
Abstract
Objective
The Psychological Assistance Service (PAS) opened in Newcastle, New South Wales in 1997 as a clinical service for the assessment and treatment of young people at high risk of psychosis and those experiencing a first psychotic episode. The aim of this paper is to describe the assessment protocol of PAS, which is strongly influenced by the neurodevelopmental perspective on early onset psychosis.
Method
The systematic assessment of patients referred to PAS using a protocol over a 2 week period is described. The protocol includes a narrative history, structured diagnostic interview, quantitative assessment of symptoms and other clinical features, a neurological examination and comprehensive neuropsychological test battery.
Results
The clinic has received over 250 referrals in a 2 year period and accepted 116 patients for a full assessment, of whom 60 were deemed to be ‘at-risk’ of psychosis and 56 were experiencing their first psychotic episode. Both groups were similar with respect to gender and there were minor age differences. The first-episode group experienced more reality distortion, schizotypal and negative symptoms. While both groups showed some neuropsychological and neurological impairment, there were no statistically significant differences between the groups on these variables except for a test of executive functioning in which the first-episode group was more impaired than the ‘at-risk’ group. A low rate of conversion to psychosis occurred in the ‘at-risk’ group.
Conclusions
The minor differences between the two groups may have been related to relatively small sample sizes, although some similarities between the groups were to be expected. The low rate of conversion to psychosis in the ‘at-risk’ group is discussed. Further analyses using larger samples are necessary to determine the validity of the various ‘at-risk’ categories and this will involve following a sufficiently large sample over an adequate time. The most efficient way of doing this would be to pool data across centres with comparable early intervention programs.
High-risk studies and epidemiological research indicate that risk factors for schizophrenia comprise family history (i.e. genetic risk), season of birth, urban birth, migrant/minority status, perinatal (including obstetric) complications, neurodevelopmental deficits, family dysfunction, and behavioural (mal) adjustment [1,2]. However, because these factors entail quite small increases in risk relative to the general population and most, if not all, have low specificity, the gap between our knowledge at this level and clinically useful risk factor screening for preventive purposes appears to be very large. The Personal Assessment and Crisis Evaluation (PACE) Clinic in Melbourne (Australia) described by Phillips and associates in this issue (pp. S164–S169) can be seen as an attempt to bridge this gap by identifying ‘at-risk mental states’ as the basis on which therapeutic interventions can be implemented to prevent or substantially delay the onset of schizophrenia.
A clinical service modelled on the PACE clinic was opened at Newcastle (Australia) in January 1997, the Psychological Assistance Service (PAS). It differed from PACE by including people experiencing a first episode of psychosis in addition to those with ‘at-risk mental states’. From the outset it was determined to adopt entry criteria and assessment methods that were compatible with those of PACE so that comparisons could be made between the two services. It was also decided to include additional assessment procedures in several areas so that PAS might also be in a position to make a unique contribution to the field of early psychosis prevention. The present paper provides a description of the operations of PAS and the assessment protocols used, including the methods of measuring schizophrenia risk factors. Some preliminary results from the data collected over the first years of the clinic's operation are also presented.
Neurodevelopmental framework
The neurodevelopmental theory of schizophrenia proposes that this disorder is the result of neurological dysfunction with possible genetic antecedents and/or origins in various forms of developmental insult in early life [3,4]. Consequently, a schizophrenia risk factor screening protocol should include measures of neurodevelopmental vulnerability to schizophrenia.
Epidemiological research has shown an association between exposure to foetal or perinatal insult and subsequent development of schizophrenia [5,6]. There is evidence of an increased incidence of obstetric complications in those who develop schizophrenia [7] and this may either be a manifestation of the underlying genetic vulnerability [8,9] or an agent influencing the development of the schizophrenia [10]. A measure of obstetric complications was therefore incorporated in the PAS assessment protocol.
Non-localising neurological (or ‘soft’) signs are frequently identified in patients with schizophrenia [11–13]. These abnormalities in the performance of sensory and motor tasks are thought to indicate nonspecific global cerebral dysfunction [14]. They occur with greater frequency in schizophrenia compared to controls [15–17] and those with affective disorders [11,18]. They are also found in high-risk groups [13,19–22]. These findings have led to the conclusion that neurological ‘soft’ signs may be a marker for the underlying neurodevelopmental impairment of schizophrenia [23,24]. Thus, the measurement of nonlocalising neurological signs was regarded as an important component of a schizophrenia risk factor screening protocol.
Premorbid adjustment can also be considered within a neurodevelopmental framework. Among genetically defined high-risk samples there is evidence for a considerable degree of variably defined poor premorbid functioning [25–28]. This is also found in case control cohorts [29,30] and in behaviourally defined high-risk groups [31]. Neurointegrative deficits, with their behavioural effects, have also been reported in genetic high-risk groups [20,26,27]. Patients with schizophrenia have significantly poorer premorbid adjustment compared to those with affective disorder and other controls [32,33]. There are also associations between poor premorbid functioning and poor prognosis [34–36], negative symptoms [37,38], and early onset of schizophrenia [37]. This has led to the conclusion that poor premorbid functioning may be another marker for the neurodevelopmental deficit underlying schizophrenia [1,25]. Consequently, assessment of premorbid adjustment has a justifiable place in a schizophrenia risk factor screening protocol within a neurodevelopmental framework.
Neuropsychological impairment is the other main area for measurement of risk of schizophrenia within the neurodevelopmental framework. Impaired intellectual functioning in preschizophrenic children has been well established [39–41]. In addition, poor verbal, organisational and speech performance, as well as other perceptual and cognitive deficits have been identified in preschizophrenic or high-risk children and adolescents [40–43]. Delay in the achievement of motor milestones [20,42,44] and abnormal motor coordination [22] have also been identified in premorbid and high-risk groups. Neuropsychological impairment in schizophrenia, particularly in memory and executive functions, is well documented in the literature (see Heinrichs and Zakzanis for a review [45]). Thus, the PAS schizophrenia risk factor protocol incorporated a thorough neuropsychological assessment.
Clinical measurement
As previously suggested, the selection criteria for entry into the PAS program are virtually identical to those used in the PACE clinic [46], with the exception that young people in the early stages of a first psychotic episode are also accepted by PAS. Those first-episode patients who are floridly psychotic, severely disturbed and unable to be managed using outpatient clinic appointments are referred directly to the hospital or a 24-h community mental health team, without undergoing assessment in PAS. The three ‘at-risk’ groups are defined as follows: (i) group A, a combination of a first- or second-degree relative with a history of any psychotic disorder or schizotypal personality, both as defined by DSM-IV criteria [47], and nonspecific psychological symptoms and a decline in functioning of 30 or more points on the Global Assessment of Functioning (GAF) scale [48]; (ii) group B, attenuated psychotic (i.e. schizotypal) symptoms of recent onset [46]; and (iii) group C, transient self-limited psychotic symptoms of less than one week's duration (BLIPS) [46]. First psychotic episode patients are defined by the presence of psychotic symptoms of more than one week's duration.
The inception of a new service, which is distinct from the rest of mainstream mental health services in that its primary function is to identify young people at risk of psychosis rather than those with established psychotic illness, presents certain challenges. Foremost among these is the establishment of a network that refers patients who have a high likelihood of meeting the selection criteria of PAS. Therefore, from the outset and at regular intervals thereafter, clinical staff have actively engaged potential referral sources to provide them with information about PAS, its purposes, mode of operation and selection criteria. This outreach included providing education sessions for general practitioners, school counsellors and mental health workers, as well as developing networks in the general community through community health centres, university health and counselling services, and nongovernment youth services. Information brochures and posters were widely distributed, and staff attended public events to disseminate information about the service.
All new referrals to the service are discussed at regular team meetings to assess their likelihood of meeting the selection criteria. Those deemed definitely unsuitable (e.g. those whose difficulties are clearly due to a pre-existing nonpsychotic condition such as a pervasive developmental disorder) are referred to a more appropriate agency. Those who appear likely to meet PAS criteria are offered an initial interview.
The initial interview is of approximately one hour's duration, and involves a clinician taking a clinical history and performing a mental status examination. Based on the information provided at the initial interview, and following discussion at a further team meeting, patients who are deemed likely to meet the PAS selection criteria are accepted for a full assessment. Those who do not appear likely to meet these criteria are referred elsewhere.
Full assessments are generally completed in approximately 2 weeks. They entail three clinical interviews with the patient, an informant interview (preferably with the patient's mother), a neurological assessment, and two neuropsychological testing sessions. The patients also complete two self-report books containing a variety of measures of symptoms, personality, coping style and level of functioning. The latter are included to gain a picture of the patient's healthy attributes, which can be built upon in the course of treatment. A complete description of the assessment battery is provided in Table 1.
The Psychological Assistance Service assessment protocol
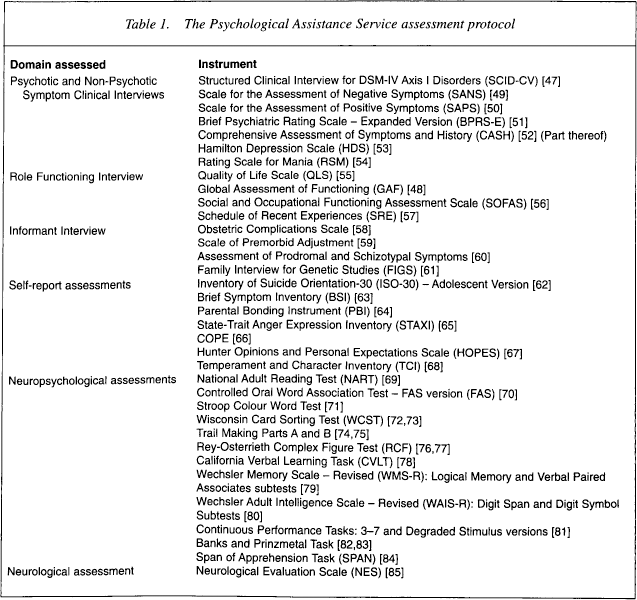
The three clinical interviews conducted with the patients are designed to systematically obtain detailed information about nonpsychotic, psychotic, attenuated psychotic and related symptoms, their onset, frequency, duration and relationship, if any, to substance abuse and level of functioning. The first two interviews are semistructured, based on existing research interviews and symptom rating scales, and enable quantification of the patient's symptomatology.
The informant interview is typically conducted with the patient's mother, although where this is not possible another relative is interviewed. This interview helps to gather information about possible neurodevelopmental risk factors; including obstetric complications, early childhood development and associated behavioural or social problems; and family psychiatric history, which enables the construction of a genogram. In addition, the informant interview serves to provide an alternate perspective on the patient's symptoms, which is particularly useful for young people who tend to under report symptoms.
The neurological examination systematically elicits and quantifies nonlocalising neurological signs. The neuropsychological test batteries are administered over two testing sessions, each of approximately 90 minutes' duration. Patients are assessed using measures covering a comprehensive range of cognitive functions, including premorbid intelligence, visual and verbal memory, attention and vigilance, and executive function.
Patients undergoing a full assessment at PAS also complete a variety of self-report instruments, covering such areas as suicide orientation, psychotic and nonpsychotic symptoms, parental bonding, anger expression, personality, coping and hopefulness.
Following completion of the full assessment all the findings are collated, presented and discussed by the PAS team at a ‘review’ meeting. At this meeting a consensus is reached as to which, if any, psychosis risk group the patient can be assigned or whether the patient meets criteria for a first psychotic episode, and what DSM-IV diagnosis is appropriate in either case. Patients who meet the criteria for one of the ‘at-risk’ groups or a first psychotic episode are offered treatment by PAS. Those who do not meet these criteria are referred to other mental health services for ongoing management. In either case the findings of the assessment are discussed with the patient and his/her family.
Audit of cases
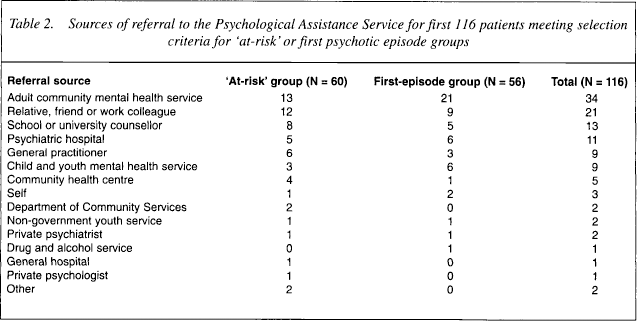
Table 2 provides information on sources of referral for the first 116 patients who met the PAS selection criteria. Table 2 shows that referrals come from diverse sources. The most frequent source is the adult community mental health service and the second most common source of referral comprises relatives, friends or work colleagues. General practitioners refer fewer patients than expected in spite of the intensive education campaign directed at this source.
Sources of referral to the Psychological Assistance Service for first 116 patients meeting selection criteria for ‘at-risk’ or first psychotic episode groups
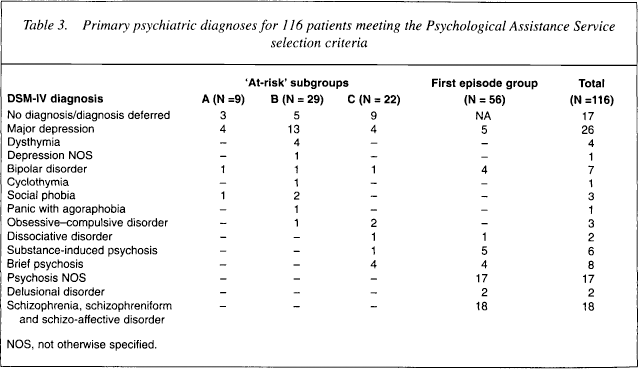
The primary diagnoses reached for 116 patients, comprising the three ‘at-risk’ subgroups and ‘first episode’ patients, following full PAS assessment are provided in Table 3. Overall, 60 young people were found to be ‘at-risk’ of psychosis using the PACE criteria; that is, they met criteria for membership of risk groups A, B and C as defined previously. There were 56 patients referred with first-episode psychosis. Note that 31 of the patients (26.7%) received a diagnosis of depressive disorder, usually major depression. Among the first-episode patients, approximately half (26/56) had nonaffective, nonschizophrenic psychoses (e.g. brief psychosis, substance-induced psychosis, psychosis not otherwise specified), while nine patients had a psychotic affective disorder, either unipolar or bipolar. At the assessment stage it is unclear whether these individuals will go on to develop an affective or schizophrenic psychosis, or whether they will recover with no further episodes.
Primary psychiatric diagnoses for 116 patients meeting the Psychological Assistance Service selection criteria
Demographic and clinical characteristics of the ‘at-risk’ and first-episode groups are shown in Table 4. There were no gender differences between the two groups and minor differences in age. The groups differed in the expected direction in terms of reality distortion symptoms, but there were no differences in disorganisation symptoms between the two groups, possibly due to the low sensitivity of the instruments in detecting mild degrees of thought disorder. Total negative symptom scores were greater in the first-episode patients but the only Scale for the Assessment of Negative Symptoms (SANS) subscale score differences were found for anhedonia/asociality. The first-episode group also had higher schizotypal symptom scores than the ‘at-risk’ patients.
Demographic and clinical characteristics of 116 Psychological Assistance Service patients
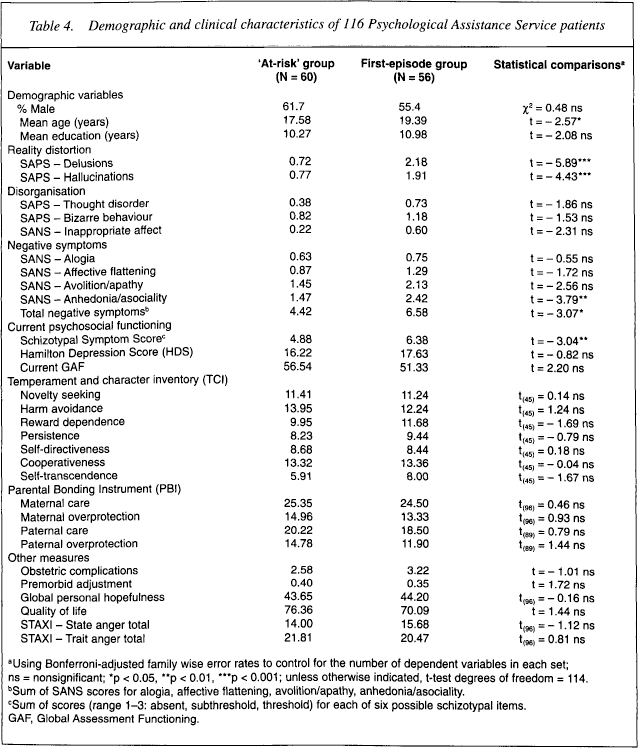
Using Bonferroni-adjusted family wise error rates to control for the number of dependent variables in each set; ns = nonsignificant;
p < 0.05
p < 0.01
p < 0.001; unless otherwise indicated, t-test degrees of freedom = 114.
Sum of SANS scores for alogia, affective flattening, avolition/apathy, anhedonia/asociality.
Sum of scores (range 1–3: absent, subthreshold, threshold) for each of six possible schizotypal items.
GAF, Global Assessment Functioning.
The Hamilton Depression Rating Scale score was quite high for the sample as a whole, which is consistent with the prevalence of depressive disorders in the groups and the ubiquity of depressive phenomena in clinical samples. The groups did not differ in their current GAF scores. There was also no evidence of differences between the ‘at-risk’ and first-episode groups with respect to temperament, parental bonding, hopefulness and quality of life. Likewise, levels of obstetric complications and premorbid adjustment were similar.
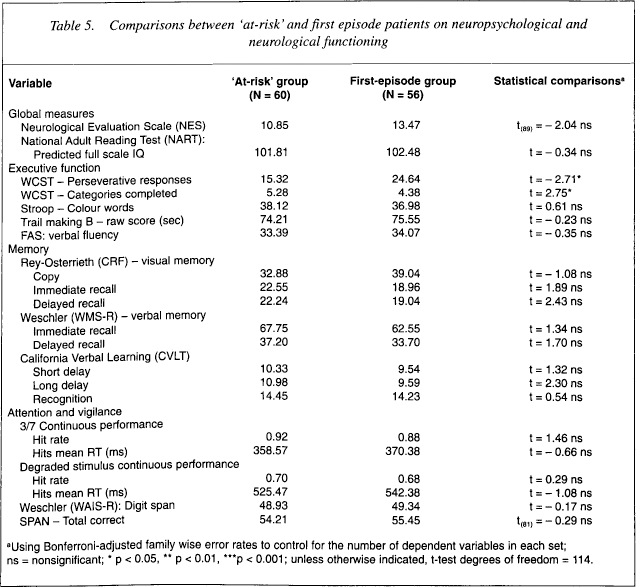
The ‘at-risk’ and first-episode groups were compared on the neuropsychological test battery and the neurological assessment as shown in Table 5. Although several of the scores fall within the impaired range there were no group differences on any neuropsychological measure except for the Wisconsin Card Sort Test in which the first-episode group showed more perseverative errors and fewer categories completed than the ‘at-risk’ group. The groups did not differ on the Neurological Evaluation Scale.
Comparisons between ‘at-risk’ and first episode patients on neuropsychological and neurological functioning
Using Bonferroni-adjusted family wise error rates to control for the number of dependent variables in each set; ns = nonsignificant;
p < 0.05, ∗∗ p < 0.01, ∗∗∗ p < 0.001; unless otherwise indicated, t-test degrees of freedom = 114.
Discussion
In summary, there were some significant differences between the ‘at-risk’ and first psychotic episode groups in terms of symptomatology. These differences were in the severity of psychotic symptoms, namely delusions and hallucinations, but not disorganisation symptoms. Negative symptoms and schizotypal symptoms also distinguished the two groups, being higher in the first-episode patients. No differences were found in premorbid adjustment, dispositional characteristics or quality of life. Somewhat unexpectedly there were no significant group differences on the neuropsychological measures, except for the Wisconsin Card Sort Test, although neuropsychological test scores obtained were often in the impaired range. At one level, these findings indicate that the ‘at-risk’ group is about as impaired as the first-episode group psychosocially and neuropsychologically, suggesting that the former, as defined by the criteria of Yung et al. [46], may indeed be vulnerable to psychosis, if not to other forms of psychopathology. Ultimately, the utility of the screening protocol can only be adequately tested when there have been sufficient numbers of patients assessed and followed over a sufficient time for definitive diagnoses in all cases to be established.
So far we have conducted follow-up evaluations on 50 patients (23 ‘at-risk’ and 27 first-episode) in the aforementioned sample, at an average of 14.6 months (range: 4–34) after the initial assessments. Of the ‘at-risk’ group, only 2 of 23 (9%) developed a psychotic episode (one psychosis not otherwise specified from group B, one schizophreniform disorder from group C). In the first-episode group, all patients with a diagnosis of schizophrenia or affective psychosis (N = 7) had their diagnoses unchanged at follow-up, and all patients with schizophreniform disorder (N = 3) went on to meet criteria for schizophrenia. Of the remaining 17 first-episode patients (brief psychosis, substance-induced psychosis, delusional disorder, psychosis not otherwise specified), eight met diagnostic criteria for schizophrenia or schizo-affective disorder at follow-up, a 47% rate of conversion to established psychosis.
The rate of conversion from ‘at-risk’ status to psychosis is disappointingly low compared to the rate reported by the Melbourne group [86]. The much higher rate of conversion we obtained for nonschizophrenic, nonaffective first-episode psychoses to established schizophrenia or schizo-affective disorder is hardly surprising given that the presence of psychotic symptoms for longer than a week is a strong indicator that a persistent psychotic illness is evolving. Given that we are using virtually the same criteria for defining ‘at-risk’ patients as PACE, what could be the reason for the different rates of conversion to psychosis among the ‘at-risk’ patients?
One possibility is that we have not followed this group for a sufficient time through the period of high risk of onset of psychosis. Our sample was certainly young and could be considered at the beginning of the age of highest risk. A second possibility is that the treatment provided by PAS is especially effective in preventing or forestalling the onset of psychosis. This would indeed be pleasing, but there is no evidence that what PAS provides therapeutically is any better than the treatment given by PACE. A third explanation is that the criteria for defining risk status are insufficiently specific, and the conversion rate obtained by PACE is due to chance. This alternative can only be tested by acquiring larger samples of ‘at-risk’ patients with adequate follow-up at both centres and comparing the data obtained. Related to this is a fourth possibility which is that the referral networks feeding into each centre at Melbourne and Newcastle differ in their ability to detect patients who are truly at risk of psychosis, yielding a higher base rate of ‘true positives’ among the Melbourne referrals compared to those at Newcastle. This alternative explanation would be impossible to test in the absence of a reliable and valid method for large-scale population screening for psychosis.
In the meantime, specialised centres like PAS and PACE must continue to apply comparable standardised assessment protocols, and conduct systematic follow-up evaluations so that large databases can accumulate and be pooled across centres. Only in this way can the effectiveness of such early intervention services be determined and screening protocols refined to achieve the desired validity.