
Abstract
Background:
The need to understand and respond to the unique characteristics and drivers of suicidal behaviour in rural areas has been enabled through the Australian Government’s 2015 mental health reforms facilitating a move to an evidence-based, regional approach to suicide prevention. However, a key challenge has been the complex decision-making environment and lack of appropriate tools to facilitate the use of evidence, data and expert knowledge in a way that can inform contextually appropriate strategies that will deliver the greatest impact. This paper reports the co-development of an advanced decision support tool that enables regional decision makers to explore the likely impacts of their decisions before implementing them in the real world.
Methods:
A system dynamics model for the rural and remote population catchment of Western New South Wales was developed. The model was based on defined pathways to mental health care and suicidal behaviour and reproduced historic trends in the incidence of attempted suicide (self-harm hospitalisations) and suicide deaths in the region. A series of intervention scenarios were investigated to forecast their impact on suicidal behaviour over a 10-year period.
Results:
Post-suicide attempt assertive aftercare was forecast to deliver the greatest impact, reducing the numbers of self-harm hospitalisations and suicide deaths by 5.65% (95% interval, 4.87−6.42%) and 5.45% (4.68−6.22%), respectively. Reductions were also projected for community support programs (self-harm hospitalisations: 2.83%, 95% interval 2.23−3.46%; suicide deaths: 4.38%, 95% interval 3.78−5.00%). Some scenarios produced unintuitive impacts or effect sizes that were significantly lower than what has been anticipated under the traditional evidence-based approach to suicide prevention and provide an opportunity for learning.
Conclusion:
Systems modelling and simulation offers significant potential for regional decision makers to better understand and respond to the unique characteristics and drivers of suicidal behaviour in their catchments and more effectively allocate limited health resources.
Keywords
Introduction
In Australia, the rates of self-harm and suicide increase with remoteness, with those living in combined remote and very remote areas being 2.0 times as likely to die by suicide (age-standardised rate of 21.4 per 100,000 population) compared to those living in major cities (age-standardised rate of 10.5 per 100,000 population) (Australian Institute of Health and Welfare, 2019). A range of explanatory factors have been proposed to account for the increased rates of suicide in rural and remote areas, including socioeconomic circumstances (Taylor et al., 2005); changing climatic conditions such as drought (Hanigan et al., 2018); higher proportions of populations known to be at increased risk of suicidal behaviours (e.g. Aboriginal and Torres Strait Islander Australians) (Kolves et al., 2015; Procter, 2005); increased access to lethal means of suicide such as firearms (Burnley, 1995; Klieve et al., 2009; Taylor et al., 2005); low population density, higher rates of migration and eroded social infrastructure that contribute to social isolation (Hirsch, 2006); heightened stigma of mental illness (Hirsch, 2006); and lower rates of mental health service access or utilisation (Caldwell et al., 2004; Taylor et al., 2005).
The need to understand and respond to the unique characteristics and drivers of suicidal behaviour in rural areas and leverage positive dimensions of rural life (such as increased civic participation and volunteering, social cohesion and informal community support networks) (Ziersch et al., 2009), has been enhanced through the Australian Government’s establishment of 31 Primary Health Networks (PHNs) across the country in 2015 (Department of Health, Australian Government, 2015; National Mental Health Commission, 2014; The Department of Health, 2016). These not-for-profit organisations have responsibilities to undertake needs analysis, planning, coordination and commissioning of primary health care services and supports across their designated region. Although PHNs do not directly deliver services, they are provided with funding to contract other organisations to deliver initiatives, including mental health and suicide prevention programmes, in accordance with local population needs, contexts and priorities. This approach facilitates a balance between national leadership and regional variation through a flexible funding stream to facilitate the commissioning of programmes that meet the unique and diverse needs of communities as well as fostering collaboration among local stakeholders. However, a recent Australian Government Senate Inquiry into the accessibility and quality of mental health services in rural and remote Australia highlighted wide variation in the effectiveness of the PHN-based approach in improving service access and delivery, citing challenges arising from funding insecurity, resource allocation, re-allocation and programme turnover, a lack of workforce capacity and variation in training, supervision and retention rates (Community Affairs Reference Committee, 2018). Added to these challenges are the vast array of suicide prevention interventions that are available, supported variably by the evidence (Kõlves et al., 2012; Krysinska et al., 2016; Ridani et al., 2016; Robinson et al., 2018) and differing expert, local and national views on the efficacy of alternative suicide prevention strategies. Moreover, PHNs can experience intense lobbying and influence from various professional, service provider and community actors vying for funding and/or the delivery of one service model in preference of others. Challenging decision-making environments such as these often give rise to comprehensive approaches that spread limited resources across too broad a range of programmes and services, diluting their potential impact (Atkinson et al., 2015). Without the appropriate decision support tools to guide effective, targeted investments to reduce suicidal behaviours, the significant potential of the regional approach to suicide prevention will not be realised and the Australian Government’s 2015 reforms run the risk of further exacerbating the already crowded, fragmented, difficult to navigate and complex environment of mental health systems in this country.
Applications of systems modelling and simulation to provide decision support capability in addressing complex and persistent public health problems have demonstrated their utility (Atkinson et al., 2018, 2019a, 2019b; Loyo et al., 2013; Page et al., 2017, 2018b; Roberts et al., 2019). These tools combine local and expert knowledge with best available data and the body of research evidence, and have the unique feature of being able to capture population and demographic dynamics, changes over time in behavioural drivers, service interactions and workforce capacity and the potentially non-additive effects of intervention combinations. The final product is an interactive decision support tool that enables regional decision-makers and their stakeholders to explore the likely impacts of intervention combinations before implementation in the real world.
This study was conducted as part of a national evaluation of a key element of the Australian Government 2015 reforms; namely the National Suicide Prevention Trial, a major initiative that involves 11 PHNs taking a systems-based approach to commissioning enhanced services for people at risk of suicide. This study describes the development and application of systems modelling and simulation undertaken as a research-practice partnership between a rural PHN and several academic institutions. The study aimed to identify (1) the likely impact over time of a range of locally prioritised interventions being considered for commissioning and (2) the interaction between interventions that generate service demand, those that increase service capacity, and the impact of this interaction on self-harm hospitalisations and suicide deaths in Western NSW PHN population catchment over the 10-year period 2021–2030.
Methods
Context
Western NSW PHN supports a population of 307,402 (as at 2016), distributed over a geographic area of approximately 433,379 square kilometres (Department of Health, Australian Government, 2018). Nearly 1 in 10 people in the Western NSW PHN catchment (9.1%) reside in Level 2 Statistical Areas (SA2s) classified as remote or very remote (Australian Bureau of Statistics, 2016), and approximately one third of the population (33.9%) lives in SA2s that are socio-economically disadvantaged (with Index of Relative Socio-Economic Disadvantage scores in the lowest quintile for NSW (Australian Bureau of Statistics, 2018). Aboriginal and Torres Strait Islander Australians comprise a substantial proportion of the population (11.6%, compared to 3.0% of the NSW population), while the proportion of the population born overseas is comparatively low (6.3% versus 25.7% for NSW) (Hopkins et al., 2017). From 2011 to 2015, the mean annual age-standardised suicide rate for Western NSW PHN (11.5 per 100,000 population) was higher than that for the NSW population (9.8 per 100,000), but is the same as the national estimate (Public Health Information Development Unit, 2019).
Model development
The system dynamics model presented here is based on a similar model recently developed for Western Sydney PHN using a participatory modelling approach that involved diverse stakeholders, including representatives from health and social policy agencies, local government, non-government organisations, primary care providers, emergency services, research institutions, community groups and people with lived experience of suicide (Page et al., 2018a). The Western Sydney model was adapted to the Western NSW context in consultation with Western NSW PHN staff to ensure that the model structure, assumptions and outputs aligned with the local context and policy priorities. Parameter estimates and other numerical inputs were derived (where possible) from published research or publicly available data or were estimated via constrained optimisation (see below and Supplementary Material). Model construction and analysis were performed using Stella Architect ver. 1.8.3 (www.iseesystems.com).
Model structure, outputs and calibration
The core model structure included (1) a population component, capturing changes over time in the size of the population resulting from births, migration and mortality; (2) a psychological distress component that models flows of people to and from states of low psychological distress (Kessler 10 [K10] score 10−15), vulnerable due to socio-economic disadvantage but not distressed (K10 score 10−15) and moderate to very high psychological distress (K10 score 16−50); (3) a mental health services component that models the movement of psychologically distressed people through one of several possible service pathways involving (potentially) general practitioners, psychiatrists and allied mental health professionals (including psychologists and mental health nurses), psychiatric inpatient care and online services; and (4) a suicidal behaviour component that captures self-harm hospitalisations and suicide deaths. A detailed description of the core model structure is provided in the Supplementary Material.
Primary model outputs included total (cumulative) numbers of self-harm hospitalisations and suicide deaths, and self-harm hospitalisation and suicide rates per 100,000 population. The model also provided estimates of the prevalence of moderate to very high psychological distress, the proportion of the population vulnerable to becoming distressed, and a range of measures of mental health service usage (e.g. mental-health-related general practice consultations, allied mental health services capacity, non-secondary and secondary services waiting times, numbers of psychologically distressed consumers that have disengaged from treatment). All outputs were calculated every 0.4375 days (i.e. one sixteenth of a week) over a period of 20 years, starting from 1 January 2011, permitting comparisons of model outputs with historic data from 2011 to 2017 and forecasts of the impacts of intervention scenarios described below simulated from the time of implementation to the end of 2030 (see Supplementary Material).
Parameter values that could not be derived directly from available data or published research were estimated via constrained optimisation, implemented in Stella Architect ver. 1.8.3, using historical time series data on the prevalence of psychological distress, self-harm hospitalisations and suicide rates and mental-health-related service usage (subsidised general practice consultations and allied mental health services claimed per year, psychiatric bed occupancy). Powell’s method was employed to obtain the set of (optimal) parameter values minimising the sum of the mean absolute percent error calculated for each time series separately (i.e. the mean of the absolute differences between the observed time series values and the corresponding model outputs, where each difference is expressed as a percentage of the observed value).
Policy testing and sensitivity analyses
We modelled the potential impacts on suicidal behaviour of a set of interventions identified by PHN staff as most relevant to the Western NSW context. Interventions were identified based on alignment with current policy priorities, feasibility of implementation and so on and included the following: (1) four specific suicide prevention interventions (post-attempt assertive aftercare, universally applied community support programmes, general practitioner training, suicide helpline services); (2) four mental health interventions (community management of severe mental disorders, mental health education programmes, re-engagement of consumers who have disengaged from treatment, online treatment services); and (3) two services planning interventions (hospital staff training, increasing non-secondary and secondary services capacity). Details of each intervention are provided in the Supplementary Material. Twelve alternative intervention scenarios were compared with a baseline (business as usual) scenario, in which existing policies and programmes remain in place and current per capita mental health service capacity is maintained until the end of the simulation (Table 1).
Suicide prevention and other intervention scenarios examined in the simulation analyses (additional details are provided in the Supplementary Material).
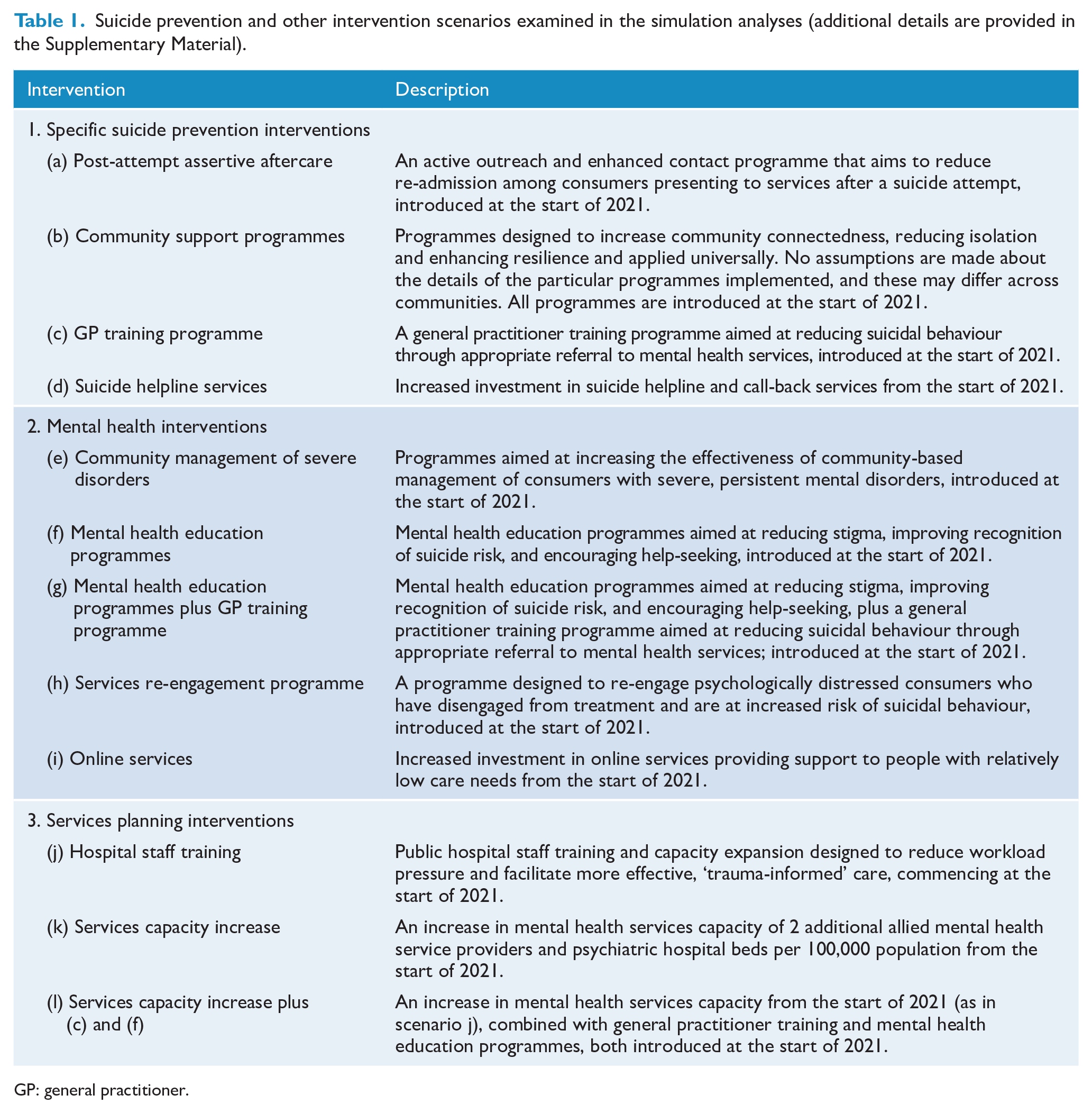
GP: general practitioner.
Sensitivity analyses were performed to assess the impact of uncertainty in estimates of the direct effects of each intervention on the simulation results. This uncertainty includes possible variation in implementation burden that can influence intervention reach, and fidelity to the models of care detailed in the research papers from which the default effects sizes were taken. We used Latin hypercube sampling to draw 100 sets of values for selected model parameters determining the direct effects of the interventions on psychological distress, suicidal behaviour and the movement of consumers through mental health service pathways from a uniform joint distribution spanning +/−20% of the default values (see Supplementary Material). Differences in projected (cumulative) numbers of self-harm hospitalisations and suicide deaths between the baseline and intervention scenarios were calculated for each set of parameter values and summarised using simple descriptive statistics (note that all intervals reported in this paper are derived from the distributions of model outputs calculated in the sensitivity analyses; they provide a measure of the impact of uncertainty in the intervention effect estimates, but should not be interpreted as confidence intervals).
Results
Figure 1 shows the modelled self-harm hospitalisation and suicide rates for the total population under the baseline (business as usual) scenario. Projected rates decline gradually over the forecast period with the self-harm hospitalisation rate decreasing from 105.70 to 90.00 per 100,000 population per year and the suicide rate declining from 12.92 to 10.91 per 100,000 population per year.
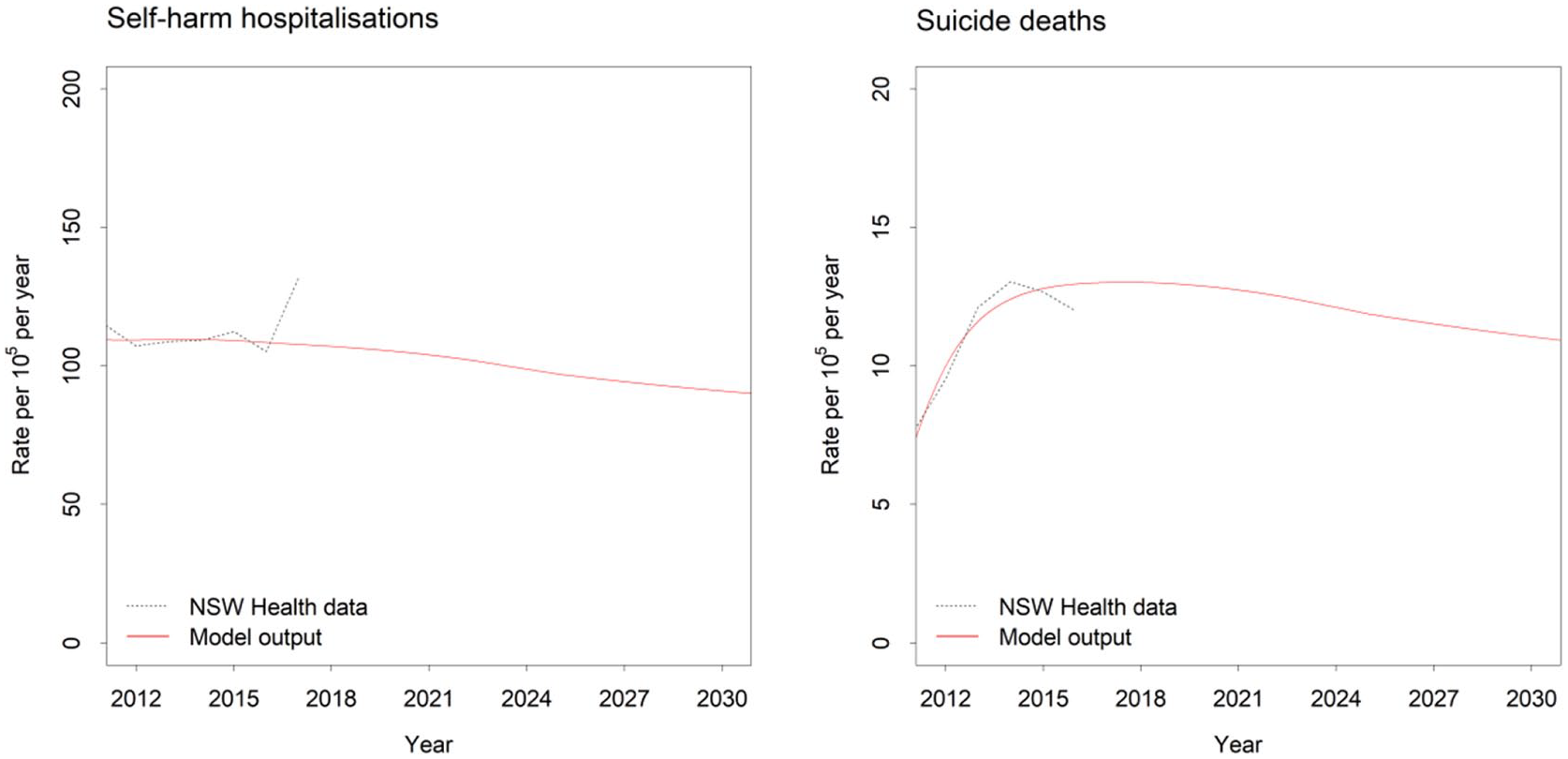
Self-harm hospitalisation and suicide rates (per 100,000 population) for the Western NSW PHN population catchment under the baseline scenario (i.e. business as usual). The dotted grey lines show estimates derived from data published by the NSW Department of Health (see www.healthstats.nsw.gov.au); the solid red lines show the modelled rates.
Under the baseline scenario, a total of 3329 self-harm hospitalisations and 376 suicide deaths were projected over the post-intervention period (1 January 2021 to the end of 2030). Reductions in the numbers of self-harm hospitalisations and suicide deaths relative to these baseline estimates for each intervention scenario are presented in Figures 2 and 3. Post-suicide attempt assertive aftercare had the greatest impact on suicidal behaviour in the total population, reducing the numbers of self-harm hospitalisations and suicide deaths by 5.65% (95% interval, [4.87%−6.42%]) and 5.45% [4.68%−6.22%], respectively. Relatively large reductions in numbers of self-harm hospitalisations and suicide deaths were also projected for community support programmes (self-harm hospitalisations: 2.83%, 95% interval, [2.23%, 3.46%]; suicide deaths: 4.38%, 95% interval [3.78%, 5.00%]) and a treatment re-engagement programme (self-harm hospitalisations: 3.16%, 95% interval, [2.62%−3.70%]; suicide deaths: 3.73%, 95% interval [3.08%−4.37%]).
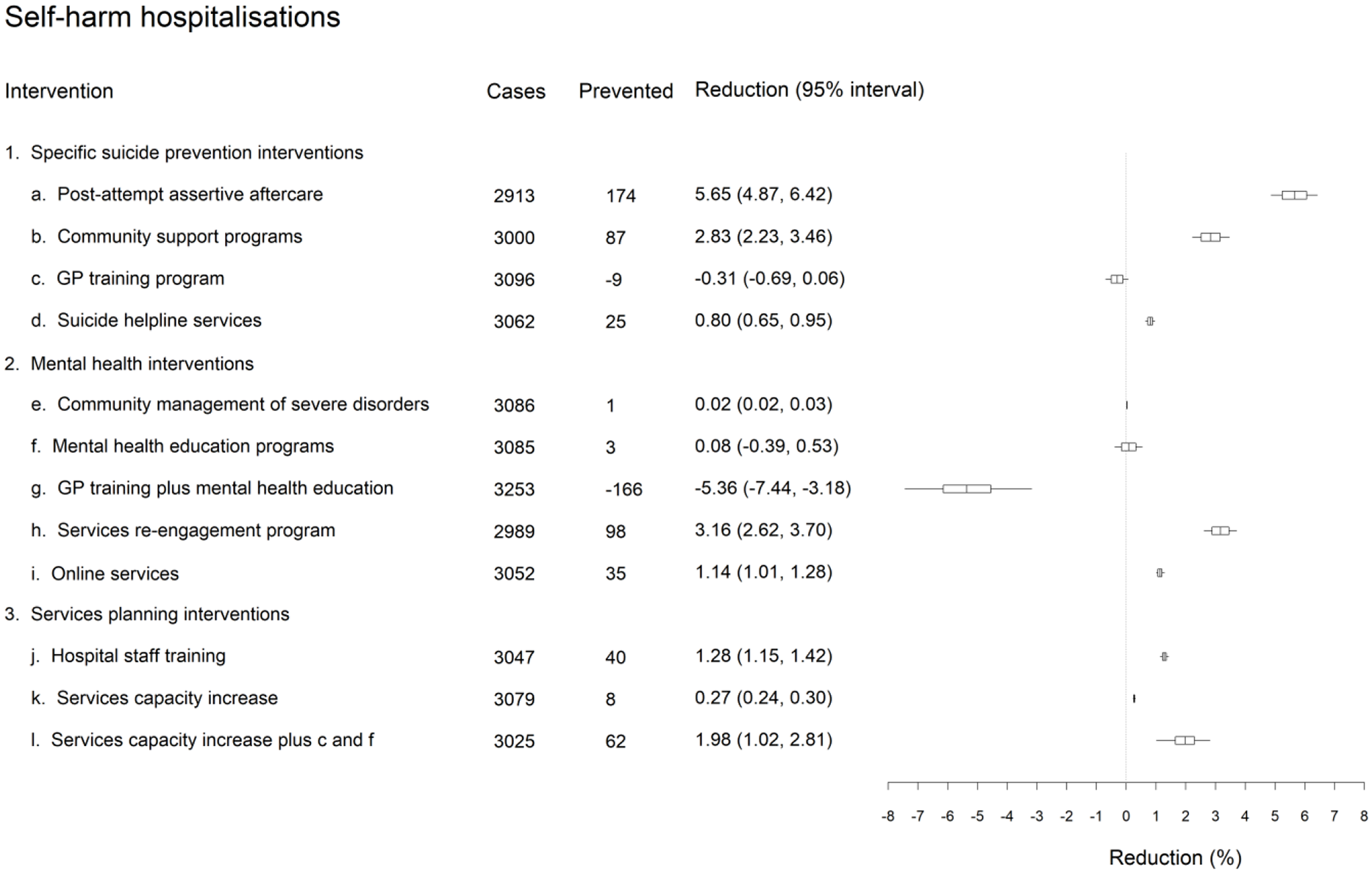
Differences in projected total (cumulative) numbers of self-harm hospitalisations between the business as usual and intervention scenarios over the period 2021−2031. Numbers of cases (i.e. hospitalisations) and cases prevented are rounded to the nearest integer and were obtained assuming the default parameter values. Mean percentage reductions and 95% intervals reported in the rightmost column were derived from the distributions of projected outcomes calculated in the sensitivity analyses (note that the 95% intervals provide a measure of the impact of uncertainty in the assumed intervention effects but should not be interpreted as confidence intervals). The plot on the right shows the mean reductions and 50% and 95% intervals.
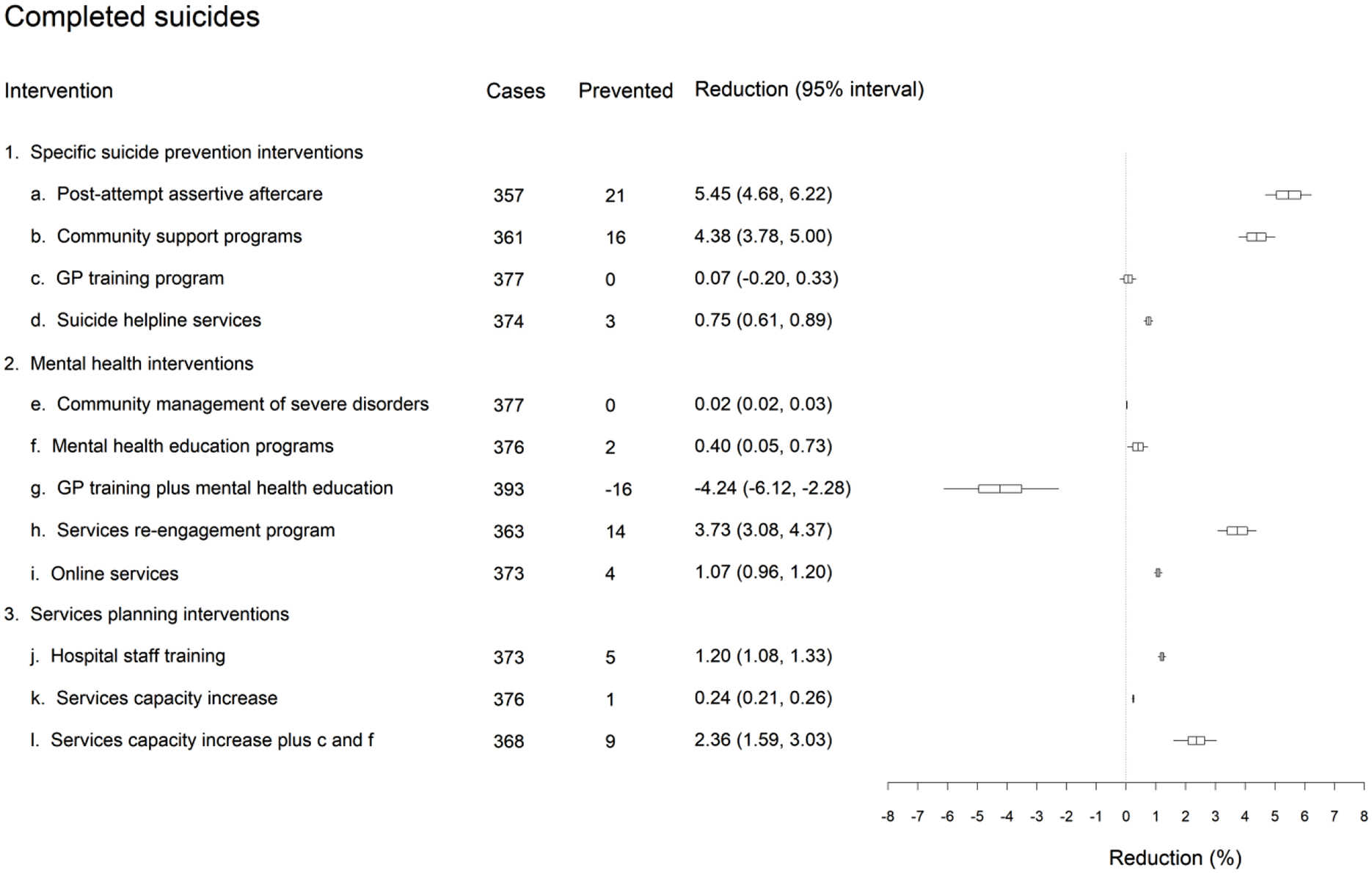
Differences in projected total (cumulative) numbers of suicide deaths between the business as usual and intervention scenarios over the period 2021−2031. Numbers of cases (i.e. suicides) and cases prevented are rounded to the nearest integer and were obtained assuming the default parameter values. Mean percentage reductions and 95% intervals reported in the rightmost column were derived from the distributions of projected outcomes calculated in the sensitivity analyses (note that the 95% intervals provide a measure of the impact of uncertainty in the assumed intervention effects but should not be interpreted as confidence intervals). The plot on the right shows the mean reductions and 50% and 95% intervals.
Hospital staff training and increased investment in online treatment and suicide helpline services all had a very modest impact on suicidal behaviour, reducing projected numbers of self-harm hospitalisations and suicide deaths by 0.80−1.28% and 0.75−1.20%, respectively (see Figures 2 and 3). Service capacity increases alone had little effect on suicidal behaviour (self-harm hospitalisations: 0.27%, 95% interval, [0.24%, 0.30%]; suicide deaths: 0.24%, 95% interval, [0.21%, 0.26%]). Surprisingly, general practitioner training combined with mental health education programmes increased suicidal behaviour (self-harm hospitalisations: -5.36%, 95% interval, [-7.44%, -3.18%]; suicide deaths: -4.24%, 95% interval, [-6.12%, -2.28%]). However, when service capacity increases were combined with general practitioner training and mental health education programmes, moderate reductions in projected numbers of self-harm hospitalisations and suicides were observed (self-harm hospitalisations: 1.98%, 95% interval, [1.02%, 2.81%]; suicide deaths: 2.36%, 95% interval, [1.59%, 3.03%]). Programmes aimed at improving community-based management of severe mental illness have minimal impact on numbers of self-harm hospitalisations and suicide deaths in the total population, due partly to the relatively low prevalence of severe mental disorders (estimated to be 4.1%) (Slade et al., 2009).
Discussion
This study used systems modelling and simulation to undertake a priori testing of the likely impact of prioritised interventions for a rural PHN catchment. Of the intervention scenarios examined, post-suicide attempt assertive aftercare was the single most effective intervention in reducing suicidal behaviour across the total population over the next 10 years, followed closely by universally applied community support programmes and a programme aimed at re-engaging those known to the mental health system but lost to follow-up. While only the broad strategy of achieving re-engagement of those lost to follow-up was modelled here, there is a potential role for the use of technology in the specific implementation of this intervention to ensure services remain more effectively connected with individuals who have previously made contact with mental health services. The relatively large forecasted impacts of community support programmes are congruous with studies highlighting social isolation as an important contributor to suicide (Dorling and Gunnell, 2003; Siahpush and Singh, 1999). The decision support tool provided through this action research has not only contributed to making a stronger case for investment in community support programmes, it has provided this case in the context of its estimated impact over the next decade compared to a suite of other commonly prioritised strategies such as increasing mental health service capacity. While the forecasted impacts of some interventions were unsurprising, others were initially unintuitive and delivered results that were significantly less than what is being anticipated under the evidence-based approach to suicide prevention being trialled across Australia (Black Dog Institute, 2015, 2018; Krysinska et al., 2016), and hence provides an opportunity for learning.
Based on evidence provided by a randomised, controlled trial conducted in an island district of Copenhagen, Denmark with an urban population (Hvid et al., 2011), and estimated using the traditional Population Preventable Fraction (PPF) method (Rockhill et al., 1998), assertive aftercare is expected to deliver a 19.8% reduction in suicide attempts in Australia (Black Dog Institute, 2015; Krysinska et al., 2016). This estimate is more than three times higher than the impact forecasted by the system dynamics model for the rural catchment of Western NSW. In addition, based on an evaluation of a medical education programme for general physicians (GPs) on depression implemented in a primarily rural county of Sweden (Henriksson and Isacsson, 2006), GP training as been estimated to deliver a 6.3% reduction in suicides in Australia (Black Dog Institute, 2015; Krysinska et al., 2016). This estimate of impact is significantly higher than the negligible impact of GP training forecasted by the system dynamics model of Western NSW, and even when coupled with population-based mental health education and service capacity increases the forecast impact on suicide deaths for the Western NSW catchment remains almost two thirds lower than the estimate derived from the PPF method.
While estimates of impact at a national level are not necessarily indicative of regional-level effects, findings such as a lack of impact of GP training unless coupled with other interventions and the synergistic effects of certain intervention combinations suggest that the discrepancy in anticipated impacts are better explained by the difference in methods applied. The static, linear approach of application of the PPF method has been shown provide unrealistic estimates of impact of interventions when applied to complex systems (Page et al., 2018b). This is because each of the parameters used in the calculation of the preventive fraction is likely to change over time, as a function of demography, behavioural factors, contextual factors and health service quality and availability (Page et al., 2018b). In contrast, systems modelling and simulation can capture such complexity and account for real-world sources of inertia and delay, feedback loops (i.e. vicious and virtuous cycles), contextually specific interactions between service demand and supply, implementation challenges in resource-constrained environments and varying intervention effects over time (Page et al., 2018b; Sterman, 2006).
The surprising, unintended increase in suicidal behaviour generated by implementing general practitioner training combined with mental health education programmes provided an opportunity for learning about likely system behaviour in the Western NSW region. Interrogation of the model revealed that this intervention combination generated mental health service demand beyond the availability of baseline service capacity, driving increases in the rate at which patients disengage from services as a result of increases in mean wait times and dissatisfaction with the quality of care they receive. In the model, disengagement from the mental health care system is assumed to increase the risk of suicidal behaviour (due to a loss of hope that effective treatment is available, or trauma associated with inadequate care), so that an increase in the disengagement rate leads to the unintended increase in self-harm hospitalisation and suicide death rates. Similarly, service capacity increases on their own beyond baseline service demand will have little impact (as results demonstrate). However, the results highlight the extent to which building mental health service capacity ahead of implementing interventions that increase service demand has synergistic effects in reducing suicidal behaviour.
Exploration of such supply versus demand dynamics in a population catchment are exceedingly difficult with the application of static, linear analytic approaches and mental models alone. The systems modelling and simulation approach provides valuable decision support capability that can help avoid unintended consequences, inform the timing and scaling of interventions, and realise the full potential of evidence-based interventions. The complexity of mental health service planning and suicide prevention at the regional level presents challenges (both analytically and politically) that demand sophisticated, transparent and interactive decision support tools that will support a more disciplined, strategic approach to the allocation of limited resources, will help manage expectations with regards to the size, nature and timing of intervention effects, and facilitate the navigation of effective partnerships to achieve aligned collective action across local stakeholder groups.
Limitations
There are a number of limitations that require consideration when interpreting the findings of this study. There is potential measurement bias in the range of secondary data used to parameterise the model including the NSW population health survey, Medicare Benefits Schedule, PHN and Local Health District (LHD) datasets and the Australian Bureau of Statistics (ABS); and, these data vary considerably in quality. The model acknowledges these potential sources of measurement bias, and a number of commonly used strategies were employed to address them, including the triangulation of multiple data sources, parameter estimation via constrained optimisation, and local verification to identify plausible estimates.
In addition, there is potentially an under-enumeration of suicide cases used to calibrate the model, due to the misclassification of suicides to International Classification of Diseases (ICD) codes relating to unintentional injury and events of ‘undetermined intent’ (Harison et al., 2009). In addition, hospital suicide attempts (from hospital admissions) likely only capture those cases serious enough to warrant medical intervention and instances of self-harm where the intent wasn’t clear may be not coded as suicide attempts; hence, potentially under-enumerating the total population burden of attempted suicide in the population catchment. However, these limitations were consistent across simulations of the baseline case and intervention scenarios and as such are unlikely to affect the forecast estimates of impact (i.e. the % reduction in suicidal behaviour) of intervention strategies or the strategic insights derived from the model. As intervention effect sizes are subject to the population, demographic, behavioural, and service dynamics of the modelled region, they should not be considered generalisable to other regions. However, qualitative insights regarding system behaviour, for example, the importance of the supply–demand dynamics in influencing the outcomes strategies to reduce suicide have broader relevance to regional commissioning of suicide prevention initiatives.
Strengths
The findings reported in the current study represent a set of intervention scenarios deemed a priority for informing the next round of commissioning of programmes and services to reduce suicidal behaviour in the rural and remote population catchment of Western NSW. The prioritised programmes and services do not represent the full scope of potentially effective strategies to reduce suicidal behaviour in the region. However, the model can be updated and expanded to include additional initiatives based on interest or new evidence that becomes available, making it a longer-term decision support asset. Within the current model, there is also scope to investigate alternative scenarios related to the timing of implementation of interventions, their scale and intensity, alternative assumptions of level of participation and uptake, and alternative combinations to provide further insights to support local stakeholder engagement and implementation of the suicide prevention strategy. Embedded in a monitoring and evaluation cycle, such models can be used to iteratively determine the extent to which the modelling corresponds with real-world outcomes over time and how implementation strategies can be enhanced to improve performance. Information from monitoring and evaluation activities can also be used to refine model parameters to improve its forecast capabilities and guide subsequent decision-making in a timely and proactive way.
Conclusion
Suicide is a complex phenomenon driven by a range of demographic, behavioural, contextual, socio-cultural and health service factors. Efforts to reduce suicide over the past decade through reforms aimed at making services and preventive interventions more effective, efficient and culturally and contextually appropriate, have not delivered the anticipated impacts. The new reforms focus on a renewed regional approach to suicide prevention. Their success will depend on the ability of PHNs to understand and respond to the unique characteristics and drivers of suicidal behaviour in their catchments, their ability to foster collaboration among local stakeholders to support implementation, and access to leading advances in decision analytic tools and methods that will help them navigate the challenging decision-making environment in which they operate. Dynamic systems modelling and simulation is unhindered by the constraints of static, linear analytic approaches and is able to bring together the many pieces of a complex puzzle in a given context, including determinants and pathways to suicidal behaviour, dynamics of service needs and supply, barriers and facilitators of access to care, and intervention effects, and deliver new insights for decision makers and their stakeholders. The interactive nature of the decision support tool enables regional decision makers and their stakeholders to explore the likely impacts of their commissioning strategies before implementation in the real world, an approach that offers significant potential for the more effective use of limited health resources.
Supplemental Material
Supplementary_Material – Supplemental material for Systems modelling and simulation to inform strategic decision making for suicide prevention in rural New South Wales (Australia)
Supplemental material, Supplementary_Material for Systems modelling and simulation to inform strategic decision making for suicide prevention in rural New South Wales (Australia) by Jo-An Atkinson, Adam Skinner, Sue Hackney, Linda Mason, Mark Heffernan, Dianne Currier, Kylie King and Jane Pirkis in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This model was developed by the Sax Institute in partnership with Western NSW Primary Health Network, Western Sydney University and The University of Melbourne. Importantly, this work was made possible by generous contributions of time, local knowledge, data and content area expertise by Professor Andrew Page (Translational Health Research Institute, Western Sydney University), Western NSW PHN staff, the Western NSW Health Intelligence Unit, Western NSW Local Health District and Far West Local Health District.
Author Contributions
Manuscript concept and drafting: J.A. and A.S.; model development: A.S.; data analysis: A.S. and J.A.; critical revision of manuscript for important intellectual content: all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This decision support tool was developed as a part of the National Suicide Prevention Trial Evaluation funded by the Commonwealth Department of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.