
Abstract
Objective:
The prevailing paradigm in suicide prevention continues to contribute to the nihilism regarding the ability to prevent suicides in healthcare settings and a sense of blame following adverse incidents. In this paper, these issues are discussed through the lens of clinicians’ experiences as second victims following a loss of a consumer to suicide, and the lens of health care organisations.
Method:
We discuss challenges related to the fallacy of risk prediction (erroneous belief that risk screening can be used to predict risk or allocate resources), and incident reviews that maintain a retrospective linear focus on errors and are highly influenced by hindsight and outcome biases.
Results:
An argument that a Restorative Just Culture should be implemented alongside a Zero Suicide Framework is developed.
Conclusions:
The current use of algorithms to determine culpability following adverse incidents, and a linear approach to learning ignores the complexity of the healthcare settings and can have devastating effects on staff and the broader healthcare community. These issues represent ‘inconvenient truths’ that must be identified, reconciled and integrated into our future pathways towards reducing suicides in health care. The introduction of Zero Suicide Framework can support the much-needed transition from relying on a retrospective focus on errors (Safety I) to a more prospective focus which acknowledges the complexities of healthcare (Safety II), when based on the Restorative Just Culture principles. Restorative Just Culture replaces backward-looking accountability with a focus on the hurts, needs and obligations of all who are affected by the event. In this paper, we argue that the implementation of Zero Suicide Framework may be compromised if not supported by a substantial workplace cultural change. The process of responding to critical incidents implemented at the Gold Coast Mental Health and Specialist Services is provided as an example of a successful implementation of Restorative Just Culture–based principles that has achieved a culture change required to support learning, improving and healing for our consumers, their families, our staff and broader communities.
Keywords
Introduction
In the Margaret Tobin Oration at the 2018 Royal Australian and New Zealand College of Psychiatrists (RANZCP) Congress, Turner (2018) outlined the need for a paradigm shift in suicide prevention in mental health services. This includes a shift away from the pervasive pessimism regarding the ability to prevent suicides, the focus on assessment and categorical risk prediction, the lack of focus on meaningful interventions, disjointed training and support provided to staff and the use of diagnosis as a gateway to services. The oration argued that an alternative approach is provided by the Zero Suicide Framework (ZSF), which emerged from the National Action Alliance’s Suicide Care in Systems Framework (Covington et al., 2011). ZSF entails suicide specific evidence-based practices, reliably delivered by well-managed whole systems of care that are continuously improving service access, quality and safety; and that are firmly rooted in core values reflecting a service culture that no longer accepts suicide as an outcome. (Mokkenstorm et al., 2017: 2)
The shift in values and culture is facilitated by the relentless pursuit of the aspiration of zero suicides within a healthcare setting, through the delivery of highly reliable healthcare (May, 2013). This framework consists of seven essential elements (see Table 1) and can complement an all-of-community systems approach such as Lifespan (Baker et al., 2018).
The seven essential elements of the Zero Suicide Framework.
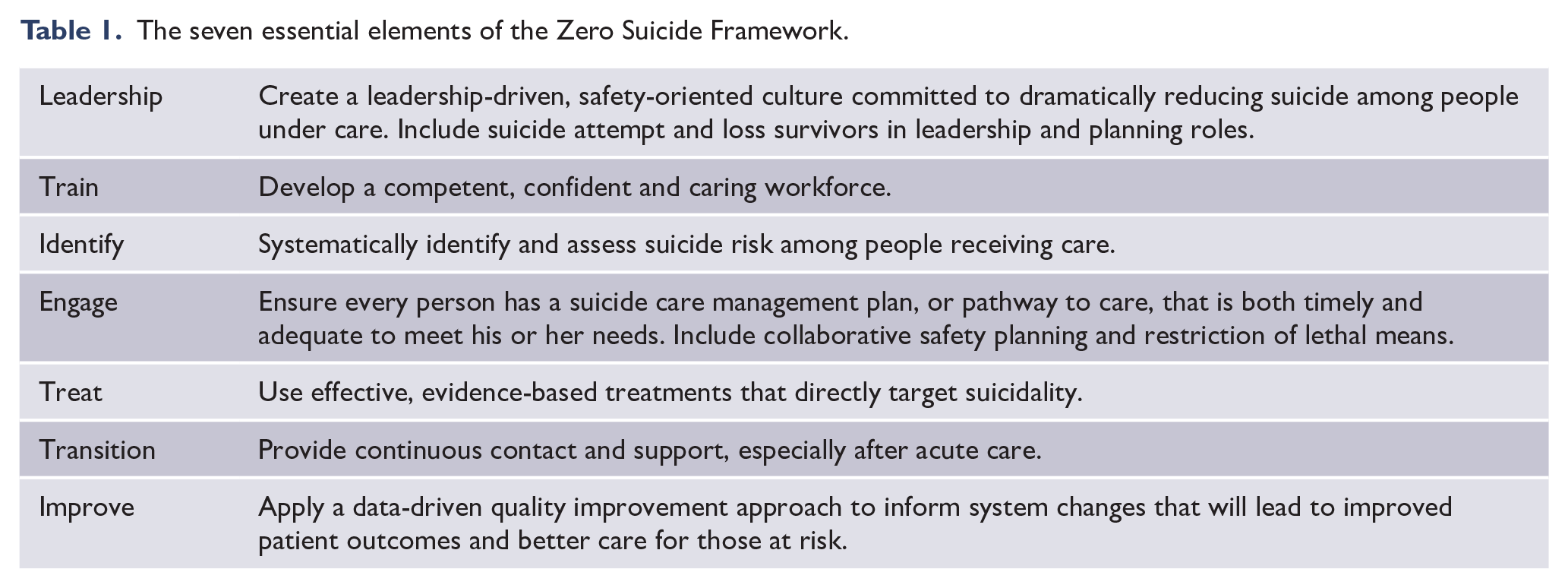
While aiming to create the cultural transformation and shift in mindset through an aspirational goal, there are potential risks associated with the use of the zero terminology. Legitimate concern has been expressed about use of the word ‘zero’ as it may be interpreted as a target or key performance indicator rather than an aspiration and may create or worsen a culture of blame or risk aversion (Coyne, 2016; Smith et al., 2015). Turner (2018) acknowledged these issues but noted that concerns about blame are not new to the ZSF and are already present and impacting clinicians.
The central thesis of this paper is that the implementation of ZSF may be compromised if not supported by a substantial cultural change, and our central recommendation is that ZSF be implemented in parallel to concerted efforts towards achieving just culture. In order to support this argument, we describe several ‘inconvenient truths’, which represent significant cultural and procedural barriers to preventing suicides in healthcare settings. We first examine the impact of deaths by suicide on frontline clinicians in health services through the concept of the second victim. We then focus specifically on the processes surrounding organisational reviews of suicide-related critical incidents, which, when done in the context of the current paradigms, have a potential to perpetuate a blame culture. We then introduce the principles of Restorative Just Culture (RJC) and discuss how workplace cultural challenges could be addressed by embedding RJC principles as a foundation to support a ZSF. Finally, we describe the learnings gained in the context of implementation of a ZSF alongside RJC in a large Hospital and Health Service in Queensland, Australia.
‘Inconvenient truths’ in suicide prevention
Through the lens of the clinician: second victims and clinician welfare
Clinicians working in the complex world of mental health and suicide prevention face many challenges. One of these is the devastating impact of the loss of a consumer to suicide. Another is the impact of working within a complex system, where those complexities are not overtly acknowledged or reconciled within our responses to critical incidents such as suicides.
Mental health workers have significant exposure to consumers who die by suicide. Nijman et al. (2005) estimated that on average, a mental health nurse working full time experiences a consumer suicide every 2.5 years. Wu (2000) introduced the term ‘second victim’ to describe healthcare providers who are involved in an adverse event and subsequently emotionally traumatised (with the consumer considered the first victim).
Death of a consumer due to suicide frequently results in mental health staff experiencing a range of adverse outcomes. Physical symptoms can include fatigue, insomnia and nausea, and psychological symptoms can include disappointment, self-blame, anger, guilt, shame, troubling memories and anxiety (Joesten et al., 2015; Newman, 1996; O’Beirne et al., 2012; Paparella, 2011). Second victims may have ideations of having failed the consumer, and second-guess their clinical skills, knowledge and even career choice (Newman, 1996; Scott et al., 2009). Involvement in an adverse event may also lead to fear of legal retribution, prejudice and loss of reputation, licensure or income or even criminal charges (Joesten et al., 2015; Paparella, 2011).
In mental health care, a ‘culture of blame’ continues to exist around events such as suicide, which is exacerbated by political forces, and criticism from public agencies and the media (Wand, 2017). Medical errors are often not discussed, which further reinforces feelings of isolation, mistrust, guilt and abandonment in second victims (Paparella, 2011). This ‘culture of silence’ (Paparella, 2011) can result in changes to clinical treatment driven by high levels of risk aversity that is potentially harmful to consumers as well as mental health services (Bowers et al., 2006; Morgan, 2007).
There have been increasing calls for organisations to provide specific support to mitigate against the second victim experience in their staff (Scott et al., 2010). Denham (2007) proposed five rights of second victims that should drive healthcare responses under the acronym TRUST: Treatment that is just, Respect, Understanding and compassion, Supportive Care, and Transparency and the opportunity to contribute.
The need to respond to second victims has been likened to a psychological emergency, and the need for a formalised response by leaders at all levels from local to national leadership has been described as ‘mission critical’ (Denham, 2007).
Through the lens of healthcare organisations
The failures to adequately recognise and support second victims are often intertwined with the limitation of the existing structures for critical incident reviews. In particular, these processes are impacted by inadequate recognition of the complexity of healthcare settings, and the resilience and flexibility required in suicide prevention endeavours. They also fail to reconcile with the limitations of risk assessment, and outcome and hindsight bias. We refer to these as ‘inconvenient truths’, as they are unsettling concepts which challenge current concepts of linear, cause-and-effect understanding, and are difficult to address.
Fallacy of risk prediction
There has long been a preoccupation with risk assessment in consumers presenting with suicidality to healthcare settings, as if this activity was an end in itself. Despite mounting evidence that the use of risk stratification (high, medium or low) cannot adequately predict suicidal outcomes and should not be used to allocate resources (e.g. make decisions about admission or interventions provided) (Large and Nielssen, 2012; Large and Ryan, 2014), documentation used in clinical practice has long supported a categorical risk prediction model. Retrospective reviews of incidents are also frequently undertaken through this lens of risk prediction, implying that an improved risk assessment could have led to a different outcome. In doing so, factors that may have equal or greater impact on preventing suicide, such as therapeutic relationships and instilling a sense of hope, are often overlooked (Steeg et al., 2018). It has been suggested that we need to acknowledge our powerlessness to usefully classify individuals or groups of patients according to future suicide risk. We need to acknowledge this to ourselves, and communicate this to health departments, to the courts, and most importantly to our patients and their families. (Large et al., 2017: 162)
In many ways, this ‘inconvenient truth’ of the fallacy of risk prediction lies at the heart of the need for both a systems approach to suicide prevention and RJC. For too long, clinicians have been judged in incident reviews after a loss of a consumer to suicide, based on this fallacy of risk prediction. Of key importance is that the ZSF is grounded on the belief that our inability to predict suicidal outcomes does not preclude us from preventing suicides through a robust systems approach. However, there are several other challenges pertaining to incident reviews, when there is a death by suicide; these are discussed next.
Fallacies of hindsight and outcome bias in incident reviews
Incident reviews frequently focus predominantly on the issues that occurred close to the time of the incident. This may have a number of repercussions, including the under-appreciation of the quality of engagement, and the therapeutic and rehabilitative care provided to the consumer. There is also the risk that proximal issues will be seen as ‘contributing factors’ leading to the implementation of restrictive practices, such as locking of units to prevent people from absconding and increase in involuntary admission to hospital (Vine and Mulder, 2013). Vine and Mulder (2013) further highlight the importance of members of the review team being trained in a recovery focus that balances personal dignity and choice with more restrictive practices. As will be described, an RJC approach provides this opportunity.
Hindsight bias is another complex issue that routinely impacts incident analyses. Reviewers who are aware of the outcome tend to overestimate the likelihood of that outcome and the ability of the involved clinicians to have predicted it. This bias tends to colour the evaluation of actions taken prior to an outcome, such that actions taken before a good outcome are deemed good, and actions taken prior to an adverse outcome are deemed negative (Dekker, 2012; Henriksen and Kaplan, 2003).
Furthermore, the processes that review rule violations as decision points in assessing culpability are highly vulnerable to hindsight bias. For example, algorithms may ask whether the clinician who departed from agreed protocols or safe procedures took an unacceptable risk (Queensland Health, 2014). The challenge with this approach is that the decision about ‘unacceptable risk’ is highly influenced by hindsight bias and fails to consider or learn why the system essentially enabled the clinician to take that decision at the time.
Hindsight bias is impossible to remove, however, may be mitigated by ‘reconstructing and understanding the mind-set of people as they experienced the events unfolding and why their assessments made sense at the time, rather than using hindsight to work out why they did not make sense’ (Henriksen and Kaplan, 2003: 49). As will be described, engagement of all stakeholders should ‘hard-wire’ this input, with the individuals or teams involved in critical incidents acting as a central component of the review process.
Outcome bias, where we allow the outcome of an event to influence our response to it, also represents a barrier to safety and a sense of justice. As noted by Marx (2019), there is a need to understand the actions of staff, rather than the outcomes they produce, as reacting to the severity of the outcome may simply punish the unlucky. Our current review systems revolve around outcome bias, focusing predominantly on events with the worst outcomes. In addition to the sense of injustice this may create, it allows unsafe actions, which do not lead to adverse outcomes, to go unexamined and therefore contributing to the persistence of an unsafe system.
Limitations of a Safety I approach given the complexity of suicide
A linear, cause-and-effect approach to patient safety has been a predominant paradigm across much of healthcare in performing incident analysis following deaths by suicide. This has been enhanced by consideration of human factors that can contribute to failures and also seeing humans as interacting with a challenging system impacted by latent factors (e.g. workload pressures, technology, resources, procedures) (Ball and Frerk, 2015; Mannion and Braithwaite, 2017). This traditional approach to patient safety, labelled ‘Safety I’ (Hollnagel et al., 2015), can lead to important learnings in the system; however, they are thought to be most effective where activities are well understood, relatively stable and have limited external influences, such as using theatre checklists, or protocols to reduce central line infections (Braithwaite et al., 2015).
Braithwaite et al. (2015), however, argue that the traditional understanding and approach to patient safety (Safety I) cannot satisfactorily address increasingly complex healthcare settings. Specifically, a retrospective view does not help foster understanding as to how clinical incidents, particularly the most complex and multifaceted ones, such as suicides, come about and what perpetuates them (Diptee and Baker, 2013). Therefore, a change in approach is required, one that ‘switches the focus from preventing things going wrong to purposefully enabling them to go right’ (Braithwaite et al., 2015: 2). This new paradigm of patient safety has been termed Safety II and can be complementary to Safety I. It ‘focuses on creating success rather than eliminating failure and pays greater attention to how clinicians create safe, high quality care through adaptation, improvisation and dedication’ (Smaggus, 2019: 667).
Human variability and trade-offs
A central consideration of Safety II is the role of human variability in health care. While Safety I and traditional frameworks for just culture view variability as violations of practice, non-compliance or deviations (Hollnagel et al., 2015), Safety II understands that in order to have a resilient system, clinicians need to adapt when the unexpected occurs and according to the conditions in which they find themselves, which includes a flexible response to procedures. In these situations, performance variability is essential to maintaining a safe system (rather than being viewed as a violation in traditional patient safety). Reason (2000) noted that human variability may be essential in emergency situations where the control must shift to ‘the experts on the spot’ (p. 770) who must adapt and compensate, and then when the emergency is over, return to consistency, albeit with an alertness to the possibility of failure.
Human variability also allows for trade-offs depending on the circumstances at the time (Sujan et al., 2016). A prime example is the so-called Efficiency-Thoroughness trade-offs; efficiency is favoured where throughputs are a focus; however, thoroughness must take precedence where safety is of paramount importance. This tension is critical in an emergency department setting, a common setting for assessments of suicidality, and although it is impossible to maximise both at the same time, there must be a minimum of each (Hollnagel, 2016). When the system does not acknowledge the trade-off being made in order to achieve efficiency, efficiency will be rewarded until there is an adverse outcome which will then be reviewed through the lens of a need for more thoroughness (McNab et al., 2016). This represents a failure of the Patient Safety focus on errors and waiting for that error, rather than understanding how work is currently being undertaken and what work-arounds are actioned to achieve functioning.
It therefore follows that both successes and failures in healthcare can arise from individual or systemic performance variability, and a more useful focus of understanding our system is on the ‘continued functioning of systems under challenging circumstances, rather than the search for and rooting out of errors and mistakes’ (Hollnagel et al., 2019: 1). Braithwaite et al. (2019) refer to ‘resilient health care’, highlighting the importance of taking an everyday clinical work perspective when reviewing incidents to achieve learnings that have more relevance to, and greater ownership from, clinical staff (Sujan et al., 2016). Everyday clinical work of mental health clinicians also includes balancing principles of recovery and least restrictive alternatives alongside responsibilities for the protection of consumers and the community.
Work as imagined versus work as done
Hollnagel et al. (2019) argue that ‘there will always be a gap in understanding between those who plan, prescribe, fund or mandate initiatives to keep things safe and those who treat, care for or intervene directly to alleviate patients’ conditions’ (p. 2). This gap is demonstrated by the contrasting concepts of Work as Imagined (WAI) and Work as Done (WAD) (Funabashi et al., 2018).
Frequently, reviews of adverse events are approached from the belief that WAD should be identical to WAI, and that safety can be maintained through widespread use of procedures and compliance that attempt to reinforce WAI. Linked to it is an assumption that good outcomes occur as a result of WAI, and bad outcomes occur because of deviations from it (Ball and Frerk, 2015; Hollnagel et al., 2015). Such bimodal thinking then reinforces the aim to keep everyone functioning in WAI. However, Hollnagel et al. (2019) recognise that it is impossible for healthcare providers to adhere completely to all the instructions, policies procedures and rules, just as it is impossible that policy makers and managers striving for WAI could alter these same procedures and rules such that they corresponded with WAD: ‘People are not the problem to be solved or standardized: they are the adaptive solution ... and we should try to understand the characteristics of everyday performance variability’ (Hollnagel et al., 2015: 16–17). In learning about our system, there is therefore a need to understand the gap between WAI and WAD, without judgement of whether one is right or wrong (Sujan et al., 2016). The authors argue that safety will rely on our better understanding of WAD, and why things go right, and ensuring that the capacities to make things go right are identified and enhanced.
Clinician welfare
Clinicians work in complex systems which are unpredictable and do not conform to the linear expectations and mechanistic thinking that often drives service improvement efforts, thus requiring highly flexible adaptive responses. These complex systems may be exhausting for clinicians to navigate, together with dealing with a system based on Safety I thinking that judges negatively variations in practice and trade-offs required (Smaggus, 2019).
This risk of a predominant focus on Safety I is that clinicians’ expertise and knowledge will be de-emphasised in favour of focusing on the importance of those who design and regulate our healthcare systems. This can have an impact on clinician well-being through loss of sense of self-esteem, self-efficacy and personal accomplishment (Smaggus, 2019). On the contrary, Safety II may provide an opportunity to better understand and support the demands and successes of their everyday work. This perspective ‘affords clinicians the esteem they deserve, as it casts them not as hazards, we must restrain, but as essential ingredients whose strength we must enable to attain safe, high-quality care’ (Smaggus, 2019: 669). This insight gives us a new incentive to engage clinicians within the learning process following adverse events, as we will not learn the right lessons without their input.
Supporting and empowering staff in health care services, as well as protecting them against blame and inappropriate guilt, represents a key determinant for success of the ZSF (Mokkenstorm et al., 2017). Furthermore, it has been recognised that continuous and sustained quality improvement – another essential element of the ZSF – is reliant primarily on changing workplace culture (Cohen et al., 2003).
From just culture to RJC
Despite the long-standing acknowledgement that culture is central to patient safety and that blame cultures are contributing to unacceptably high rates of adverse events (Catchpole et al., 2006; Cook et al., 2004), organizations have struggled to move away from cultures of blame (Khatri et al., 2009). This can have impacts on risk aversion, increasing restrictive practices and failure to support capacity building and autonomy (Wand, 2017). A just culture, on the contrary, seeks to achieve a balance between ensuring learning from adverse events and accountability of staff. The predominant paradigm, documented in most existing guidelines on post-incident processes, focuses on algorithms which aim to differentiate between acceptable and unacceptable behaviour (Marx, 2001; Reason, 1997; Wachter and Pronovost, 2009). It assumes that answering a variety of questions – What rule is broken? How bad is it? What should the consequences be? – leads to the development of a proportional and fair response (Boysen, 2013; Dekker et al., 2013).
However, several authors have raised concerns around just culture, citing limited evidence that it has led to improvements in reporting or reductions of the blame culture (Edwards, 2018). Von Thaden et al. (2006) and Dekker and Hugh (2010) express caution about the ability to draw a line between blameworthy and blameless acts, and about who should draw that line. An algorithmic approach ‘may imply that actions committed by staff are binary (either acceptable or unacceptable) without appropriate appreciation of the messiness of the system in which the action occurred’ (Peerally et al., 2016: 419).
In addition, the prevailing paradigm of just culture offers limited engagement for either the clinician or the consumer, and their family or carers. Instead, it implies that those in the organisation will know where to draw the line between blameworthy and blameless actions (Reason et al., 1997) and that ‘... clinicians know they will be treated fairly and will be held accountable for their actions and behaviours’ (Queensland Health, 2014: 27).
The insights provided by Safety II suggest alternative perspectives to reviewing critical incidents. These include the need to understand and reconcile WAI versus WAD without assuming one is right; to understand why things are done the way that they are at the ‘sharp end’ of business; to understand what trade-offs are being undertaken by staff; and to understand that the same variability in practices found in retrospective reviews may be the reasons for successes as well as failures. These considerations are far less convenient than a retrospective lens that sees all human variability as ‘violations’ which must be assessed against an arbitrary line separating errors from reckless acts. Yet, adopting these considerations has been shown to reduce the fear of blame which impedes improvement in complex human systems (Berwick, 2013).
RJC poses very different questions from the traditional retributive questions posed by just culture approaches. RJC asks: Who is hurt? What they need? and Whose obligation it is to meet those needs? It promotes the healing of trust, relationships and people (Weitekamp, 1999; Zehr, 2002) and empowers first and second victims (Barton, 2003). RJC moves away from asking who did something wrong and what should be done about them, to what was responsible for things going wrong and how this can be addressed. This framework accepts that involved staff can have both accountabilities and needs, and is predicated on the principle of inclusive engagement of all stakeholders. This aligns well with the second victim rights as outlined by Denham (2007).
Accountability is a strong theme of RJC, which recognises that staff are accountable for being part of the healing, learning and improving process after a clinical incident; however, at the same time, they too may have needs for support, and these needs are recognised within this framework. RJC is action orientated, assigning roles and responsibilities for all who have a stake in the event and advocates for forward-looking rather than backward-looking accountability, and the avoidance of blame (Dekker, 2016; Khatri et al., 2009; Sharpe, 2004; von Thaden et al., 2006). A peer led, non-punitive, restorative response has proven more successful in changing behaviour towards a safer system (Dekker, 2016). Implementing RJC has also been found to be cost effective (Kaur et al., 2019).
Engagement of all stakeholders in the post-incident review acknowledges that the greatest learning can be achieved through a social and participative process (Macrae, 2016). Leistikow et al. (2016) argue that staff participating in the learning at a local level, and coming up with local solutions, can improve safety in that setting by changing the way they think about, and maintain an awareness of, risk. Safety II principles imply an imperative to understand everyday clinical practice, WAI, WAD, and trade-offs occurring in our healthcare settings. This may challenge some in positions of power; however, it is only with true engagement of all stakeholders that the WAI versus WAD gap can be reflected upon, ensuring that ‘double loop learning’ occurs (Sujan et al., 2016: 116). An RJC approach, which requires the engagement of all stakeholders, is well placed to bring together everyone’s perspective to gain that understanding – from clinicians involved in the event, to families, consumers and healthcare leaders.
RJC also places obligations and accountability on health care organisations and leaders to provide support for all of those in need and to provide clinicians with an adequate response to their distress. This can be crucial for suicide prevention among healthcare staff who become second victims (Dekker et al., 2013; Jones and Treiber, 2012; Wu, 2000).
We propose that an RJC helps an organisation learn and improve, and equips staff and management with processes to offset or remedy the guilt and other negative emotions commonly experienced by second victims (Bowers et al., 2006; Joesten et al., 2015; Paparella, 2011).
Where is individual performance accountability?
Healthcare systems have various processes in place to deal with individual performance of concern, impaired clinicians or (very rarely) malicious criminal acts. This occurs by way of supervision frameworks, performance reviews and appropriate state legislation. These frameworks and processes are critical for effective maintenance of high professional standards and should be adhered to regardless of the occurrence of critical incidents. Outcome bias should not be the driver of professional development and accountability frameworks, and therefore, the algorithms suggested by the traditional just culture frameworks should not be required – in fact, they can easily become misleading.
Implications for incident review processes and root cause analyses
There have been reservations expressed about the widespread adoption of root cause analysis (RCA) in healthcare (Peerally et al., 2016). As the name implies, this process searches for a ‘root cause’ behind a critical incident by using tools such as the ‘five whys’ and timelines which may favour a ‘temporal narrative’ rather than consider the complex interplay of factors in a system. They are often performed independently from the treating team.
Due to these concerns, the Canadian Incident Analysis framework (Incident Analysis Collaborating Parties, 2012), for example, decided to discontinue use of the term RCA. Instead, it proposes the use of concepts related to complexity theory to avoid the trap of linear representation. The use of a constellation diagram presents clusters of possible factors rather than suggesting cause-and-effect relationships. These clusters of factors provide an opportunity to consider systems, and their connections, including tasks, equipment, work environment, consumer, care team, and organisational factors.
Peerally et al. (2016) suggest that some RCA reports are overtaken by other competing factors and may end up containing information in them that does not always reflect the actual events or the discussions with the review team. Causes for this may include pressure of timelines and a focus on the report as the end point rather than the learning process, as well as lack of independence, attempts to preserve relationships, and partisan interests. Recommendations that arise from RCAs are frequently weak in strength and are often not shared across the service or even fed back to the involved team. Many of these concerns resonate well with the drivers towards RJC.
Implementation of RJC at the Gold Coast Hospital and Health Services: lessons learned
The Gold Coast Mental Health and Specialist Services (GCMHSS), based in Queensland, Australia, adopted ZSF in 2015 as part of the GCMHSS Suicide Prevention Strategy (Gold Coast Mental Health and Specialist Services, 2016). A central component of the implementation of ZSF at GCMHSS was the replacement of a categorical risk prediction approach (high, medium, low) with the Prevention Oriented Risk Formulation (Pisani et al., 2016). The purpose of the risk assessment within ZSF therefore is not to predict suicide but rather to inform effective suicide care. This change was based on the identified need to move away from the expectation that clinicians should be able to predict risk of a consumer’s suicide and respond to that prediction. The new framework supports universal approaches to people presenting with suicide risk, and support for clinicians to develop improved skills for engaging collaboratively with consumers to understand their stories, develop individualised risk formulations that inform a care plan, engage in collaborative safety planning (Stanley and Brown, 2012) and support smooth transitions of care.
The principles of RJC have been embedded into the implementation of the Suicide Prevention Strategy from the very beginning, particularly through an increased focus on training of all staff and enforcing of the message that suicides in healthcare are preventable, while at the same time safeguarding clinicians’ own well-being. Based on staff feedback, a review of the literature and focus groups, the following main issues were identified with respect to responding to and learning from incidents, which also represent the underlying principles that became drivers of change in the service:
Building the culture
Clinicians require a high level of trust in the organisation to engage in a Zero Suicide aspiration and to openly learn from incidents. Trust is fostered through the use of an RJC framework.
Everyone is accountable: RJC demands actions by all, by allocating roles and responsibilities for those who have a stake in the event. Some may have multiple roles, including the need to support the healing of others, learn and improve, but they may also be in need of support for healing.
Healing
The negative impacts of being a second victim are significant, foreseeable and require an urgent response by leaders at all levels of our healthcare system.
Healing for all is an important consideration, including availability of skilled staff and pathways for supporting consumers, their families and the community following critical incidents.
Learning
A strong foundation of incident review expertise is important, including expertise in Human Factors within the review teams.
Reviewing the continuum of care for the consumer rather than focus on issues proximal to and leading back from the incident in a linear way, to allow for mitigation of hindsight bias, and a greater understanding of important issues such as development of a therapeutic relationship over time.
Use of tools that can assist with understanding complexity such as constellation diagrams, and avoidance of linear approaches to learning.
Use of tools that can support enhanced quality and strength of recommendations.
Some independent representation on the review teams can further enhance accountability.
Involving the clinical teams in the review process is essential to: ○ Allow the ‘right’ lessons being learned through a true understanding of WAD, everyday clinical work, trade-offs, and appropriateness of human variability in practice. ○ Ensure involvement of staff with a good understanding of recovery principles to allow for a balance between personal dignity and more restrictive practices. ○ Ultimately will support the translation of learnings into improvements in the workplace.
Ensuring a place for the service leadership to be involved in the review, allows opportunities for ‘double-loop’ learning where the WAI is overtly critiqued.
Hardwiring opportunities for the consumer, family or carers to input into the review process, to ensure a full understanding of the many perspectives of the event.
Reviewing a range of clinical incidents instead of focusing on a small group of severe adverse events. These may include near misses, or more frequent yet less severe events (e.g. suicide attempts), as well as analyses of groups of incidents.
Improving
Greater involvement in and ownership by the clinical teams will facilitate translation of recommendations into actions in their workplaces to make the system safer.
Feedback of learnings and recommendations to the teams and other teams across the service will maximise the opportunity for learning and improvements.
As part of this process, and based on the above findings, GCMHSS decided to move away from the ‘commissioned’ RCAs which give legislative protection to the teams reviewing incidents (Queensland Health, 2014), as the process was seen as secretive, and would frequently produce recommendations that were difficult to reconcile with available information from both a clinician and management perspective. They also appeared to be out of step with the philosophy of RJC that emphasises engagement of all stakeholders, including clinicians and consumers’ families. However, it is recognised that there will be some instances where a process involving a fully independent team with legislative protections will be more desirable. These are now rare instances and would include events surrounded by particular political or media sensitivities.
Activities outlined in Table 2 describe the approach towards responding to critical incidents that has been implemented at GCMHSS, aligned with the principles of RJC.
Responding to incidents using an RJC framework.
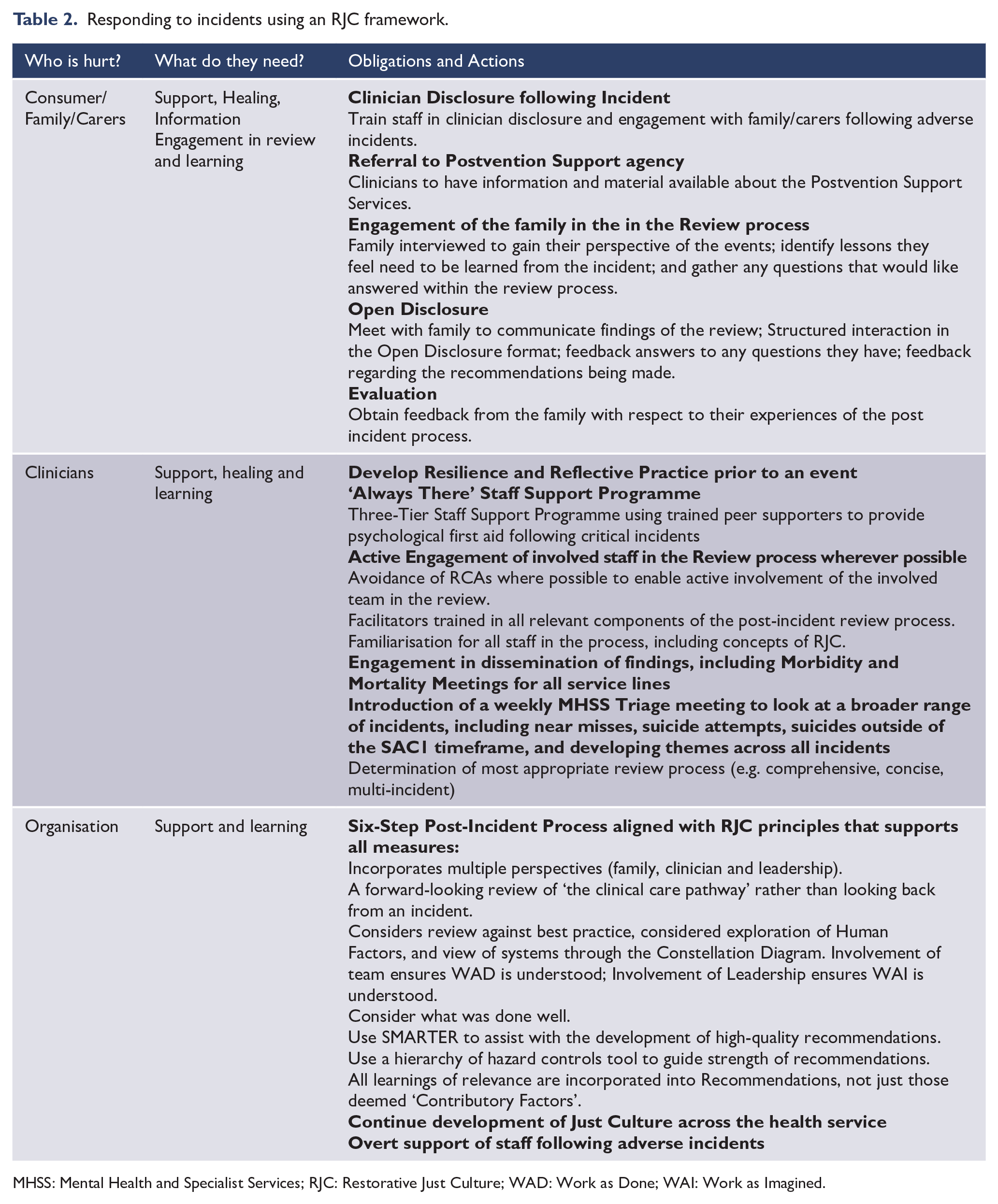
MHSS: Mental Health and Specialist Services; RJC: Restorative Just Culture; WAD: Work as Done; WAI: Work as Imagined.
Conclusion
Despite the recognition that just culture needs to be a key consideration in ensuring patient safety, organisations have struggled to move from cultures of blame (Khatri et al., 2009). In mental health care, in addition to the risk to clinician welfare, a culture of blame can lead to risk aversion, increasing restrictive practices, and failure to work within a recovery paradigm.
RJC, as a foundation to a ZSF, can counteract the risk of blame culture and system anxiety following a critical incident. It provides an ideal framework that can build trust among staff to adopt a bold goal and aspirational challenge of zero suicide by creating an environment in which all stakeholders involved in an incident can feel safe to be open to learning and improving care systems. RJC also provides a framework that mandates the involvement of all parties, so that the complexities of the work can begin to be understood and appropriate learnings made. It provides tools to assist in mitigating against the old paradigms that relied on the fallacies of risk prediction, and outcome and hindsight bias. Equally important, it helps to overcome pessimism and nihilism with respect to our ability to learn from, and prevent, suicides. Involvement of all stakeholders also fosters greater engagement in the improvement process, resulting in a safer system for all, and facilitating healing, learning and improvement for all.
The authors argue that there is an urgent need for greater recognition and understanding of the concepts of RJC, given the adoption of the ZSF across 11 health services in Queensland, Australia, following its successful implementation at Gold Coast Health, and the recent announcement by the New South Wales government of their adoption of a Zero Suicides in Care framework (Mental Health Commission of NSW, 2018).
On the balance of evidence, a change towards RJC and active support of healthcare staff is imperative for a systems approach to suicide prevention to succeed within a hospital and health service. Leaders at a national, state and local level have accountability for addressing these cultural changes as a matter of priority, not only because healthcare workers are already overrepresented in suicide statistics (Milner et al., 2013; Tramutola, 2015), but also because, as has been outlined, this is a vital patient safety issue. A Zero Suicide aspiration not only supports the accommodation of RJC but demands it as a necessary accompaniment to ensure healing, learning and improvement for all.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.