
Abstract
Background:
Hospital-treated deliberate self-poisoning is common, with a median patient age of around 33 years. Clinicians are less familiar with assessing older adults with self-poisoning and little is known about their specific clinical requirements.
Objective:
To identify clinically important factors in the older-age population by comparing older adults (65+ years) with middle-aged adults (45–64 years) during an index episode of hospital-treated deliberate self-poisoning.
Methods:
A prospective, longitudinal, cohort study of people presenting to a regional referral centre for deliberate self-poisoning (Calvary Mater Newcastle, Australia) over a 10-year period (2003–2013). We compared older-aged adults with middle-aged adults on demographic, toxicological and psychiatric variables and modelled independent predictors of referral for psychiatric hospitalisation on discharge with logistic regression.
Results:
There were (n = 157) older-aged and (n = 925) middle-aged adults. The older-aged group was similar to the middle-aged group in several ways: proportion living alone, reporting suicidal ideation/planning, prescribed antidepressant and antipsychotic drugs, and with a psychiatric diagnosis. However, the older-aged group were also different in several ways: greater proportion with cognitive impairment, higher medical morbidity, longer length of stay, and greater prescription and ingestion of benzodiazepines in the deliberate self-poisoning event. Older age was not a predictor of referral for psychiatric hospitalisation in the multivariate model.
Conclusion:
Older-aged patients treated for deliberate self-poisoning have a range of clinical needs including ones that are both similar to and different from middle-aged patients. Individual clinical assessment to identify these needs should be followed by targeted interventions, including reduced exposure to benzodiazepines.
Introduction
Hospital-treated deliberate self-harm (DSH) is common and costly, and deliberate self-poisoning (DSP) is the predominant variant: 90% for all ages (Carroll et al., 2014) and 86% for older adults (Troya et al., 2019). The official rates of hospital-treated DSH in Australia are known to be underestimates, usually reporting on admitted patients only and reliant on accurate coding (Carter et al., 2016). Nevertheless, DSH is estimated at about 30,000 hospital admissions each year (Australian Institute of Health and Welfare [AIHW] and Flinders University, 2018), while DSP might account for 5% of all hospital admissions (McGrath, 1989) in Australia. Older-aged patients account for 4–15% of all DSH admissions internationally (AIHW and Flinders University, 2018; Nieto et al., 1992); for annual DSH rates of 19–65 per 100,000 population (Troya et al., 2019).
Systematic reviews of original studies using a variety of study designs have concluded that older adult DSH is associated with different characteristics and risk profile than younger adults (Chan et al., 2007; Troya et al., 2019). One limitation in many cohort studies is the comparison of the older-age patients with all other DSH patients, which is potentially misleading because of the very young median age (approximately 29–34 years) of the hospital-treated DSH population and hence very different patterns of poisoning agents and social and physical factors. When compared to all other age groups, older-adult DSH populations have been reported to have, for example, higher level of suicidal or lethal intent (Miret et al., 2010); more frequent diagnosis of major depression (Ticehurst et al., 2002); and different ingestion patterns, longer length of stay and greater mortality during admission (Doak et al., 2009).
The UK NICE guideline (National Institute of Health Care & Excellence, 2016) and the Royal Australian and New Zealand College of Psychiatrists (RANZCP) Clinical Practice Guideline for the management of DSH (Carter et al., 2016) recommend an assessment based on clinical and social needs rather than risk stratification (Carter and Spittal, 2018). This needs assessment encompasses a comprehensive evaluation of the patient’s situation and treatment needs, including modifiable social, psychological and motivational factors linked with self-harm, repeated self-harm or suicide. Better elucidation of the specific clinical needs of the older-aged DSH patient would help to inform clinical assessment procedures.
One of the key short-term outcomes of an episode of hospital-treated DSH or DSP is the clinical decision to discharge to home or to the psychiatric hospital. Psychiatric hospitalisation may be used for the management of suicidal behaviours, treatment of psychiatric disorders, and/or resolution of interpersonal or social crisis. There is considerable variation in the reported rates of psychiatric inpatient treatment for older-aged patients after DSP; 36% in Australia (Ticehurst et al., 2002) and for DSH 11–19% in the United Kingdom (Doak et al., 2009). The characteristics of older adults referred for psychiatric hospitalisation are not known, and we do not know if older-aged adults are referred at different rates than younger adults. Psychiatric hospitalisation after an episode of DSP in Australia has been independently associated with age 25 or older, homelessness, unemployment, previous self-harm, psychiatric inpatient treatment within 12 months, earlier psychiatric inpatient treatment, suicidal ideation or plan, mood or psychotic disorders, and lower clinician experience (Carter et al., 2006). However, this model used hospital-treated DSP patients of all ages for analysis, and so the identification of predictors of psychiatric hospitalisation more relevant to older-aged DSP patient populations was not specifically examined. Identification of these patient characteristics might help to understand this important area of clinical decision-making undertaken by clinicians.
This study aims to understand some of the specific similarities and differences and hence clinical needs of older-aged DSP patients compared to middle-aged adult DSP patients, which we believe to be a more relevant comparator group. We have investigated some key clinical characteristics, known modifiable risk factors for suicidal behaviours, and discharge destination, which will help to inform the recommended clinical needs assessment of older-aged patients with hospital-treated DSP.
Aims
To compare older-aged to middle-aged, adult, hospital-treated DSP patients on demographic, toxicological and psychiatric variables including discharge destination.
To develop a multivariate explanatory model of discharge to the psychiatric hospital for the older and middle-aged, adult, hospital-treated DSP population.
To test any unadjusted effect for age and any interaction effects for age on the decision for discharge to the psychiatric hospital, for older versus middle-aged, adult, hospital-treated DSP patients.
Methods
Setting
Newcastle, 160 km north of Sydney on the East coast of New South Wales, is the seventh largest city in Australia and the second most populated area in the State. The surrounding Hunter region also includes the local government areas of Lake Macquarie, Cessnock, Maitland, Port Stephens, Muswellbrook, Dungog, Singleton and Upper Hunter.
The Hunter Area Toxicology Service (HATS) is a regional toxicology service situated at the Newcastle Calvary Mater that serves a primary referral urban population of over 410,000 (Newcastle, Lake Macquarie and Port Stephens) and is also a tertiary referral centre for a further rural population of over 243,000 (Lower and Upper Hunter Valley). All poisoning presentations in the primary referral area are directed to the Calvary Mater Newcastle Emergency Department and admitted to the clinical toxicology unit (or notified if admitted to another hospital) under the care of the attending clinical toxicologist (Buckley et al., 2015; Carter et al., 2006; Whyte et al., 1997). Recreational (including chronic misuse), iatrogenic and accidental self-poisoning are also admitted by HATS, but were excluded from the analyses for this study. Although there is no consistently accepted definition in the literature, DSP is commonly defined as ‘the intentional self-administration of more than the prescribed dose of any drug whether or not there was evidence that the act was intended to cause self-harm’ (Bancroft et al., 1975).
Hunter New England Local Health District provides acute and community-based public psychiatric care through the Mental Health Service. A 100-bed psychiatric hospital (co-located on-site with HATS since 2009), which includes a specialist mental health service for older people (65+ years) and a 24-bed general adult unit at Maitland Hospital services the Hunter area population. There are also three private hospitals with psychiatric wards and a range of private mental health community-based providers in the local area.
Study design
The design was a prospective, longitudinal, cohort study of a 10-year period (1 July 2003 to 30 June 2013) of hospital-treated DSP at HATS (age 45+ years), comparing persons aged 65 years and older with those aged 45–64 years at the index admission. For the purpose of this study, persons from the age of 45 to 64 years are described as ‘middle-aged’ and those aged 65 years and over as ‘older-aged’ adults. Index episodes (first episode in the study period) were used to identify participants and for all comparisons.
Ethical approval for this study was obtained from the Hunter New England Human Research Ethics Committee (Registration number 14/02/19/5.01).
Clinical assessment and prospective data recording
The HATS database is a clinical case register that involves prospective data collection of toxicological and psychiatric variables using a preformatted clinical record sheet for all patients (Buckley et al., 1999) and additional information from the medical record entered by two trained personnel blinded to any study hypotheses. Drug prescription and drug ingestion data were determined by medical and toxicology staff from patient, family, ambulance, pharmacist and treating doctor sources as appropriate. Medical morbidity variables including intensive care unit admission, arrhythmia, seizure and delirium were determined from the clinical record.
The Department of Consultation Liaison Psychiatry provided psychiatric assessment for all DSP HATS patients (Whyte et al., 1997). All psychiatric diagnoses were made according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) (American Psychiatric Association [APA], 2000) based on clinical assessment (interview, collateral history and case note review). These clinical psychiatric assessments were undertaken during office hours (defined as 08:30–17:00, Monday to Friday) by trainee psychiatrists (psychiatric registrars) or a clinical nurse consultant within the department; after-hours assessments were undertaken by trainee psychiatrists on an on-call roster. Psychiatric assessments included patient interviews, informant interviews (general practitioner, other treatment services, family member or others) and a review of available public sector clinical records. All psychiatric diagnoses were reviewed at a weekly meeting and on entry into HATS database. All data entry is entered prospectively (i.e. after patient discharge) by trained data managers who are also clinicians.
Individual diagnoses for the period preceding the DSP event were identified by psychiatric staff and mapped to selected DSM-IV major diagnostic groups for analysis (mood, anxiety or psychotic disorder, substance use disorder), DSM-IV Relational Problems (within V codes), cognitive impairment (including diagnosis of dementia or cognitive disorder not otherwise specified) and ‘other’ diagnosis (including personality disorder). Suicidality was recorded using a three-level clinician-rated variable reflecting the clinician’s assessment of patient’s responses at the time of psychiatric assessment: no suicidal plan or ideation, low or moderate suicidal ideation and no plan, and high or intense suicidal ideation and/or a suicide plan.
Analysis
All statistics were performed using IBM SPSS Statistics 20 (SPSS Inc., Chicago, IL, USA). Number, percentage and chi-square tests were used to compare categorical variables for three domains: demographic, toxicological and psychiatric. Bonferroni adjustment for up to 15 tests of significance (for each of the three domains of comparison) was made and set at the level of p ⩽ 0.003 (Shott, 1990).
The specific variables for comparison are as follows:
Demographic: gender, marital status, employment, housing, support at home;
Toxicological: currently prescribed drugs by major drug groups, ingestions by major drug groups and medical morbidity;
Psychiatric: selected DSM-IV major diagnostic groups, suicidality at the time of psychiatric assessment, past suicide attempt, past psychiatric treatment, professional who completed psychiatric assessment (registrar in hours, registrar out of hours, clinical nurse consultant), life events prior to DSP (e.g. relational discord, physical illness, bereavement) and discharge destination (psychiatric hospital versus home).
We used a forward, step-wise, logistic regression to model and identify independent risk factors for discharge to the psychiatric hospital versus discharge home (including nursing home) as the binary dependent variable. Variables that showed significant association at the univariate level were included in the multivariate model; results were reported as odds ratio (OR) with 95% confidence interval (CI). Before possible inclusion in the multivariate model, predictor variables were examined for multicollinearity and when present, a decision made to select one variable. Interaction term variables were not used in this model.
Two analyses were conducted to detect interaction effects of age group on discharge destination. First, an unadjusted logistic regression for age group predicting discharge to the psychiatric hospital was conducted, followed by sequential, adjusted models, for each of the predictor variables that were significant in the original multivariate model, with reporting of the OR with 95% CI for age group. This allowed examination of any significant changes in the ORs for the age-group variable, after adjustment for each of the predictor variables, which, if significant, would suggest a possible interaction effect. Second, for each of the significant predictor variables (suicidality and any mood, anxiety or psychotic disorder), an age interaction term was created and used in two adjusted models. Results were reported as OR with 95% CI for the age-group variable with the middle-aged group used as the referent group.
Results
During the study period of interest, 5935 index presentations occurred for DSP patients aged 15 years and over. We excluded from this analysis a total of 4853 who were aged 15–44 years, leaving a total of 1082 index episode presentations for people aged 45 years and over. Of these 1082 patients, 157 (15%) were aged 65 years or over (older adult) and 925 (85%) were aged 45–64 years (middle-aged). The middle-aged group had a mean age of 52.3 years (SD = 5.08, range = 45–64 years) and the older adult group had a mean age of 74.23 years (SD = 7.33, range = 65–94 years).
Demographics
There were significant differences between the older- and middle-aged groups for marital, employment and housing status, but no difference in gender or support at home (Table 1). Older-aged adults commonly lived in their own home (68%) and were commonly separated, divorced or widowed (47%).
Demographic characteristics at index DSP episode.
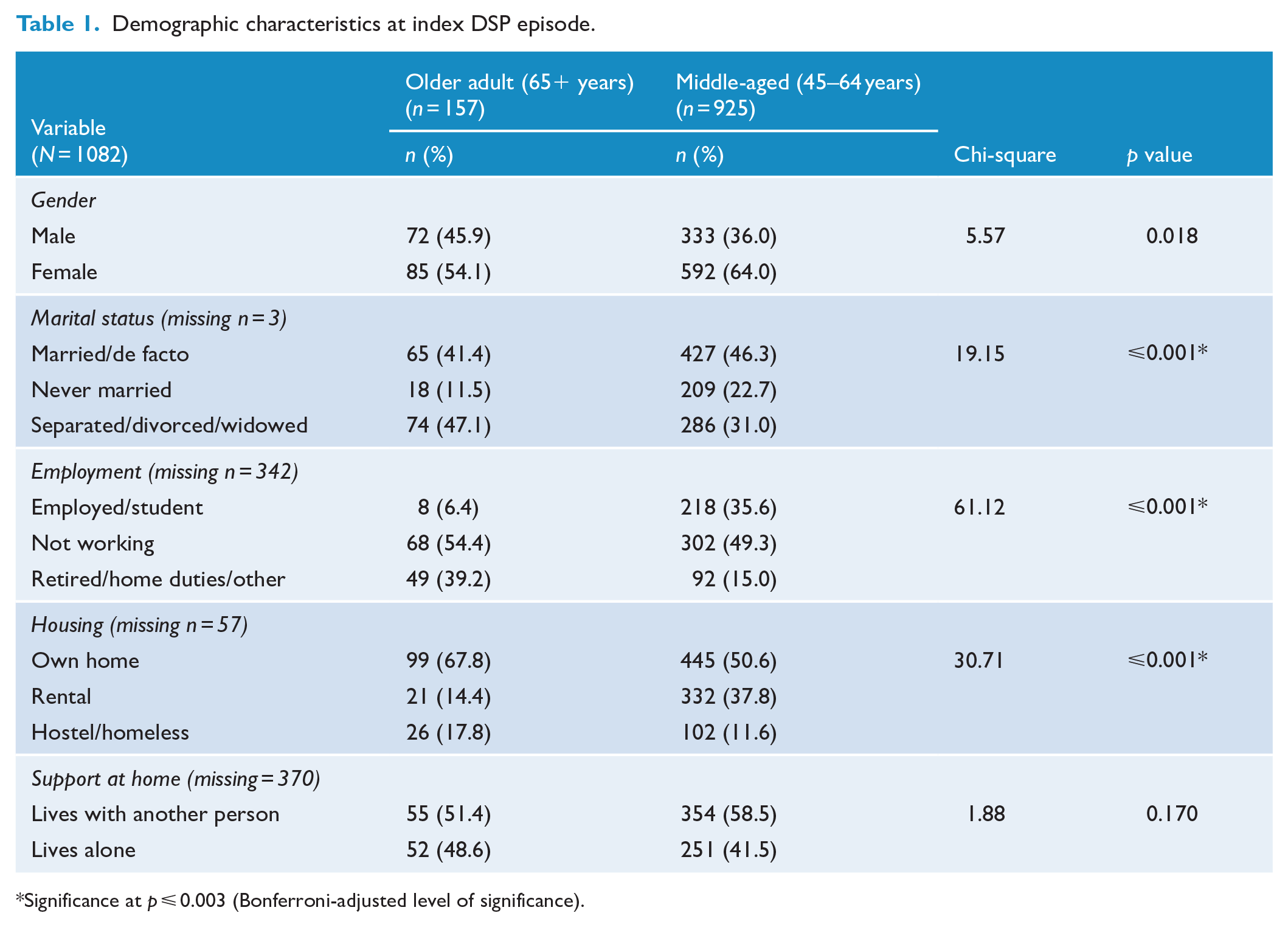
Significance at p ⩽ 0.003 (Bonferroni-adjusted level of significance).
Toxicological characteristics
Prescribed medication
There were no differences between the groups for the prescription of several common psychotropic medications (antidepressants, mood stabilisers and antipsychotic medications); however, the older-aged adults were significantly more likely to be prescribed benzodiazepines (54% vs 37%) and drugs for treatment of medical conditions (65% vs 40%) in the period preceding the DSP event (Table 2).
Toxicological characteristics at index DSP episode.
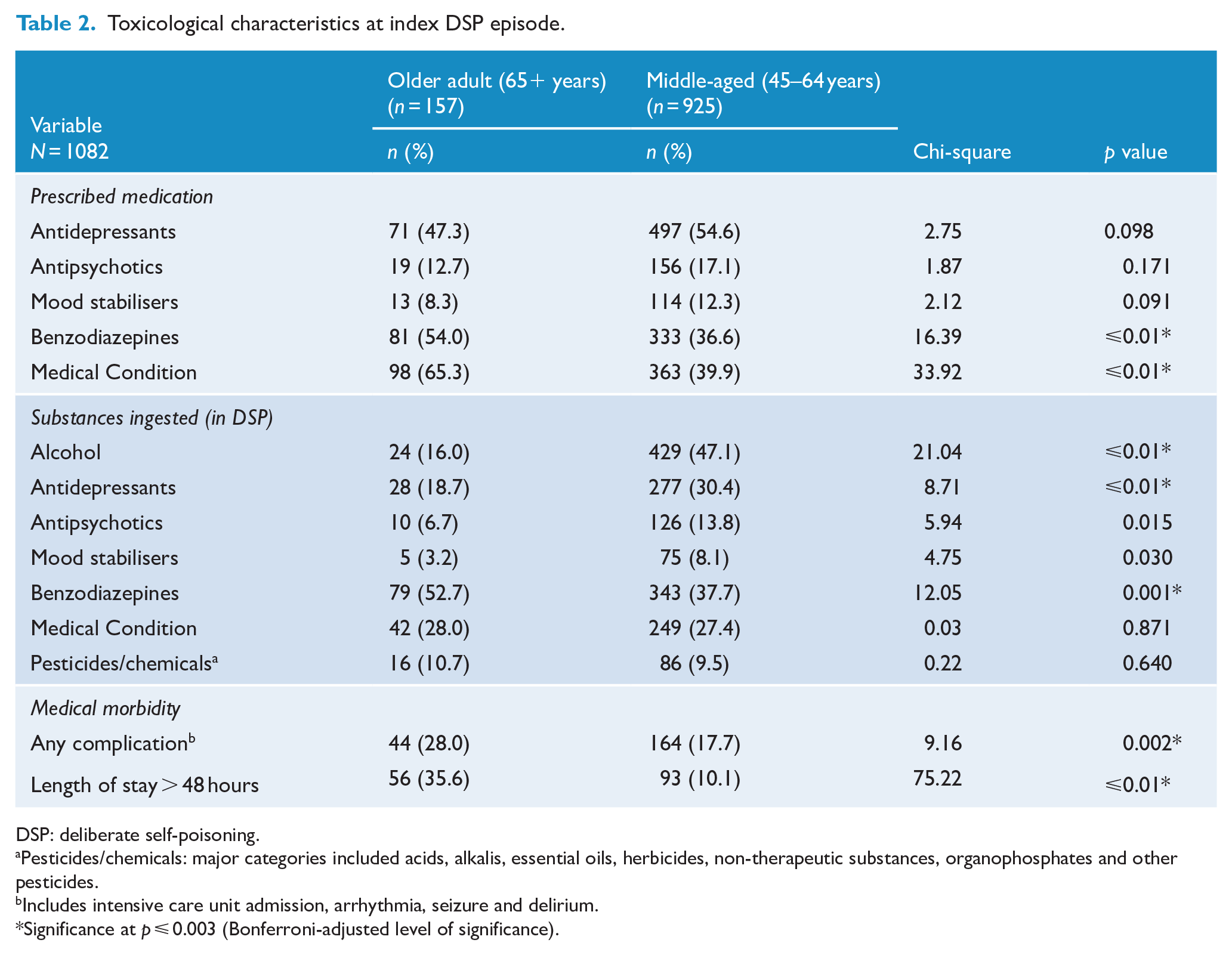
DSP: deliberate self-poisoning.
Pesticides/chemicals: major categories included acids, alkalis, essential oils, herbicides, non-therapeutic substances, organophosphates and other pesticides.
Includes intensive care unit admission, arrhythmia, seizure and delirium.
Significance at p ⩽ 0.003 (Bonferroni-adjusted level of significance).
Substances ingested (in the DSP)
The middle-aged group was significantly more likely to ingest antidepressant medications in the DSP episode (30% vs 19%), while the older-aged adults were significantly more likely to ingest benzodiazepines in the DSP episode (53% vs 38%). The middle-aged adults were also significantly more likely to ingest alcohol at the time of DSP (47% vs 16%).
Medical morbidity
The older-aged adults were more likely to develop complications during their episode of care (including any intensive care unit admission, arrhythmia, seizure or delirium) (28% vs 18%) and to be admitted for more than 48 hours (36% vs 10%).
Psychiatric characteristics
There were no differences between the older-aged and middle-aged groups for proportion presenting with any mood, anxiety or psychotic disorder (Table 3). However, the middle-aged group had a significantly higher proportion who presented with substance use disorders (52% vs 24%), relational problems (49% vs 31%), ‘other’ disorders (36% vs 18%), a past history of suicide attempt (55% vs 33%) and past psychiatric treatment (63% vs 49%), and they also reported more recent life events (65% vs 51%). When analysed independently (separated from the ‘other’ disorders), the middle-aged group also had a significantly higher proportion with a personality disorder (12% vs 1%). Conversely, cognitive impairment was higher in the older adult group (7% vs 2%). There were no differences between the two groups for current suicidality, the professional who conducted the assessment, or discharge destination.
Psychiatric characteristics at index DSP episode.
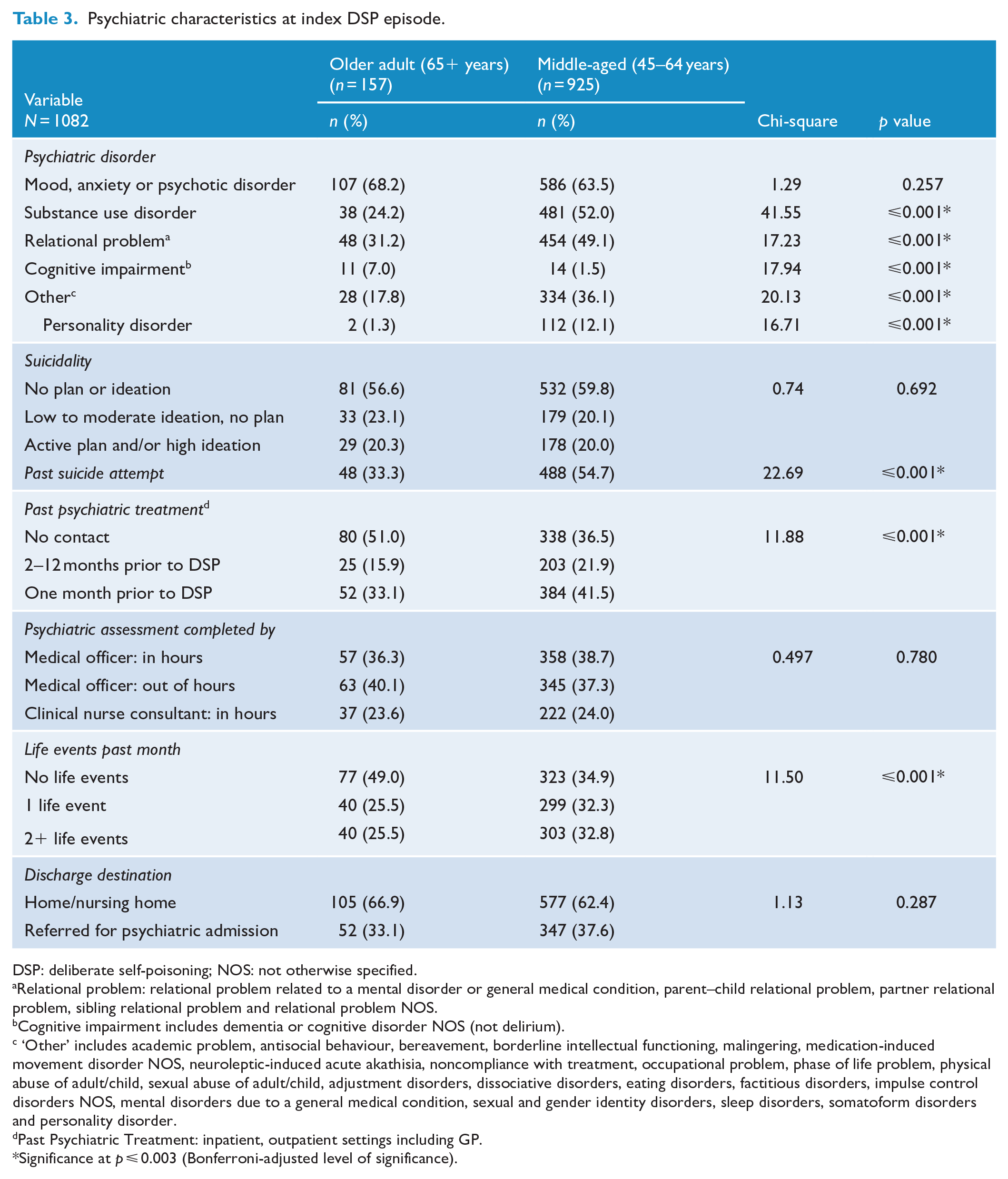
DSP: deliberate self-poisoning; NOS: not otherwise specified.
Relational problem: relational problem related to a mental disorder or general medical condition, parent–child relational problem, partner relational problem, sibling relational problem and relational problem NOS.
Cognitive impairment includes dementia or cognitive disorder NOS (not delirium).
‘Other’ includes academic problem, antisocial behaviour, bereavement, borderline intellectual functioning, malingering, medication-induced movement disorder NOS, neuroleptic-induced acute akathisia, noncompliance with treatment, occupational problem, phase of life problem, physical abuse of adult/child, sexual abuse of adult/child, adjustment disorders, dissociative disorders, eating disorders, factitious disorders, impulse control disorders NOS, mental disorders due to a general medical condition, sexual and gender identity disorders, sleep disorders, somatoform disorders and personality disorder.
Past Psychiatric Treatment: inpatient, outpatient settings including GP.
Significance at p ⩽ 0.003 (Bonferroni-adjusted level of significance).
Multivariate models for discharge to psychiatric hospital
The multivariate model for discharge to psychiatric hospital showed two significant predictor variables: current suicidality – using a referent group of no suicide plan/thoughts, low/moderate suicidal ideation with no plan had an OR of 12.10 (95% CI = [8.09, 18.09]), while those with strong/intense suicidal ideation and/or an active suicidal plan had an OR of 64.28 (95% CI = [37.12, 111.33]); and psychiatric diagnosis – using a referent group of no diagnosis, a diagnosis of any mood, anxiety or psychotic disorder had an OR of 2.74 (95% CI = [1.81, 4.15]) (Table 4).
Forward stepwise regression model for discharge to psychiatric hospital.
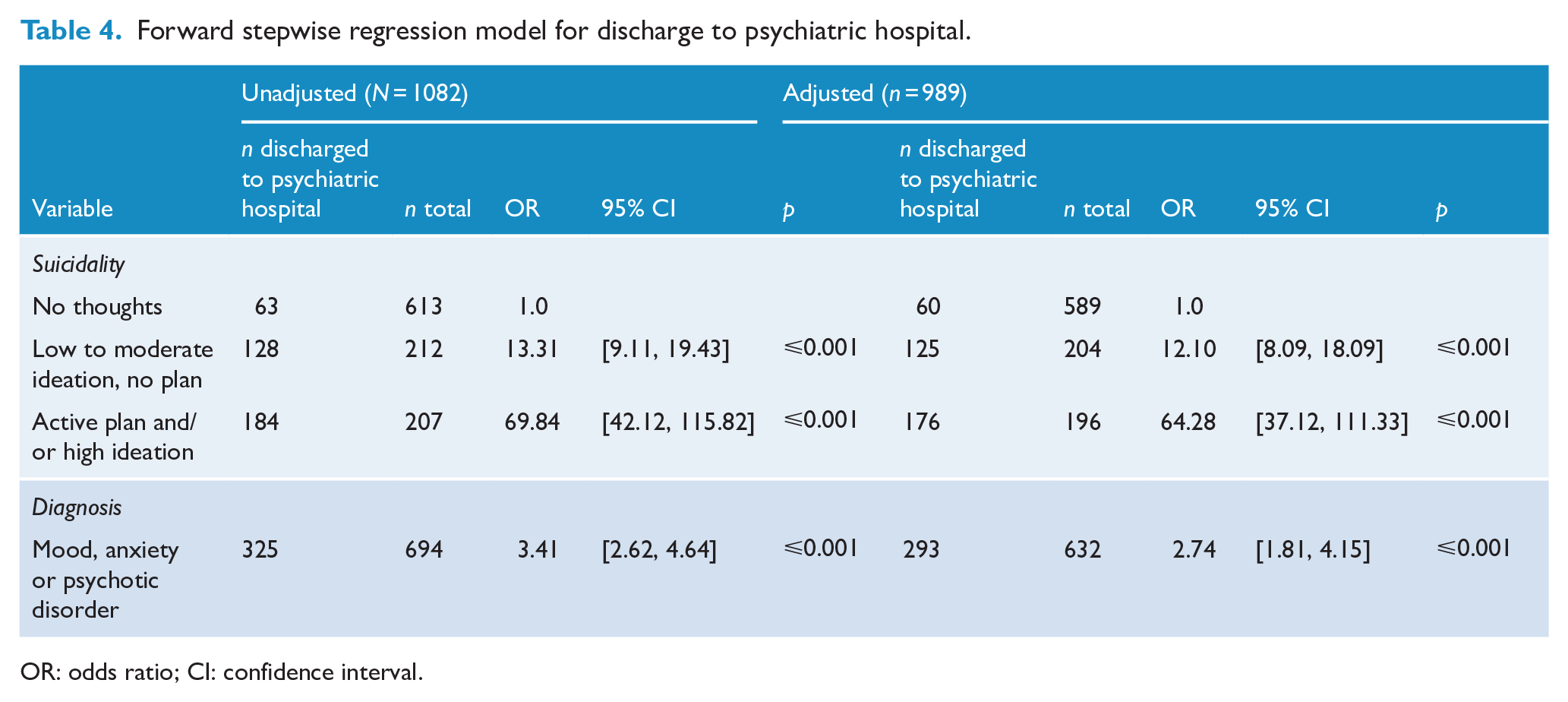
OR: odds ratio; CI: confidence interval.
Unadjusted and adjusted estimates of discharge to psychiatric hospital by age group
The unadjusted model of age group as a predictor for discharge to psychiatric hospital showed no significant association (OR = 0.83, 95% CI = [0.58, 1.18]) with middle-aged as the referent group. The sequential adjusted model to explore possible interaction for age group after adjustment for suicide level was (OR = 0.63, 95% CI = [0.38, 1.05]) and for any mood, anxiety or psychotic disorder was (OR = 0.76, 95% CI = [0.52, 1.10]). Adjustment for each of the two variables did not substantially change the ORs for the age-group variable or make the relationship of age group and discharge to psychiatric hospital become significant.
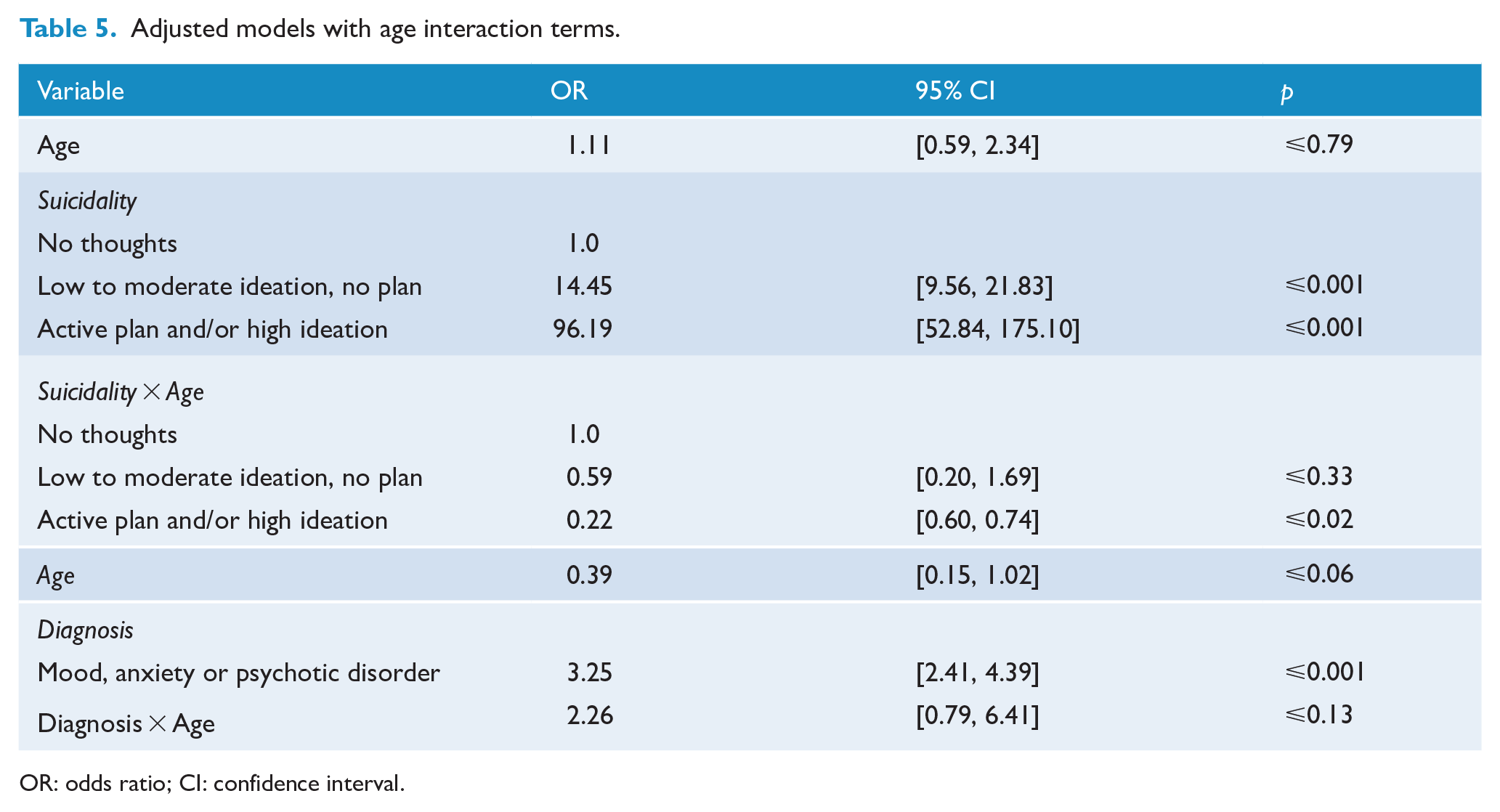
In models adjusting for interaction terms (suicide level by age, and for any mood, anxiety or psychotic disorder by age), there was no significant effect for age on discharge to a psychiatric hospital. There was only one minor age interaction effect; for an active plan and/or high ideation, the older-aged patient had a reduced likelihood for discharge to the psychiatric hospital (OR = 0.22, 95% CI = [0.60, 0.74]; see Table 5).
Adjusted models with age interaction terms.
OR: odds ratio; CI: confidence interval.
Discussion
Main findings
The older-aged group was similar to the middle-aged group in several ways: proportion living alone, reporting suicidal ideation/planning, prescribed antidepressant and antipsychotic drugs, and with a psychiatric diagnosis. However, the older-aged group were also different in several ways: greater proportion with cognitive impairment, higher medical morbidity, longer length of stay and greater prescription and ingestion of benzodiazepines in the DSP event. Suicidality at the time of psychiatric assessment and the presence of common psychiatric disorders (any mood, anxiety or psychotic disorder) were the independent predictors of discharge to the psychiatric hospital. Older age was not a predictor of referral for psychiatric hospitalisation in the multivariate model.
Clinical needs of older-aged DSP patients
Older adults present less frequently to hospital with DSP and so clinicians will be more familiar with younger patients. The previous president of the RANZCP identified mental health care for adults over 65 years as a priority and identified DSH as an important area for intervention (Hopwood, 2017). The RANZCP clinical practice guidelines for DSH suggested that each DSH patient requires ‘an assessment of modifiable risk factors for self-harm, such as substance use, psychosis, mood disorder, anxiety disorder, eating disorder, personality disorder, medical conditions, relationship difficulties and social problems’ (Carter et al., 2016). This study helps us to identify some of the features of these modifiable risk factors in the older-age population, which should help to inform clinical assessment.
A substantial proportion of the older-aged adults presented with DSM-IV mood, anxiety or psychotic disorders (68%), lower support at home (living alone) (49%), and an active suicide plan and/or high suicidal ideation (20%), which might require interventions to reduce exposure to these risk factors. The prescribed medications in the older-aged patients included antidepressants (47%) and antipsychotics (13%), which flag necessary points of review.
In other ways, the pattern of modifiable risk factors for subsequent suicidal behaviours in the older-aged group was different to the middle-aged group. Older-aged patients were less likely to be diagnosed with substance use (24%), relational problems (31%) and ‘other’ disorders (18%), although these would still warrant intervention. The diagnosis of a quarter of older-aged patients (and half of middle-aged patients) with substance use disorder supports recent recommendations for the inclusion of routine screening and assessment for alcohol use disorders following self-harm (Cheung et al., 2017).
Unsurprisingly, a greater proportion of the older-aged patients were found to have cognitive impairment (diagnosis of dementia or cognitive disorder not otherwise specified) (7%), complications during treatment (intensive care unit admission, arrhythmia, seizure and/or delirium) (28%) and longer lengths of stay (more than 48 hours) (36%). In a New South Wales population study of older-aged adults, dementia was associated with a 1.5 times higher rate of hospital-treated DSP than those without a dementia diagnosis (Mitchell et al., 2015). The presence of dementia and cognitive disorders will affect the process of, and the setting for, clinical assessment and have implications for after-care management.
Benzodiazepines and older-aged adults
A substantial proportion of the older-age patients reported they were prescribed benzodiazepines (54%). Benzodiazepine prescription has been associated with older adult suicide death (Carlsten et al., 1999; Gavrielatos et al., 2006; Nowers, 1993; Stein et al., 1993; Vukcevic et al., 2016), although this may represent confounding by indication rather than a causal association. A previous HATS study of hospital-treated older-aged DSP (Ticehurst et al., 2002) found a similar proportion prescribed benzodiazepines (62%), suggesting there has been little change over at least 15 years in prescribing patterns for this population. Moreover, these rates are higher than the substantial benzodiazepine prescription rates reported for the Australian ‘elderly’ in the general community (5–30%) (Kirby et al., 1999; Tamblyn et al., 2005) or for community populations with suicidal ideation (17%) (Almeida et al., 2012). These findings suggest an important consideration should be identifying the prescription of benzodiazepines and deciding on appropriate management during inpatient care (with the medical and psychiatric teams) and after-care (with primary care providers or community mental health services). The assessment for relevant diagnoses (e.g. depression, anxiety, insomnia) would be a necessary minimum when reviewing alternate management options, as would the assessment and management of judicious benzodiazepine withdrawal where indicated.
The prescription of benzodiazepines in older adults may represent undiagnosed or sub-optimally treated anxiety and/or depression, with benzodiazepines prescribed in preference to more appropriate medications and psychological treatments. In a community population, 44% of older adults with anxiety and 34% with depression were prescribed benzodiazepines (Shah et al., 2002). This pattern of preferential benzodiazepine prescription (Draper, 1994; Shah et al., 2002; Wolitzky-Taylor et al., 2010) is apparent despite the many significant known adverse effects including falls, cognitive impairment, sedation and impaired driving skills (Madhusoodanan and Bogunovic, 2004; Tamblyn et al., 2005; Windle et al., 2007). Prescription of benzodiazepines may be a consequence of time constraints for clinicians, lack of access to allied health professionals and limitations of the Medicare billing structure in general practice (Anthierens et al., 2007). It could also be speculated that the prescription of benzodiazepines in older adults represents treatment efforts for comorbid anxiety disorders. This may be significant when 30–50% of older depressed adults have a diagnosis of comorbid anxiety (Lenze et al., 2000; Mehta et al., 2003; Wolitzky-Taylor et al., 2010). Furthermore, comorbid anxiety (Bartels et al., 2002), and obsessional and anxious personality traits (Harwood et al., 2001) have been identified as predictors for suicidal ideation and suicide in the older adult.
The common ingestion of benzodiazepines in the DSP event is also noteworthy. In older adults, benzodiazepines are frequently prescribed on a long-term basis for anxiety and insomnia, and it has been suggested that this ready availability is linked to the ingestion in the DSP event (Carlsten et al., 2003; Gavrielatos et al., 2006; Stein et al., 1993; Vukcevic et al., 2016). In our study, benzodiazepines were commonly ingested in the DSP event (53%), almost the same level reported in a Sydney DSP older age population (64%) (Draper, 1994) and an earlier HATS study (62%) (Ticehurst et al., 2002). A recent HATS study of both DSP and non-intentional poisoning cases in older adults has also shown that benzodiazepines are the most commonly ingested medications; however, there has been a relative reduction of around 50% of admissions where benzodiazepine ingestion was implicated (Pillans et al., 2017), suggesting a possible reduction in ingestion despite availability.
However, the choice to take benzodiazepines in the DSP event may be driven by more than the concept of taking available medications. Older-aged adults were commonly prescribed antidepressant medications (47%) or medications for medical conditions (65%), but ingested them less commonly in the DSP event (19% and 28%, respectively). Our study cannot explain this apparent differential ingestion of benzodiazepines in the DSP; however, we offer some speculative explanations. The differential ingestion of benzodiazepines in DSP may represent an incorrect perception by older-aged adults that benzodiazepines are a drug of higher lethality, which would be consistent with a previous finding that DSP in older-aged adults was associated with a higher degree of planning and intent (De Leo et al., 2001; Draper, 2014; Frierson, 1991; Hawton and Harriss, 2006), although the level of suicidal thoughts and plans was not higher than the middle-aged group in our study. Alternatively, older-aged patients may perceive benzodiazepines to be a less distressing method of suicide whereby they will ‘just go to sleep’, because these medications are recognised as ‘sleeping tablets’. Future studies exploring perceptions of benzodiazepines by the older-aged are needed.
Discharge to the psychiatric hospital
Older age and discharge to the psychiatric hospital
In our study, the referral for psychiatric hospitalisation did not differ by age group. Nor did we find any strong interaction of age group with two key predictor variables for the decision to refer for psychiatric hospitalisation (level of suicidality and any mood, anxiety or psychotic disorder). Older-aged patients with a suicide plan or high suicidal ideation were less likely to be discharged to a psychiatric hospital than similarly suicidal middle-aged patients, but there were no other interaction effects. This suggests, at least for our population, that the rating of suicidality and the diagnosis of these psychiatric disorders were seen as important modifiable risk factors that could be addressed at least in part by psychiatric hospitalisation, largely unaffected by the age of the patient. It is possible that discharge to the psychiatric hospital might be affected by bed availability in the local area, although this clinical population is relatively well served for public and private psychiatric beds. We would not expect bed availability to necessarily produce a differential effect on discharge destination based on patient age; however, our study design does not allow us to address this question.
Strengths and limitations
All the psychiatric clinical exposure variables including level of suicidal ideation, suicidal planning and psychiatric disorder were made as a result of clinical assessment, using clinical ratings rather than self-report or structured instruments. Additional limitations include the limited power of the study to test multiple predictors in the multivariate model of discharge to psychiatric hospital since our study only included 157 older-aged participants. Furthermore, we modelled only the clinician decision to transfer to a psychiatric hospital as the primary outcome and did not model actual admission to the psychiatric hospital. This study excluded other forms of DSH such as jumping, hanging and cutting, so generalisation of these findings to other self-harm populations needs caution.
The strengths of this study are the prospective, longitudinal cohort design with all DSP events from a representative population for one geographical area. This enabled consistency of data collection for all DSP index episodes. This study also used a systematic, standardised recording of psychiatric assessment variables for DSP patients and compared older-aged adults with a more appropriate age group than previous studies.
Conclusion
This study identified several specific areas that need to be addressed in the clinical assessment of older-aged adults after a DSP event. These include identification of modifiable risk factors for subsequent suicidal behaviours such as mood, anxiety or psychotic disorders, lower support at home, active suicidal plan or intense suicidal ideation. Furthermore, despite fewer older-aged adults having substance use disorders, relationship problems or other DSM-IV disorders, these modifiable risk factors should be included in the assessment of clinical needs of older adults. The older adults were also more likely to present with cognitive impairment, medical complications, a longer length of stay and greater proportion with ingestions of benzodiazepine in the DSP event, which may impact on the process of clinical assessment and clinical management in the general hospital. Benzodiazepine prescription may be an important focus of clinical attention during the inpatient stay in the general or psychiatric hospital and during the period of follow-up care in the community.
Footnotes
Acknowledgements
M.J. was awarded a passing grade for her RANZCP scholarly project, which presented aspects of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: K.M.’s position is funded by the Burdekin Suicide Prevention initiative administered by Hunter New England Mental Health Service.