
Abstract
Objective:
The study investigated factors associated with frequent (admissions), high (total length of stay) or heavy (frequent and high) hospital use, and with ongoing increased hospital use, for mental health conditions in a regional health district.
Methods:
A retrospective population-based study using longitudinal hospital, emergency department and community service use data for people admitted with a mental health condition between 1 January 2012 and 31 December 2016. Multivariate logistic regression models assessed the association of predisposing, enabling and need factors with increased, and ongoing increased, hospital use.
Results:
A total of 5,631 people had at least one mental health admission. Frequent admission was associated with not being married (odds ratio = 2.3, 95% confidence interval = [1.5, 3.3]), no private hospital insurance (odds ratio = 2.2, 95% confidence interval = [1.2, 3.8]), previous mental health service use (community, emergency department, lengthy admissions) and a history of a substance use disorder, childhood trauma, self-harm or chronic obstructive pulmonary disease. High and heavy hospital use was associated with marital status, hospital insurance, admission for schizophrenia, previous mental health service use and a history of self-harm. Ongoing frequent use was less likely among those aged 65 and older (odds ratio = 0.2, 95% confidence interval = [0.1, 1.0]) but more likely among those with a history of depression (odds ratio = 2.2, 95% confidence interval = [1.1, 4.4]). Ongoing high use was also associated with admissions for schizophrenia and a history of self-harm.
Conclusion:
Interventions targeted at younger people hospitalised with schizophrenia, a history of depression or self-harm, particularly with evidence of social and or health disadvantage, should be considered to improve long-term consumer and health system outcomes. These data can support policymakers to better understand the context and need for improvements in stepped or staged care for people frequently using inpatient mental health care.
Introduction
Mental disorders are a significant and increasing public health problem in Australia, with adverse personal, social and economic outcomes. The prevalence of mental or behavioural disorders increased from 17.5% in 2014–2015 to 20.1% in 2017–2018 (Australian Bureau of Statistics (ABS), 2019). Mental disorders not only have adverse consequences for people but also come at a significant personal cost (i.e. social isolation, work productivity and financial loss) for their carers (Hayes et al., 2015). Almost AUD$10 billion was spent on mental health-related services in Australia in 2017–2018, including AUD$2.6 billion on public inpatient hospital services and a further AUD$2.3 billion on community mental health care (Australian Institute of Health and Welfare (AIHW), 2019).
Based on the complexity and severity of the mental health condition and the associated need for care, people may use health services across community, emergency department (ED) and inpatient care settings. In 2017–2018, there were 42,992 care episodes for people admitted with a principal or additional mental disorder diagnosis in specialised mental health inpatient units in New South Wales (NSW) public hospitals, with overnight stays for the majority of people (91%) (Bureau of Health Information (BHI), 2019). The most common principal or additional diagnoses in specialised mental health inpatient units were psychotic disorders (35%) and mood disorders (21%). Public mental health service contacts have increased in community and inpatient settings in Australia in the 5 years to 2017-18, by 0.7% per year in the community setting (averaging 22 contacts per year) and more rapidly by 3.5% per year in overnight admissions (averaging one overnight admission per year). The average length of stay (LOS) increased from 12.7 days in 2016–2017 to 14 days in 2017–2018. People experiencing a severe mental health episode often attend the ED and are potentially admitted to hospital because of a lack of after-hour community-based alternatives (BHI, 2019). Western Australian results from a 2019 national snapshot survey completed by inpatient nurse managers in acute mental health wards showed that 27% of people may be more appropriately cared for in non-inpatient settings if services such as community-based residential care with mental health support were available (Government of Western Australia Mental Health Commission, 2019).
People with a mental health condition have higher rates of physical comorbidities than people without mental health conditions, and many also have a comorbid mental health condition (The Royal Australian & New Zealand College of Psychiatrists (RANZCP), 2016). In 2007, 11.7% of people with a mental health condition in the previous 12 months also reported a comorbid physical condition (ABS, 2008). People admitted for a mental health diagnosis often have significant physical needs which may not be addressed in the admission. For example, among people hospitalised with psychoactive substance use disorders, 64.9% of readmissions were for the same condition, but 22.3% were for chronic obstructive pulmonary disease (COPD) and 9.6% for congestive heart failure (Westley-Wise et al., 2020).
People with a mental health and comorbid physical condition make more continuous use of mental health services compared to those without physical comorbidity (Harber-Aschan et al., 2019). A challenge for the health system is providing coordinated and appropriate levels of support to people who have severe and persistent mental health needs (Whiteford et al., 2017). Interventions which decrease long-term patterns of fragmented inpatient and community care associated with both mental and physical conditions are needed to improve both consumer and health system outcomes (Harris et al., 2018). Ensuring continuity of care is becoming even more critical in the context of an ageing population and increasing prevalence of mental disorders, putting pressure on EDs and hospital beds.
Mental disorders can develop from a complex interaction of individual and contextual factors. Many studies conceptualise these factors using Andersen’s health care utilisation model (Roberts et al., 2018). This model groups predictors of health service use into (1) predisposing factors, such as sociodemographic characteristics and attitudes and beliefs that influence the selection of health services; (2) enabling factors that facilitate access to health services, such as health insurance and social support; and (3) need for care factors, which include evaluated needs (clinical diagnosis) and perceived needs (individual’s self-assessment of health status) (Andersen, 1995). Evidence of an association between predisposing factors (gender, ethnicity, education and marital status) and mental health service use is inconsistent (Roberts et al., 2018). Organisational measures including health system factors (e.g. availability and accessibility of services) are enabling factors, but are under-researched (Andersen, 1995; Roberts et al., 2018; van Orden et al., 2017). Evidence of an association between mental health service use and other enabling factors like employment, health insurance, income and rurality is inconsistent (Roberts et al., 2018). Need factors such as self-evaluated health status, duration of symptoms and comorbid mental disorders are consistently associated with service use (Roberts et al., 2018).
The first aim of this study is to identify predisposing, enabling and need for care factors associated with frequent (admissions), high (total LOS) or heavy (frequent and high) use of inpatient mental health services. Second, we aim to identify which of these factors are associated with ongoing frequent or high use continuing for at least 2 years after an initial 12-month period of increased use.
Methods
Study design and population
This retrospective, population-based study used routinely collected data from the eight hospitals in the Illawarra Shoalhaven Local Health District (ISLHD), including three hospitals with acute mental health units and two with sub-acute mental health units. The catchment population comprises over 400,000 residents across an area of 5,700 km2, covering urban and rural areas. The study population comprised people (aged 18 years and older) who were admitted between 1 January 2012 and 31 December 2016 (reference period) with a mental disorder as the principal diagnosis, within six subgroups of ICD-10-AM 9th edition codes (International Statistical Classification of Diseases and Related Health Problems, 10th revision, Australian Modification, Ninth Edition), Australian Consortium for Classification Development (2015):
Mental and behavioural disorders due to psychoactive substance use (F10–F19);
Schizophrenia, schizotypal and delusional disorders (F20–F29);
Mood (affective) disorders (F30–F39);
Neurotic, stress-related and somatoform disorders (F40–F48);
Behavioural syndromes associated with physiological disturbances and physical factors (F50–F59);
Disorders of adult personality and behaviour (F60–F69).
The factor classification of Andersen’s behavioural model of health services use was the framework of this study (Andersen, 1995).
Data source
Routinely collected data were sourced from the Admitted Patient, ED and Community Mental Health Datasets, accessed from the Illawarra Health Information Platform, a non-identifiable databank established by the ISLHD and University of Wollongong research partnership (Mullan et al., 2019).
The University of Wollongong and ISLHD’s Health and Medical Human Research Ethics Committee approved the establishment of the non-identifiable databank on 14 November 2016 (2016/306) and this research project on 8 June 2018 (2018/222).
Sociodemographic, clinical and service use measures
The longitudinal administrative population-level data enabled us to contrast a range of predisposing, enabling and need factors between temporary (frequent, high and heavy) and ongoing frequent and ongoing high service use. The longitudinal regional perspective allowed us to include the person’s 5-year history of mental and physical conditions across hospitals in the health district, given the long-term course of severe mental and chronic physical conditions.
Predisposing factors included age group (18–24, 25–44, 45–64, 65 and older), sex, preferred language (English, other), marital status (registered and de facto, not married) and socioeconomic status (Socio-Economic Indexes for Areas [SEIFA], Index of Relative Socio-economic Advantage and Disadvantage quintiles; ABS, 2016). Enabling factors were rurality (urban, rural), insurance status (private hospital insurance) and previous mental health service use (admissions, total LOS, ED visits and community contacts). Need factors included the six mental disorder subgroups, based on the principal diagnosis at the index hospitalisation, and a history of specific mental and physical conditions. A history of mental conditions included anxiety with onset specific to childhood (F06.4, F40.8-9, F41.0-3, F41.8-9, F93.0-2); depression including postnatal (F06.33, F20.4, F31.3-5, F32, F33, F34.1, F41.2, F43.2, F53.0); post-traumatic stress disorder (PTSD) (F43.1); substance use disorders excluding tobacco and including personal history of psychoactive substance use disorder (F10-F16, F18, F19, I42.6-7, K29.2, K70.0, K70.3, K70.9, Z50.2-3, Z71.4-5, Z72.1-2, Z86.41-42); self-harm including personal history of self-harm (X60-X84, Y87.0, Z91.5); and childhood trauma including sexual and physical abuse (Z61). Physical conditions were defined as the Charlson Index chronic conditions (Sundararajan et al., 2004), a summary measure predictive of death and readmission (Charlson et al., 1987). The five most common physical conditions in the study population were identified.
Stays at private facilities within the district, and public or private facilities outside the district, were not included.
The proportion of missing data was low, from less than 1% for preferred language and postcode (used to determine SEIFA), 1% for marital status and 2.1% for private hospital insurance. The analyses excluded missing data.
Definitions
A stay was defined as episodes of admitted care with no discharge between, which includes transfers. The study population consisted of people with a mental disorder as principal diagnosis at the index stay (first admission) in the reference period (Figure 1). All further stays with a mental disorder as principal or additional diagnosis in the reference period were used to determine the 12-month moving window of frequent or high service use. People who sustained, secondary to their mental illness, a physical condition requiring admission under a medical team were included in the study if the person had a mental health principal diagnosis. Previously established data-driven thresholds for admissions (frequency) or total LOS (duration) were applied to the person’s first 12-month moving window of frequent or high use (Suesse et al., under review). Frequent use was defined as having six or more admissions in a 12-month moving window. High use was defined as spending 45 or more days in hospital in a 12-month moving window. Heavy use was defined as meeting both frequent and high use thresholds. Ongoing frequent or high hospital use was defined as having a second 12-month moving window of frequent or high use within 2 years of the index window. The study period, including a look-forward and a look-back, comprised 12 years from 1 January 2007 to 31 December 2018. A 1-year look-back determined immediately prior mental health service utilisation, a 2-year look-back the persons’ preferred language, marital and socioeconomic status, and a 5-year look-back persons’ history of health conditions. A 2-year look forward determined ongoing use.
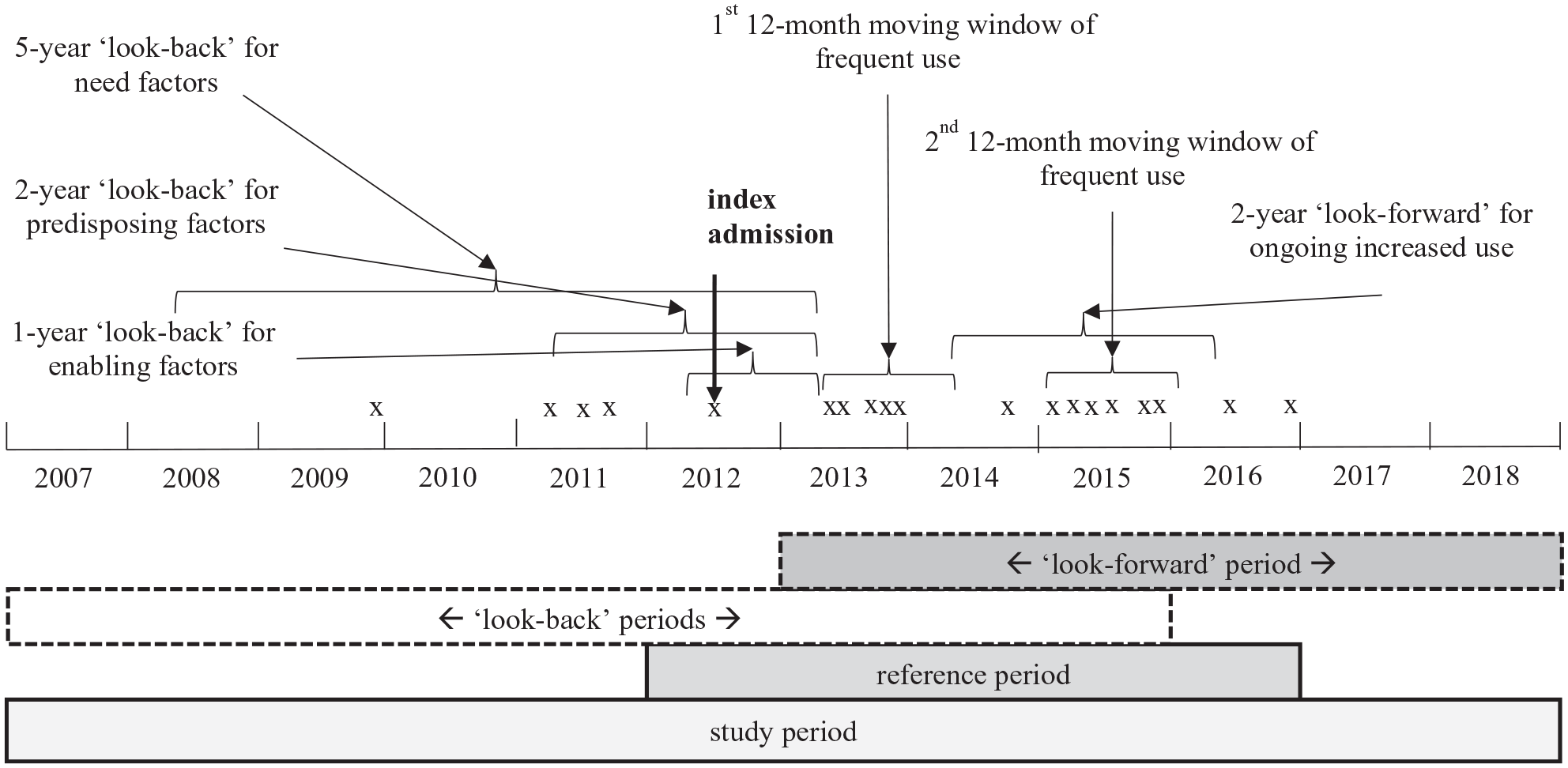
Schematic representation of the 12-month moving window of frequent (admissions) use for people with a mental disorder principal diagnosis at index admission in the reference period including ‘look-back’ and ‘look-forward’ periods before and after the first window.
Statistical analysis
Descriptive analysis was conducted for each cohort of increased use (frequent, high, heavy and ongoing frequent and high) and the study population. Univariate analyses were performed to examine frequency distributions for categorical variables, and means and standard deviations were calculated for discrete variables. Multivariate logistic regression was used to identify factors associated with frequent, high and heavy service use, and ongoing frequent or high service use. Statistical significance was set at 5%. Factors which had non-significant associations in unadjusted models were excluded from the multivariate analyses. Variance inflation factor and tolerance were used to test multicollinearity (Schreiber-Gregory et al., 2017). A sensitivity analysis assessed whether including index mental disorder modified the modelled impact of a person’s disease history. Data were analysed using SAS V.9.4 (SAS Institute Inc., 2013). Multivariate logistic models were fit using PROC LOGISTIC with maximum likelihood estimation.
Results
Sociodemographic, clinical and service use characteristics
A total of 5,631 people in the study population had 15,692 stays with a mental disorder as principal or additional diagnosis. The study population had the highest representation in the 25–44 age group (41.1%), male (51.4%), with English as their preferred language (97.2%), not married (71.6%) and from a medium to a high socioeconomic background (40.8%) (Table 1). A high proportion lived in urban areas (73%) and had no private hospital insurance (85.4%). The most common principal diagnosis at index admission was mood disorder (26%), and a history of substance use disorder (52.8%) or depression (46.7%) was common. About 17.3% of people with a mental health condition presented with a history of a chronic physical condition.
Characteristics of people with a mental health condition having frequent, high and heavy use and ongoing frequent or high use of inpatient mental health services.
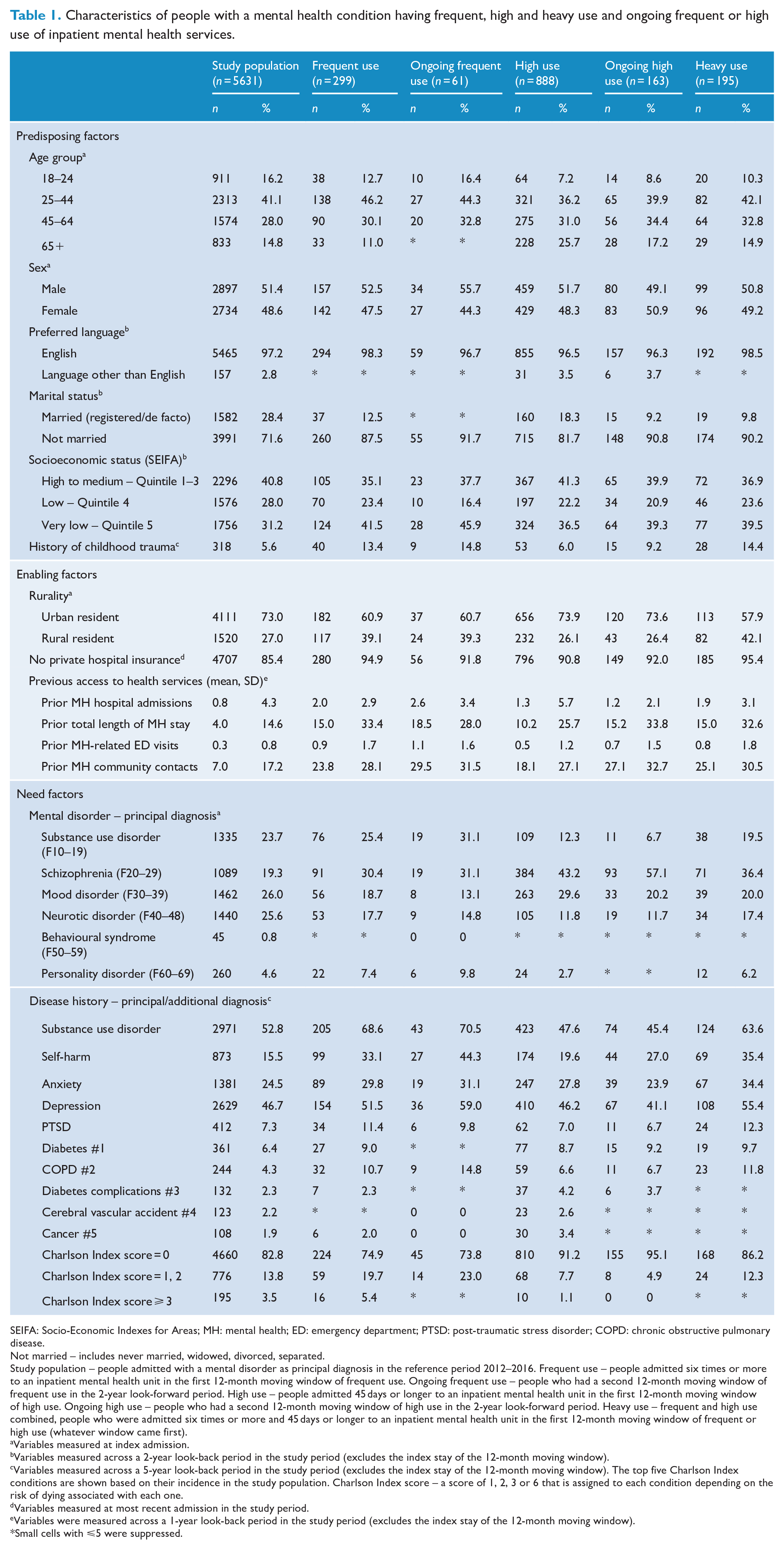
SEIFA: Socio-Economic Indexes for Areas; MH: mental health; ED: emergency department; PTSD: post-traumatic stress disorder; COPD: chronic obstructive pulmonary disease.
Not married – includes never married, widowed, divorced, separated.
Study population – people admitted with a mental disorder as principal diagnosis in the reference period 2012–2016. Frequent use – people admitted six times or more to an inpatient mental health unit in the first 12-month moving window of frequent use. Ongoing frequent use – people who had a second 12-month moving window of frequent use in the 2-year look-forward period. High use – people admitted 45 days or longer to an inpatient mental health unit in the first 12-month moving window of high use. Ongoing high use – people who had a second 12-month moving window of high use in the 2-year look-forward period. Heavy use – frequent and high use combined, people who were admitted six times or more and 45 days or longer to an inpatient mental health unit in the first 12-month moving window of frequent or high use (whatever window came first).
Variables measured at index admission.
Variables measured across a 2-year look-back period in the study period (excludes the index stay of the 12-month moving window).
Variables measured across a 5-year look-back period in the study period (excludes the index stay of the 12-month moving window). The top five Charlson Index conditions are shown based on their incidence in the study population. Charlson Index score – a score of 1, 2, 3 or 6 that is assigned to each condition depending on the risk of dying associated with each one.
Variables measured at most recent admission in the study period.
Variables were measured across a 1-year look-back period in the study period (excludes the index stay of the 12-month moving window).
Small cells with ⩽5 were suppressed.
Just over 5% of people had at least one period of frequent use (six or more admissions, n = 299), 15.0% a period of high use (45 or more days, n = 888) and 3.5% a period of heavy use (six or more admissions and 45 or more days, n = 195) (Figure 2). Most people with frequent, high or heavy use were aged 25–44, with English as their preferred language, not married, urban resident, without private hospital insurance, and their most common diagnosis at index admission was schizophrenia (Table 1).
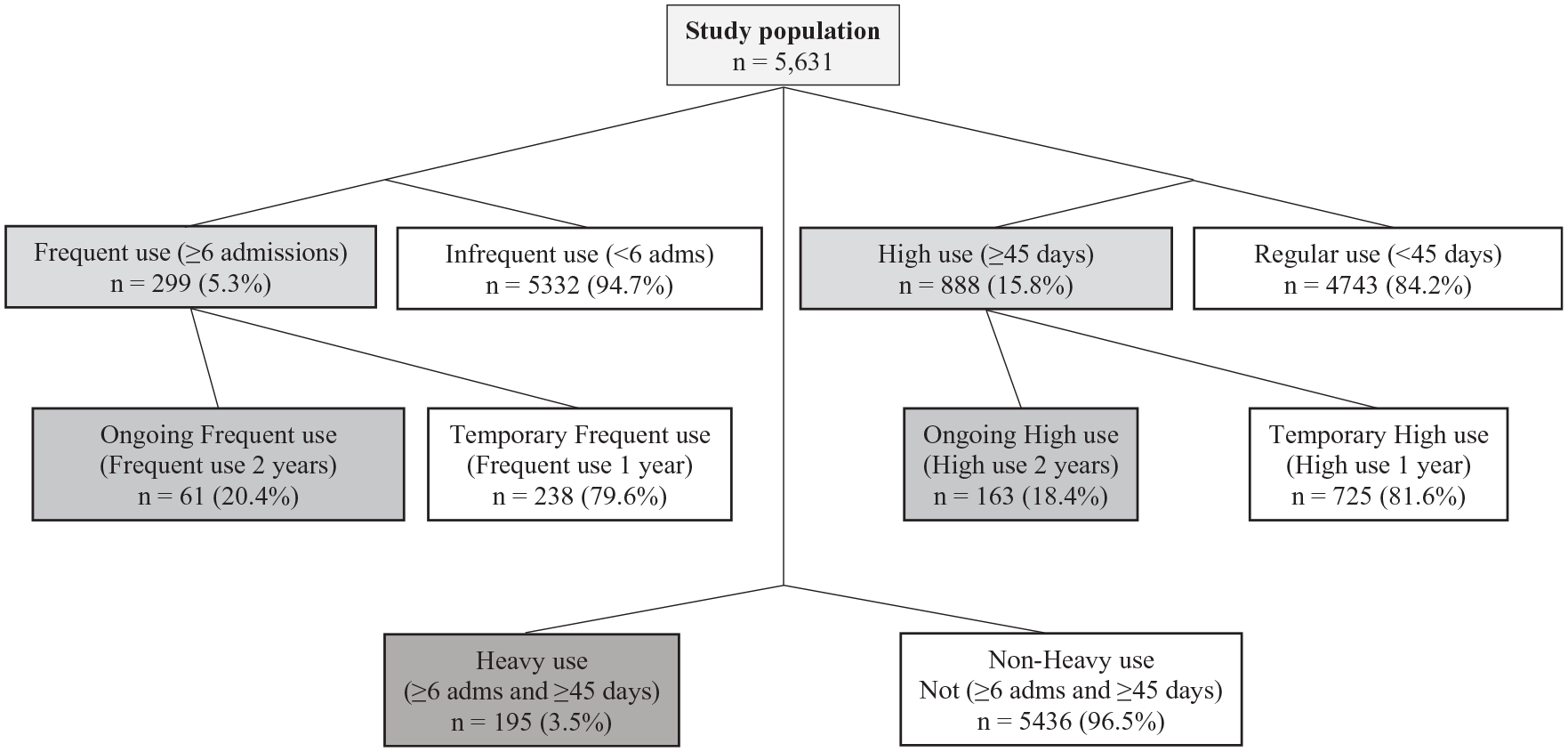
Overview of the study cohorts.
People from a very low socioeconomic background were over-represented among those in all categories of increased use, but particularly among those with ongoing frequent use (45.9%) (Table 1). Just under one-third of people (31.1%) with ongoing frequent use had a principal diagnosis of schizophrenia at index admission, and another 31.1% had a substance use disorder. The proportion of people presenting with a history of substance use disorder was high in the frequent (68.6%), ongoing frequent (70.5%) and heavy use (63.6%) cohorts. A history of substance use disorder was less common among people with high (47.6%) and ongoing high use (45.4%) than observed in those with frequent (68.6%) and ongoing frequent use (70.5%).
People with ongoing frequent use (two periods of frequent use) commonly presented with a history of self-harm (44.3%) or depression (59.0%) (Table 1). Over a quarter of people with ongoing high use (two periods of high use) had a history of self-harm (27.0%) and over a third a history of depression (41.1%). Only about 5% of people with ongoing high use had a history of physical conditions.
Association of frequent, high or heavy service use with predisposing, enabling and need factors
Predisposing factors associated with frequent use were not being married (adjusted odds ratio [AOR] = 2.3, 95% confidence interval [CI] = [1.5, 3.3]) and a history of childhood trauma (AOR = 1.7, 95% CI = [1.1, 2.6]) (Table 2). Enabling factors associated with frequent use were living in rural areas (AOR = 2.2, 95% CI = [1.6, 2.9]), no private hospital insurance (AOR = 2.2, 95% CI = [1.2, 3.8]) and prior mental health-related total LOS, ED visits and community contacts. Need factors associated with frequent use included a history of substance use disorder, self-harm or COPD.
Odds ratios and adjusted odds ratios with associated 95% confidence intervals for predisposing, enabling and need factors associated with frequent, high and heavy use of inpatient mental health services.
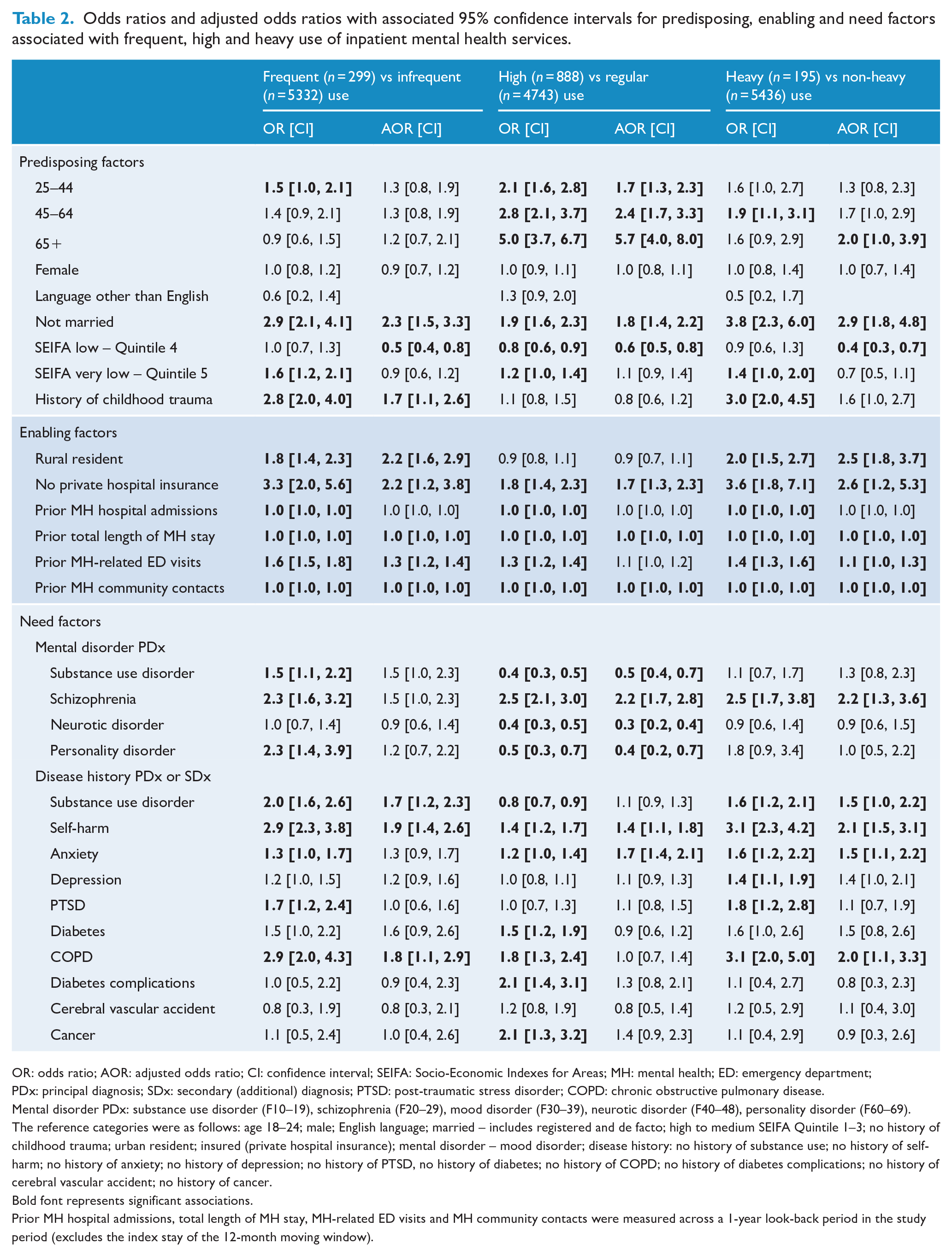
OR: odds ratio; AOR: adjusted odds ratio; CI: confidence interval; SEIFA: Socio-Economic Indexes for Areas; MH: mental health; ED: emergency department; PDx: principal diagnosis; SDx: secondary (additional) diagnosis; PTSD: post-traumatic stress disorder; COPD: chronic obstructive pulmonary disease.
Mental disorder PDx: substance use disorder (F10–19), schizophrenia (F20–29), mood disorder (F30–39), neurotic disorder (F40–48), personality disorder (F60–69).
The reference categories were as follows: age 18–24; male; English language; married – includes registered and de facto; high to medium SEIFA Quintile 1–3; no history of childhood trauma; urban resident; insured (private hospital insurance); mental disorder – mood disorder; disease history: no history of substance use; no history of self-harm; no history of anxiety; no history of depression; no history of PTSD, no history of diabetes; no history of COPD; no history of diabetes complications; no history of cerebral vascular accident; no history of cancer.
Bold font represents significant associations.
Prior MH hospital admissions, total length of MH stay, MH-related ED visits and MH community contacts were measured across a 1-year look-back period in the study period (excludes the index stay of the 12-month moving window).
Predisposing factors associated with high use were older age, in particular those aged 65 and older (AOR = 5.7, 95% CI = [4.0, 8.0]) and not being married (AOR = 1.8, 95% CI = [1.4, 2.2], Table 2). People from socioeconomically disadvantaged areas were less likely to have high service use. Having no private hospital insurance and prior mental health-related total LOS and community contacts were significant enabling factors associated with high use. Compared to those with mood disorders, people with an index admission for schizophrenia were more likely to have high use, and those admitted for substance use disorder, neurotic disorder and personality disorder were less likely to have high use. People with a history of self-harm or anxiety were also more likely to have high use.
Both frequent and long admission (‘heavy use’) were associated with living in rural areas (AOR = 2.5, 95% CI = [1.8, 3.7]) and with prior mental health-related ED visits (AOR = 1.1, 95% CI = [1.0, 1.3]) (Table 2). Heavy use was associated with a schizophrenia diagnosis at index admission and with a history of a substance use disorder, self-harm, anxiety or COPD.
Association of ongoing service use with predisposing, enabling and need factors
A history of depression (AOR = 2.2, 95% CI = [1.1, 4.4]) was associated with ongoing frequent use (Table 3). In contrast to high and heavy use, people aged 65 years or older were less likely to have ongoing frequent use (AOR = 0.2, 95% CI = [0.1, 1.0]). Ongoing high use was associated with not being married (AOR = 2.4, 95% CI = [1.3, 4.3]), schizophrenia at index admission (AOR = 1.8, 95% CI = [1.0, 3.1]) and a history of self-harm (AOR = 1.7, 95% CI = [1.1, 2.7]).
Odds ratios and adjusted odds ratios with associated 95% confidence intervals for predisposing, enabling and need factors associated with ongoing frequent and ongoing high use of inpatient mental health services.
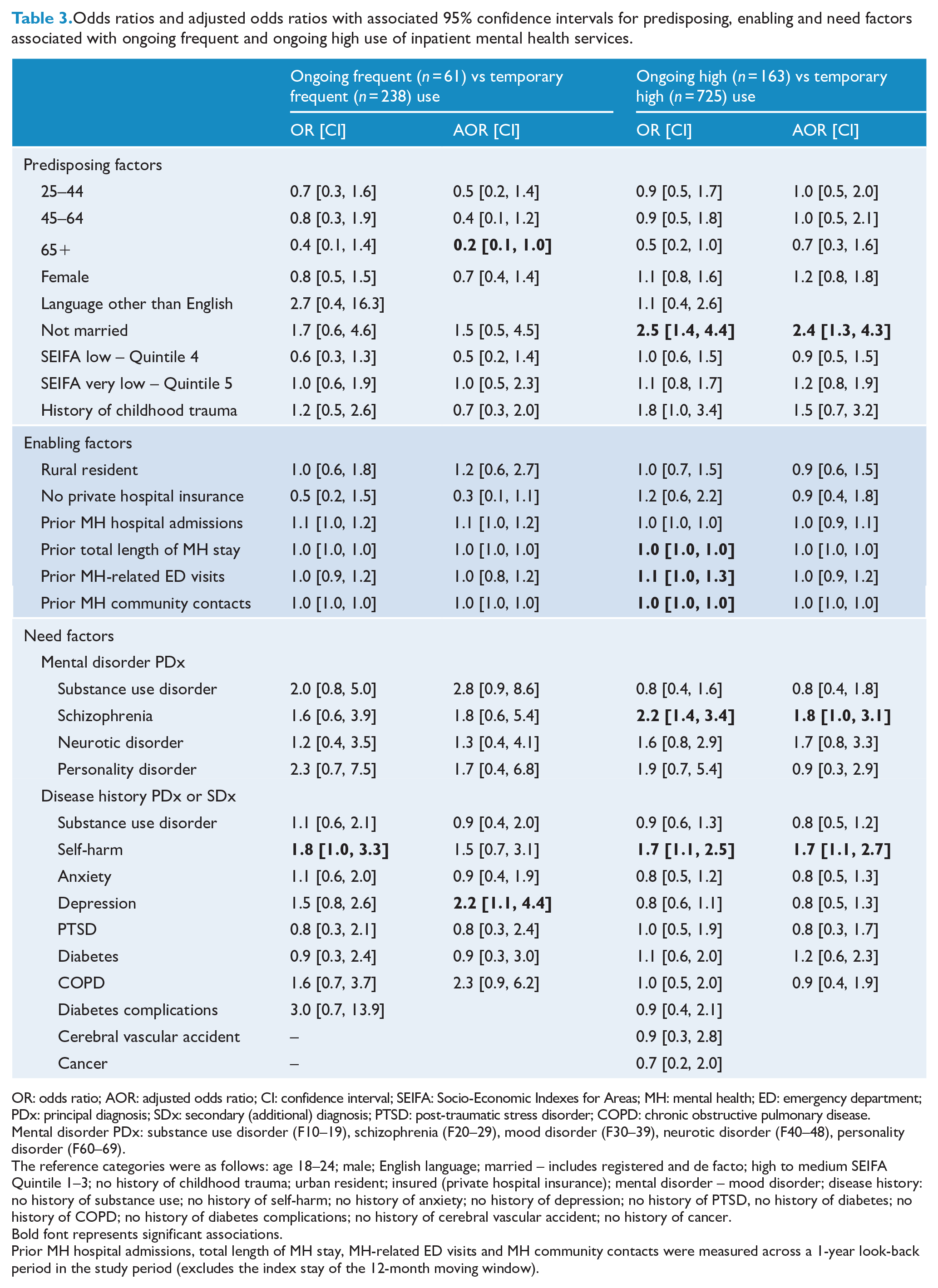
OR: odds ratio; AOR: adjusted odds ratio; CI: confidence interval; SEIFA: Socio-Economic Indexes for Areas; MH: mental health; ED: emergency department; PDx: principal diagnosis; SDx: secondary (additional) diagnosis; PTSD: post-traumatic stress disorder; COPD: chronic obstructive pulmonary disease.
Mental disorder PDx: substance use disorder (F10–19), schizophrenia (F20–29), mood disorder (F30–39), neurotic disorder (F40–48), personality disorder (F60–69).
The reference categories were as follows: age 18–24; male; English language; married – includes registered and de facto; high to medium SEIFA Quintile 1–3; no history of childhood trauma; urban resident; insured (private hospital insurance); mental disorder – mood disorder; disease history: no history of substance use; no history of self-harm; no history of anxiety; no history of depression; no history of PTSD, no history of diabetes; no history of COPD; no history of diabetes complications; no history of cerebral vascular accident; no history of cancer.
Bold font represents significant associations.
Prior MH hospital admissions, total length of MH stay, MH-related ED visits and MH community contacts were measured across a 1-year look-back period in the study period (excludes the index stay of the 12-month moving window).
Supplementary Tables 1 and 2 provide results of a sensitivity analysis excluding mental disorder principal diagnoses from the model. This change did not substantially affect the associations of mental disorder history with any outcome. Supplementary Table 3 shows the frequencies of frequent, high and heavy use of people admitted with a mental health condition as a principal diagnosis and a history of mental or physical conditions.
Discussion
This study found that an initial schizophrenia diagnosis or a history of self-harm as need factors were strongly associated with temporary high as well as ongoing high inpatient mental health service use. About 43% of people with prolonged admissions had an initial schizophrenia diagnosis, and about 18% of high use inpatients had ongoing prolonged admissions in the subsequent 2 years. This finding is consistent with a longitudinal study of adults in the United States on recovery trajectories from severe mental disorders including schizophrenia which found that 24% of people had persistently high mental and physical health-related problems and high mental health service use over 2 years (Green et al., 2013). People with a schizophrenia diagnosis are considered to have a severe illness, especially if the person has been significantly impacted by past-year mental health-related inpatient admissions (Whiteford et al., 2017). Schizophrenia severity has previously been associated with longer LOS (Newman et al., 2018). The study finding that a history of self-harm was associated with ongoing high inpatient mental health service use is consistent with evidence that self-harm is a known risk factor for further self-harm (Madge et al., 2008). Other risk factors for self-harm include substance use, psychosis, mood, anxiety and personality disorder, medical conditions and social problems (Carter et al., 2016).
In this study, almost 60% of people with ongoing frequent inpatient mental health service use had a history of depression as an associated need factor. Depression is a recurrent and severe mood disorder. Comorbid depression in people with COPD has been associated with longer hospitalisations (Ng et al., 2007). We found a history of COPD in people admitted with a mental health condition was associated with temporary frequent and prolonged admissions. There is existing evidence from longitudinal studies that depression and anxiety increased the risk of COPD exacerbation in adult populations, and inversely, that COPD increased the risk of developing depression (Atlantis et al., 2013). Meeting the care needs for mental and physical conditions through more integrated support improves the quality of life for both; however, care for mental and physical multimorbidity has been uncoordinated and ineffective (Naylor et al., 2012).
Age and marital status were predisposing factors which influenced temporary and ongoing increased inpatient mental health service use. People aged 65 and older had increased odds of having high and heavy service use, but being 65 years and older significantly decreased the odds for ongoing frequent use. A Canadian population-based study also found that older adults with mental health conditions had significantly higher inpatient service use (prolonged hospitalisations, higher readmission rates and increased costs) than those without a mental disorder (Adams et al., 2015). They found that mental disorders were often overlooked or misdiagnosed in older adults. Hence, increased resource use of older adults with mental health conditions could include inadequate age-specific assessment, diagnosis and treatment, inefficient in-hospital and discharge processes, or insufficient community resources. Since medical comorbidities increase with age, an emphasis on effectively managing mental health issues in younger people to prevent the development of chronic mental or physical illness later in life is warranted (Harris et al., 2018). Of overnight admitted acute care episodes in 2017–2018, those for people aged 15–24 years had the highest growth rate of 23% (BHI, 2019). This study found people with a mental disorder who were not married had a temporary increased frequency of admission and ongoing long admissions, perhaps due to a lack of physical, emotional and financial support, and consequently reduced rates of insurance and difficulty accessing care. People who have never been married have a higher prevalence of mental disorders (ABS, 2008).
A history of childhood trauma as a predisposing factor was associated with temporary frequent hospital admissions in this study. Childhood trauma poses a significant risk for later development of severe mental and physical illnesses, e.g., substance use, personality, eating and autoimmune disorders and irritable bowel syndrome (Kendler et al., 2000; Mulvihill, 2005). People with depression or anxiety who experienced childhood trauma have increased risk of recurrent and persistent episodes, suicidal ideation and developing chronic depression later in life (Devi et al., 2019; Kendler et al., 2000). Another Australian study found that exposure to childhood trauma was predictive of mental health visits by adults to general practitioners (Mills et al., 2012).
This study found associations between enabling factors such as insurance, rurality and prior mental health service use and temporary frequent, high and heavy inpatient mental health service use, while previous evidence has been inconsistent (Roberts et al., 2018). Unlike need and predisposing factors, none of the enabling factors in this study was associated with ongoing increased inpatient mental health service use. Rural residents with mental health conditions frequently accessed inpatient care and also had prolonged admissions in this study. The Australian study by Mills et al. (2012), however, found that rural living was associated with lower odds of mental health-related consultations with mental health specialists and other health service professionals. Therefore, rural residents might not have received the required level of care in the community and subsequently required acute care. In this study, people with mental health conditions without private hospital insurance had temporary frequent, high and heavy use of public inpatient services. People with private hospital insurance might be less socioeconomically disadvantaged and instead transfer to or seek private hospital or community care. Prior mental health-related ED visits increased the odds for frequent service use, which is consistent with other evidence that previous use of mental health services (i.e. for depression) is associated with subsequent use (Gwynn et al., 2008; Roberts et al., 2018).
Limitations
One of the limitations is that the measures of inpatient mental health service use, i.e., the number of admissions and total LOS used to define frequent, high and heavy use, reflect the access to these services not the actual need for care. This study is based on a specific regional population and given that there are different policy and practice across jurisdictions, the results may not be generalisable. The sample may consist of a large proportion of people with serious mental health conditions; however, a measure of illness severity was not available. As a consequence, the findings might not generalise to other mental health patient populations. The number of people who had ongoing frequent or ongoing high use was relatively small and thus there may be undetected true associations with predisposing, enabling and need factors. This study did not assess the coexistence of mental-mental or mental-physical conditions at the person’s initial admission. Other limitations arise from patient information not routinely or poorly recorded in administrative datasets. For instance, data on a history of child abuse, neglect and sexual assault or alcohol abuse, which are known risk factors for mental health service use, might be underestimated. Due to changes in reporting rules and processes for community mental health data, the community dataset might underestimate service contacts earlier in the study period. It was not possible with the current dataset to distinguish services provided in hospital outpatient clinics versus those provided in community settings to understand the extent to which mental health resources are directed towards hospital-based care over other care types. Another limitation is that data on non-government organisations were also not available.
Implications for research, clinical care and health service delivery
The findings in this study align with some areas identified in the regional mental health and suicide prevention plan (COORDINARE – South Eastern NSW, 2018). These include a need to improve care for people with mental health needs (including self-harm) and mental and physical comorbidity, previous childhood trauma and support for rural residents. Current NSW policy recommends ‘holistic, person-centred’, ‘safe, high-quality’ and ‘connected care’ for people with mental health conditions with continuity, better integration and improved equity of access (NSW Ministry of Health, 2018). However, there is an inequitable distribution of services with a limited workforce in some parts of the study region, and service availability does not match population needs, especially in rural areas (COORDINARE – South Eastern NSW, 2018). Further areas of concern identified at the regional level by consumers, carers and service providers included fragmentation of service delivery and poor transitions, services and pathways not focused on the spectrum of consumer needs, treatment not focused on prevention or early intervention, and poor mental health and physical health outcomes. A recently established mental health service in the rural area of the study region, ‘MIND the GaP initiative’, aims to improve mental health service delivery and outcomes in areas of suicide prevention, traumatic stress responses and community resilience (MIND the GaP, 2018). Although the opening of this service coincided with the end of the study period, it aims to serve as a ‘testbed for a translatable regional model of mental health and wellbeing’. There is an increasing awareness in Australia that a general practitioner can effectively coordinate recovery-oriented and trauma-focused care for people with previous childhood trauma if local services are limited (Su and Stone, 2020).
The extent to which hospital avoidance is useful or desirable has not been clearly defined in ‘The Fifth National Mental Health and Suicide Prevention Plan’ (Australian Government Department of Health, 2017); however, this study helps to illuminate for whom hospital avoidance could occur. Since not all hospitalisations are avoidable and acute inpatient mental health beds are still needed, some people with persistent, complex and severe mental health conditions would benefit from increased specialised community-based treatment and residential care but not inpatient care for extended periods (Productivity Commission, 2019). Timely access (after-hour) to a team of service providers matching complex care needs would be in line with the nationally adopted stepped model of mental health care (Productivity Commission, 2019). New approaches are proposed to engage the community sector to work together with other services in organising mental health care in the community to support consumers. This includes multidisciplinary community mental health teams comprising social workers, psychologists, peer workers, occupational therapists, nurses and medical professionals (Rosenberg, 2015).
Understanding the characteristics of people with increased inpatient service use is an important first step to be able to design alternatives that improve support for care needs in the community instead of being overly reliant on hospital-based care. Rather than assuming that a community-hospital interface will reduce frequent admissions and prolonged hospitalisations, future research could focus on a community-hospital interface redesign to investigate whether an improved alternative approach of integrated community-hospital care improves outcomes for current users of inpatient services compared to standard care. Care pathways of specific subgroups (e.g. people with schizophrenia, previous self-harm or mental and physical multimorbidity) can also be investigated at the community-hospital interface using hospital and community data linkage.
Further research using cross-sector linkage could investigate non-clinical aspects of people’s circumstances, e.g., disability, ageing, homelessness and social housing, to better understand the reasons for the ongoing need of inpatient mental health care. A retrospective thematic analysis by Meng et al. (2017) determined frequent ED use of people with primary mental health problems was associated with substance use/abuse (alcohol or illicit drugs), mood and anxiety disorders, social and personal stressors with or without mental disorders, and cognitive impairment with concurrent mental disorders. Linkage with datasets from the NSW Government Family and Community Services, e.g., Ageing, Disability and Home Care, Specialist Homelessness Services, and Social Housing, would help to uncover patterns in people’s health trajectory and better respond to their complex needs.
Supplemental Material
sj-pdf-1-anp-10.1177_0004867420976848 – Supplemental material for Predisposing, enabling and need factors associated with increased use and ongoing increased use of inpatient mental health care: A population-based longitudinal study
Supplemental material, sj-pdf-1-anp-10.1177_0004867420976848 for Predisposing, enabling and need factors associated with increased use and ongoing increased use of inpatient mental health care: A population-based longitudinal study by Bianca Suesse, Luise Lago, Victoria Westley-Wise, Jose Cuenca and Nagesh Pai in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors thank Brendan McAlister and David Webster for assistance with accessing data and Brendan McAlister, Rachel Condon, Michelle Hudoba, Nicola Palmer and Julie Hider for assistance with interpretation of the community data. Patients and the public were not involved in the design or conduct of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the Illawarra Health Information Platform (IHIP) research partnership established between the Illawarra Shoalhaven Local Health District (ISLHD) and the University of Wollongong, with ISLHD providing funding support and the data used in this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.