
Abstract
Background:
The Accredited Persons Programme was introduced in 2003. The relevant Mental Health Acts (NSW) authorised reviews by appropriately credentialed non-medical health professionals as part of the process of detaining and treating a person without consent: an authority previously held by medical officers. Evaluations of the Programme are needed.
Objective:
To compare discharge decisions for hospital-treated deliberate self-poisoning patients made by an Accredited Person and Medical Officers.
Methods:
For a 10-year cohort (2003–2012) of index hospital-treated deliberate self-poisoning admissions at the Calvary Mater Newcastle, we compared Accredited Person and Medical Officer discharge decisions from the general hospital. We specifically examined discharges to the psychiatric hospital under a Mental Health Act certificate (used as an index of the Accredited Person’s use of the authority under the Accredited Persons Programme) compared to any other discharge destination. Unadjusted and adjusted logistic regression models and a propensity score analysis were used to explore the relationship between clinician type and discharge destination.
Results:
There were 2237 index assessments (Accredited Person = 884; Medical Officer = 1443). One-quarter (27%) were referred for assessment under the Act at the psychiatric hospital, with the Accredited Person significantly more likely (32%) to require this compared to the Medical Officers (24%); Risk Difference: 8.3% (4.5 to 12.1). However, after adjusting for patient characteristics; Risk Difference: −3.0% (−5.9 to −0.1) and for propensity score, Risk Difference: −3.3% (−6.7 to 0.1), the Accredited Person and Medical Officer likelihood of discharging for an assessment under the Act was similar.
Conclusions:
The Accredited Person assessed more clinically complex patients than the Medical Officers. After adjusting for clinical complexity and propensity score, the likelihood of referral for involuntary psychiatric hospital care was similar for Accredited Person and Medical Officers. Our evaluation of the Accredited Person programme in the general hospital was favourable, and wider implementation and evaluation is warranted.
Keywords
Background
In New South Wales (NSW) Australia, the Mental Health Act 2007 (NSW; MHA; NSW Government, 2007) is the legislation that currently covers the care and treatment of people with mental illness. The ‘Objects’ of the Act are to ‘provide for the care, treatment and control of persons who are mentally ill or mentally disordered’, usually in the community or in hospital on a voluntary basis, ‘and, in a limited number of situations, on an involuntary basis’, ‘while protecting the civil rights of those persons’ (NSW Government, 2007); in effect to ensure that people receive mental health assessment and appropriate care. This care can be provided on an involuntary basis, when ‘there are reasonable grounds for believing that care, treatment or control of the person is necessary for the person’s own protection from serious harm, or for the protection of others from serious harm’ under Section 14, in the context of narrowly defined symptoms indicating they are ‘mentally ill’; if the person’s behaviour for the time being is so irrational as to justify a conclusion on reasonable grounds that temporary care, treatment or control of the person is necessary for the person’s own protection from serious physical harm, or for the protection of others from serious physical harm
or under Section 15 for a less specific and broader range of behaviours indicating ‘mental disorder’ (NSW Government, 2007).
The two Acts of relevance (Mental Health Act 1990; NSW and Mental Health Act 2007 (NSW); NSW Government, 1990, 2007) during the period of this study included provisions to allow a person to be required to present for the purposes of further psychiatric assessment or ‘medical examination’ at a ‘mental health facility’ in the Mental Health Act 2007 (NSW; NSW Government, 2007). Specifically using the Mental Health Act 2007 (NSW) as an illustrative example, ‘Section 19: Detention on certificate of medical practitioner or accredited person (cf 1990 Act, s 21)’.
(1) A person may be taken to and detained in a declared mental health facility on the basis of a certificate about the person’s condition issued by a medical practitioner or accredited person. The certificate is to be in the form set out in Part 1 of Schedule 1 (NSW Government, 2007). This detention of a patient with associated transfer to a mental health facility can currently occur after initial assessment and completion of the relevant certificate by a select group of professionals (e.g. registered medical practitioners, ambulance and police officers), including an ‘accredited person’ (Mental Health Act, 1990; No9, section 287A) (NSW Government, 1990) with ‘the primary role of an accredited person [being] to make an initial decision about a person’s need for involuntary admission under the NSW Mental Health Act 2007’, including the authority to complete the appropriate Mental health Act certificate (Health Education and Training Institute, 2019; New South Wales Institute of Psychiatry, 2009).
The Accredited Persons Programme was introduced in NSW in 2003 to train and authorise the appointment of Accredited Persons. The programme approved experienced mental health clinicians (non-medical practitioners) who had completed an accreditation training programme the capacity to issue Mental Health Certificates under the MHA (‘MHA certificates’). The objective of introducing the Accredited Persons Programme was to increase capacity and efficiency of responses to people requiring mental health assessments and access to care under the MHA and it was anticipated that the programme would particularly benefit areas where medical practitioners were scarce or difficult to access (e.g. rural and remote regions; New South Wales Institute of Psychiatry, 2009).
Four studies have investigated the use of MHA certificates requiring presentation for mental health assessment at a psychiatric facility within NSW. A review of all MHA certificate presentations to a Sydney Emergency Department (ED) over 3 months found 27% of certificate-mandated presentations by ambulance officers resulted in an admission to a psychiatric hospital, compared to 60% of those issued by medical practitioners or accredited persons (Cutler et al., 2013). A separate study found that MHA certificates completed by generalist medical officers were much less likely to have adequate or accurate information compared to those by psychiatric registrars (Lamont et al., 2016). A study of all (n = 172) MHA certificate presentations to a Sydney ED over 3 months found 70% of police and 60% of ambulance MHA certificates did not result in admission, while only 3 were completed by an AP, so no conclusions could be drawn about AP-associated outcomes (Derrick et al., 2015). Finally, a 12-month study from a Sydney tertiary hospital ED co-located with a psychiatric emergency care centre (n = 258) found significantly fewer patients presenting on police-MHA certificates (38%) resulted in involuntary psychiatric admissions than those on medical (including nurse) MHA certificates (79%; Llewellin et al., 2011). While there is limited evidence about the proportion of certificate-mandated assessments that result in admission to the psychiatric hospital, we know of no studies comparing the utility of MHA certificates issued by an AP compared to MOs. The studies noted above have been limited by relatively short time-frames, small sample sizes and broad patient inclusion criteria.
Hospital-treated deliberate self-poisoning is common and costly and this clinical population is the highest risk population for subsequent suicide (Carter et al., 2016). No studies have specifically investigated whether the use of MHA certificates by APs is similar or different to MOs, the group who have traditionally managed these discharge decisions. We anticipate that there will be independent patient characteristics and service characteristics that will predict discharge to a psychiatric hospital (Carter et al., 2006) and that patient allocation may vary by clinician group resulting in a selection bias.
Aims
Thus, the aims of this study were for a cohort of hospital-treated deliberate self-poisoning admissions assessed during business hours to:
Describe the clinical characteristics of the patient cohort by type of assessing clinician (MO vs AP).
Compare unadjusted discharge decisions (specifically referral for an involuntary mental health assessment under an MHA certificate) by type of assessing clinician.
Compare discharge decisions (specifically referral for an involuntary mental health assessment under an MHA certificate) by type of assessing clinician; after adjustment for patient and service characteristics.
Method
Design
This study used a prospective longitudinal cohort design for a 10-year period (1 July 2003–30 June 2013) of index admissions to the Calvary Mater Newcastle hospital for deliberate self-poisoning. The first episode for each person for the study period was used as the index admission. This study period corresponds to the first 10 years of the AP appointment to this clinical service and the first 10 years of the state-wide implementation of the initiative.
Setting, participants and data recording
Newcastle, 160 km north of Sydney on the east coast of NSW, is the seventh largest city in Australia and the second most populated area in the State. The surrounding Hunter region also includes the local government areas of Lake Macquarie, Cessnock, Maitland, Port Stephens, Muswellbrook, Dungog, Singleton and Upper Hunter.
The Hunter Area Toxicology Service (HATS) is a regional toxicology service situated at the Calvary Mater Newcastle hospital. It serves a primary referral urban population of over 410,000 (Newcastle, Lake Macquarie and Port Stephens) and is a tertiary referral centre for a further rural population of over 243,000 (Lower and Upper Hunter Valley). Almost all poisoning presentations in the primary referral area are directed to the Calvary Mater Newcastle ED and admitted to the clinical toxicology unit under the care of the attending clinical toxicologist. A minority of cases, usually requiring Intensive Care Unit treatment, are admitted to another hospital with consultation by the Calvary Mater Newcastle clinical toxicologist. A mental health assessment is conducted for all HATS patients admitted for deliberate self-poisoning (Whyte et al., 1997). The mental health assessments are undertaken by three groups of people. During business hours (8:30 a.m.–5 p.m., Monday to Friday), assessments are conducted by trainee psychiatrists on clinical rotation to the service, the attending psychiatrist or the clinical nurse consultant who was registered as an AP in 2003. Recreational (including chronic misuse), iatrogenic and accidental self-poisoning are also admitted by HATS, but were excluded from the analyses for this study. After-hours assessments, which are only done by MOs, were excluded. Admissions that were assessed in business hours, either by MO or the AP, were included in this study.
Standardised pre-formatted data collection sheets were used by clinicians to record information about participant demographic and clinical variables (Buckley et al., 1999), based on reporting from the patient, family, ambulance, pharmacist and treating doctors, while discharge disposition was recorded in the clinical record data system. All psychiatric diagnoses were made according to the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition; DSM-IV) following clinical assessment and based on patient interview, collateral informant history and case record review. All mental health diagnoses were reviewed at a weekly clinical meeting. All toxicological and psychiatric information were entered into a relational database by trained personnel blind to study aims. Discharge destination was determined by the clinician who conducted the mental health assessment.
Variable definitions
Data were extracted for all index deliberate self-poisoning presentations. This included demographic characteristics (gender, age group, Indigenous identity, marital status, highest level of education, housing, employment), clinical characteristics (ingestions by major drug groups, DSM-IV major categories, level of suicidality at the time of psychiatric assessment, recency and type of psychiatric contact in the past year), assessing clinician (MO vs AP) and discharge destination (involuntary referral to psychiatric hospital vs other).
For analysis, individual mental health diagnoses and conditions included in ‘additional codes’ were mapped to major DSM-IV diagnostic categories for (any anxiety, mood, psychotic, substance use, personality, all other disorders and V-code relational problems). Suicidality was recorded using a three-level clinician-rated variable reflecting the patient’s responses at the time of psychiatric assessment: no suicidal plan or ideation, low or moderate suicidal ideation and no plan or high or intense suicidal ideation and/or a suicide plan. For the primary outcome, discharge destination was dichotomised into involuntary discharge to psychiatric hospital (discharge under an MHA certificate for transfer to the psychiatric hospital for an involuntary mental health assessment) and other destinations (including voluntary discharge to psychiatric hospital, discharge home, to the general hospital, gaol and other).
Descriptive analyses were conducted for participant characteristics, with chi-square tests to examine the magnitude of the association of categorical demographic or clinical variables, and assessment clinician. Analysis then focused on the relationship between type of assessing clinician and the outcome of discharge to the psychiatric hospital for an involuntary mental health assessment (under an MHA certificate).
We calculated the unadjusted proportion of patients who were referred for an involuntary mental health assessment at the psychiatric hospital by clinician (MO vs AP). Using these values, we calculated the difference in proportions between the two clinician groups (and the 95% confidence interval). We then fit a multivariate logistic regression model where the key predictor was clinician type and the covariates included patient demographic and clinical characteristics. So that the results were comparable with the unadjusted analysis and the propensity score analysis (see in the following), and we used the model coefficients to estimate the adjusted proportion of patients who were discharged to the psychiatric hospital for an involuntary mental health assessment by clinician type, and using this we calculated the adjusted difference between these two proportions. We reported these results using marginal effects. We then used a propensity score analysis to estimate the outcomes of patients that were as similar as possible, with the only difference being whether they were assessed by a medical officer or an accredited person.
The propensity score analysis was undertaken in several stages. In the first stage, we identified a set of demographic, clinical and admission characteristics that predicted whether a given patient was assessed by a medical officer or the accredited person. We did this using stepwise regression that fit a series of multivariate logistic regressions to the data until a final model was identified that contained only those variables that had a significant association with clinician type. In the second stage, we entered these significant variables into a propensity score analysis. Propensity score analysis seeks to match patients in the ‘treatment group’ (assessed by AP) to one or more similar patients in the alternative group (assessed by MO). The variables from the first step were used to calculate a measure of similarity between patients in each group (based on the probability that any given patient was treated by an AP). Once this matching was done, we estimated the average treatment effect, which was the difference in proportions of the outcome between the two groups. This analysis was repeated in a sensitivity analysis, where we redefined the outcome variable by excluding all voluntary discharges to the psychiatric hospital from the ‘other’ category. All descriptive analyses were undertaken in SPSS. All multivariate analyses were undertaken in Stata 16.1.
Ethical approval
Ethical approval for this study was obtained from the Hunter New England Human Research Ethics Committee (HNEHREC Reference No: 14/02/19/5.01).
Results
Participant characteristics
A total of 2327 admissions were included. Demographic characteristics are provided in Table 1. Clinical characteristics are provided in Table 2. Females, those under 40 years of age and those with a high school education, comprised the majority of the sample. Psychiatric medications were the most commonly ingested medication group. Co-ingestion of drugs from two or more medication groups and co-ingestion with alcohol were also common. The most common types of diagnoses were Mood Disorders, Substance Use Disorders and Relational Problems, with frequent co-morbidity across diagnostic groups. The majority of the sample reported no thoughts of suicide or suicidal plans at the time of assessment. Approximately one-third had no contact with any service for mental health issues in the year before admission.
Demographic characteristics.
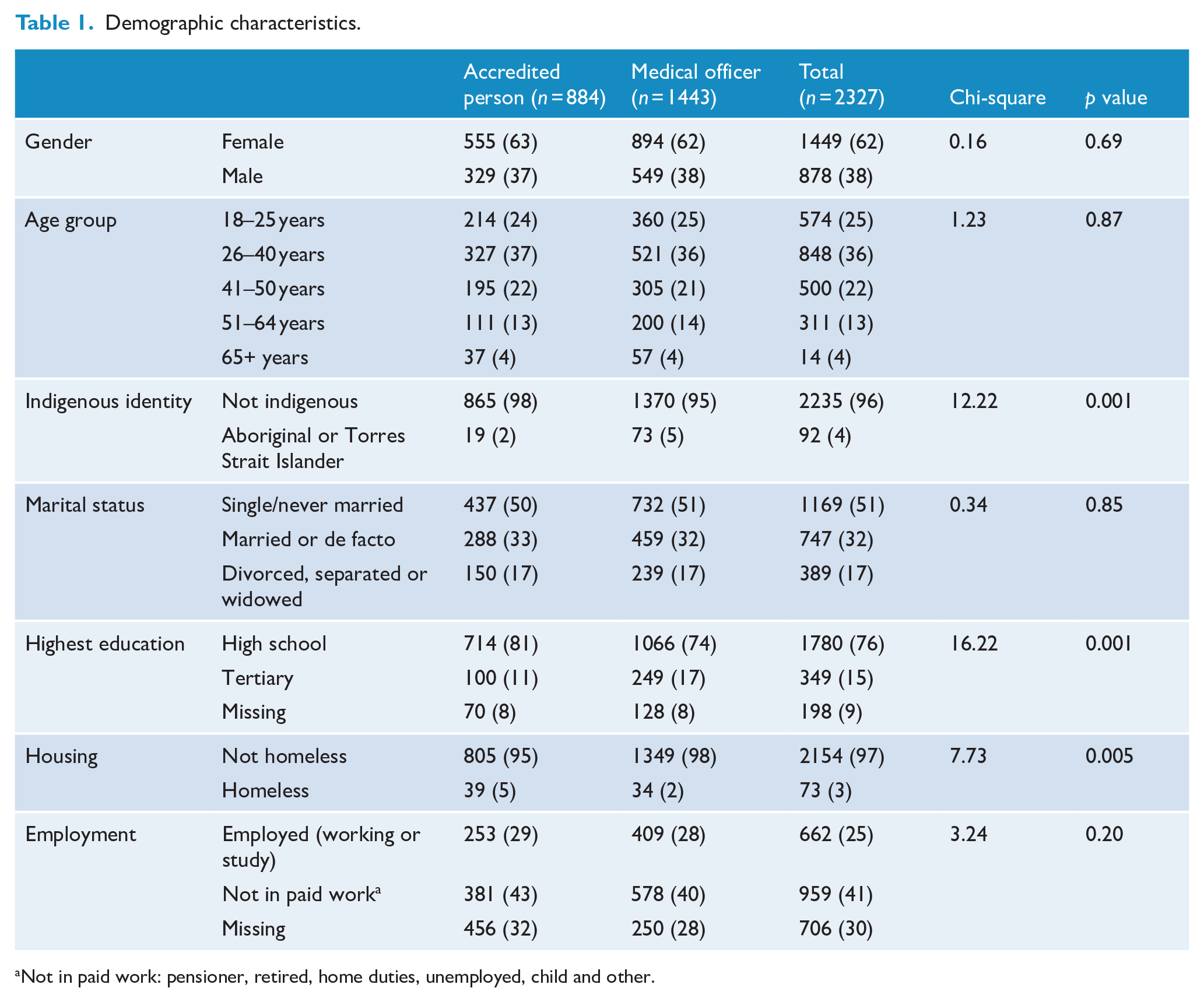
Not in paid work: pensioner, retired, home duties, unemployed, child and other.
Clinical characteristics.
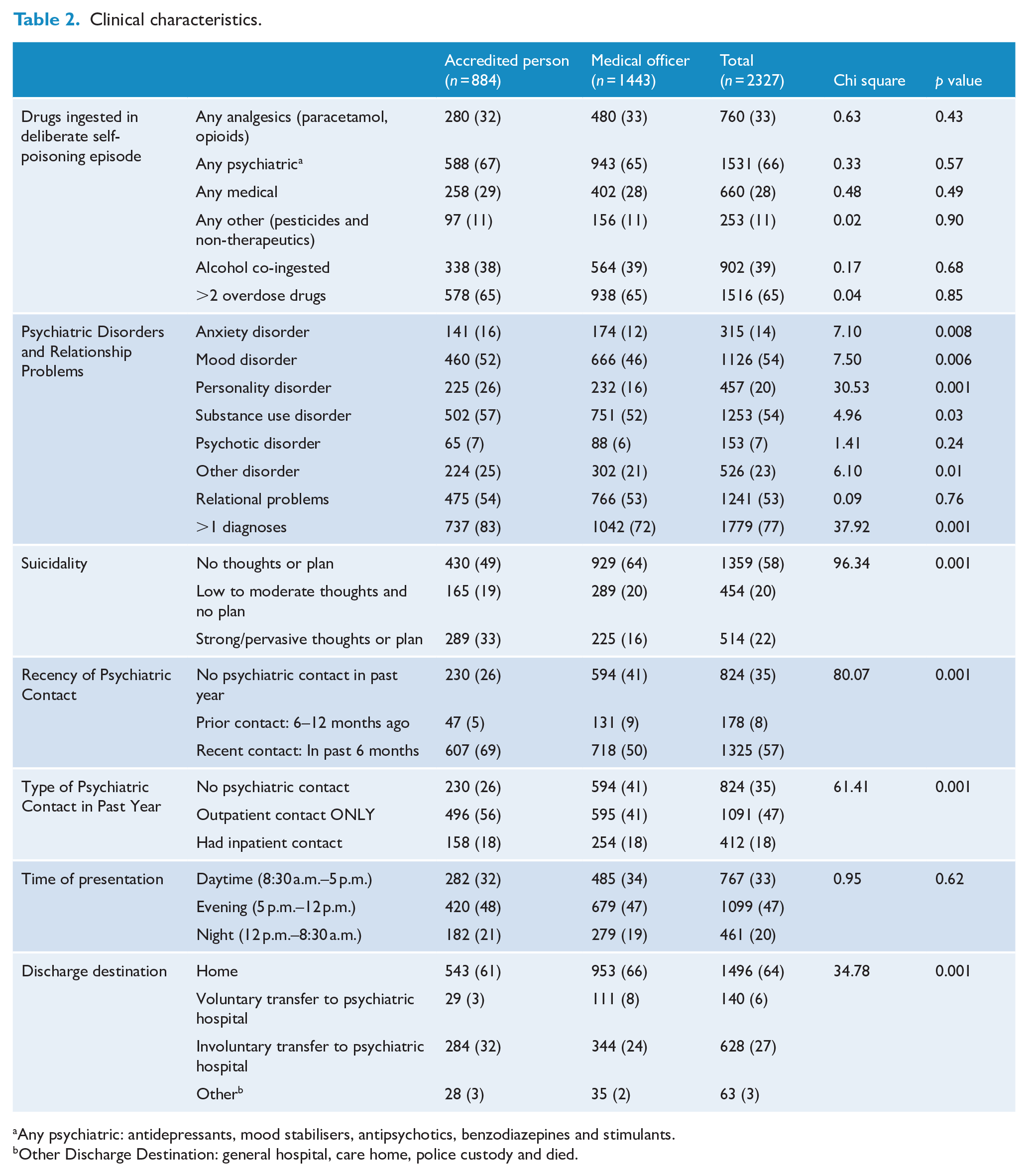
Any psychiatric: antidepressants, mood stabilisers, antipsychotics, benzodiazepines and stimulants.
Other Discharge Destination: general hospital, care home, police custody and died.
Participant characteristics by clinician group
There were no differences in patient characteristics by clinician group for gender, age group, marital status or employment. However, the AP saw more people with lower educational attainment, a greater proportion who identified as homeless, and the MOs saw a greater proportion of Indigenous patients. Patients assessed by the AP were also more likely to have a diagnosis of anxiety disorder, mood disorder, personality disorder, substance use disorder, other disorder, as well as co-morbidity of more than one psychiatric disorder. The AP had a greater proportion with higher suicidality ratings at the time of assessment, more people reporting recent mental health service use and more people reporting previous outpatient mental health care (by service type).
Involuntary discharge to psychiatric hospital by clinician group
Overall, two-thirds (64%) of the cohort were discharged home after the general hospital admission. One-third (33%) were discharged to the psychiatric hospital, with the vast majority of this group (82% of those discharged to the psychiatric hospital; 27% of the whole cohort) discharged to the psychiatric hospital for an involuntary mental health assessment under an MHA certificate. In unadjusted analyses, a greater proportion of people assessed by the AP (32.1%) were discharged for an involuntary mental health assessment compared to those assessed by the MOs (23.8%), representing a Risk Difference of 8.3% (95% confidence interval [CI]: 4.5, 12.1), p < .001. Once differences in patient characteristics were adjusted for by including demographic, clinical and admission characteristics in a multivariate model, the direction of this relationship reversed such that those assessed by the AP were less likely to be discharged under an MHA certificate compared to those assessed by the MO, Risk Difference = −3.0% (−5.9, −0.1). In the analysis using the propensity score, there was a non-significant difference between AP and MO for discharge under an MHA certificate, Risk Difference = −3.3% (−6.7, 0.1). For the unadjusted sensitivity analyses (voluntary referral to the psychiatric hospital removed from the discharge destination variable), the AP was more likely to discharge to the psychiatric hospital than the MO. However, after adjustment in the multivariate model and in the propensity score analysis, the AP was significantly less likely to refer to the psychiatric hospital than the MO. Details of these analyses are shown in Table 3.
Discharge to psychiatric hospital for involuntary mental health assessment by accredited persons and medical officers.
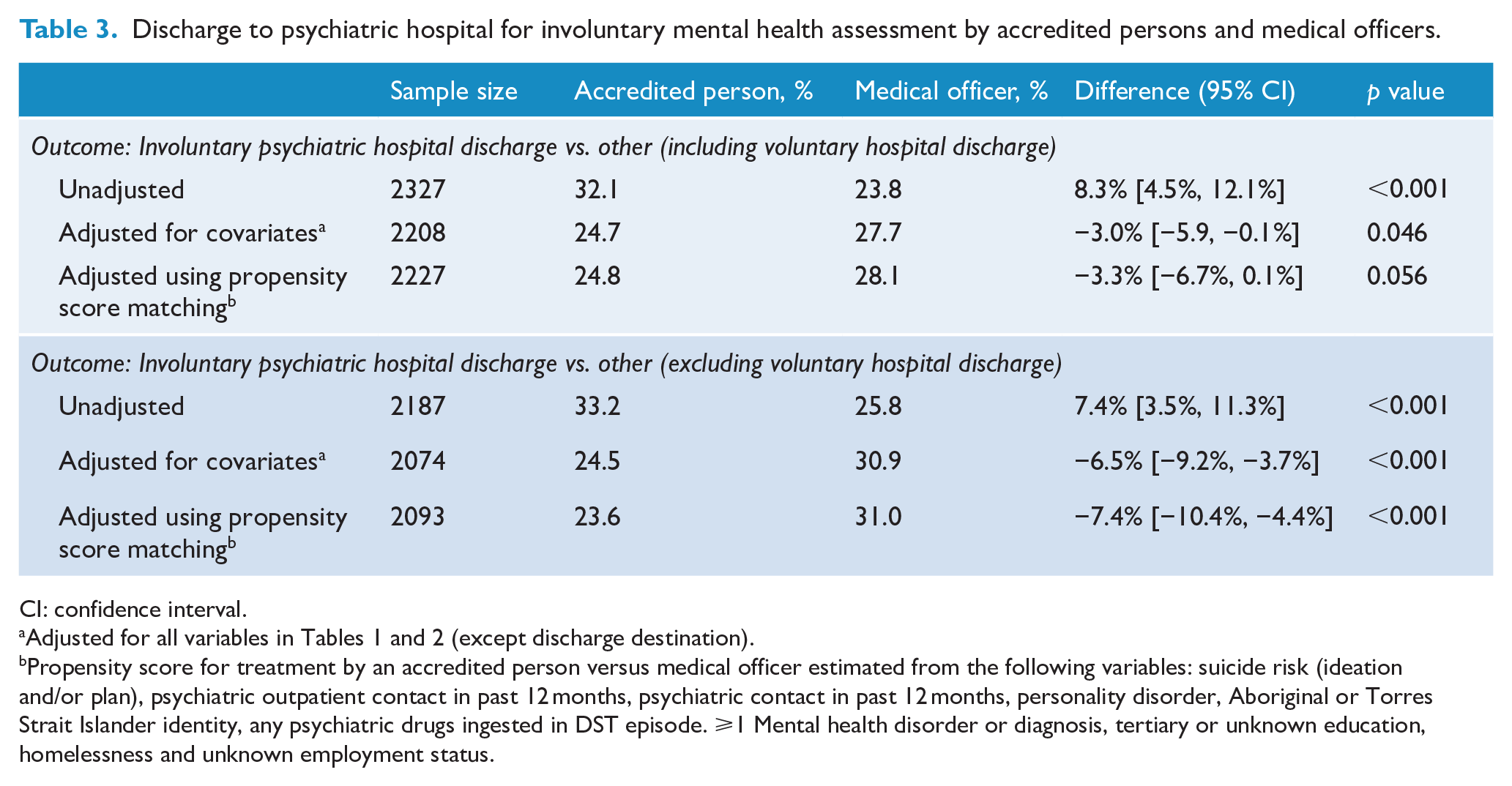
CI: confidence interval.
Propensity score for treatment by an accredited person versus medical officer estimated from the following variables: suicide risk (ideation and/or plan), psychiatric outpatient contact in past 12 months, psychiatric contact in past 12 months, personality disorder, Aboriginal or Torres Strait Islander identity, any psychiatric drugs ingested in DST episode. ⩾1 Mental health disorder or diagnosis, tertiary or unknown education, homelessness and unknown employment status.
Discussion
This study has investigated the clinical characteristics of a 10-year cohort of patients who presented to hospital after self-poisoning and the disposition arrangements associated with the type of clinician who conducted the mental health assessment (MO or AP) in the general hospital. In summary, differences in both patient characteristics and discharge decisions were found to vary by the type of assessing clinician, while adjustment for patient characteristics in the disposition arrangements changed the implications drawn from the initial univariate associations. The key findings are discussed.
First, we identified that in this hospital, there were differences in patient characteristics associated with the type of clinician who conducted the assessment. Specifically, there were indications that the AP (an experienced nurse appointed at the level of Clinical Nurse Consultant) was allocated more patients with greater clinical complexity, psychosocial vulnerability and disadvantage (e.g. homeless, lower educational achievement, more previous psychiatric service contact, greater psychiatric illness burden, higher ratings of suicidality at the time of assessment). While it is possible that these differences may reflect clinician differences in assessment approaches, conceptualisation and ratings of presenting issues, or greater capacity to elicit information relevant to these variables (e.g. the AP systematically engaging in more comprehensive assessments), we believe the differences in patient characteristics are, to a large extent, reflective of the outcome of service allocation processes. Differential allocation of patients occurs because of a perceived need for expertise beyond that which might be expected of a relatively junior MO (psychiatric registrar) on rotation to a Consultation-Liaison service, especially during the initial weeks on the service. In short, clinician allocation was unlikely to be random and these analyses highlight the importance of accounting for case-mix when seeking to compare disposition decisions by different clinician groups.
Overall, we identified that over one-quarter (27%) of all people who were admitted to the general hospital after deliberate self-poisoning were discharged to the psychiatric hospital, with the vast majority of those (82% of those discharged to the psychiatric hospital) transferred involuntarily under an MHA certificate. This is a relatively high proportion and emphasises the degree to which serious acuity and complexity is associated with hospital presentation for deliberate self-poisoning, at least for a substantial minority of people.
Furthermore, in the unadjusted analysis, it was clear that the AP was more likely to require a person to have an involuntary mental health assessment at the psychiatric hospital than the comparator group of MOs. On the surface, this could be taken to indicate that the Accredited Persons programme was not being used in an equivalent manner compared to Medical Officers, who have traditionally managed these decisions and specifically that the AP was more likely to use more restrictive treatment settings when this was available to them.
However, once patient characteristics were taken into account, the AP was either less likely to discharge people on an involuntary basis to the psychiatric hospital than the MOs or did so at the same rate as MOs, with the absolute differences being very small after adjustment for clinical complexity. This pattern was confirmed once the potential for non-random allocation of patients to the different clinician groups were taken into account (through the propensity score analysis). This suggests that the clinical complexity of patients’ presenting needs were the key factor in the decision to require a person to have an involuntary mental health assessment at the psychiatric hospital, not whether the assessment was conducted by an AP or MO.
Finally, the fundamental implication from this study is that the local AP has been using the MHA certificate powers in a similar way to MOs. This suggests that an expansion of this programme could provide general hospitals with a multi-disciplinary, less costly and comparable means of providing acute mental health care to an important clinical population, although it will be important to investigate the longer term outcomes (e.g. deliberate self-poisoning re-presentation rate and psychiatric hospitalisation rates) to fully understand the effectiveness and impact of the implementation of the Accredited Persons programme. Although this study reports on the performance of the first 10 years of the Accredited Person Programme, this clinical service has been maintained at the Calvary Mater Newcastle hospital to the present time.
Study limitations
While we have been able to access a sizable patient cohort covering the first 10 years of the Accredited Persons Programme, the AP was a single, highly trained and very experienced Clinical Nurse Consultant staff member, whereas the MOs are usually psychiatric registrars of various experience levels on a 6-month rotation to the service. The performance of a single Accredited Person may be representative of the individual rather than of Accredited Persons more generally. Caution should be used when generalising these findings to other staff classifications, service models and clinical populations. Furthermore, this evaluation of the use of the MHA certificate powers is within the context of standardised hospital admission and assessment processes for people presenting to hospital with deliberate self-poisoning, reflecting a best practice environment.
Conclusion
In summary, the findings from this study suggest that mental health nurses with appropriate experience and training make disposition arrangements requiring similar or possibly less restrictive care than MOs for this important clinical population. While there is a need to investigate the functioning of the programme and the use of the AP powers among a larger group of clinicians and with a broader range of presentations, the findings from this study (which captures functioning of the programme over a long period of time) are promising. If patient outcomes are shown to be equivalent, it suggests that the NSW Accredited Persons programme can provide hospitals (and other settings) a lower cost and equally efficient means of extending the capacity of health services to be able to respond to acute mental health presentations and can provide reassurance to the health service about the effectiveness and appropriateness of the clinical care delivered within the parameters of this policy initiative.
Footnotes
Acknowledgements
The HATS database and included Psychiatric case register has had contributions over many years from many people including past registrars, advanced trainees, fellows, nursing staff, research assistants and computer programmers. We gratefully acknowledge their contribution to this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: K. McGill’s position was funded by the Burdekin Suicide Prevention Programme and administered by Hunter New England Mental Health Services. Katie is the recipient of a PhD scholarship from the Suicide Prevention Research Fund, made possible through a partnership between Suicide Prevention Australia and the Regional Australia Bank. Matthew Spittal is a recipient of an Australian Research Council Future Fellowship (project number FT180100075) funded by the Australian Government.