related variables were associated with increased treatment-seeking, including higher levels of ED pathology, ED-related distress and ED-related physical health impairments (Regan et al., 2017). Other identified factors that significantly increase treatment-seeking include greater psychological distress, poorer psychosocial functioning, lower mental health–related quality of life and lower overvaluation of weight/shape (Fatt et al., 2020; Thapilyal et al., 2018). Historically, it has been believed that gender also significantly impacts treatment-seeking for EDs; however, emerging research shows that functional health impairments and other ED-related symptoms are stronger predictors of ED-specific treatment-seeking than gender (Thapilyal et al., 2020). ED type and symptoms were also associated with increased treatment-seeking (Regan et al., 2017). In the adolescent population, individuals with AN and BN were 2.4 and 1.9 times more likely to seek treatment than adolescents with BED (Forrest et al., 2017). Moreover, ED behaviours (e.g. restriction and purging) and more severe ED-related impairment were both associated with greater treatment-seeking (Cachelin et al., 2006; Hart et al., 2011). The impact of behaviours, such as self-induced purging, and other forms of restriction are often more visible, such as weight loss and dermatologic symptoms (Strumia, 2006), and have more severe physiological consequences like arrhythmia or hypotension (Forney et al., 2016) that may be more easily identified by the individual, family, friends or health professionals. It has been shown that individuals with counter-stereotypical ED presentations (e.g. individuals with a higher BMI) are the least likely to seek treatment (Forrest et al., 2017).
Poor mental health literacy (especially a lack of knowledge about EDs) has been associated with individuals and their social networks overlooking or incorrectly identifying ED behaviour, thus preventing individuals from seeking appropriate treatment (Hepworth and Paxton, 2007; Mond et al., 2010). Furthermore, symptoms of lesser known EDs (e.g. BED) often go unrecognised by healthcare professionals (Hart et al., 2011), and this can be due to underlying biases about the type of person who can suffer from an ED (Becker et al., 2005; Mond et al., 2007).
An American study of adolescent treatment-seeking found that only 20% of adolescents sought ED-specific treatment (Forrest et al., 2017), and this was even lower in the Australian context with only 10% of adolescents seeking treatment (Fatt et al., 2020). While overall treatment-seeking appears to be limited for individuals with EDs, people with counter-stereotypical ED presentations are even less likely to seek treatment (Bohrer et al., 2017), and when they do present to primary care facilities, their ED symptoms often go unrecognised (Hudson et al., 2007). Ali et al. (2020) examined help-seeking in young adults with ED symptomatology and found that 73% of participants did not believe they needed help for their symptoms. Participants with AN or BN were more likely to endorse previous negative beliefs about the effectiveness of treatment and negative past experiences in treatment, whereas individuals with BED indicated that they would more likely access friends for support rather than formal treatment options. Hence, using a sample of individuals with varied ED diagnoses (e.g. AN, BN, BED or OSFED [Other Specified Feeding and Eating Disorder]), this study aimed to examine (1) the length of time between symptom onset and accessing ED-specific treatment providers, and (2) the perceived barriers to accessing treatment that each diagnostic group faced. Based on previous research (e.g. Forrest et al., 2017; Regan et al., 2017; Thompson and Park, 2016), it was expected that the length of delay would be longer for BN, BED and OSFED groups compared to the AN group. It was also hypothesised that there would be some overlap in terms of the perceived barriers to treatment-seeking. It is likely that all the diagnostic groups would report barriers such as stigma and shame and practical barriers; however, it was predicted that barriers related to the recognition of illness would be more prevalent for BN, BED and OSFED compared to AN.
Methods
Participants
Data from 119 participants were included in this study (94.96% female, mean age = 23.77 years, SD = 9.74). Participants were recruited as part of a project called the Clinical and Demographic Correlates of Eating Disorder Treatment-Seekers (known as the TrEAT Study), a multi-phase consortium study investigating the characteristics of individuals referred to and receiving specialised treatment for EDs. The TrEAT database included data collected from seven private ED services across Sydney and Perth, Australia. Participants (aged 12 or older) were recruited from the participating ED services, where consent was formally obtained from each participant or from their parents for those under the age of 18 years. Participants completed an online survey prior to or in conjunction with their first consultation, as part of routine assessment, and were asked by administration staff whether they wanted their de-identified data to be included in the TrEAT database for research purposes. The treating clinician (psychologist, clinical psychologist or dietitian with specialised training or expertise in EDs) was then asked to add information on weight, height and diagnosis.
Only data from participants who provided responses to the relevant questionnaires for this study (i.e. latency to treatment-seeking and perceived barriers to seeking and utilising ED treatment) and who had corresponding data on diagnosis provided by their treating clinician were included. The diagnosis provided by the treating clinician was based on DSM-5 (APA, 2013) criteria and was used to classify participants into four main diagnostic groups: AN, BN, BED and OSFED. Individuals diagnosed with unspecified feeding or eating disorder (UFED) were not included in the study as there was an insufficient number of participants (n = 3) with this diagnosis to create a separate group. As such, they were excluded from the study.
Measures
The survey included self-reported socio-demographic information, clinician-reported diagnostic information and self-report clinical questionnaires.
Socio-demographic and treatment history information
Participants were asked to provide socio-demographic information such as age, gender, ED service and number of sessions attended.
Clinician-reported information
Treating clinicians, all of whom have had additional training and experience with EDs, were asked to report the participant’s weight, height and diagnosis. The clinicians made the diagnosis based on clinical interview and reviewing responses to the Eating Disorder Examination–Questionnaire version (EDE-Q; Fairburn and Beglin, 1994).
ED symptoms
The EDE-Q (Fairburn and Beglin, 1994) was used to assess the nature and frequency of symptoms of eating pathology over the past 28 days. It comprised four subscales with 22 self-report items rated on a 7-point Likert-type scale, ranging from 0 (no days, not at all or none of the time) to 6 (every day, markedly or every time). This study only used the global score which was calculated by summing the subscale scores and dividing by the number of subscales. Higher global scores indicated more severe ED pathology. Cronbach’s alpha for the global score was 0.92.
Latency to treatment-seeking
Two self-report questions determined the length of time between onset of ED symptomatology and seeking treatment and the length of time between seeking treatment and accessing treatment. The two questions were as follows: ‘From the time of the onset of your eating disorder symptoms, approximately how long did you wait to seek treatment?’ and ‘From the time you began to seek treatment, how long did you have to wait to access it?’ Participant responses were converted to length of time in years.
Perceived barriers to seeking and accessing treatment
A 7-item measure was created to assess the impact of various perceived barriers to seeking and accessing treatment for EDs. The measure was modified from the questionnaire developed by Thompson and Park (2016) to be more applicable for the Australian context. The questionnaire comprised a list of seven perceived barriers (cost, stigma, accessibility, social/work concerns, lack of ED knowledge in the general practitioner, personal lack of ED knowledge and other). This included measures such as the following: Please rate how much stigma associated with eating disorders (e.g. did not feel comfortable disclosing my condition to my GP, guilt or shame associated with my symptoms, fear of judgement from family/social groups) affected your access or use of outpatient or inpatient eating disorder treatment.
Participants were asked to rate how impactful each barrier was on a 5-point Likert-type scale, ranging between 1 (no impact at all), 3 (moderately impactful) and 5 (extremely impactful), with higher scores indicating greater impact on help-seeking. Cronbach’s alpha was 0.64. The measure can be found in Appendix 1.
Procedure
The TrEAT Study was approved by the Macquarie University Human Research Ethics Committee. Consenting participants completed an online survey using Qualtrics Survey Software prior to their first appointment. Following the initial session, the treating clinician then completed a section of the online questionnaire and added diagnostic information. Participants were not provided any reimbursement for their participation in this research.
Statistical analysis
Descriptive statistics and all analyses were conducted using the IBM SPSS Statistics (version 25) program. Assumptions of parametric and non-parametric tests were assessed and corrected for (if violated). To measure the effect size for significant interactions, partial eta squared
First, parametric tests were conducted to examine between-group (i.e. diagnostic subgroups) differences in the continuous demographic variables (age, BMI and EDE-Q global score). Significant F-tests were followed up with Bonferroni-adjusted pairwise comparisons. Chi-square tests of independence were conducted to examine between-group differences in the categorical demographic variable (gender). Variables with significant between-group differences were considered as potential covariates in subsequent analyses.
Comparisons between diagnostic groups were conducted using an analysis of covariance (ANCOVA) (using age as a covariate) to investigate the difference in length of time between the onset of ED symptoms and accessing treatment. Similar tests were carried out to examine differences between the ED subgroups in the length of time between seeking and accessing treatment. Post hoc Bonferroni-adjusted pairwise comparisons were conducted to investigate significant results.
A series of ANCOVAs were conducted to compare differences in perceived barriers to accessing and utilising ED-specific treatment providers between the diagnostic groups. Age was used as a covariate to account for pre-existing group differences as a function of age. Repeated-measures analyses of variance (ANOVAs) were used to investigate within-group differences in the rating of each perceived barrier for each diagnostic group. Post hoc Bonferroni-adjusted pairwise comparisons were used to further investigate significant test results and control for inflated Type 1 error rates.
Results
Description of sample
Participants were predominantly female (94.96%) aged between 12 and 60 years with a mean age of 23.77 years (SD = 9.74). The diagnostic groups included in the study were AN (n = 37; 31.09%), BN (n = 26; 21.85%), BED (n = 17; 14.29%) and OSFED (n = 39; 32.77%). The AN group comprised both the binge/purge subtype (n = 6; 16.22%) and the restrictive subtype (n = 31; 83.78%), and the OSFED group included the following subgroups: atypical AN (n = 29; 74.36%), BN of low frequency and/or limited duration (n = 2; 5.13%), BED of low frequency and/or limited duration (n = 5; 12.8%) and purging disorder (n = 4; 10.26%). Overall, the average length of time between symptom onset and treatment-seeking for the whole sample was 5.28 years (SD = 7.79) and between treatment-seeking and treatment access was 0.35 years (SD = 1.50). Demographic information for each diagnostic group and comparative statistics are presented in Table 1.
Demographics for all participants: mean age, gender, BMI and scores of eating disorder pathology for each diagnostic group. (N = 119).
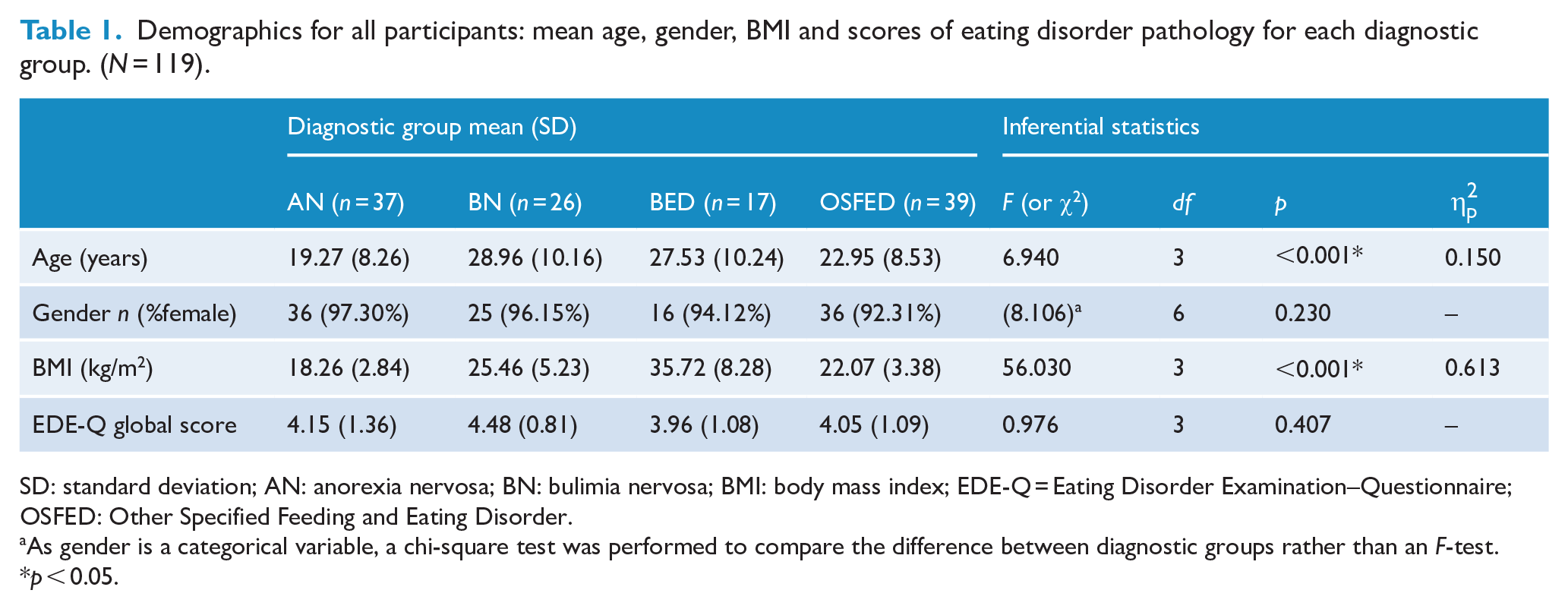
SD: standard deviation; AN: anorexia nervosa; BN: bulimia nervosa; BMI: body mass index; EDE-Q = Eating Disorder Examination–Questionnaire; OSFED: Other Specified Feeding and Eating Disorder.
As gender is a categorical variable, a chi-square test was performed to compare the difference between diagnostic groups rather than an F-test.
p < 0.05.
ANOVAs comparing the diagnostic groups on the demographic and study variables revealed that age, F(3) = 6.94, p < 0.001,
Latency to access and utilisation of ED-specific providers
An ANCOVA conducted comparing length of time between symptom onset and treatment-seeking between diagnostic groups revealed a significant and moderately sized main effect of diagnostic group, F(3) = 5.071, p = .002,
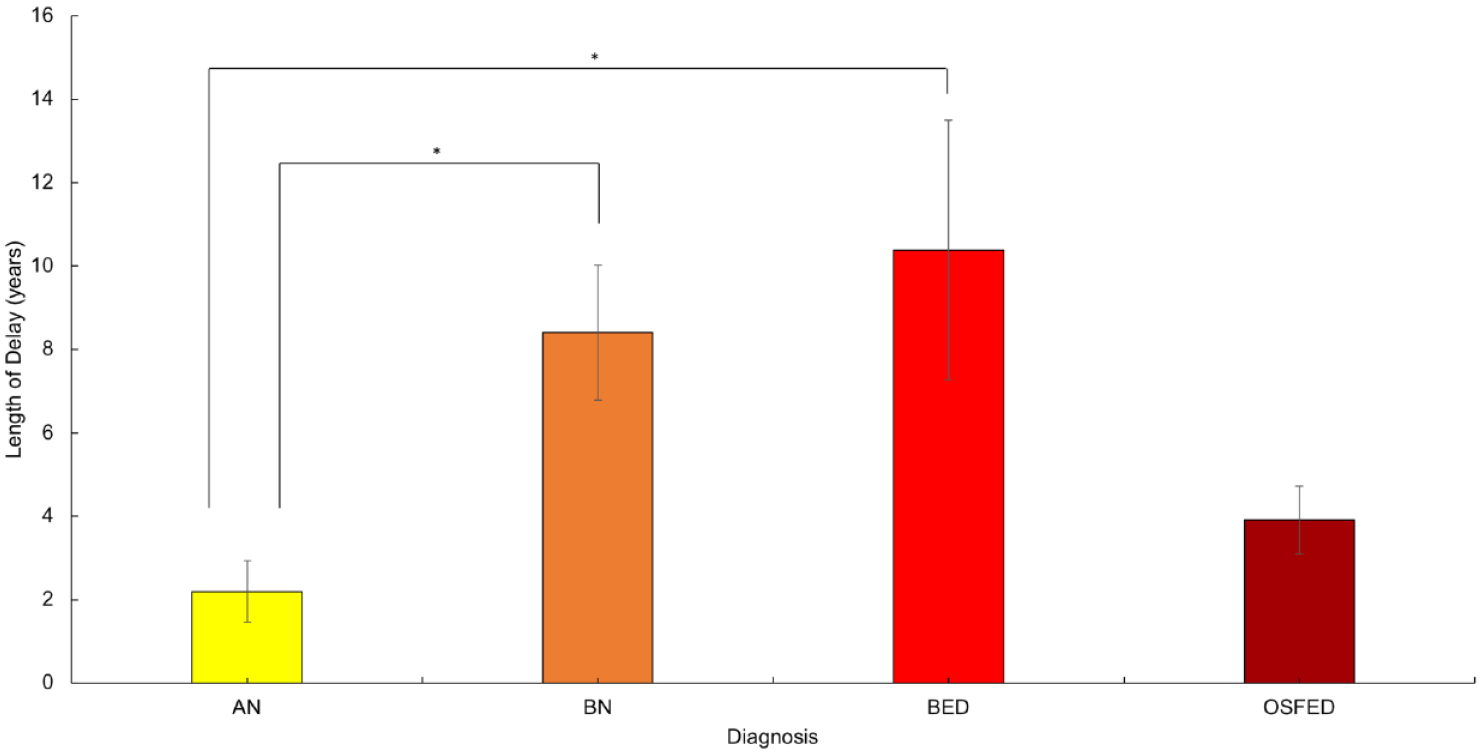
Average length of delay (in years) between onset of ED symptoms and initial treatment-seeking.
There were no significant differences in the length of time between treatment-seeking and treatment access between the ED subgroups,, F(3) = 0.793, p = 0.500.
Perceived barriers to access and utilisation of ED treatment
Overall, for the AN group the mean score for each barrier was between 2.14 (SD = 1.25) and 3.35 (SD = 1.42), indicating that scores on all barriers were considered to be within the moderately impactful range. Similarly, for the BN group, mean scores ranged from 2.04 (SD = 1.12) to 4.04 (SD = 1.27); for the BED group, mean scores ranged from 1.94 (SD = 1.35) to 3.47 (SD = 1.23); and for the OSFED group, mean scores were between 2.05 (SD = 1.12) and 3.69 (SD = 1.22) (Figure 2). Despite some variability in the scores for the different perceived barriers, no significant between-diagnostic group effects emerged, indicating that the impact of each perceived barrier was similar across diagnoses.
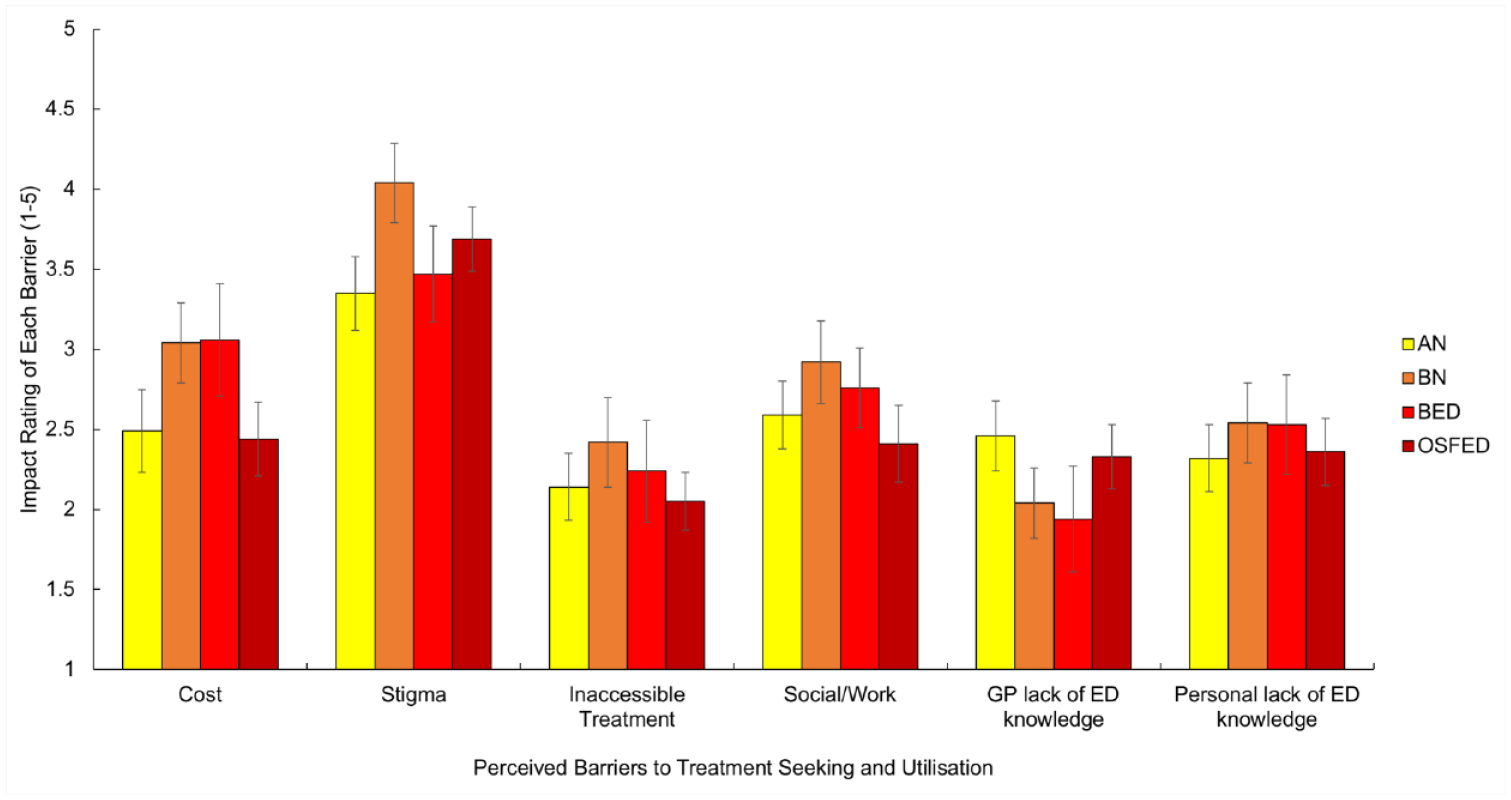
Mean scores on the perceived barriers to seeking and accessing treatment questionnaire. Higher scores indicated greater impact on help-seeking.
Impact scores for each barrier were compared within each diagnostic group using repeated-measures ANOVAs. Each ANOVA produced significant main effects that were moderate to large in size, indicating differences in the impact of specific barriers within each group (for AN, F(5, 180) = 5.302, p < 0.001
Summary of significant repeated-measures ANOVAs examining within-group differences in the impact of perceived barriers to treatment-seeking.
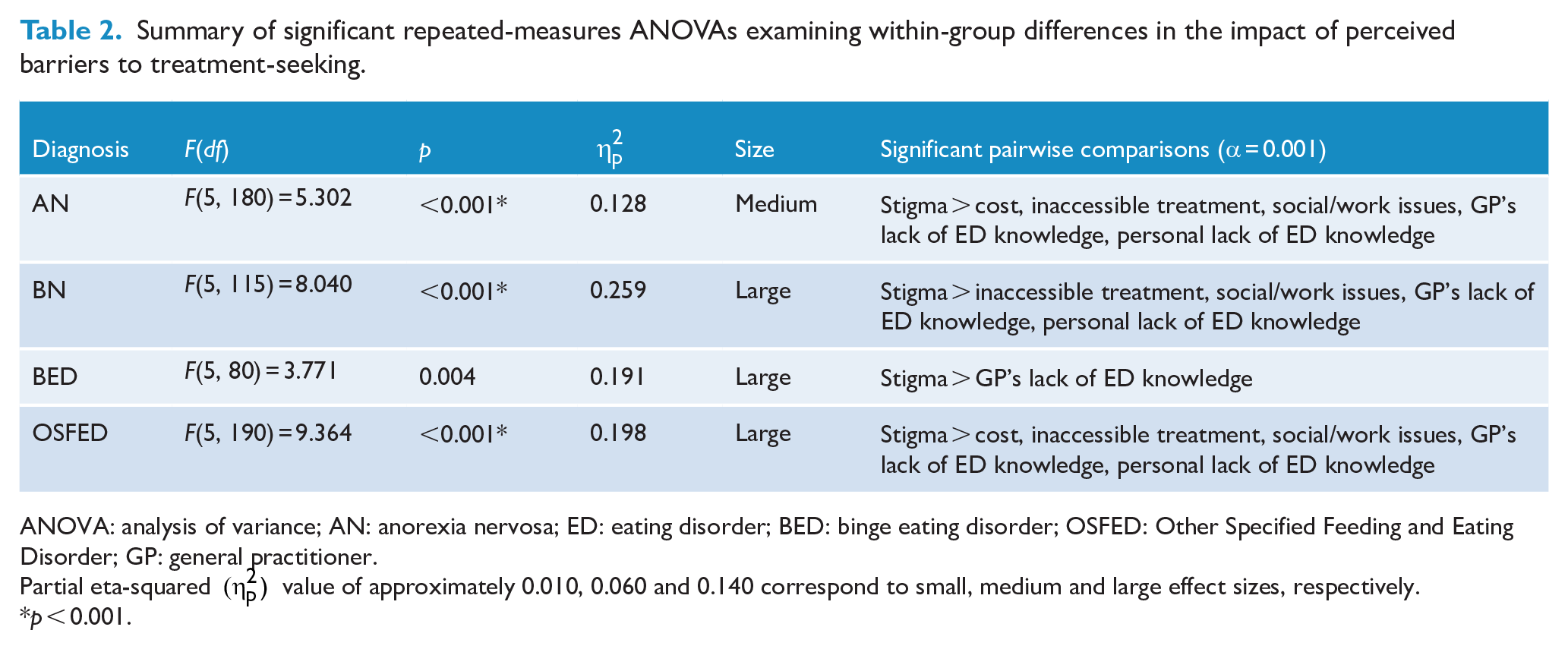
ANOVA: analysis of variance; AN: anorexia nervosa; ED: eating disorder; BED: binge eating disorder; OSFED: Other Specified Feeding and Eating Disorder; GP: general practitioner.
Partial eta-squared
p < 0.001.
Discussion
The results of this study revealed three important findings. First, as expected, individuals with BN and BED experienced a significantly longer delay from onset of symptoms to ED-specific treatment-seeking when compared to AN. Second, contrary to the hypothesis, when barriers to treatment-seeking were investigated, no significant differences between the diagnostic groups were established that would account for the difference in latency to treatment-seeking. Third, for each diagnostic group, stigma was identified as the most impactful barrier.
As anticipated, individuals with a diagnosis of BN and BED reported a substantial delay between the onset of their ED symptoms and seeking ED-specific treatment, which is particularly concerning considering the greater prevalence of these disorders compared to AN. This finding supports the current literature that suggests individuals with BN and BED are less likely to seek treatment (e.g. Fatt et al., 2020; Forrest et al., 2017; Thompson and Park, 2016). Limited research has looked at length of the delay for each specific diagnostic group. Cachelin et al. (2001) found that the average length of delay between symptom onset and first treatment contact was 3.6 years; however, they reported data on a small sample with varied diagnoses. This was shorter than the average length of delay for the overall sample in this study (5.28 years). This study confirms that individuals with EDs face substantial delays to treatment. The results propose that individuals with AN experience a delay of approximately 2.20 years and that individuals with BN and BED are likely to experience average delays of 8.40 and 10.38 years, respectively. This is somewhat aligned with the average length of delay suggested by Austin et al. (2020) after averaging the duration of untreated EDs across 14 studies.
Our findings have serious clinical implications. First, 2 years is a substantial length of time for someone to experience a severe and debilitating illness such as AN without treatment, especially given the onset of illness is likely to occur during a pivotal developmental period and the medical morbidity is so serious. Second, the length of delay more than triples when the perceived severity of symptoms (namely, BMI within the normal weight range) is not as high, and this results in people at healthy body weights being less urgently encouraged to seek treatment or perhaps being able to conceal their ED for longer.
For individuals with AN, obvious signs of emaciation mean that their ED is more likely to be noticed by family and friends and/or picked up by healthcare professionals. Furthermore, the younger presentation age of AN implies that it is often teens presenting to treatment. When these adolescents present to treatment, it is likely to be at the behest of their families, and this is a critical factor that could be shortening their latency to treatment-seeking. Other EDs often tend to be a lot less visible, and as our findings suggest, significant levels of perceived stigma are likely to lead to greater secrecy of symptoms and delayed treatment-seeking.
The average length of delay for the OSFED group was nearly 4 years, and this was not significantly different from the other diagnostic groups. Interestingly, individuals with a diagnosis of OSFED made up the largest group in the study, and the group primarily comprised individuals diagnosed with atypical AN, defined in DSM-5 as an ED where ‘all of the criteria for anorexia nervosa are met, except that despite significant weight loss, the individual’s weight is within or above the normal range’ (APA, 2013: 365). Instances of restrictive EDs where individuals remain within a normal weight range have dramatically increased over the past few years, especially in the adolescent population (Whitelaw et al., 2014). Considering the only differentiating criterion between AN and atypical AN is the individual’s BMI, it is unsurprising that the length of delay was slightly but not significantly longer than those with AN.
When perceived barriers to treatment-seeking were examined (e.g. cost of treatment, stigma and shame, accessibility of treatment, social/work issues, GP’s lack of ED knowledge and personal lack of ED knowledge), no difference in barriers to treatment-seeking between the different disorders was reported. This was surprising considering the substantial difference in length of time to treatment-seeking between the groups. Previous research has suggested that individuals with BED may have experienced barriers related to poor mental health literacy within the community and healthcare settings (Hart et al., 2011; Hepworth and Paxton, 2007; Mond et al., 2007); therefore, higher ratings for barriers such as personal lack of ED knowledge and GP’s lack of ED knowledge were expected. Similarly, individuals with BN were expected to endorse higher ratings of the stigma and shame barriers as well as the social/work issues as they may have been more reluctant to disclose their ED symptoms to family and friends (Thompson and Park, 2016). As such, the findings from this study do not replicate these results. Given this study only included six types of perceived barriers, it is possible that some barriers are not included in the study (e.g. low motivation to change and negative attitudes towards treatment (Ali et al., 2017)), which may have better accounted for the differences between the groups. It is equally probable that the grouping of the perceived barriers was too broad to capture nuanced differences in the experiences of the different diagnostic groups.
Unsurprisingly, stigma and shame related to ED symptomatology were perceived to be the most prominent barriers to treatment-seeking across all diagnostic groups. While stigma and shame have been consistently identified as key barriers to treatment-seeking (Cachelin et al., 2006; Reyes-Rodríguez et al., 2013), more recent literature has noted other barriers as potentially being more prominent (e.g. ‘concern for others’ – Ali et al., 2020; ‘fear of losing control/ fear of change’ – Griffiths et al., 2018; ‘lack of time/lack of perceived need’ – Lipson et al., 2017). This is likely due to variations in the measurement of stigma and shame (i.e. different phrasing and inclusion of different types of barriers in each study) as well as stigma and shame manifesting in different ways for individuals with different EDs. Stigma towards EDs has been associated with attributions of blame and personal responsibility (Puhl and Suh, 2015). The same studies found that when attitudes towards EDs were compared to other psychological illnesses, individuals with an ED (specifically AN and BN) were considered to be more responsible for their illness. Furthermore, individuals with BED were more likely to be blamed for their disorder (when compared to AN and BN) and were perceived to be lacking in self-discipline (Ebneter and Latner, 2013). As obesity commonly occurs among individuals with BED, they often experience weight stigma alongside ED-specific stigma. Attributions of personal responsibility and negative stereotypes (e.g. lacking self-discipline) have also been associated with BN (Ebneter et al., 2011). Individuals with atypical AN experience more severe distress related to eating and body image compared to patients with AN (Sawyer et al., 2016), and it is possible that their level of distress could be exacerbated by their experience of weight stigma.
Ali et al. (2020) found that individuals with AN and BN were more likely to endorse feelings of embarrassment about their symptoms, whereas they infrequently endorsed items of perceived stigma from others. It is important to note that in this study the AN and BN groups were significantly smaller than the BED or Other-ED groups and were likely to have higher symptom severity, so this could account for higher scores on items related to stigma and shame. Furthermore, there is significant conceptual overlap between embarrassment and internalised stigma. Stigma is a complex construct that is likely to be experienced, interpreted and expressed differently depending on the type and severity of ED symptomatology. Stigma is often measured by a single item (as in this study), and therefore this form of measurement may not be sensitive enough to detect sufficient variability within this construct.
It is clear from the research that community beliefs about EDs often perpetuate the interpretation that EDs are a lifestyle choice rather than an illness. Individuals with EDs have reported often experiencing stigmatising attitudes of families and friends in regard to their symptoms (e.g. Akey et al., 2013; Becker et al., 2010; Reyes-Rodríguez et al., 2013). Stigmatisation often results in feelings of intense shame or embarrassment as shown in the study by Cachelin et al. (2001), revealing that women receiving ED treatment experienced higher levels of shame than comparable controls. Furthermore, there is a strong relationship between shame and lack of disclosure in therapy (Swan and Andrews, 2003). Evidence clearly shows that weight bias is still widely prevalent among professionals who treat EDs (Puhl et al., 2014), and this is likely to play a considerable role in reduced treatment-seeking for individuals with BMIs in the healthy or higher ranges. Therefore, our findings corroborate previous research and add to it by suggesting that individuals with any ED diagnosis experience significant perceived stigma, and this may impact their ability to seek help; disclose their symptoms to family, friends and/or health professionals; and access the treatment that they need.
Clinical and theoretical implications
Taken together, there are significant clinical and theoretical implications of these findings. Moderately effective treatments for various EDs are available (Hay et al., 2003, 2014; Murray et al., 2019), yet there is a significant delay in accessing these treatments. Hence, determining the factors that impede treatment-seeking for EDs is imperative in successfully treating these serious and debilitating disorders. This study has highlighted the substantial length of time that symptoms persist prior to accessing treatment. Recovery from EDs, especially from AN, becomes much less likely the longer the duration of the illness (Von Holle et al., 2008); therefore, individuals need to access appropriate ED-specific treatment as soon as possible to increase treatment effectiveness.
The current findings suggest that stigma plays a pivotal role in preventing earlier treatment-seeking. As such, healthcare professionals need to be cognisant of the perceived stigmatisation individuals with EDs may have experienced and ensure sensitivity when assessing and treating these individuals. Increased psychoeducation regarding EDs needs to be provided to both treating clinicians and the community to aid earlier detection of symptoms and reduce stigma.
From a theoretical perspective, it is noteworthy that the OSFED group, primarily comprised of individuals with atypical AN, was the largest group in this study. Despite not being underweight, research has shown that individuals with atypical AN experience significant physical and psychological complications (Sawyer et al., 2016). The prevalence of atypical AN in our sample may be reflective of a changing ED landscape. Growing diet culture, particularly in Western society, is likely to have exacerbated the distress associated with wanting to be thinner and led to intense fears of fatness experienced by individuals with atypical AN. A rapid growth in the number of adolescent atypical AN patients in inpatient care settings has been reported (Whitelaw et al., 2014), with one-third of inpatients having this diagnosis (Peebles et al., 2017). The DSM-5 attempted to better define EDs by making significant changes to the eating disorders not otherwise specified (EDNOS) category (now OSFED), by adding BED as a standalone ED and by relaxing the classification criteria of AN (APA, 2013). However, given the increasing prevalence of atypical AN and the fact that it is only captured within the OSFED group, it may be time to consider the utility of this diagnosis and contemplate better defining this growing category to ensure individuals receive the most appropriate treatment.
Limitations
Several limitations of this study should be considered when interpreting the findings. First, the small and unequal sample sizes of the diagnostic groups limited the scope of statistical analysis and interpretation, and it is therefore necessary to replicate the findings in a larger sample to ensure validity. Overall, the descriptive variables (e.g. age and BMI) in our sample were consistent with the lifetime prevalence estimates found in previous studies (e.g. Hudson et al., 2007). Previous epidemiological studies indicated that AN and BN are more common in females than males, but BED symptoms are more common in males (Striegel et al., 2009). Our study revealed a significantly smaller ratio of males to female than has previously been suggested, with males accounting for only 3–8% of each diagnostic group. Forrest et al. (2017) found that less than 10% of males with an ED sought treatment; therefore, it is understandable that the number of males included in the study is small given it is a treatment-seeking sample. It would be important to replicate these findings in a larger sample to explore whether the proportion of treatment-seeking males is potentially less than has previously been proposed.
Second, all participants in this study were accessing treatment at private ED facilities in metropolitan areas. Therefore, while this study captured barriers that were ultimately overcome, we did not assess potentially insurmountable barriers among people living with EDs in the community who have never accessed treatment. Similarly, it is unlikely that cost-related or geography-related barriers limiting the accessibility of treatment would have been endorsed in this sample given participants were accessing private healthcare.
Finally, as previously discussed, this study only included six types of perceived barriers to treatment-seeking; however, it is conceivable that other barriers not included in this study could have potentially differentiated the diagnostic groups (e.g. individual characteristics such as motivation and perceived control). While this study was being undertaken, Ali et al. (2020) created and used a more comprehensive measure that incorporated several questions for each barrier in order to capture the complex nature of each construct. Different measures in each study may account for some of the variation in results. This highlights the importance of consistency in measurement to allow for more reliable and generalisable findings. The measure in this study has not been validated in this population in its altered form. The Cronbach’s alpha was quite low when using this scale; however, as each barrier was interpreted separately, this did not significantly impact the results. As with all self-report measures, recall difficulties can be a confounding factor, but this is standard practice in research assessing treatment-seeking.
Recommendations for future research
This was an important study in an under-researched area, and it is imperative to reproduce and further these findings in forthcoming research. It would be essential to replicate this study in a larger and more representative sample to establish the generalisability of the results. Future studies should consider conducting this research in a country with no publicly funded national healthcare system, in both urban and regional areas, and with individuals from diverse ethnicities and social-economic backgrounds to capture the full spectrum of barriers that individuals with EDs may face.
Future research should also consider including additional perceived barriers that were not included in this study (e.g. personal characteristics) and attempt to tease out the impact of the involvement of others in treatment-seeking (e.g. involvement of parents/carers/family members in recognising symptoms and initiating treatment). Moreover, future studies should attempt to better understand the role of stigma for each disorder, especially how the latency to treatment-seeking for BED, BN and atypical AN could be explained by secrecy around illness and symptoms, as well as shame and fear of stigmatisation from the community and health professionals.
Previous research conducted in this area has varied greatly in terms of quality and methodology (e.g. behavioural coding, self-report questionnaires and clinical interviews; Regan et al., 2017), so it would be useful to develop a standardised measure to assess ED-specific treatment-seeking that can be employed across various populations to ensure consistency of findings. This study modified the questionnaire developed by Thompson and Park (2016) to be appropriate for the Australian context; however, more research is needed to determine the validity and reliability of this measure.
Conclusion
This study highlights the substantial and damaging delay in seeking and receiving appropriate ED-specific treatment. Our findings suggest that while individuals with AN experience a delay of over 2 years on average, individuals with BN and BED face significantly longer delays to treatment-seeking. Stigma appears to be a significant barrier preventing individuals with all ED diagnoses from seeking treatment; however, further research is needed to investigate other factors contributing to this delay.
Footnotes
Appendix 1
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: S.T. is the Co-Chair of the Takeda Virtual Clinical Advisory Board for BED and has also received honoraria for commissioned reports, public speaking engagements, webinars and consultancy. He also receives honoraria from Hogrefe and Huber, McGraw Hill and Taylor and Frances for published work. He is a member of the Commonwealth Technical Advisory Committee on Eating Disorders and a mental health consultant to the Commonwealth Department of Veterans Affairs. He is a member of the steering committee of the National Eating disorders Collaboration. S.T. is the cofounding editor-in-chief of the Journal of Eating Disorders. P.H. receives/has received sessional fees and lecture fees from the Australian Medical Council, Therapeutic Guidelines publication and New South Wales Institute of Psychiatry, and royalties/honoraria from Hogrefe and Huber, McGraw Hill Education, and Blackwell Scientific Publications, Biomed Central and PlosMedicine, and she has received research grants from the NHMRC and ARC. She is Chair of the National Eating Disorders Collaboration Steering Committee in Australia (2019–) and was Member of the ICD-11 Working Group for Eating Disorders (2012–2019) and was Chair Clinical Practice Guidelines Project Working Group (Eating Disorders) of RANZCP (2012–2015). She has prepared a report under contract and consulted to Takeda Pharmaceuticals. A.H., D.M., C.B., S.B., M.G., G.H. and C.T. have no conflict of interest to declare.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.