
Abstract
Introduction:
An association between schizophrenia and urbanicity has long been observed, with studies in many countries, including several from Denmark, reporting that individuals born/raised in densely populated urban settings have an increased risk of developing schizophrenia compared to those born/raised in rural settings. However, these findings have not been replicated in all studies. In particular, a Western Australian study showed a gradient in the opposite direction which disappeared after adjustment for covariates. Given the different findings for Denmark and Western Australia, our aim was to investigate the relationship between schizophrenia and urbanicity in these two regions to determine which factors may be influencing the relationship.
Methods:
We used population-based cohorts of children born alive between 1980 and 2001 in Western Australia (N = 428,784) and Denmark (N = 1,357,874). Children were categorised according to the level of urbanicity of their mother’s residence at time of birth and followed-up through to 30 June 2015. Linkage to State-based registers provided information on schizophrenia diagnosis and a range of covariates. Rates of being diagnosed with schizophrenia for each category of urbanicity were estimated using Cox proportional hazards models adjusted for covariates.
Results:
During follow-up, 1618 (0.4%) children in Western Australia and 11,875 (0.9%) children in Denmark were diagnosed with schizophrenia. In Western Australia, those born in the most remote areas did not experience lower rates of schizophrenia than those born in the most urban areas (hazard ratio = 1.02 [95% confidence interval: 0.81, 1.29]), unlike their Danish counterparts (hazard ratio = 0.62 [95% confidence interval: 0.58, 0.66]). However, when the Western Australian cohort was restricted to children of non-Aboriginal Indigenous status, results were consistent with Danish findings (hazard ratio = 0.46 [95% confidence interval: 0.29, 0.72]).
Discussion:
Our study highlights the potential for disadvantaged subgroups to mask the contribution of urban-related risk factors to risk of schizophrenia and the importance of stratified analysis in such cases.
Introduction
The association between schizophrenia and urbanicity has a venerable history in psychiatric epidemiology. It has long been appreciated that those who develop schizophrenia may subsequently move into inner city and densely populated settings: most probably, this is a consequence of disability-related decline in socioeconomic status (Faris and Dunham, 1939; Jarvis, 1851). In more recent decades, observational epidemiology based in countries such as Denmark, Sweden and the Netherlands has identified that those who are born and/or raised in densely populated urban settings have an increased risk of subsequently developing schizophrenia (Radua et al., 2018). In particular, studies based on Danish registers have found that urbanicity of the place of birth and longer duration of being raised in urban settings both contributed to a higher risk of schizophrenia (Pedersen, 2015; Pedersen and Mortensen, 2006b; Vassos et al., 2012, 2016). More recent population-based studies have found that individuals with higher polygenic risk scores related to risk of schizophrenia (but without the clinical diagnosis) are more likely to live in more densely populated settings (Engemann et al., 2020; Fan et al., 2018; Paksarian et al., 2018). However, this effect is relatively small, and it is not sufficient to explain the association between the urbanicity and risk of schizophrenia (Plana-Ripoll et al., 2018).
Recently, some studies have reported findings which suggest that the apparent urban–rural gradient detected in Nordic and northern European countries is not found in other sites. For example, a recently published multi-site incidence study (Jongsma et al., 2018) confirmed substantial variation in the incidence of first episode psychosis across 17 catchment areas in six countries. However, within these sites, there was no association with urbanicity, as defined by population density. Indeed, the expected urban–rural pattern was only confirmed for England and the Netherlands, while no significant association was found for Spain or France, and an inverse (urban protective) finding was identified in Italy. A study based in Western Australia also failed to confirm the expected urban–rural gradient, showing a gradient in the opposite direction which disappeared after adjustment for a range of covariates (Morgan et al., 2019).
The precise nature of the underlying risk factors that underpin these findings remain poorly understood (McGrath and Scott, 2006). Candidates range from environmental exposures related to air pollution (Engemann et al., 2019, 2020; Horsdal et al., 2019; Khan et al., 2019) to socially mediated risk factors related to marginalisation and social stressors (Kirkbride et al., 2010, 2014).
We had the opportunity to explore the association between urbanicity of birth and risk of schizophrenia using two population-based health registers from Denmark and Western Australia. The two sites differ markedly on a number of factors that are of interest to the aims of this study. Western Australia, a state within the Commonwealth of Australia, has a small population (approximately 2.6 million) spread over a very large area (2.5 million square kilometres). It is, geographically, one of the most isolated populations in the world, surrounded by ocean and desert. Population density is non-homogeneous and highly concentrated, with 74% of its inhabitants living in the greater metropolitan area of its capital city, Perth. Western Australia also has many remote towns and small settlements of Aboriginal Indigenous Australians. The prevalence of current common mental disorders in Indigenous Australians is more than four times that of the general Australian population (Nasir et al., 2018). There is less information on the prevalence of schizophrenia in these groups; however, recent studies have reported markedly high prevalence estimates for psychosis (Gynther et al., 2019). In contrast, Denmark is a small homogeneous country with a larger population (approximately 5.8 million) spread over a relatively small area (approximately 43,000 square kilometres). Distances are small and most people live within 25 km of a city with more than 30,000 inhabitants. Both Australia and Denmark have universal health care but, because Western Australia is 58 times the size of Denmark with only half the number of people, its population is much more sparely distributed outside of the capital city, where people experience reduced access to health services, particularly in remote areas. Based on the weight of evidence from the literature, we predicted that the risk of schizophrenia would be higher in urban settings in Denmark but not Western Australia, and that this difference may be influenced by the presence of Aboriginal Australians within the Western Australian setting.
Methods
Study population
We designed a population-based cohort study including 1,786,658 children born alive between 1980 and 2001: N = 428,784 born in Western Australia and N = 1,357,874 born in Denmark. Children were categorised depending on the level of urbanicity of their mother’s residence at time of birth and were followed-up through to 30 June 2015 to estimate their rates of schizophrenia.
Registers in Western Australia
In Western Australia, children were identified on the Midwives’ Notification System (Gee and Dawes, 1994), which includes mandatory, prospectively collected data on all infants born in Western Australia. The study was designed to compare children of mothers with severe mental illness to children of mothers with no recorded mental health contacts; consequently, data on children of mothers with other mental disorders were not provided to the investigators for inclusion in analysis. Mothers with a severe mental illness (see Supplementary Table 1) were identified through linkage of records on the Midwives’ Notification System to the Hospital Morbidity Data Collection and Mental Health Information System, which cover records of all public and private inpatient hospital admissions, as well as public outpatient and ambulatory care contacts with mental health services across the State, dating back to 1966. Additional covariates used in analyses were obtained from State registers linked to the Midwives’ Notification System. Indigenous status of the child was scored as Aboriginal if the child and/or either parent was identified as Aboriginal in any of the data sources available. We note that the term ‘Aboriginal’ is used throughout this article in accordance with Western Australian government best practice for describing Australian Indigenous populations in Western Australia. Linkage was carried out by the Data Linkage Branch of the Western Australian Department of Health. Quintiles of socioeconomic disadvantage were captured using census-derived area level measures (Australian Bureau of Statistics, 2008). The date of the census used was the census closest in time to the date of birth. Full details on the linked registers used to establish and characterise this birth cohort have been published (Di Prinzio et al., 2018; Morgan et al., 2011). The diagnostic system used was the International Classification of Diseases (Eighth Revision; ICD-8) up to the end of 1978, Ninth Revision (ICD-9) from 1979 to 30 June 1999, and Tenth Revision (ICD-10) from 1 July 1999 onwards. See Supplementary Table 1.
Registers in Denmark
Since 1968, the Danish Civil Registration System (Pedersen, 2011) has maintained information on all residents, including sex, date of birth, continuously updated information on vital status, and a unique personal identification number that can be used to link information from various national registries. From this register, we obtained the linkage of each child to their parents and information about municipality at birth. Information on maternal socioeconomic characteristics at the time of the child’s birth was obtained from Statistics Denmark (annual income, highest education achieved, labour market affiliation and marital status). Finally, information on schizophrenia and parental mental disorders was obtained from the Danish Psychiatric Central Research Register (Mors et al., 2011), which contains data on all admissions to psychiatric inpatient facilities since 1969 and visits to outpatient psychiatric departments and emergency departments since 1995. The diagnostic system used was the Danish modification of the International Classification of Diseases, Eighth Revision (ICD-8) from 1969 to 1993, and Tenth Revision (ICD-10) from 1994 onwards. See Supplementary Table 1.
Assessment of urbanisation at birth
Urbanicity area categories in Western Australia were classified according to criteria used by the Australian Bureau of Statistics (2006) as: (1) Major City, (2) Inner Regional, (3) Outer regional, (4) Remote and (5) Very Remote. This classification is based on the road distance of a location from the nearest population centres providing access to goods and services, taking into account population size. In Denmark, municipality at birth was classified according to degree of urbanisation in five categories: (1) capital, (2) capital suburb, (3) provincial cities, (4) provincial towns and (5) rural areas.
Schizophrenia diagnoses
Children in both locations were considered to have schizophrenia if they were diagnosed with ICD-10 codes F20, F21, F23.1, F23.2 and F25 (or corresponding ICD-8 or ICD-9 code 295). The date of onset for each disorder was defined as the date of first diagnosis. See Supplementary Table 1.
Statistical analysis
Children were categorised depending on urbanicity at time of birth and were followed-up from birth until a diagnosis of schizophrenia, death, emigration (available only in Denmark), or 30 June 2015, whichever occurred first. Rates of being diagnosed with schizophrenia for each urbanicity category were compared by means of hazard ratios (HRs) and 95% confidence intervals (CIs) separately for Western Australia and Denmark, estimated using Cox proportional hazards models stratified on birth year, that is, we assumed different baseline rates for each birth year. As a mother may have more than one child in the database, we used robust standard errors to adjust the CI for possible correlation within sibships. Models were adjusted for sex, maternal and paternal age at birth, maternal and paternal history of mental disorders before birth (classified according to the model shown in Supplementary Table 1), maternal marital status at time of birth and maternal socioeconomic characteristics at birth. Finally, models in Western Australia were further stratified by Aboriginal status of the child to investigate a potential effect measure modification. All analyses were performed on a secured internal platform (Western Australia data) and Statistics Denmark platform (Danish data) using STATA version 15.1.
Ethics and data protection
This study was approved by the Western Australian Department of Health Human Research Ethics Committee (2011/75), the University of Western Australia Human Research Ethics Committee (RA/4/1/1322), the Danish Data Protection Agency and the Danish Health Data Authority. According to Danish law, informed consent is not required for register-based studies. All data were de-identified and not recognisable at an individual level.
Results
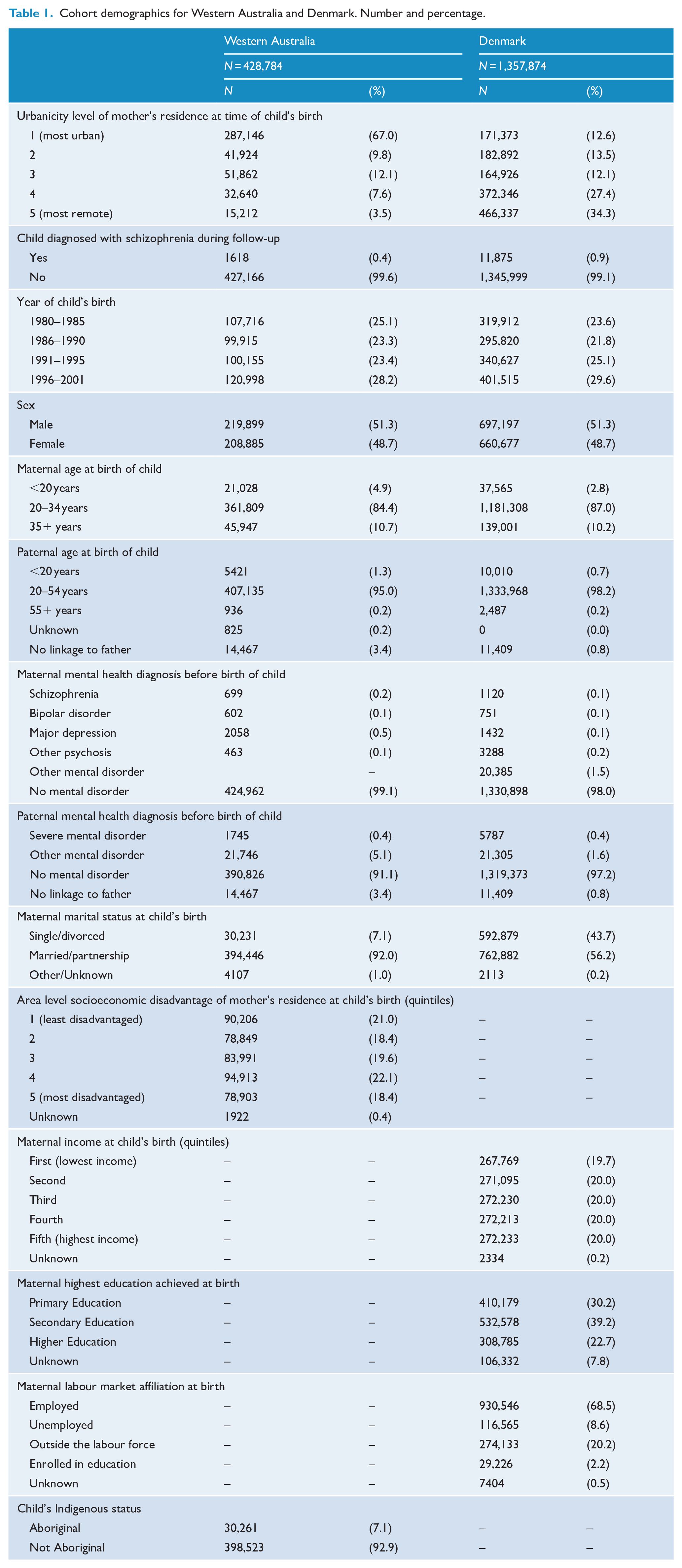
There were 1,786,658 children followed-up for a total of 43.0 million person-years (11.3 million in Western Australia and 31.7 million in Denmark); the longest individual follow-up time was 35.5 years. In Western Australia, 287,146 (67.0%) children were born in the most urban areas, compared to only 171,373 (12.6%) in Denmark. However, the number of children born in the most remote areas was 15,212 (3.5%) in Western Australia and 466,337 (34.3%) in Denmark. During follow-up, 1618 children in Western Australia (0.4%; 0.3% among non-Aboriginal children and 1.0% among Aboriginal children) and 11,875 children in Denmark (0.9%) were diagnosed with schizophrenia (Table 1). Baseline characteristics by urbanicity level at birth for children in Western Australia and Denmark separately are shown in Supplementary Tables 2 and 3.
Cohort demographics for Western Australia and Denmark. Number and percentage.
In Western Australia, being born in remote areas – compared to urban areas – was not associated with lower rates of schizophrenia. For example, those born in the most remote areas experienced 2% higher rates of schizophrenia than those in born in the most urban areas (HR = 1.02 [95% CI: 0.81, 1.29]). On the contrary, being born in remote areas in Denmark was associated with lower schizophrenia rates (those in the most remote areas experienced 38% lower schizophrenia rates: HR = 0.62 [95% CI: 0.58, 0.66]). Results for all urbanicity categories are shown in Table 2.
Risk of schizophrenia by urbanicity level of mother’s residence at child’s birth including, for Western Australia, by Indigenous status. Hazard ratios and 95% confidence intervals.
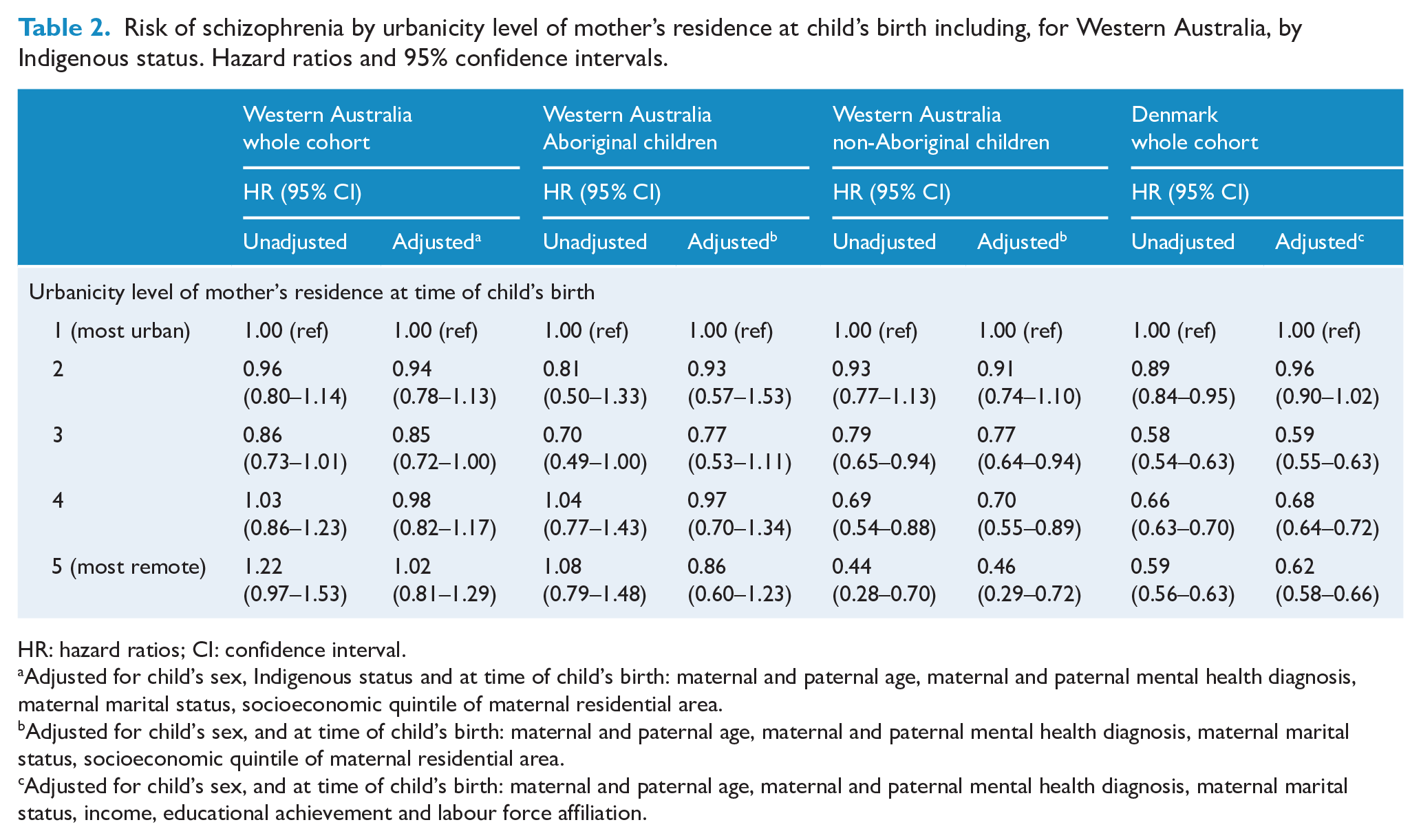
HR: hazard ratios; CI: confidence interval.
Adjusted for child’s sex, Indigenous status and at time of child’s birth: maternal and paternal age, maternal and paternal mental health diagnosis, maternal marital status, socioeconomic quintile of maternal residential area.
Adjusted for child’s sex, and at time of child’s birth: maternal and paternal age, maternal and paternal mental health diagnosis, maternal marital status, socioeconomic quintile of maternal residential area.
Adjusted for child’s sex, and at time of child’s birth: maternal and paternal age, maternal and paternal mental health diagnosis, maternal marital status, income, educational achievement and labour force affiliation.
However, when we stratified the Western Australia sample by Indigenous status, we found that the association between urbanicity and rate of schizophrenia among non-Aboriginal children was similar to the pattern in Denmark (Table 2 and Figure 1). For example, non-Aboriginal children born in the most remote areas experienced schizophrenia rates 54% lower than children born in the most urban areas (HR = 0.46 [95% CI: 0.29, 0.72]). For Aboriginal children, while there was no clear association between urbanicity and schizophrenia rates (Table 2 and Figure 1), we observed that schizophrenia rates were comparatively high across all levels of urbanicity (data not shown). Supplementary Tables 4 and 5 present the adjusted HRs for all covariates.
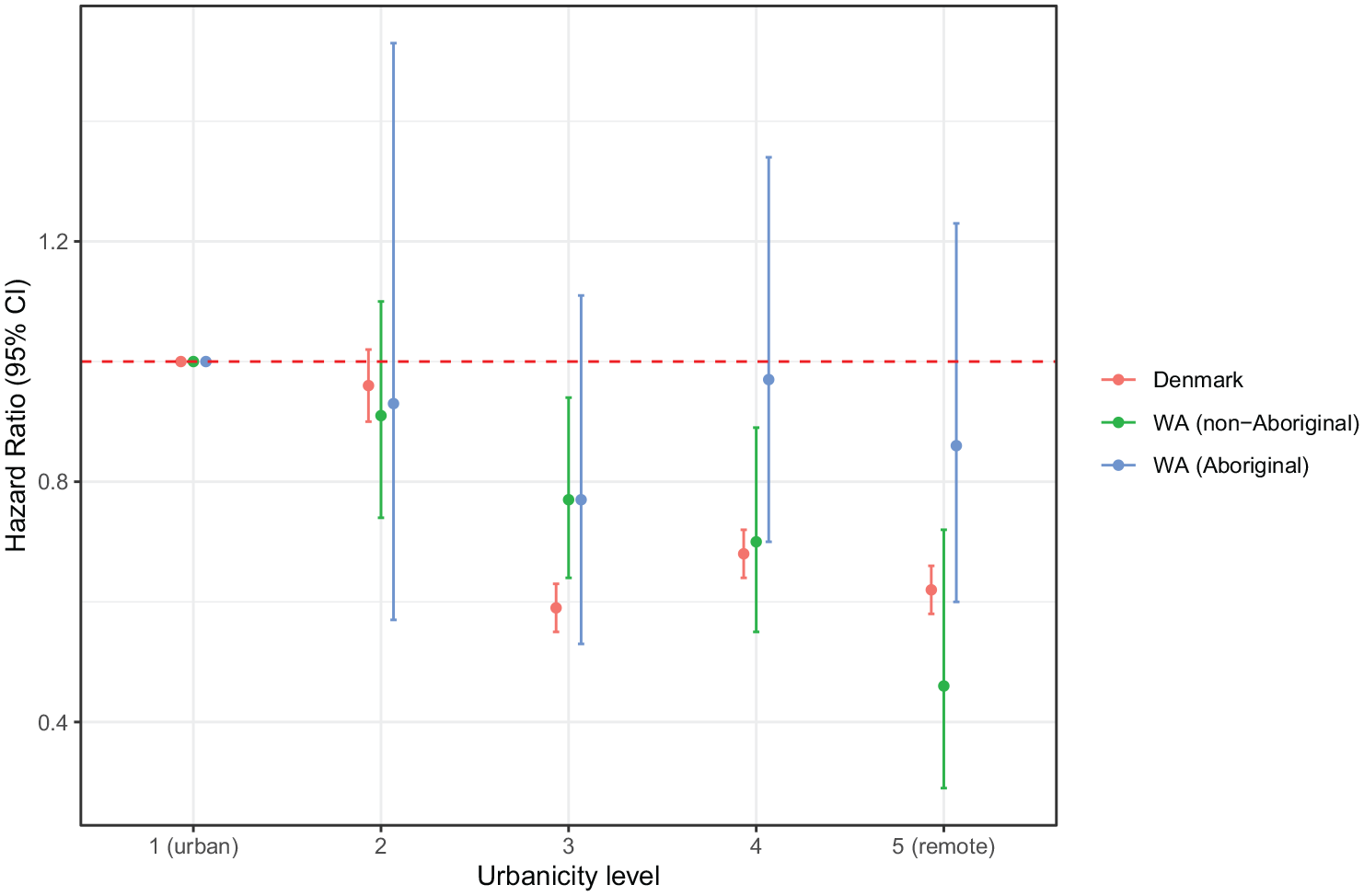
Risk of schizophrenia by urbanicity level of mother’s residence at child’s birth for Denmark and Western Australia.
Discussion
Consistent with previous studies, we found robust support for an association between urbanicity and risk of schizophrenia in Denmark (Pedersen and Agerbo, 2005; Pedersen and Mortensen, 2001, 2006a, 2006b). However, the data from Western Australia revealed nuances within the population related to Indigenous status. The non-Aboriginal population showed the expected significant urban–rural gradient consistent with the Danish sample. For example, compared to those in the most urban setting (namely, Perth), those born in the most remote settings had a markedly decreased risk of schizophrenia (adjusted HR = 0.46 [95% CI: 0.29, 0.72]). However, Aboriginal cohort members had a markedly increased risk of schizophrenia compared to non-Aboriginal members, but no significant gradient of risk associated with degree of urbanicity.
There are several particular issues that warrant attention. First, in these population-based cohorts selected using very similar protocols, the proportion of schizophrenia cases in the two regions differed (0.4% vs 0.9% in Western Australia and Denmark, respectively). While the estimates for Denmark are consistent with previous studies (Pedersen et al., 2014), the proportion for Western Australia is low, despite the inclusion of the at-risk Aboriginal population. It is possible that the non-inclusion of children of women with non-psychotic disorders in the Western Australian data may have partially contributed to this, as well as some loss to follow-up through out-migration. However, although high quality incidence estimates for Australia are sparse (McGrath et al., 2004), Australian prevalence studies (Jablensky et al., 2000; Morgan et al., 2014) have also reported lower estimates compared to many other nations (Jongsma et al., 2019; McGrath et al., 2004). Such differences are also in keeping with the observed variation in the incidence and prevalence of schizophrenia across sites which has been described in the literature (McGrath, 2006).
Our study highlights how particular disadvantaged subgroups may mask the contribution of urban-related risk factors to the risk of schizophrenia. In Western Australia, only when the analyses were stratified by Aboriginal status did we observe the commonly-reported urban-rural gradient of risk – in the non-Aboriginal cohort only. The high rates of schizophrenia among Aboriginal Western Australians, observed across all levels of urbanicity, have impacted on our findings prior to stratification. These high rates reflect psychosis prevalence data for Aboriginal and Torres Strait Islander communities in remote Northern regions of the State of Queensland where rates were five times higher than population rates for men and three times higher for women (Gynther et al., 2019). Similarly, New Zealand data show that the incidence of schizophrenia is twice as high among Indigenous Māori people compared to non-Māori (Tapsell et al., 2018). Recently, Charlson et al (2021) supplemented findings from their earlier paper (Gynther et al., 2019) with new data showing high rates in the same sample for a range of biological, neurodevelopmental, environmental and contextual factors implicated in psychosis vulnerability and onset. It is highly probable that these findings extend beyond remote Northern Queensland and that, irrespective of level of urbanicity, Aboriginal people are much more likely than non-Aboriginal Australians to be exposed to a range of environmental risk factors for schizophrenia such as obstetric complications, social adversity and psychosocial stress, trauma and abuse (Zubrick et al., 2004), all of which have been associated with an increased risk of schizophrenia (Cannon et al., 2002; Morgan and Gayer-Anderson, 2016; Selten et al., 2017; Wicks et al., 2005). These may also include stressors specific to many Indigenous populations related to social upheaval, loss of cultural identity through loss of country and anomie; of relevance, Grynther and colleagues found that rates were particularly high in communities that, historically, had been resettled onto mission stations and similar reserves (Gynther et al., 2019). In addition, cross-cultural factors may result in differential diagnostic practices for Aboriginal compared to non-Aboriginal cohorts, although Grynther et al. suggest the impact was very small in their study. In general, even though previous Danish studies have found that the urban–rural risk gradient persists when adjusted for a range of socioeconomic factors such as parental education and income, it is likely that the complex interplay of factors affecting Aboriginal children cannot be captured in relatively simple measures and require independent study.
Our study had the advantage of access to large, population-based cohorts, which is important to ensure adequate power to avoid Type II errors when exploring hypotheses related to a low prevalence disorder such as schizophrenia. Moreover, information was collected prospectively on the registers, and the risk for selection bias was negligible. Although diagnoses of schizophrenia were based on clinical diagnoses rather than diagnostic interviews, it is unlikely that any misclassification would have been differential across the different urbanicity groups. While we were able to harmonise many aspects of design across the two samples, there were several coding differences. We were unable to harmonise de facto relationships within the variable marital status, with Denmark counting de facto couples as single. Nonetheless, in each dataset, the distribution for marital status remained relatively consistent across levels of urbanicity, suggesting that this coding difference did not influence on our findings. In addition, the construction of categories of urbanicity reflected vast geographical differences between the two sites: even so, we observed very similar patterns, with risk of schizophrenia decreasing with decreasing level of urbanicity in both the non-Aboriginal Western Australian sample and the Danish sample. Finally, the Western Australian cohort did not include the offspring of women with a recorded diagnosis of a non-psychotic disorder. This may have had some impact on the lower rates of schizophrenia reported although, as noted above, lower rates have been reported in other Australian data. It is also possible that there was some misclassification of cases in Western Australia due to unrecorded loss to follow-up of cohort members who had moved out of the State. However, not only does Western Australia have one of the highest rates of in-migration and one of the lowest levels of out-migration of all the Australian states (Morgan et al., 2011), but also there is no reason to assume that such movement would have varied across outcome groups to introduce a misclassification bias.
We have demonstrated the utility of exploring research questions in disparate samples. The findings in Western Australia highlight how subgroups can contribute to the direction of the findings on urbanicity as a risk for schizophrenia and, in this case, on the importance of stratifying analyses on Indigenous status. While our study cannot draw strong conclusions as to the nature of the factors contributing to the urban-rural gradient, we hope it will stimulate the next generation of research in this area.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211009615 – Supplemental material for Factors that contribute to urban–rural gradients in risk of schizophrenia: Comparing Danish and Western Australian registers
Supplemental material, sj-docx-1-anp-10.1177_00048674211009615 for Factors that contribute to urban–rural gradients in risk of schizophrenia: Comparing Danish and Western Australian registers by Oleguer Plana-Ripoll, Patsy Di Prinzio, John J McGrath, Preben B Mortensen and Vera A Morgan in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We thank the Data Linkage Branch of the Western Australia (WA) Department of Health for data linkage and extraction of the WA data, and for client support. We also thank the custodians of the WA Hospital Morbidity Data Collection, Mental Health Information System, the WA Midwives Notification System and the WA Registry of Births, Deaths and Marriages for the provision of data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Western Australian work was supported by grants from the Australian National Health and Medical Research Council (#303235; #458702; APP1002259; APP1080606) and March of Dimes (#12-FY04-48; #12-FY07-224). John McGrath is supported by the Danish National Research Foundation (Niels Bohr Professorship). Oleguer Plana-Ripoll has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Sklodowska-Curie grant agreement No 837180. The Western Australian-Danish collaboration was supported by the Raine Medical Research Foundation and a 2019 Cockell Research Collaboration Award. The funders had no role in the design and conduct of the study, collection, management, analysis, interpretation of the data, nor in the preparation, review or approval of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.