
Abstract
Medium secure mental health units (MSUs) provide a specialised secure environment to assist people recovering from mental illness where less restrictive care has been unsuccessful or been unable to provide safety for the person or the community.
Internationally, it has been found that these units can be associated with prolonged admissions, posing ethical and resource issues.
Objectives
This ‘Realist Review’ aimed to investigate the factors associated with length of stay and outcomes of medium secure care to help inform the development of a local secure care pathway.
Method
The searches generated a total of 1570 entries across multiple search engines. Following removal of duplicates, application of inclusion/exclusion criteria and selection of articles, a total of 18 were reviewed in detail, including a further five articles obtained from references and the explored grey literature.
Results
Several issues influenced not only admission to medium secure units, but also the outcomes. Many articles were retrospective studies relying on administrative data. The realist synthesis provides contextual data to inform program development.
Conclusions
The existing literature, though variable in quality, was limited by the varied jurisdictions and contexts. However it may be useful to inform care pathways for the optimal use of medium secure beds.
Medium secure mental health units (MSUs) exist to provide 24-h secure mental health care for people whose mental health recovery needs are not safely met in other less restrictive forms of care.1,2 They may be used as step-down care from more secure forensic mental health facilities and provide a secure mode of care for non-forensic patients who have complex care needs that cannot be met in other parts of the mental health system. 3
The establishment of forensic mental health services relates back historically to an appreciation in law in the nineteenth century that a person may not be responsible for a crime due to mental illness at the time of the offence (the insanity defence), and were entitled to treatment rather than incarceration. With advances in mental health care treatment, forensic (or secure care) has increasingly incorporated ideas of rehabilitation and a focus on human rights. 4
Such secure facilities are restrictive, and therefore, there are ethical concerns about who is referred and whether the care achieves the goal of improved patient outcomes. Globally, the ethical issue of unnecessary, prolonged stays in forensic services have been identified.5–7
The ideal upper limit for length of admission to medium secure units (MSU) has been defined as 2 years 2 (Simpson et al., 1976 2 ). In 2011, a UK paper identified an increasing trend for patients to be detained in medium secure units for longer than 2 years. 7 Shah et al. (2011) 7 cited research identifying an increasing trend for patients in MSUs to be detained beyond 2 years.
A systematic review and meta-analysis conducted in 2016 examined adverse outcomes for patients in secure hospitals from 10 countries and found some evidence for discharged forensic patients having lower offending outcomes, however noted premature mortality, particularly suicide post discharge. 8 Understanding the optimal use of medium secure beds requires an exploration of care pathways both to, within and from MSUs.9,10
This review aims to synthesise the literature on factors associated with length of stay and outcomes of medium secure care to inform referral and care pathways particularly in the Australian context and in the state of Queensland.
Models of service (MOS) for the various service units within Queensland (QLD) mental health service were developed and included medium secure units. The intent behind these MOS was to inform care based on the principles outlined in the Queensland Mental Health Plan. 11 The Queensland medium secure MOS is not operationally prescriptive about referral pathways or about length of stay. The MOS remains under review. This review was conducted in the context of building a new medium secure unit in Queensland.
Aim
1) To define factors associated with admission to medium secure units. 2) To determine the factors leading to admissions that are prolonged or exceeding the recommended duration of care.
Method
A scoping review was undertaken to map the existing evidence related to the topic. 12 During this phase it became evident that a limited amount of data was available, with only one systematic review obtained. 8 A realist review was deemed the most appropriate methodology as we were interested in a complex system (medium secure mental health care) where contextual factors are influential in the function of this form of care. This approach is recommended to expand the knowledge base in areas of policy development and for research questions involving ‘what works, for whom, under what circumstances’ and the mechanism and reasons for effect.
Realist reviews can focus on the mechanism of how an intervention, in this case medium secure care works and then inform further improvement in models of the intervention. This form of review aligned to the local context of planned review of the medium secure MOS which applies to Brisbane, QLD.
Key steps in realist review (Pawson et al., 2005) 13
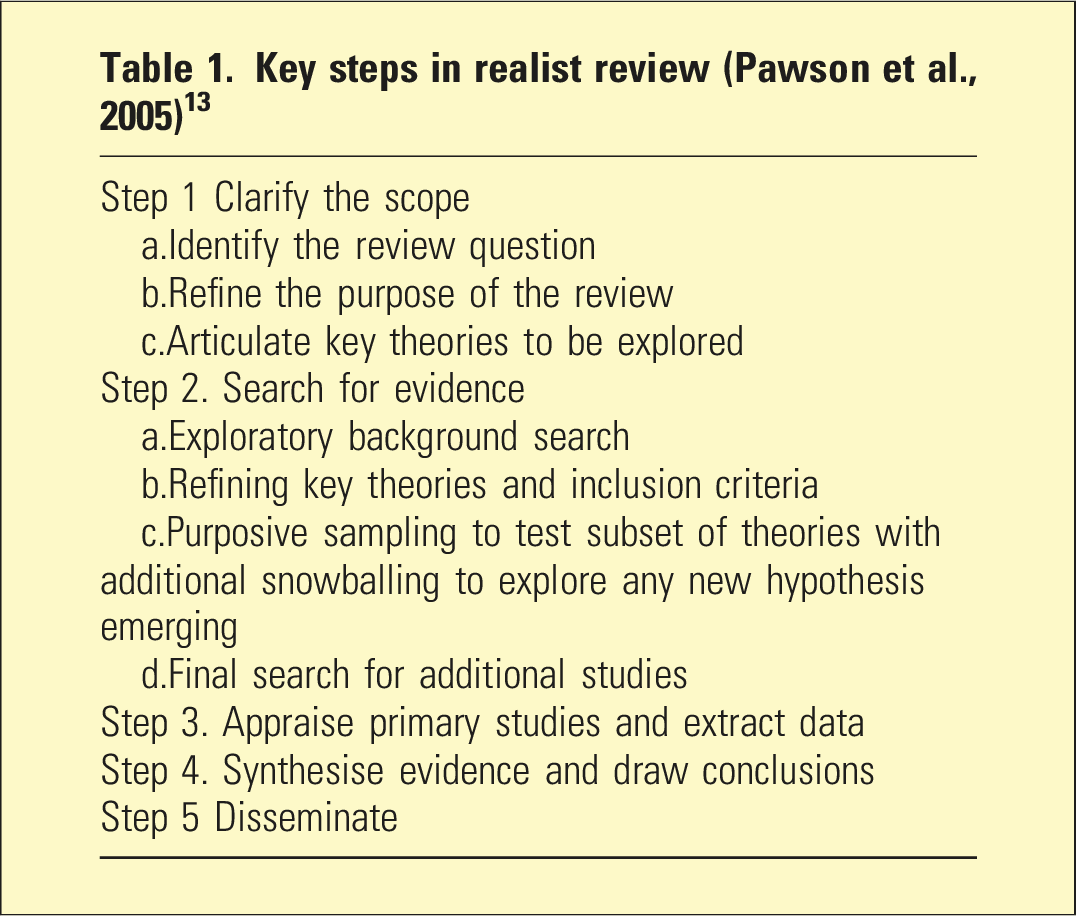
A realist review method was used to compare and analyse acceptable study standards. Quality and consistency was addressed by utilisation of RAMESES (Realist And Meta-Narrative Evidence Syntheses – Evolving Standards) standards 14 which and the STROBE 15 checklists which were comparable to Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) checklist. 16
A realist review method was compared to acceptable standards and compared to accepted standards of systematic review reporting (See Appendix*14–16).
Step1. Clarify the scope of the review and key theories
A computerised search of PubMed, Google scholar, Springer link and Cochrane Library was conducted for the years 2000 to 2021, using search terms: Medium Secure Mental Health Unit, Secure Mental Health Facility, Secure Psychiatric Unit Australia. This initial scoping review was conducted to understand the heterogeneity and complexity of the area of interest and to refine the theories extant and to inform the inclusion/exclusion criteria.
This initial search identified 1570 unique articles but only one systematic review and meta-analysis. 8
The studies were of variable methodologies and quality.
Several pertinent themes emerged from this scoping review including the impact of the social climate, progress during and after admission to secure units, risk reduction strategies in the units, physical health monitoring and wellbeing, characteristics and needs of patients in mediums secure settings.
An additional search using keywords including ‘forensic mental health legislation’ revealed policy documents, articles and editorials from Australian, UK and European sources. The information obtained from the initial scoping exercise provided the basis for a realist synthesis methodology and a further analysis of the research question.
Step 2. Search for evidence
From the scoping review it was evident that the area was characterised by complexity, contextual specificity with variable quality of studies and sources of evidence. A subsequent electronic search was completed using four electronic databases; PubMed, SpringerLink, Cochrane library and Google search engine (n = 496) and yielded 85 papers after applying the inclusion criteria and the removal of duplicates.
The search terms ((‘medium secure unit*’ OR ‘high secure unit*’ OR ‘secure psychiatric unit’ OR ‘forensic mental health’ OR ‘secure psychiatric hospital’ OR ‘medium secure mental health rehabilitation unit*’ OR ‘secure mental health unit*’ OR ‘high secure hospital’ OR ‘medium secure hospital’ OR ‘therapeutic security’) OR (‘secure mental health unit*’)) AND (outcome* OR recover* OR rehabilitation).
Step 3. Appraise primary studies and extract data
An in-depth review of the 18 papers conducted by two of the authors revealed three data categories of relevance to our aims: a. Studies focussed on length of stay in medium secure units. b. Studies focussed on patient characteristics associated with outcomes. c. Studies focussed outcomes following discharge.
Step 4: Data extraction, analysis, and synthesis
Inclusion/exclusion criteria
The articles found were reviewed according to inclusion criteria of: a. Published in English b. Published between 2000 and 2021 c. Key word/topic/theme
The articles excluded were as follows: a. Non-English publication b. Single case studies c. Studies of forensic inpatient services not specifying medium secure d. Studies with the primary aim is evaluating outcome measures e. Papers reporting on regional legislation
An additional eight potential articles were found in the hand search, of which a further five were included for the final literature review (Figure 1). Flow diagram of literature search.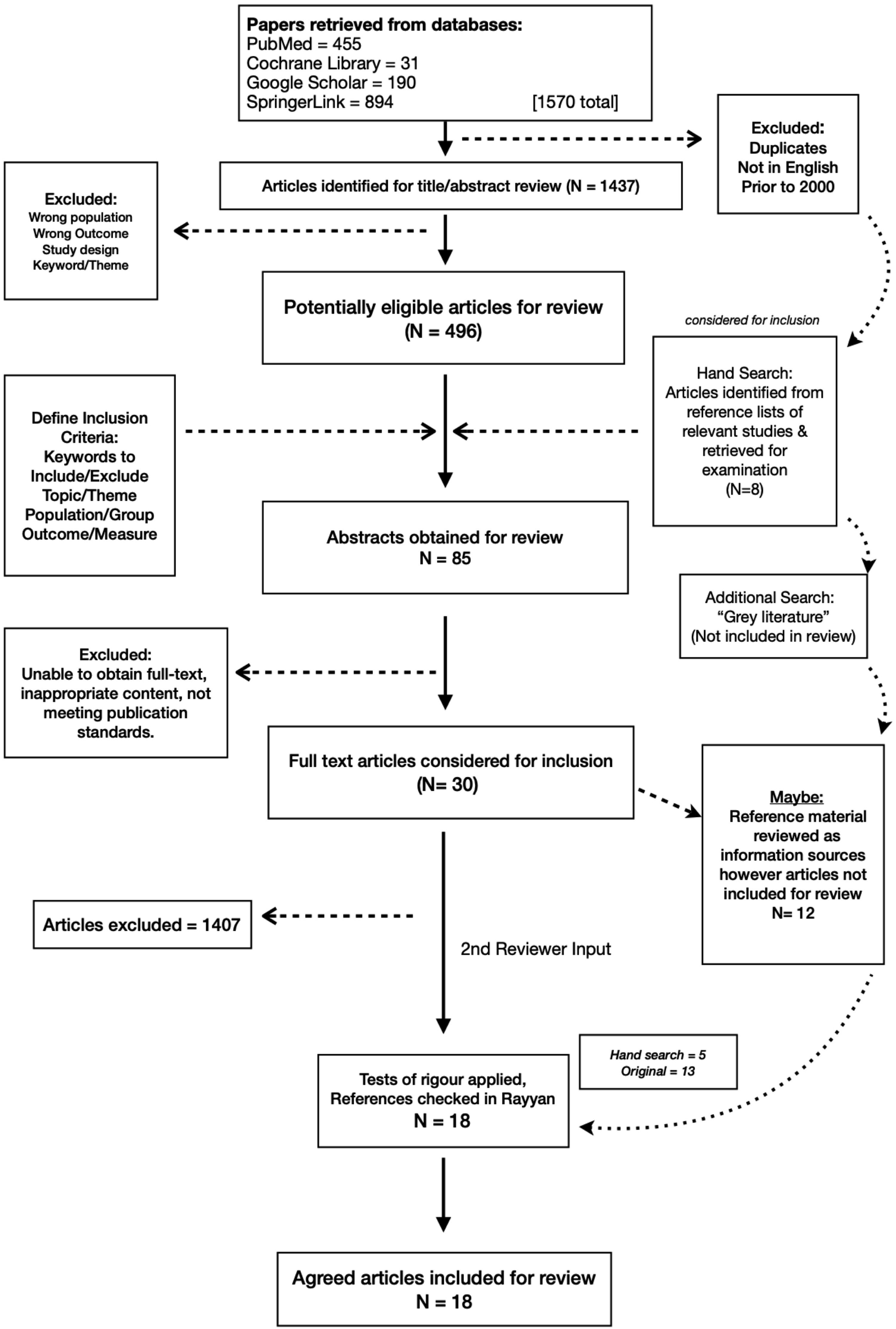
Results
Study quality
12 of these studies were retrospective cohort study designs.
Summary of articles
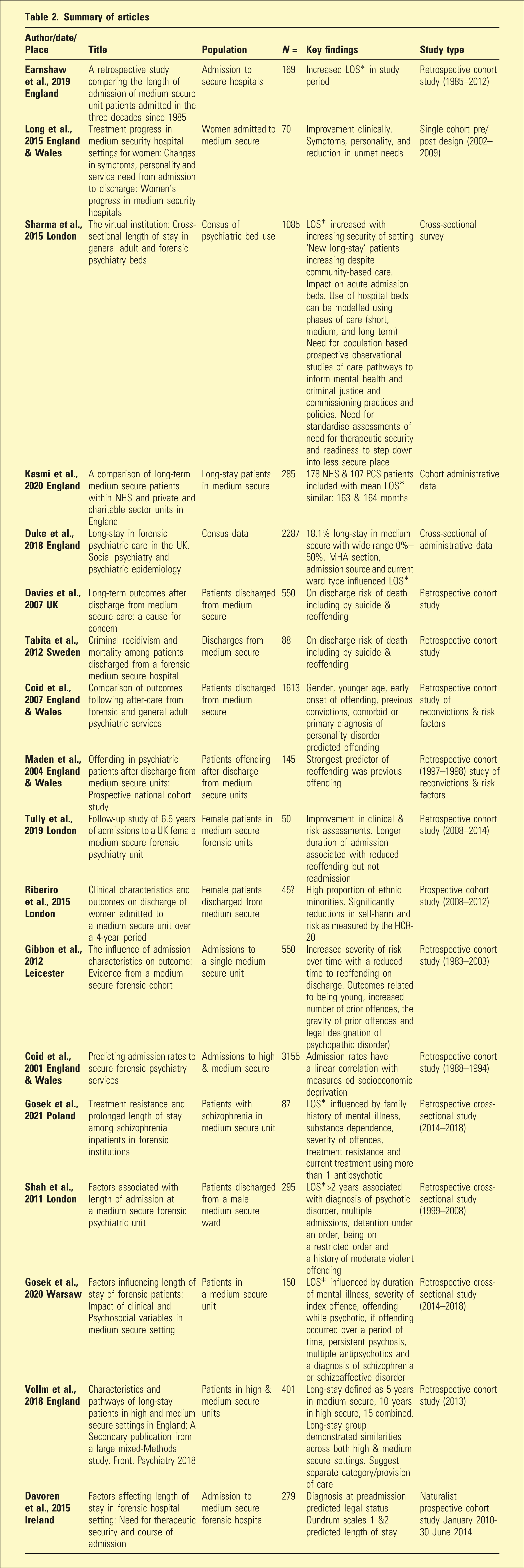
Whilst each paper looked at several elements impacting medium secure forensic patients, it became apparent that admissions, discharges and prolonged stays were multi-factorial.
Some of the studies focussed on length of stay as the main variable of interest.3,5–7,17–19
Several studies examined admission characteristics of patients20–22 four studies looked at characteristics of people within medium secure23,24,26 and four primarily 27 analysed post discharge outcomes.26,28–30
Though most of the chosen articles featured several key areas of interest, they were broadly categorised into articles with a primary focus on length of stay, admission characteristics or outcomes.
The ideal upper limit for length of admission to medium secure units (MSUs) has been defined as 2 years. 2
Prolonged admissions were more likely to be associated with diagnosed psychotic disorders, multiple prior admissions, detainment under hospital, or restriction orders or history of moderately violent offending.
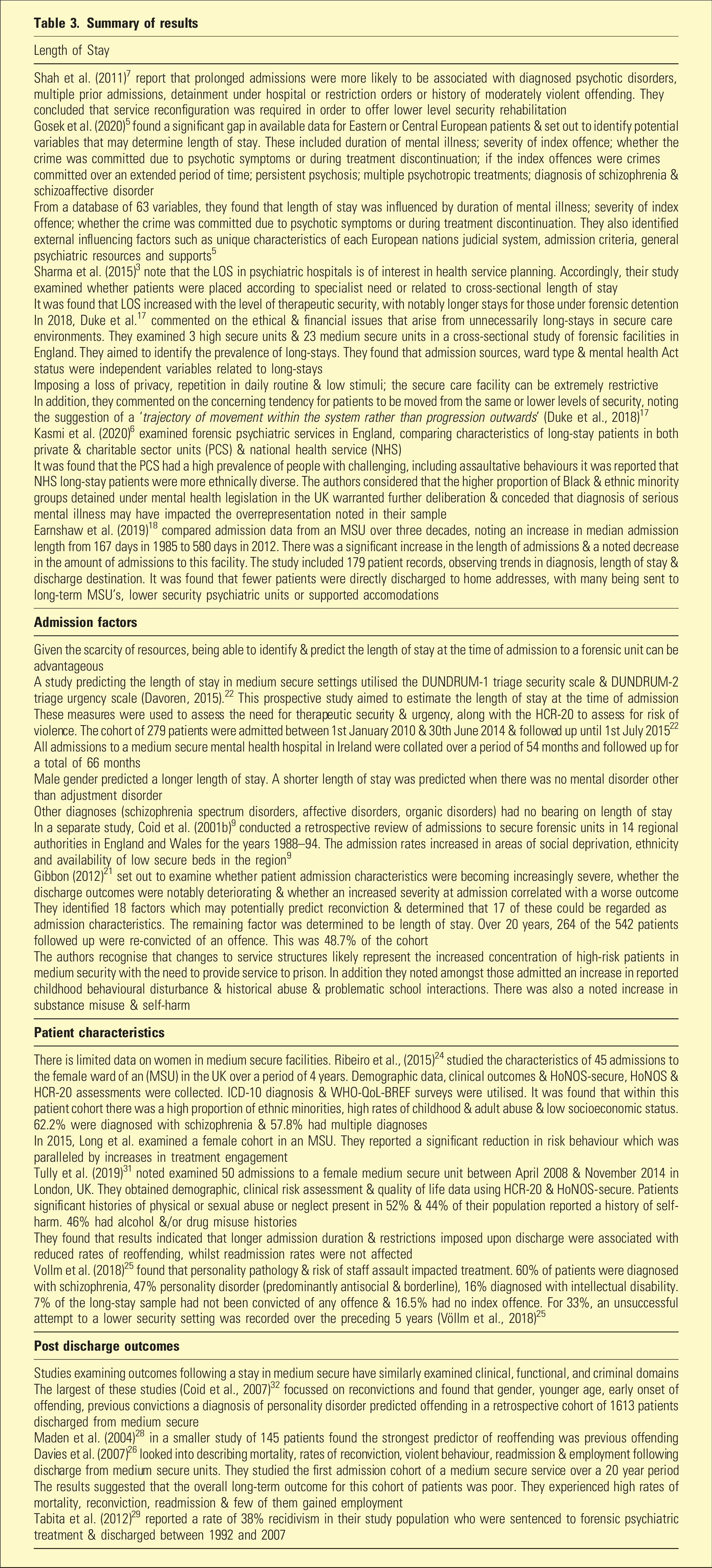
Summary of results
Discussion
Specialised secure mental health services have been set up with a dual purpose of optimising mental health care for patients who have not had their needs met in less restrictive care while also attending to community risk issues. There are numerous research challenges in these settings, which are reflected in the predominance of retrospective cohort studies using administrative data.
Völlm et al. (2018) 25 highlight the potential ethical implications of prolonged admissions. Some people admitted to forensic psychiatric care may be held for longer than they had been incarcerated for the same offence if not mentally disordered.
Length of stay
Six of the studies reviewed examined factors in length of stay (LOS). The evidence is mixed. Despite the ethical concerns of unnecessary long LOS often influenced by limited step-down options, there are also individuals where a longer than recommend 2 years LOS is required for optimal outcomes. 26 This issue is identified in smaller studies in this review examining issues for females in medium secure.23,31 There are other factors that are beginning to be a focus of research including the impact of ethnicity, 24 and socioeconomic variables on LOS. 9
In the studies reviewed, extended LOS were related to several common factors including multiple prior admissions; history of offending, particularly recidivism and severe offending; diagnosis of psychotic disorder (especially treatment resistant) and referrals from higher secure settings.
The rationale for understanding patient characteristics is to be able to predict the care needs and potential length of stay. As this patient population requires a high level of support and allocation of funding, there are often fiscal restrictions and limited resources available.
Most of the available literature pertaining to patient characteristics is published in the UK or Europe, with definitions of standards of care and quantification of risk often being led by clinicians and investigators from this part of the world.3,5–9,21,23,24,26,28–30
Earnshaw et al. 18 noted the proportion of schizophrenia diagnoses amongst their study population and the inherent risks involved when re-integrating patients into the community. They examined 47, 65, 37 and 30 patients who were admitted to the MSU over the years 1985, 1995, 2005 and 2015. Most were diagnosed with paranoid schizophrenia. The authors commented that offering extended care in supported environments may be beneficial in reducing risk to others at a population level (2019). 18
Sharma et al. (2015) noted that when studying systems, general adult and forensic psychiatric beds are preferentially compared as they tend to be inter-dependent. 3
Duke et al. (2018) concluded that there was a lack of consistency in admission criteria and discharge procedures. They also noted that sociodemographic factors may hold less significance in prediction of long-stays in forensic settings.
In 2020, Kasmi et al. found that private and charitable sector units (PCS) had a higher likelihood of accepting care of civil detention cases and intellectual disabilities, who were often long-stay residents in secure services.
Interestingly, they note similar difficulties with the development of medium secure hospital services (2020).
Gosek et al. (2021) reported that increased lengths of stay were noted in cases of: index offences of crimes committed over an extended period; persistent psychosis; multiple psychotropic treatments; diagnosis of schizophrenia and schizoaffective disorder. This review of 150 patients in medium secure setting also analysed psychosocial variables associated with length of stay. 5
Admission factors
Coid et al. (2001a 20 ) highlight the need to be aware of the social determinants of mental health, especially in health service planning. Factors associated with increased LOS (younger age, history of offending, males, diagnosis of personality disorder) also influenced admission to medium secure.
Personality pathology and risk of staff and co-patient assault further impact upon treatment and management. Poor response to treatment, ongoing safety concerns and lack of suitable step-down facilities are also identified as reasons for delayed discharge.
The findings from Davoren (2015) 22 revealed that approximating the length of stay for forensic patients may be useful for clinicians, service planners and commissioners, considering the financial implications of secure psychiatric care. 22 They reported that legal status upon admission and predicted legal status was indicative of length of stay when criminal justice disposal predicted shorter length of stay (Davoren, 2015). 22
Gibbon 2012, noted increased severity in admission characteristics that was deemed to be anecdotal and this study supported this observation.
Patient characteristics
Attributes of long-stay forensic patients in high and medium secure settings in England remain poorly understood. Völlm et al. (2018) 25 sought to clarify the patient characteristics that led to admissions beyond 5 years in medium secure care. In their sample of 401 forensic patients who met the criteria for long-stay it was determined that one fifth of the forensic inpatient population were represented by long-stayers.
It was found that of the sample of patients meeting criteria for long-stay, the authors found that 58% of these were violent offenders (22% both sexual and violent), 27% had committed violent or sexual offences in an institutional setting and 26% had committed a serious assault on staff in the preceding 5 years (Völlm et al., 2018). 25
Discharge outcomes
Particularly sobering are the studies identifying the risks of suicide and death on discharge from medium secure.8,25,28
Clinicians need to be aware that discharge from medium secure facilities can be a time of high risk of suicide.
As MSUs have an equally important role in improving the mental health of patients it is of concern that both Davies et al. (2007) 26 in a study of 550 patients and Tabita et al. (2012) 29 in a study of 88 patients noted an increased risk of death as well as reoffending.
Strengths and limitations
This review was conducted with the aim of understanding why there is a difficulty in accessing secure care. We found that there was limited local data pertaining to our area of interest. It was interesting to note that a number of international researchers considered a number of different variables which may impact an individual patient experience as well as service provision and resource limitations.
We considered this to be part of a more in-depth study to begin to understand how to inform policy around the provision of a new MSU.
Whilst a systematic review remains a gold standard of literature review, it does not address how or if an intervention works and can often result in some aspects being left unresolved. A realist review was determined to be an appropriate investigation tool; however, this remains a new and emerging method. 13
Our research team were English speakers only and our review included some limitations.
Non-English documents were excluded from our searches. An inclusive approach and broad definitions to search terms were applied.
There are several challenges influencing the type and quality of research in secure settings which is reflected in the predominance of retrospective studies using administrative data identified in this review. In addition, these services vary based on country and jurisdictions, with most studies in this review emanating from the United Kingdom.
We conducted our realist review within a 1 year timeframe. Subsequently, it became difficult to publish the results of the analysis.
The review did not look at details of the programs run in MSUs and the influence of care offered on outcomes. Many studies were from the UK which needs to be considered in extrapolating to other jurisdictions. MSUs in the UK are managed by forensic services and admit patients with serious violent or sexual offences (that would meet the criteria for high secure admission in Queensland, Australia).
In Queensland, the secure rehabilitation units are generally managed by district services. The UK also has ‘secure rehabilitation units’ analogous to those in Queensland and managed by districts (not forensic services).
Ultimately it was found that the value of the realist synthesis is to provide more contextual information in the development of program theory.
Future research directions
The authors plan to use this information to inform medium care pathways in the Australian context.
There is need for further research to test theories developed from this review. 32 These include a need for improved understanding of the medium secure MOS; incorporating complex care reviews in management/treatment planning; and discharge planning to ensure transitional care.
A retrospective cohort study of patients currently admitted to The Park Centre for Mental Health’s Medium Secure Unit has been considered.
In addition, a prospective study will be undertaken to do a longitudinal assessment of referrals to new medium secure rehabilitation unit. The objectives would be to evaluate the policy and procedures developed for admission to that facility, the degree of integration with the broader mental health system and the discharge options available.
Conclusion
This study was undertaken to address the need for development of a referral pathway into local medium secure services. A realist review was utilised with the aim of synthesising relevant data and applying it in the appropriate context to inform policy and procedure.
MSUs are necessary to meet the specialised needs of a minority of patients with mental illness requiring secure mental health care to recover. They need to be well integrated into the broader mainstream mental health service that will refer to the unit and be part of care after discharge.
Pathways of care need to be clear to ensure less restrictive interventions have been tried prior to referral to a medium secure and that step-down options are available that give a level of support to mitigate against the risk of suicide and reoffending.
Supplemental Material
Supplemental Material - Factors associated with length of stay in medium secure units: A realist review
Supplemental Material for Factors associated with length of stay in medium secure units: A realist review by Wajeeha Zagham, Steve Kiseley, Terry Stedman, Karen Brown, and Frances Dark in Australasian Psychiatry
Footnotes
Acknowledgement
Thanks to co-authors SK, TS, KB.
Author contributions
W.Z. and F.D. conducted the searches and independently screened the abstracts and full text articles. All authors were involved in writing the article.
Disclosure
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
On request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.