
Abstract
Inpatient admissions to mental health services have long been a focus for politicians, policy-makers, administrators, and insurers responsible for health budgets [1]. Inpatient admissions are costly [2], [3], have been decreasing in duration over past decades [4], but remain a necessary component in a comprehensive mental health service [5–7]. Thus, stakeholders strive to ensure that inpatient admissions are used effectively [8–10] and efficiently [2], [3]. As occupancy levels continue to increase and the pressure on existing beds in mental health continues to rise, finding ways to manage existing resources is a high priority for clinicians, administrators, and policy makers. In achieving this difficult task of delivering cost-effective mental health services, there are many systemic pressures acting upon psychiatrists (e.g. government funding decisions, insurer requirements, etc.) that are largely out of an individual's control. Nevertheless, there are many components over which individual doctors can exert influence. One such component is the length of stay during an inpatient admission. Within that sphere of influence, psychiatrists are continuing to endeavour to make decisions in the best interests of patients. One way to make these decisions most effectively is by recruiting the support of colleagues in the form of second opinions and review panels. Therefore, we decided to develop a methodology to inform a review schedule of inpatient length of hospital stay. In doing so, we continued to bear two important considerations in mind.
First, length of hospital stay is not normally distributed and therefore parametric statistics are typically inappropriate and many descriptive statistics are potentially misleading [11], [12]. Length of stay is governed by a hazard-based process and tends to follow a negative exponential function with most patients being discharged after short periods of time, while ever smaller numbers stay for longer periods of time. For example, Stevens and colleagues [12] found that an exponential function was able to fit their length of hospital stay data well. Thus, it was important to take the nature of the distribution into account when examining the data.
Second, to identify a maximally effective time for review, it was necessary to identify occasions when the conditional probability of discharge was decreasing rather than increasing. That is, there is little value in routinely obtaining a second opinion at a time when many inpatients are likely to be discharged; since many patients being reviewed will be likely to leave hospital in the normal course of events. To achieve the goal of measuring the conditional probability of discharge, we transformed the length of stay data from the percentage of the cohort of patients in hospital for a given length of stay (i.e. a typical survival function), to the conditional probability that those patients remaining in hospital on a given day will be discharged in the following 7 days. Thus, as time increased, there was a ‘sliding window’ that allowed calculation of the probability of discharge within a relatively short period of time of those patients still in hospital. The period of 7 days was selected arbitrarily as a sufficiently short period of time that a doctor might be interested to know about. The probabilities were then calculated for each day and the resulting curve presented to the treating doctors to enable them to decide when were the best times for them to implement different forms of review as they sought to be in the patients' best interest. The remainder of the paper will describe the methodology and its implementation.
Method
Participants were 1227 consecutive inpatient admissions to a private psychiatric hospital in the 2002 calendar year. They had a mean age of 41.6 (SD = 16.7), 71% were female, and for 50% of the sample the current inpatient admission was either their first or second contact with the hospital, where a prior contact could be inpatient or daypatient treatment. The length of hospital stay was calculated by subtracting the date of discharge from the date of admission, even if discharge date was outside the calendar year. Each patient was diagnosed by their consultant psychiatrist according to ICD-10-AM criteria [13]. Most patients had primary diagnoses of affective (63.8), neurotic (19.1), substance use (6.1%) disorders or schizophrenia (5.0%). In addition, 28.3% had a medical condition and the most common comorbid psychiatric disorders were neurotic (18.1%), affective (10.6%), and substance use (7.8%) disorders.
Results
Firstly, it was necessary to examine the distribution of the length of hospital stay. As expected, the survival curve showed that as time increased the probability of being in hospital decreased at a decreasing rate (Fig. 1). The median length of stay was 12 days.
A survival curve illustrating the probability of 1227 inpatient admissions being in hospital at a given length of stay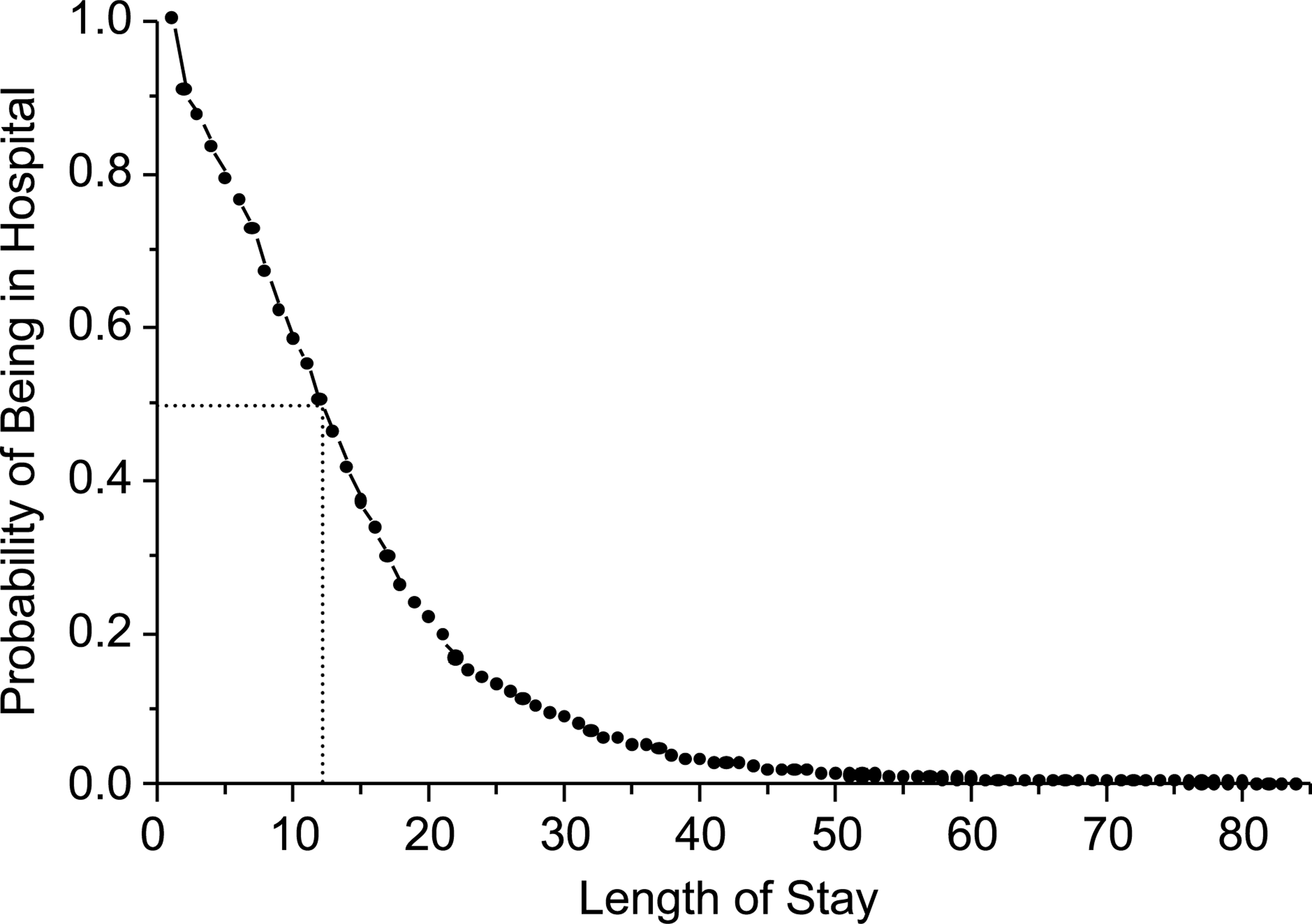
Secondly, we calculated the conditional probability of discharge. This was achieved by using the data generated to produce the survival function displayed in Fig. 1. For each length of stay the number of patients leaving hospital in the next 7 days was divided by the number of patients in hospital at that day. For example, of the 1227 inpatients patients in hospital on day n, 115 were discharged on day n + 1, 40 were discharged on day n + 2, 48 on day n + 3, and 52, 33, 47, and 70 on the subsequent days. Therefore, the probability of being discharged in the following week (115 + 40 + 48 + 52 + 33 + 47 + 70)/1277 was 0.33 (or 33%). (The relevant data can be generated using areadily available spreadsheet [e.g. Excel] and graph [e.g. Prism] packages. However, if using SPSS, the text output from a survival analysis can be imported into a spreadsheet program for easy calculations and the values in the column titled ‘number exposed to risk’ can be used to generate the denominator and the numerator can be derived from the next seven row values in the column titled ‘number of terminal events’.) The resulting probabilities (represented as percentages of patients being discharged) are displayed in Fig. 2 for each length of stay. (Since the number of patients becomes increasingly small, the variability in the data beyond a certain point becomes unstable and hard to interpret. Therefore, the lengths of stay have been truncated at 70 days.) For ease of interpretation the data have been smoothed and the resulting function overlaid on the raw data. Examining the graph it is apparent that for the first 2 weeks, the probability of being discharged in the next 7 days is increasing from a third to a half of remaining patients. However, after 2 weeks, the probability of discharge declines and starts to climb once more for the patients who remain inpatients after 3 weeks. By 1 month the probability of discharge remains stable at around 40% and then drops markedly once a length of stay exceeds 50 days. Thus, one might decide to consider some form of review at the occasions when the curve is declining (i.e. 2 weeks, 1 month, or just before 2 months).
The raw (small circles) and smoothed (large circles) data depicting the conditional probability of being discharged from hospital in the following seven days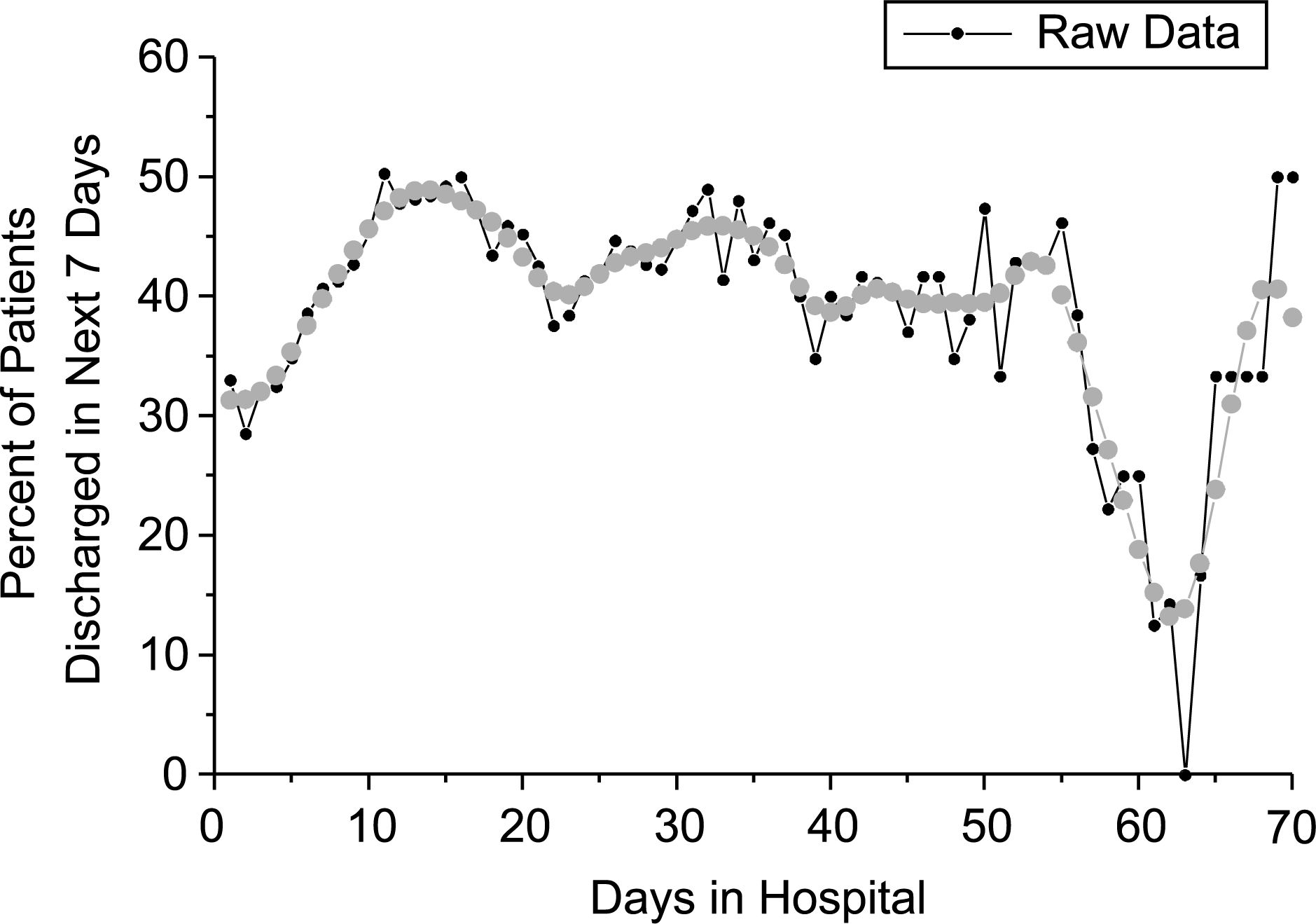
Discussion
The psychiatric length of stay data exhibited the form of a simple decaying exponential function, which is consistent with suggestion that hazard-based processes are responsible for the shape of the distribution. Despite the overall ‘decay’ evident in the data when plotted over time, calculating the conditional probability of discharge at each length of stay revealed that the probability of discharge varied with length of stay. Specifically, the probability of discharge rose rapidly within the first few days of an inpatient stay but declined at around 2 weeks, 1 month and 2 months. Therefore, these three points in time were potential options to review length of stay. These data were then presented to hospital management and psychiatrists associated with the clinic so that they could evaluate existing practices in light of the data.
By way of illustration, these data were considered by psychiatrists associated with Perth Clinic and they decided to modify existing practices so that after 20 days of stay the referring doctor receives a letter from his or her colleagues on the Clinic's Medical Advisory Committee requesting a second opinion. If the patient is still in hospital after 40 days the doctor presents the patient's current clinical situation and the second opinion to a committee comprising three psychiatrists. The purpose of the two forms of review is to provide peer support in the psychiatric decision making and informal feedback indicates that newer psychiatrists are especially appreciative of this support when weighing up the benefits and risks of discharge at a given point in time. These time points were selected by the Medical Advisory Committee not only based upon the data reported in the present paper, but they were also informed by psychiatrists' clinical judgements. The chief goal of implementing a new system was not a change in length of stay of patient outcome per se, but rather a more efficient use of a psychiatrists' time in that doctors were reviewing each patient's stay in hospital when the probability of discharge was relatively low. Notwithstanding, implementation of the system of reviews has been associated with a reduction in length of hospital stay. In 2003, the median length of stay was 11.5 days (mean = 13.8; comparable to the median of 12 days in 2002) which declined to a median of 10 days (mean = 12.7; F1,2256 = 5.782; p < 0.05) in January to July 2004. However, in the absence of a control condition it is not possible to claim that the implementation of the review system caused the recent reduction in length of stay.
Having described the method of analysis and the decision-making process that followed a series of caveats must be added. First, it is important not to assume prescription from description. Although the methodology applied in the present circumstances is generalisable to other settings, the timings of review are not. The particular timings reflect historical data from Perth Clinic and the numbers of patients per length of stay will be dependent on different factors in different hospitals. Furthermore, length of stay is a dynamic process and the implementation of a different review process could reasonably be expected to change the patterns of discharge. For instance, randomised controlled trials (typically from the US) identify that at least 20% of inpatients with mental health problems could be treated equally or better in daypatient settings [14]. Therefore, it may be possible to more easily identify patients who could be better treated as daypatients or to consider if a particular treatment option is better delivered as a daypatient (see [9]). If clinical decisions altered the probability of discharge, then the timing of reviews might be reconsidered in light of the changes. Second, the results do not provide any information about the optimal length of hospital stay or the reasons for or against discharge. Our approach took for granted that doctors and the review teams made decisions informed by a patient's clinical data, but we assumed that they might benefit from specific information about the best way to time these decisions taking into account the probability of discharge. Third, it is not possible to infer from a decreasing conditional probability of discharge that patients are remaining in hospital shorter or longer than necessary. The data describe what occurred and the pattern is consistent with three ‘types’ of admissions; namely those who might benefit from a relatively short stay (e.g. depression being treated with ECT), those who may require a moderate time in hospital, and those who may call for more continued or sustained care (e.g. anorexia nervosa complicated by comorbid diagnoses). The data cannot prescribe an appropriate length of stay, since these decisions need to be informed by clinical outcomes. Finally, although the methodology described is readily applicable to all hospitals, the degree to which the patterns of discharge are comparable between settings (e.g. private versus acute public services) and across time is not evident from the present data. Replication in different samples is the only way to address these issues.
In conclusion, inpatient stay is an important component of a comprehensive mental health service. However, the costs associated with inpatient care place a burden of responsibility on treating doctors to ensure that resources are being used effectively and efficiently. By examining the conditional probability of discharge, it is possible to inform decisions about the most effective times to schedule reviews (e.g. second opinion, peer review). In so doing, doctors may be able to continue to use their time efficiently in the effective management of patients as they weigh up the competing pressures of patient need and responsible management of mental health budgets. As part of this broader process it might be worthwhile starting to assess the reasons and obstacles for discharge in addition to the reasons for admission [15].