
Abstract
Objective:
Voltage-gated potassium channel antibodies are implicated in limbic encephalitis and currently included in first-episode psychosis organic screening guidelines. Individuals with high-positive voltage-gated potassium channel titres most commonly present with neurological symptoms as well as sleep, cognitive, behaviour, psychosis and mood disturbance. The significance of low-positive voltage-gated potassium channel antibody titres in psychiatric patients is unclear and has not been previously examined. We aim to describe a statewide cohort of psychiatric patients with low- and high-positive voltage-gated potassium channel titres and explore if this finding influenced clinical management and patient outcomes.
Methods:
A retrospective review of all voltage-gated potassium channel antibodies testing performed in public psychiatric services in Queensland, Australia, with comparison of the clinical presentation and long-term outcomes of low- and high-positive voltage-gated potassium channel titre cases. Specific antigen targets (leucine-rich glioma-inactivated protein 1 and contactin-associated protein 2 antibodies) were also assessed.
Results:
The overall prevalence of voltage-gated potassium channel antibody positivity in Queensland, public, psychiatric service testing was 0.3% (14/4098), with 12 cases of low-positive voltage-gated potassium channel titre, 2 cases of high-positive (leucine-rich glioma-inactivated protein 1 antibody positive) cases and a voltage-gated potassium channel negative contactin-associated protein 2 antibody positive case. No low-positive case developed neurological abnormalities or had abnormal paraclinical investigations. In comparison, both high-positive voltage-gated potassium channel/leucine-rich glioma-inactivated protein 1 cases and the contactin-associated protein 2 antibody positive case rapidly developed neurological symptoms, had abnormal paraclinical testing and improved only with immunotherapy. There was no later development of encephalitic symptoms in the low-positive cases over an average of 1067 days follow-up.
Conclusion:
Voltage-gated potassium channel antibody–associated limbic encephalitis was rare, and always associated with high antibody titres. Low-positive titres were not associated with the development of encephalitis over a long period of follow-up. The value of universal voltage-gated potassium channel antibody screening is unclear, and further prospective studies in first-episode psychosis populations are required.
Introduction
Antibodies to the voltage-gated potassium channel (VGKC) complex have been implicated in the pathogenesis of limbic encephalitis and other syndromes including dystonic seizures and peripheral nerve hyperexcitability (Irani et al., 2010, 2011, Buckley et al., 2001). Neurological symptoms such as seizures, movement disorder and dysautonomia dominate the clinical presentation, with sleep disorders (insomnia and hypersomnia) and cognitive deficits (typically memory impairment and confusion) being common features (Cornelius et al., 2011; Frisch et al., 2013; Somers et al., 2011). Psychiatric symptoms such as personality change, psychosis, mood and anxiety disturbance have been reported, but will usually be accompanied by neurological abnormalities (Irani et al., 2010; Pollak et al., 2016; Somers et al., 2011; Tang et al., 2015). Rarely, psychiatric presentation with delayed neurological progression has led to diagnostic difficulty, and VGKC antibody testing has been included in recommended organic screening for psychiatric patients, particularly in first-episode psychosis (Galletly et al., 2016; Guirindhra Koumar Radja and Andrea Eugenio Cavanna, 2013; Somers et al., 2011).
VGKC syndromes may be paraneoplastic and are primarily associated with strongly positive VGKC titres (>300 pM) (Irani et al., 2010; Paterson et al., 2014). The significance of ‘low-positive’ titres in the 85–300 pM range is unclear (Huda et al., 2015; Jammoul et al., 2016; Paterson et al., 2014; Van Sonderen et al., 2016). In addition, it is now understood that classical syndromes associated with positive VGKC testing usually have specific antibodies directed to components of the VGKC complex (leucine-rich glioma-inactivated protein 1 [LGi1] and contactin-associated protein 2 [CASPR2]) (Irani et al., 2010; Van Sonderen et al., 2016). These antibodies are not routinely tested in psychiatric populations; only assessed after VGKC antibody positivity (Galletly et al., 2016).
As a result, there are increasing numbers of psychiatric patients with low-positive VGKC antibodies detected in serum, without specific antigenic targets, that present a diagnostic and management challenge. Clinical diagnostic criteria for autoimmune encephalitis have been proposed, but not yet validated in this group (Graus et al., 2016). This study aims to describe a cohort of psychiatric patients with low- and high-positive VGKC titres and explore if this finding influenced clinical management and patient outcomes.
Method
A retrospective electronic and paper chart review of a statewide cohort of VGKC antibody cases, titre over 85 pM, presenting to psychiatric services in Queensland, Australia, up to and including December 2019, was performed. Ethical approval for this study was granted from the Metro South Human Research and Ethics Committee (HREC/17/QPAH/423A).
All VGKC antibodies testing for the state since 2010 has been performed in a single laboratory (Pathology Queensland, Brisbane, Australia) which is a diagnostic referral laboratory offering specialised neuroimmunology testing. VGKC antibodies are detected through a commercial radioimmunoprecipitation assay of iodinated dendrotoxin (125I-α-DTX)-labelled VGKCs in digitonin-solubilised mammalian brain homogenates (RSR, United Kingdom). LGi1 and CASPR2 antibodies were detected by a commercially available cell-based assay of antigen-transfected cells (Euroimmun, Germany). The cell-based assay was performed if there was a positive VGKC antibody result or if another anti-neuronal antibody which uses the same test (methyl-D-aspartate, alpha-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid, G-protein coupled receptors for gamma-aminobutyric acid B) was requested. Cases were identified by the laboratory records with additional review of positive CASPR2 and LGi1 antibody results. Adult cases were included if there was a positive immunoglobulin G (IgG) VGKC antibody result over 85 (pM) (as per manufacturer’s instructions) in serum, and testing was performed by psychiatric services. Cases were excluded if residing out of state or tested by a private physician.
Case identification and data collection were performed separately by two authors (F.C. and N.W.) with any discrepancy discussed with all authors. Collected variables were pre-selected, based on literature review, and included the following: demographics, admission details, medical and psychiatric history, clinical features of presentation, results of investigations and treatment received. Variables of the probable and definitive clinical diagnostic criteria for autoimmune encephalitis were noted (Graus et al., 2016). A diagnosis and symptom list from the most recent clinical assessment was also collected. For clinical features, missing data were recorded as absence of that feature. For investigations, missing data were recorded as not tested.
Cases were clustered, based on the manufacturer instructions (RSR) and literature review, into two groups for comparison: low-positive VGKC (VGKC titre 85–300 pM) and high-positive VGKC (VGKC titre >300 pM) (Huda et al., 2015; Jammoul et al., 2016; Paterson et al., 2014; Van Sonderen et al., 2016). Descriptive statistics were employed for analysis of the data.
Results
From 4098 anti-VGKC antibody tests in public psychiatric services, Queensland, Australia, between 2015 and 2019, there were 14 positive cases with a VGKC antibody titre over 85 pM, comprising 12 cases of low-positive titre 85–300 pM and 2 cases of high-positive titre >300 pM (Figure 1).
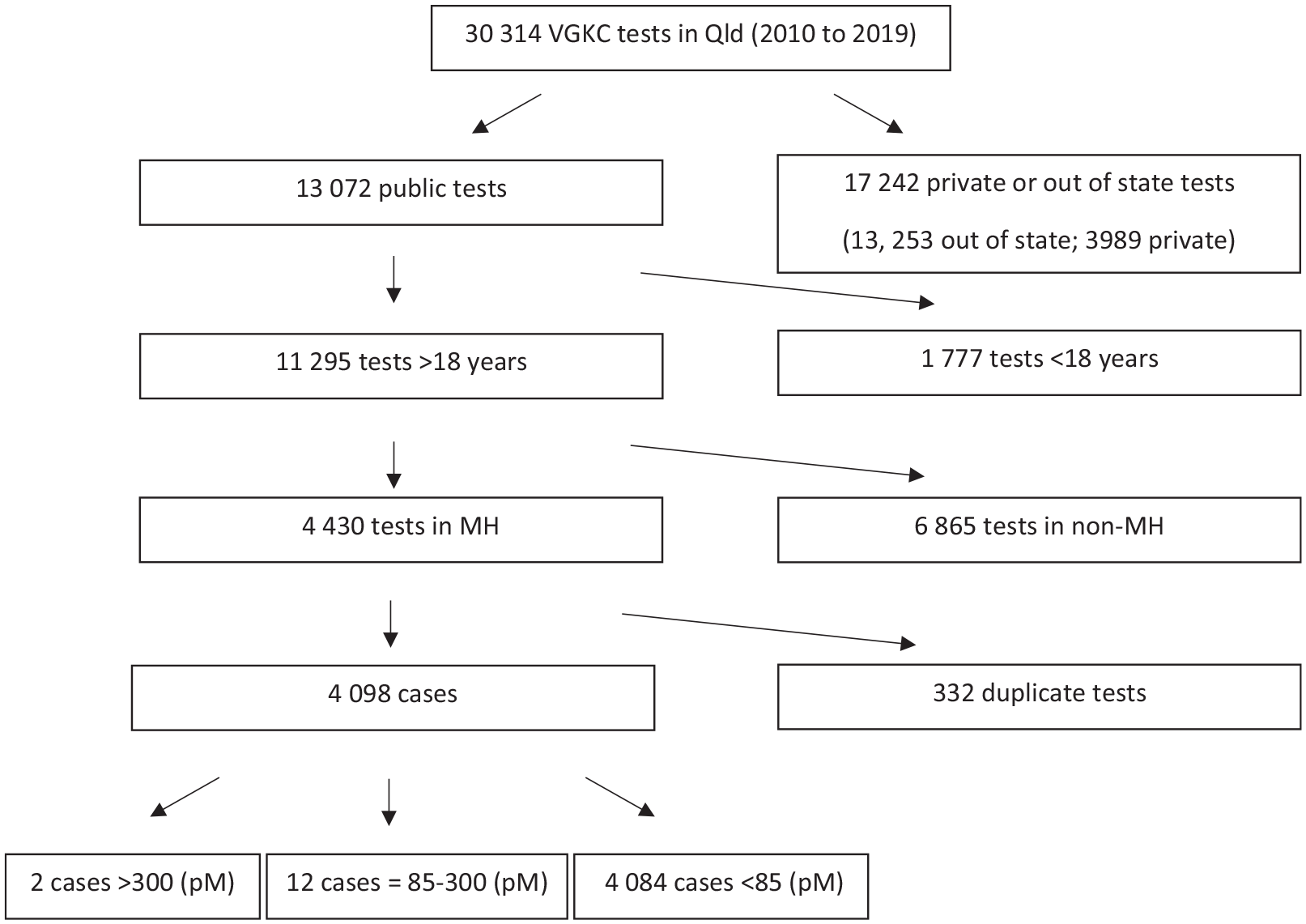
VGKC testing in Queensland, Australia.
Of the 4084 negative cases with a VGKC antibody titre under 85 pM, the mean average age was 39.74 years (standard deviation [SD] = 15.4, age range = 18–78 years) and the male-to-female ratio was 1.9:1. The mean average VGKC antibody titre for these cases was 5.3 pM (SD = 13.0). All negative VGKC antibody cases were tested for LGi1 and CASPR2 antibodies, and there was one case of negative VGKC (titre 79 pM) with positive CASPR2 antibody.
In the low-positive titre cases (Table 1), the male-to-female ratio was 2:1 and age range = 19–70 years – mean = 36.3 years (SD = 14.0). Testing was completed as part of first-episode psychosis screening in eight cases and due to a deterioration in mental state with a background of psychotic disorder in four cases – schizophrenia (three cases) and bipolar affective disorder (BPAD) (one case). VGKC titre ranged from 97 to 233 pM, with repeated testing in all cases again returning a low-positive titre result. No case had positive LGi1, CASPR2 or other anti-neuronal antibodies. Cerebrospinal fluid (CSF) testing occurred in 6/12 cases with no abnormal findings. All cases were reviewed by a neurologist or general physician, and there was no identified paraneoplastic cause identified. Two cases had a past history of non-neuronal autoimmune disorders (one case of autoimmune hepatitis and one case of Graves’ disease).
Low-positive VGKC antibody titre cases.
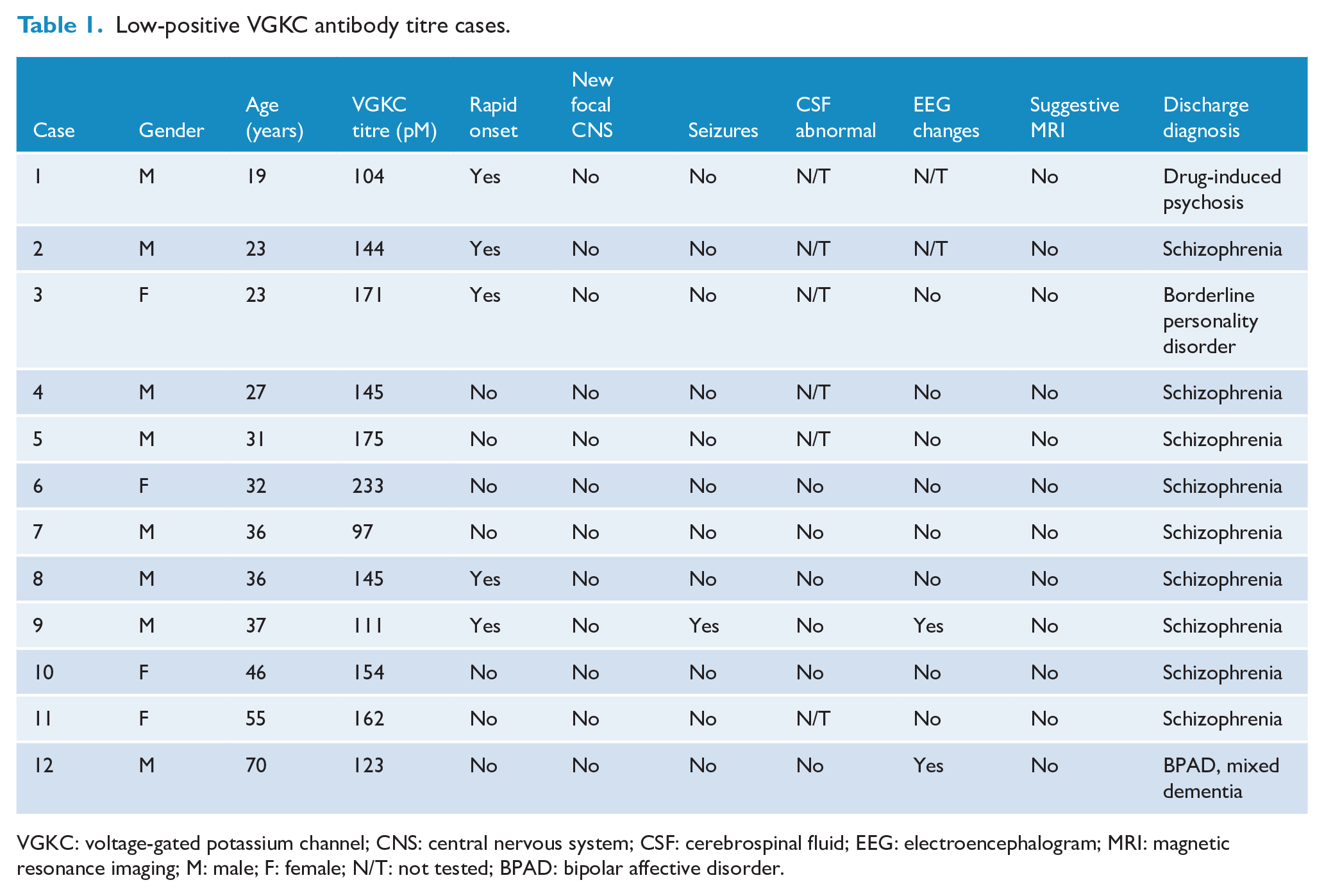
VGKC: voltage-gated potassium channel; CNS: central nervous system; CSF: cerebrospinal fluid; EEG: electroencephalogram; MRI: magnetic resonance imaging; M: male; F: female; N/T: not tested; BPAD: bipolar affective disorder.
The majority of low-positive titre cases presented with psychosis (11/12 cases) and agitation (9/12 cases). Insomnia and anxiety were both reported in 5/12 cases, with 3/12 cases noting depressed mood and no case reporting elevated mood or labile affect. Disorientation was noted in 3/12 cases and memory disturbance in one case with no cases reporting decreased or clouding of consciousness. No focal neurological abnormality, speech disturbance or autonomic dysregulation were seen. No low-positive titre case fulfilled the proposed definitive clinical diagnostic criteria. Initially, one case fulfilled the probable clinical diagnostic criteria, due to a seizure on day 2 of admission and an abnormal electroencephalogram (EEG) (moderate encephalopathy) although this was later attributed to alcohol withdrawal and there were no further neurological symptoms or abnormal investigations.
No low-positive titre case received immunomodulatory treatment; all were treated with antipsychotics and reported improvement by discharge with a mean average admission time of 31.7 days (SD = 34.6). An extrapyramidal side effect (EPSE) of parkinsonism was reported in 2/12 cases, both of which resolved with changed antipsychotic. Discharge diagnoses were schizophrenia in 9/12 cases, drug-induced psychosis 1/12, borderline personality disorder 1/12 and bipolar affective disorder with mixed neurocognitive disorder 1/12. On follow-up to May 2020, a mean average time of 1067 days post discharge (SD = 391.1), all cases remained under the care of psychiatric services and showed stability of diagnosis, except the drug-induced psychosis case, later recorded as having a diagnosis of schizophrenia. At final review, no case has reported neurological symptoms or further cognitive decline (including the case with a mixed neurocognitive disorder diagnosis).
The two high-positive titre cases (Table 2) (female 46 years and male 58 years) each presented with a rapid onset of new psychiatric symptoms of agitation, insomnia, disorientation and short-term memory disturbance, with one case reporting psychosis and the other noting severe depressive symptoms. Antibody testing was performed as routine screening, but both developed neurological symptoms (focal movement disturbance or seizures) within a short time (mean = 3.3 days, SD = 1.3), prior to the return of antibody results. VGKC titre was 332 and 678 pM, respectively, and both were positive for LGi1 antibodies. Abnormal EEG (diffuse encephalopathy) or magnetic resonance imaging (MRI) (T2/FLAIR signal in medial temporal lobes) suggestive of encephalitis was present. Neither case demonstrated elevated white cells or oligoclonal banding in CSF, one case reporting elevated protein (580 mg/L). There was no associated malignancy or history of autoimmunity. Both cases were prescribed olanzapine, but this was ceased due to concern for EPSE. Each received immunomodulatory therapy (intravenous immunoglobulin and methylprednisolone) noting an improvement of symptoms with ongoing mild cognitive deficits noted in both at discharge (56 and 85 days). One case was lost to follow-up (last reviewed 360 days post discharge), and the other continues with clinic reviews (595 days post discharge). There was no continuation or recurrence of psychiatric or neurological symptoms in either case.
High-positive VGKC antibody titre or specific antigen target positive cases.
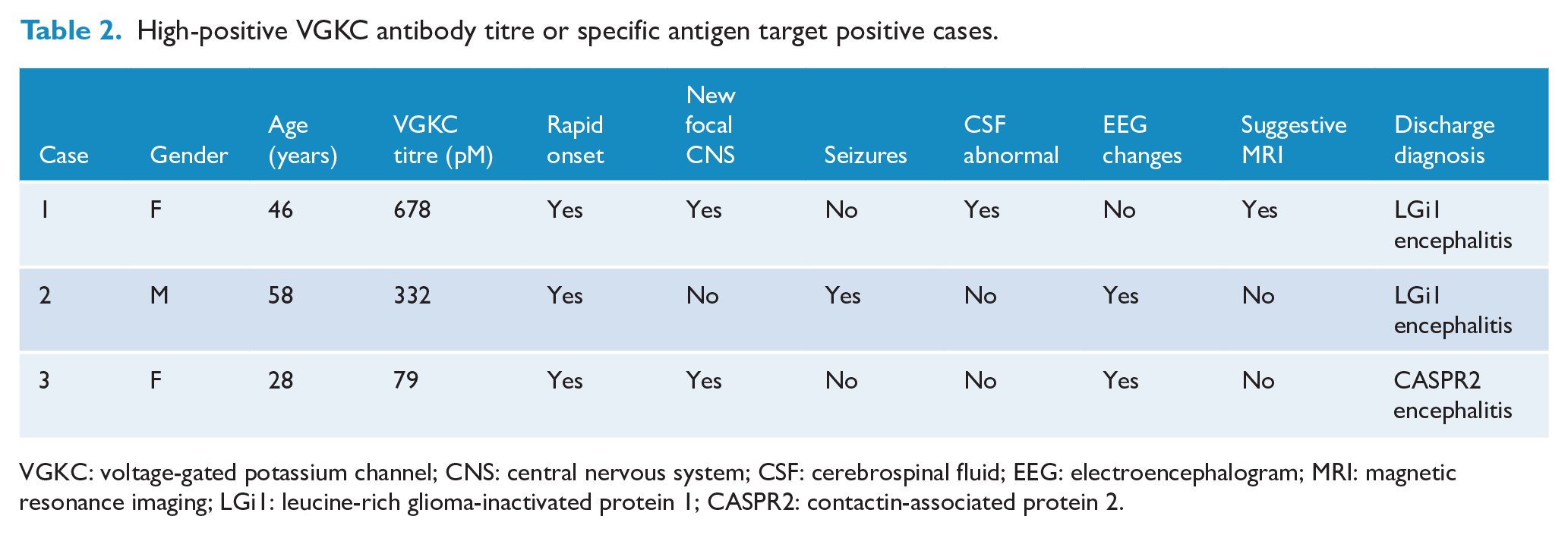
VGKC: voltage-gated potassium channel; CNS: central nervous system; CSF: cerebrospinal fluid; EEG: electroencephalogram; MRI: magnetic resonance imaging; LGi1: leucine-rich glioma-inactivated protein 1; CASPR2: contactin-associated protein 2.
There was an additional case of negative VGKC antibody (titre 79 pM) with positive CASPR2 antibodies (Table 2). This case, previously reported by the authors, was of a 28-year-old female, 6 weeks postpartum, who presented with rapid onset psychosis, developing focal movement disorder 1 day post admission (Warren et al., 2019). CSF and MRI brain were normal; EEG demonstrated diffuse encephalopathy. There was significant treatment resistance to psychotropics and electroconvulsive therapy, but resolution of all symptoms following immunomodulation therapy. Review at 320 days post discharge notes no ongoing or recurrent psychiatric or neurological symptoms, no associated malignancy, but some mild cognitive deficits.
Discussion
This study demonstrates that psychiatric presentations with low-positive VGKC antibody levels in the absence of LGi1 or CASPR2 antibodies do not develop neurological abnormalities and had normal paraclinical investigations. In comparison, psychiatric presentations with high-positive VGKC titres and/or LGi1 or CASPR2 antibodies rapidly developed neurologic symptoms and had other abnormalities on EEG, CSF analysis or MRI. The proposed clinical diagnostic criteria for autoimmune encephalitis were effective at differentiating these two groups within the first week following admission, as did the presence of any new or unexplained neurological symptoms. Long-term follow-up, over an average of 1067 days, confirmed that no low-positive VGKC titre case developed neurological symptoms and all maintained their diagnosis with a primary psychiatric disorder. The overall prevalence of VGKC antibody positivity in psychiatric service testing was 0.3% (14/4098), with a prevalence of 0.05% (2/4098) for cases of VGKC antibody positivity that had clinical/paraclinical findings consistent with an encephalitis.
Rarely, VGKC antibodies have been associated with cognitive and psychiatric abnormalities without the development of neurologic features (Guirindhra Koumar Radja and Andrea Eugenio Cavanna, 2013). These cases reported short-term memory deficits, affective or psychotic symptoms and abnormal paraclinical tests (Buckley et al., 2001; Chan et al., 2007; Kartsounis and De Silva, 2011; McKeon et al., 2007; Parthasarathi et al., 2006; Tang et al., 2015; Vincent et al., 2004). In all of the cases reported in the literature, however, the VGKC titres were high (over 400 pM), noting the majority pre-dated CASPR2 or LGi1 testing (Guirindhra Koumar Radja and Andrea Eugenio Cavanna, 2013; Tang et al., 2015). Studies looking specifically at first-episode psychosis have not shown significant difference in levels of VGKC antibodies from healthy controls (Gaughran et al., 2018; Lennox et al., 2017).
Retrospective review of low-positive VGKC cohorts has found that most cases were not associated with any encephalitic syndrome and those that were, had early prominent neurological symptoms (Hacohen et al., 2013; Huda et al., 2015; Jammoul et al., 2016; Paterson et al., 2014). Rather than being directly pathogenic, it is hypothesised that the antibodies in the low-positive VGKC cases may result from neuronal damage, such as in association with multiple sclerosis, amyotrophic lateral sclerosis or Creutzfeldt–Jakob disease, or may indicate non-neuronal autoimmunity (Fujita et al., 2012; Huda et al., 2015; Jammoul et al., 2016; Lang et al., 2017). In addition, VGKC antibodies may be an oncogenic marker, with higher than expected rates of malignancy seen, even in low-positive cases scanning (Jammoul et al., 2016; Klein et al., 2013; Paterson et al., 2014). No low-positive VGKC case in this study had evidence of neurological illness or malignancy, although this cohort is significantly younger than other neurological VGKC cohorts described, but two cases did have a past history of non-neurological autoimmunity (Pozo-Rosich et al., 2003; Tan et al., 2008). Low-positive VGKC antibodies may also be found in up to 5% of healthy individuals with no pathogenic association (Dahm et al., 2014; Jammoul et al., 2016; Paterson et al., 2014; Vincent et al., 2004).
Cases with low-positive or negative VGKC testing may still have positive LGi1 or CASPR2 antibodies (Klein et al., 2013; Paterson et al., 2014; Van Sonderen et al., 2016). As with the case described in this study, neurological deterioration is again usually overt but may be historical, given antibodies have been shown to be persistent in the serum for up to 2 years post resolution of clinical symptoms (Finke et al., 2017). The relevance of VGKC antibody positivity in the absence of LGi1 and CASPR2 antibodies has been increasingly debated to the point of recent recommendations to stop VGKC antibody testing (Lang et al., 2017; Michael et al., 2020). This may have pathology service implications given the difference in the scalability of using radioimmune assay testing for VGKC antibodies, as compared to cell-based immunoassay with manual reading by a skilled operator, that is required for testing LGi1 and CASPR2 antibodies. However, as with the VGKC negative cases in this study, LGi1 and CASPR2 antibodies are already tested on the same immunoassay as the anti-NMDA receptor antibody test, which is currently recommended for all first-episode psychosis presentations (Galletly et al., 2016).
VGKC antibody testing, used as a screening tool, in the absence of suggestive clinical encephalitic presentations, may be associated with unnecessary invasive investigations, as well as the potential for delayed psychiatric diagnosis and treatment, with subsequent individual, financial and resource implications. The average time to discharge the low-positive VGKC cases in this study was relatively high in comparison to other Australian studies looking at primary psychiatric admissions (Systema et al., 2002; Wade et al., 2006; Zhang et al., 2011). An alternative hypothesis is that the low-positive VGKC group has a greater severity of illness or resistance to treatment. There is emerging evidence that systemic pro-inflammatory processes are associated with severity of psychosis and other psychiatric symptoms (Fraguas et al., 2019; Köhler-Forsberg et al., 2017; Miller et al., 2011).
The findings from this study have several possible limitations. Due to the retrospective nature of the study and exclusion of paediatric testing, selection and informational bias may result. Antibody tests that were performed privately were also excluded, and it is not possible to determine the number of adult private cases which were tested in the context of psychiatric symptoms. However, it should be noted that cases with encephalitic symptoms would likely be transferred and re-tested in the public healthcare system. There were a small number of positive cases overall and paraclinical testing was not performed on all low-positive cases, potentially limiting generalisability of the results. The majority of psychiatric patients (99.6%) tested for VGKC did not have a positive result and clinical comparison was not made with these cases; thus, caution should be maintained when applying the findings to a broader psychiatric cohort.
The prevalence of VGKC antibody-associated autoimmune encephalitis in a statewide account of public psychiatric services was very low and identification through clinical symptoms was unchallenging. No low-positive VGKC case developed encephalitic features and all retained a primary psychiatric diagnosis on longitudinal review. Further review, through prospective studies, of the effectiveness and cost-benefit of universal VGKC antibody screening in first-episode psychosis is warranted, with consideration of the value of VGKC antibody testing in the absence of LGi1 or CASPR2 antibodies. Accurate early identification of autoimmune limbic encephalitis is crucial, but this does need to be balanced with the understanding that there may be personal and health service consequences associated with low pre-test probability screening.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.