
Abstract
Objective:
Personal Health Budget has been provided to consumers with severe mental illness within a policy shift toward a person-tailored mental healthcare treatment based on individual unmet needs. Evidence of beneficial effects of Personal Health Budget is still scarce. The aim of this study was to provide preliminary data on clinical and social benefits of adding Personal Health Budget to a standard pharmacotherapy in patients with severe mental illness across a 24-month follow-up period.
Methods:
Participants (n = 137) were individuals with severe mental illness, aged 18–50 years, recruited in one of the adult mental health services of the Parma Department of Mental Health. They completed the Global Assessment of Functioning scale, the Health of the Nation Outcome Scale and the Brief Psychiatric Rating Scale. This age range was chosen to limit Personal Health Budget interventions to adults with a non-prolonged illness duration. Friedman’s test for repeated measure was used to assess the longitudinal stability of functioning and clinical parameters. A linear regression analysis was also performed.
Results:
A significant decrease in all Global Assessment of Functioning scale, Health of the Nation Outcome Scale and Brief Psychiatric Rating Scale scores along the 24 months of follow-up was observed. Regression analysis results specifically showed a relevant association between a Personal Health Budget multiaxial intervention and the longitudinal reduction in Brief Psychiatric Rating Scale ‘Negative Symptoms’ and Health of the Nation Outcome Scale ‘Social Problems’ subscores.
Conclusion:
Our findings support the useful implementation of a Health of the Nation Outcome Scale approach for severe mental illness patients within the Italian mental health service network.
Keywords
Introduction
In recent years, welfare systems in Western societies implemented mental health services increasingly centered on individual unmet needs and local caring community, also due to the public resource scarcity and the consequent renewal toward healthcare intervention effectiveness (Tyrer et al., 2017). In this context, new mental healthcare practices gradually developed in Europe, most of which implementing a new network-based welfare system consisting of an increased harmonization of resources jointly made available by public health services, patient, family members and local community agencies (Wirrmann Gadsby, 2013). Since the 1990s, in order to promote more ‘person-tailored’ healthcare programs for individuals with severe mental illness (SMI), such rehabilitation approaches concretely translated into a reduction in intensive treatments in favor of long-term care interventions at home, within the local community (Davidson et al., 2013).
Personal Health Budget
The ‘Personal Health Budget’ (PHB) has been proposed as an innovative rehabilitation model consisting of cumulative person-centered funds expressly aimed at strengthening individual health, as well as social and personal needs (Wirrmann Gadsby, 2013). The PHB is a contract-like, commitment agreement between patients, their family members and the social/healthcare services involved in their care pathway in order to achieve social inclusion and to make them empowered, self-determined ‘service integrators’ who can generate and manage the support they need (Davidson et al., 2013). Depending on the legal frame of the country concerned, PHB can be either directly provided as monetary support and payment or (like in Italy) offered via indirect budget, made available to the patient by third parties (e.g. family members, healthcare and/or social services) within a person-tailored rehabilitation intervention whose primary goals can be reached only through the mutual cooperation and coordination of all parties involved.
PHB: the Italian model
Italy approved a crucial mental health reform law in 1978, which led to the very closure of all psychiatric hospitals over the following two decades. For a more complete execution of this reform, the Italian welfare system has gradually moved from an ‘institution-based’ healthcare model (with growing costs for the society) (Ceccherini-Nelli and Priebe, 2007) to a ‘community-based’ service model, aimed at enhancing the patient’s point of view (his strengths/needs) and to be realized within the belonging community. In this context, some Italian mental health departments introduced the PHB as a crucial part of the patients’ ‘Individual Rehabilitation Plan’ (IRP) to implement their social inclusion, despite they being affected by SMI that usually required a remarkable rehabilitation support combining both healthcare and social interventions.
In the Italian context, the PHB is composed of family, individual, social and healthcare resources (both economic and human or/and technological), collected together to avoid/prevent SMI relapses and chronic low functioning and to counteract patients’ isolation and stigma. It was originally developed either to allow patients’ discharge from psychiatric facilities (rehabilitative purpose) or to avoid/delay patients’ new residential admissions (preventive purpose) (Webber et al., 2014). However, PHB has gained more ambitious aims over time, such as focusing specific interventions on patients’ disorder in order to prevent the most vulnerable people from being isolated in their native communities (Jones et al., 2013).
The 2015 Emilia-Romagna Regional Council Deliberation Act n.1554 (‘Guidelines for the implementation of individual pathway to care through the PHB methodology application’) (Regione Emilia Romagna [RER], 2016) has officially started PHB implementation in all the regional mental health departments. However, since 2001 the Parma Department of Mental Health and Pathological Addiction introduced innovative person-centered rehabilitation pathways that, although designated by other names, were configured as PHB interventions (i.e. supporting housing, employment and social participation). A simple perspective, observational evaluation performed after the first 5 years of the implementation of such specific rehabilitation interventions revealed that a significant reduction in hospital admissions (with subsequent life quality improvement) occurred in 70% of SMI patients who had received PHB-like treatments (Leuci et al., 2020).
To date, within the Parma Department of Mental Health, the PHB intervention has electively been offered as an integrated (social and healthcare) treatment for people with SMI, aimed at improving their clinical, personal and functional recovery, as well as their social inclusion and active participation in the native community through the activation of specific and person-tailored rehabilitation programs (Slasberg et al., 2014; Wacker, 2009).
Aim of this study was thus twofold: (a) to offer a general description of the Italian PHB methodology implemented in the Parma Department of Mental Health since 2016 and (b) to provide preliminary data on the beneficial effects of such PHB intervention in adults with SMI. Specifically, we compared functional and clinical outcome indicators across a 2-year follow-up period. Main hypothesis of the present research was that positive outcomes could be obtained in terms of socio-occupational functioning and clinical recovery, thanks to the PHB approach application.
Methods
Participants and setting
Data were retrospectively collected at baseline and at the follow-up routine assessments of patients with SMI recruited in one of the six adult mental health services of the Parma Department of Mental Health from January 2016 to December 2018. Participants were recruited only in community-based mental health settings (i.e. inpatients were not included). They were potentially enrolled at any point during their care, although the Parma Department of Mental Health explicitly indicated preferring SMI consumers with early illness episodes. Baseline assessments thus corresponded to PHB intervention entry.
All participants (n = 137) agreed to participate in the research and gave their written informed consent prior to their inclusion in the study. Local relevant ethical approval was obtained for the research (AVEN Ethics Committee: protocol no. 36102/09.09.2019). This study has been also carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for medical research. The data that support the findings of this research are available on request from the corresponding author. The data are not publicly available due to privacy/ethical restrictions.
For the purpose of this study, inclusion criteria were (a) age between 18 and 50 years; (b) presence of SMI within one of the following psychiatric diagnoses as defined in accordance with the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revised (DSM-IV-TR) (American Psychiatric Association [APA], 2000): schizophrenia or other psychotic disorders, and affective psychosis (i.e. bipolar disorder with psychotic features and major depressive disorder with psychotic features); and (c) a Global Assessment of Functioning (GAF) score (APA, 2000) ⩽50. Specifically, according to the Substance Abuse and Mental Health Services Administration (2015), we considered an SMI as a ‘diagnosable mental, behavioral or emotional disorder causing serious functioning impairment that substantially interferes with or limits one or more major life activities’ (primarily affecting employment, sociality and housing) and mainly includes bipolar disorders, major depression, schizophrenia and other psychosis, which often have poorer access to health care services and worse health outcomes than the general population (Goldman et al., 2018). Precisely, we included such diagnoses because psychotic symptoms are usually associated with a greater socio-occupational functioning decline and a poorer prognosis (Hunt et al., 2019).
Exclusion criteria were (a) current substance abuse/dependence, according to the DSM-IV-TR (APA, 2000); (b) known moderate/severe intellectual disability (Intelligence Quotient <50); and (c) neurological disorders, head injury or any other medical condition associated with psychiatric symptoms. SMI individuals with current substance abuse/dependence were excluded in order to create a more clinically homogeneous group of consumers for a first evaluation of the PHB methodology and its potential beneficial effects. As dual diagnosis is relatively common in the SMI population, current substance abuse/dependence will be an inclusion criterion for a future research on the effectiveness of PHB interventions.
Instruments
In the current research, the psychopathological evaluation included the Brief Psychiatric Rating Scale (BPRS)—version 4.0 (Ventura et al., 1993), the GAF scale (APA, 2000) and the Health of the Nation Outcome Scale (HoNOS) (Wing et al., 1999). These psychometric instruments were administered at baseline and repeated after 12 and 24 months of follow-up.
The BPRS—version 4.0—is a clinical interview specifically developed to quickly collect information about the absence/presence and the severity of 24 main psychiatric symptoms, rated on a Likert-type scale ranging from 1 (‘not present’) to 7 ( ‘extremely severe’). According to Dazzi et al. (2016), BPRS items were grouped in a 5-factor model solution including ‘Positive’, ‘Negative’, ‘Affect’, ‘Activation’ and ‘Disorganization’ dimensions. In this study, we used the authorized Italian translation of the BPRS—version 4.0 (Roncone et al., 1999), which showed good psychometric properties in Italian clinical population (Pelizza et al., 2020c).
The GAF is a scale widely used to rate patient’s social, occupational and psychological functioning. Scores range from 100 ( ‘extremely high functioning’) to 1 ( ‘severely impaired functioning’). In this study, we used the Italian version of the GAF scale included in the DSM-IV-TR (Andreoli et al., 2007), previously administered in Italian clinical samples with good psychometric properties (Landi et al., 2020).
The HoNOS was developed to assess improvements in health and social functioning of people with enduring mental health problems (Wing et al., 1999). Structurally, the HoNOS includes 12 items, each one rated on a 4-point Likert-type scale (from 0 = ‘no problem’ to 4 = ‘severe to very severe problems’). A total score was obtained, and subscale scores were calculated by combining groups of items as follows: (a) ‘Behavioral Problems’ (items 1–3), (b) ‘Impairment’ (items 4 and 5), (c) ‘Psychiatric Symptoms’ (items 6–8) and (d) ‘Social Problems’ (items 9–12) (Golay et al., 2016). In this study, we used the Italian version of the HoNOS that showed good psychometric properties in Italian clinical population (Ruggeri, 2001).
Procedures
The axis-I diagnosis was made by two trained psychiatrists through the Structured Clinical Interview for DSM-IV-TR axis I disorders (SCID-I) (First et al., 2002).
In the current research, the PHB methodology was proposed as an integration of the standard (‘as usual’) pharmacological intervention usually provided to patients affected by SMI in accordance with the current guidelines (e.g. National Institute for Health and Care Excellence [NICE], 2016, 2020a, 2020b). In particular, the PHB intervention was offered to all SMI subjects with a GAF score ⩽50, also showing a relevant complexity and severe difficulties in the following areas of functioning: housing, employment and/or social participation. Subjects who accepted the PHB proposal were included in the study. As mentioned above, the Italian PHB model was intended as an integrated, person-tailored rehabilitation intervention supporting the IRP of individuals with SMI and consisting of a mixture of social, health, personal and family resources (RER, 2016). Specifically, it was aimed to improve patients’ clinical and functional recovery, as well as their social inclusion and active participation in the native community (Slasberg et al., 2014).
In detail, the qualifying elements of the PHB approach are (a) a Multidimensional Evaluation Unit (MEU), including social and mental health services, defining the IRP and the PHB resources according to the principles of equity and appropriateness, and (b) an IRP (person-tailored and recovery-oriented) based on a careful assessment of the individual abilities and needs (rather than depending on the services’ offer), developed together with the patients, their family members and other local community agencies (such as third-sector cooperatives) (RER, 2016). Specifically, the IRP allows specific rehabilitation interventions within the social areas most affecting people’s health (i.e. housing, sociality, employment) in order to maintain and/or create virtuous connections between community social and healthcare systems through an appropriate use of their economic, technological and human resources.
Within the ‘Housing’ axis, interventions can include actions aimed at supporting life at home or at gaining a new home/accommodation, either individually or in co-housing groups. Depending on patient’s needs, different forms of support are provided, ranging from temporary, active home support (in order to strengthen the autonomy in everyday life) to more prolonged interventions for maintaining good environmental/family conditions. These actions are mainly displayed, thanks to the integration of clinical/rehabilitation treatments (offered by local public mental health services) with social/educational ones (provided by the local social system).
Within the ‘Sociality’ axis, rehabilitation treatments aim at promoting friendship, family relationships and social networks, enhancing the patient’s empowerment and/or the development of social skills. Specifically, interventions have to encourage a positive social identity, stimulating the participation in cultural, relational, recreational and sport activities within the native community. In this process, it is crucial to involve family members, voluntary associations and informal local agencies.
Finally, the ‘Employment’ (Training/Work) intervention axis includes all actions aimed at promoting social inclusion and active participation in the community through training activities and supported employment, also within the Italian legal framework regarding apprenticeships and job placements.
Therefore, PHB resources can include (a) healthcare ones, provided by community (adult-child/adolescent) mental health centers, often relying on social cooperatives; (b) social resources provided by local social services for integration and social inclusion (social workers, educators, public housing, meals at home, financial aids); (c) patients’ resources including both economic and relational ones (family members, friends); and (d) resources coming from local voluntary associations (Figure 1). The IRP must be signed by all the subjects involved in order to make the individual PHB official. Therefore, there is no a priori budget amount, but it is determined and planned on the specific individual unmet needs in the above-mentioned PHB axes. It is not only directly provided as a payment or monetary support (e.g. health/social financial resources allocated for ‘Sociality’ axis and offered as psychosocial interventions disbursed through social cooperatives) but also via indirect budget made available by all the parties involved in the IRP (e.g. the consumers can share their disability benefits, a car to reach a workplace and/or an educational qualification for searching a job; family members may offer a car, a house or a willingness to pay a house rent and the related bills; social services can provide public housing and/or meals at home; mental health services can make available a professional educator for individual rehabilitation or a job searching pathway such as the Individual Placement and Support [IPS]). Each part offers what it can realistically support, taking into account the co-planned PHB goals based on the consumer’s wishes and needs. PHB interventions were updated overtime and monitored every months (through meetings with all the parties involved) in order to be able to redefine the IRP objectives, if necessary. At the moment, SMI consumers receive the PHB resources for a prolonged period not exceeding 2 years (hoping to have achieved a greater functioning and a fuller social integration in the native community during this defined time period).
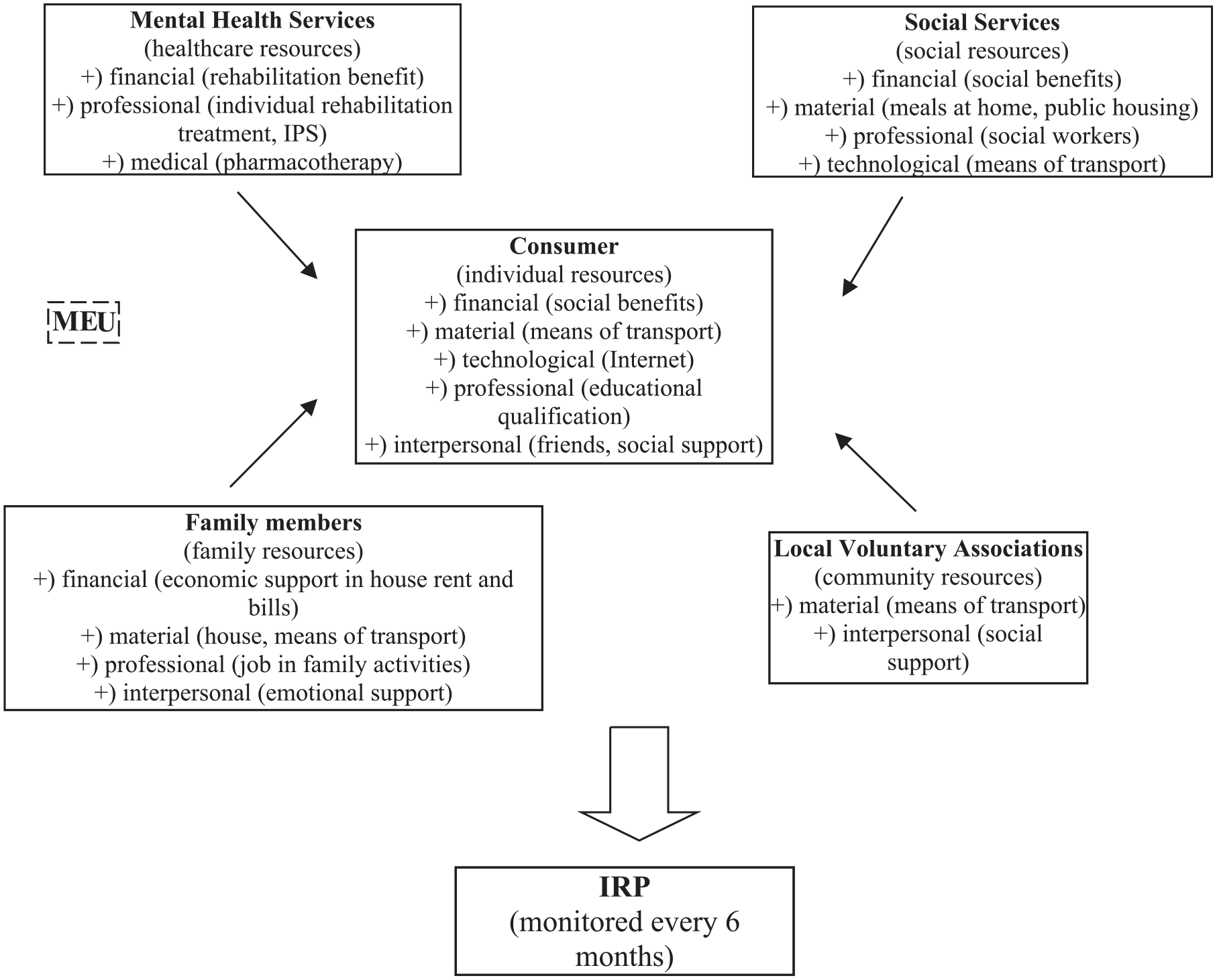
The PHB intervention model in Italy.
As the main aim of the current research was to examine preliminary data about the beneficial effects of the Italian PHB model in adults with SMI, functional and clinical outcome indicators across a 2-year follow-up period were compared.
Statistical analysis
Data were analyzed using the Statistical Package for Social Science (SPSS) for Windows, version 15.0 (SPSS Inc, 2010). All tests were two-tailed with a threshold of significance set at p = 0.05. Frequencies and percentages were used to describe qualitative variables, whereas mean values ± standard deviation were calculated to represent quantitative variables. Due to non-normality in all explorations (i.e. Kolmogorov–Smirnov test with Lilliefors correction: p < 0.05), non-parametric statistics were performed. Specifically, Friedman’s test for repeated measures (and Wilcoxon test with Bonferroni correction as post hoc procedure for multiple comparisons) was used to assess the longitudinal stability of BPRS, HoNOS and GAF scores across the 2-year follow-up period. Finally, a linear regression analysis (with functioning and psychopathological scores as dependent parameters, and PHB intervention [multiaxial vs uniaxial] and daily dose of antipsychotic medication as independent parameters) was also performed.
Results
Over the course of this study, the PHB intervention was consecutively proposed to 150 SMI patients, but only 137 (91.3%) of them (85 [62.0%] males, 94 [68.7%] White Caucasians, mean age at entry = 32.74 ± 11.15 years) agreed and were enrolled in the research (see Table 1 for details on sociodemographic and clinical characteristics). The duration of taking charge within the Community Mental Health Centers (CMHC) (i.e. the time period of treated illness in the community-based setting) was 23.27 ± 12.22 months, suggesting a relatively non-prolonged illness phase.
Sociodemographic and clinical characteristics of the total sample (n = 137).
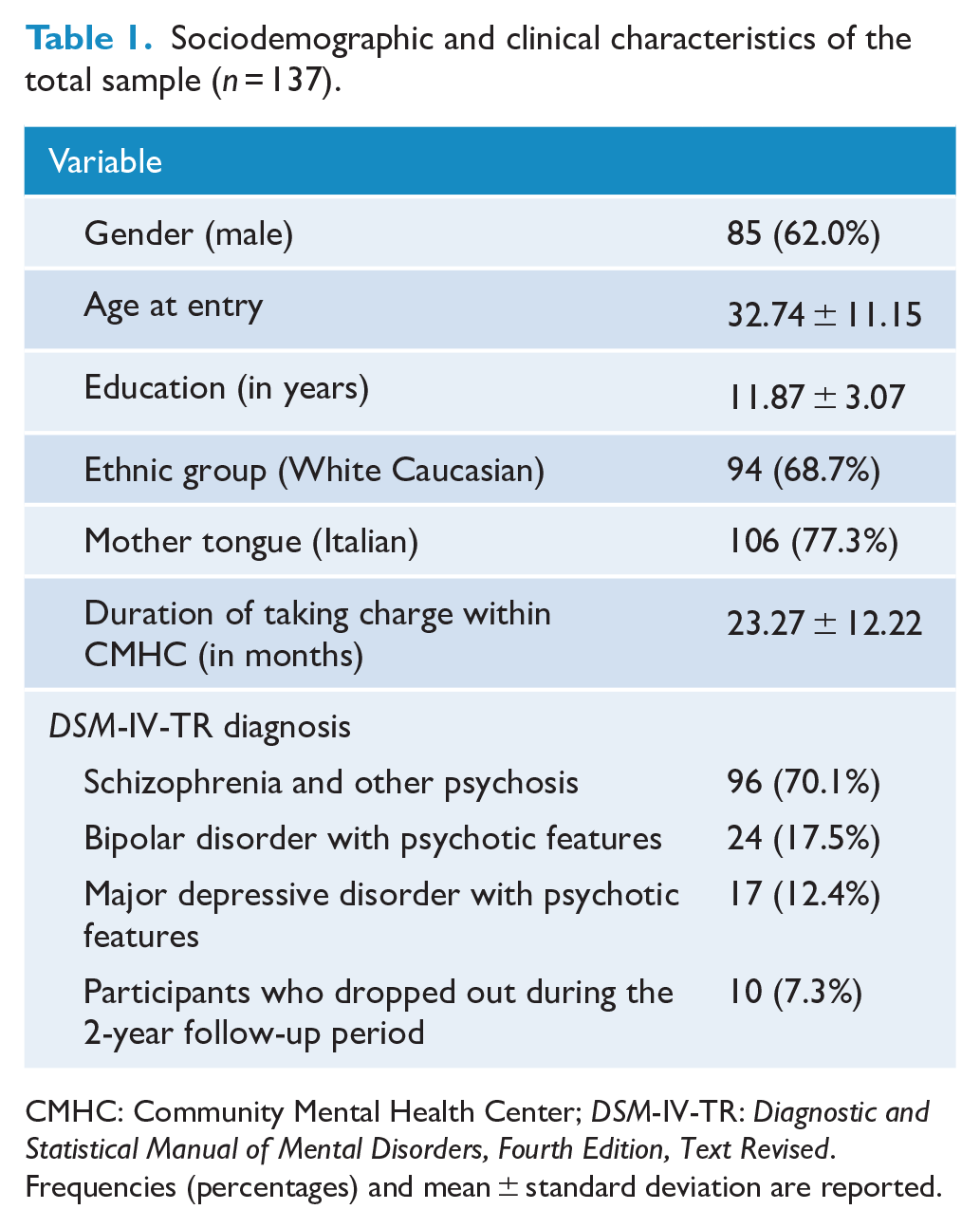
CMHC: Community Mental Health Center; DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revised.
Frequencies (percentages) and mean ± standard deviation are reported.
The total sample included patients with DSM-IV-TR schizophrenia or other psychotic disorder (n = 96; 70.1%), bipolar disorder with psychotic features (n = 24; 17.5%) and major depressive disorder with psychotic features (n = 17; 12.4%). As regards the PHB intervention typology, 55 (40.1%) participants received a PHB multiaxis intervention. Moreover, 123 (89.8%) patients were provided with a PHB approach on the ‘Training/Work’ axis, 59 (43.1%) on the ‘Sociality’ axis and 12 (8.7%) on the ‘Housing’ axis. All participants concluded the 2-year follow-up period, with the exception of 10 (7.3%) individuals who dropped out during the second year of the study. Five of them moved out of the catchment area (i.e. the Parma Department of Mental Health), and it was not possible to reach them for final assessments. Antipsychotics represented the most used psychotropic medication at baseline (being taken by 130 [94.9%] subjects with SMI).
Follow-up data
Across the 24 months of follow-up, a relevant decrease in severity of all BPRS and HoNOS scores was found (Table 2). Moreover, a significant longitudinal improvement in GAF score was also observed.
Functioning and psychopathological characteristics across the 2-year follow-up period in the total group (n = 137).
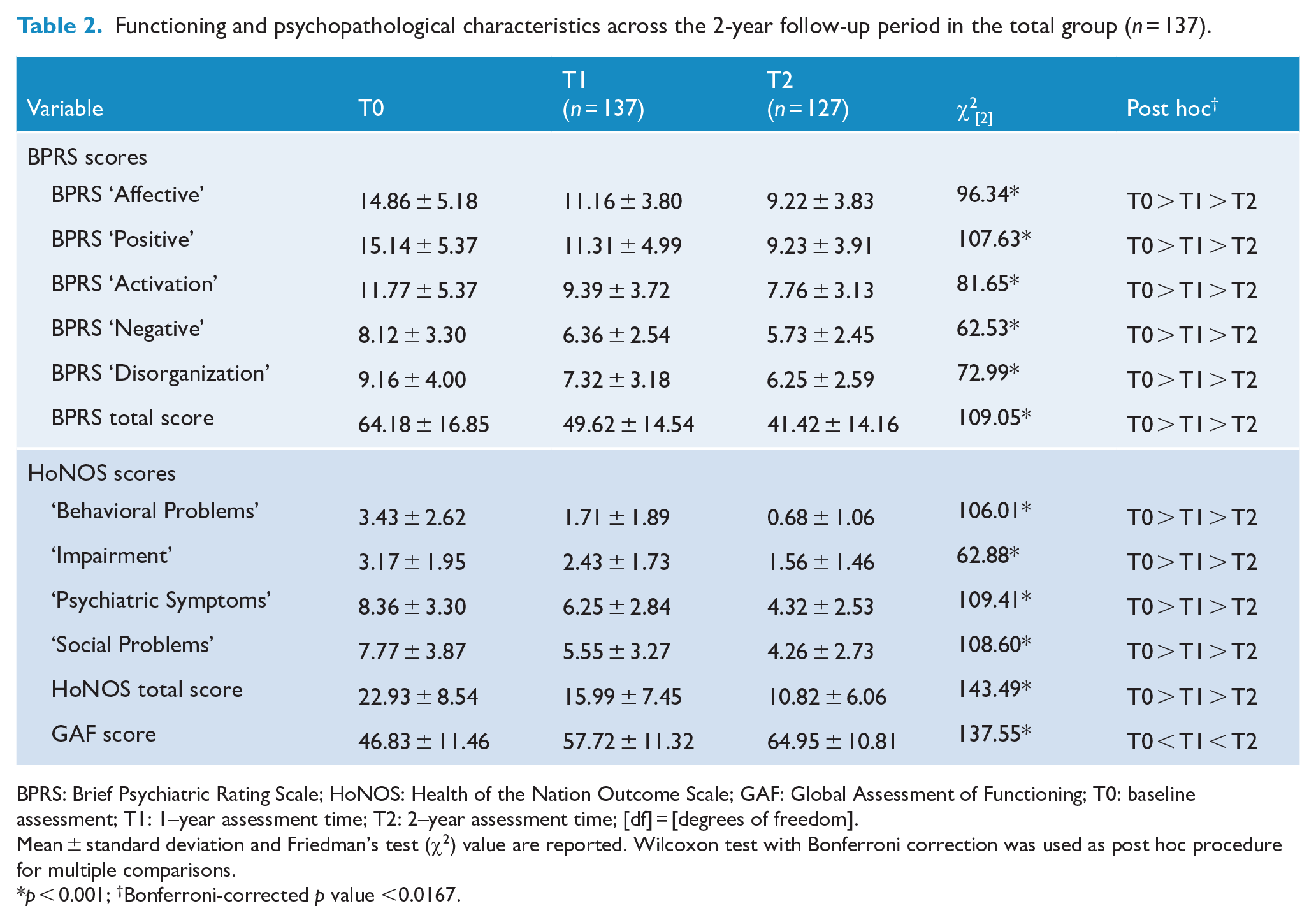
BPRS: Brief Psychiatric Rating Scale; HoNOS: Health of the Nation Outcome Scale; GAF: Global Assessment of Functioning; T0: baseline assessment; T1: 1–year assessment time; T2: 2–year assessment time; [df] = [degrees of freedom].
Mean ± standard deviation and Friedman’s test (χ2) value are reported. Wilcoxon test with Bonferroni correction was used as post hoc procedure for multiple comparisons.
p < 0.001; †Bonferroni-corrected p value <0.0167.
Finally, linear regression analysis results showed a relevant negative association of multiaxial PHB intervention (as independent variable) with the difference (delta) between T2 (2-year assessment time) and T0 (baseline) BPRS ‘Negative’ factor subscores, as well as with the delta between T2 and T0 HoNOS ‘Social problems’ subscale scores (as dependent variables). In contrast, no associations of the delta between T2 and T0 antipsychotic dose with functioning and psychopathological characteristics were found (Table 3).
Linear regression analysis results by multiaxis PHB intervention and daily dose of antipsychotic medication (independent variables) on functioning and psychopathological characteristics across the 2–year follow-up period (dependent variables) in the total group (n = 127).
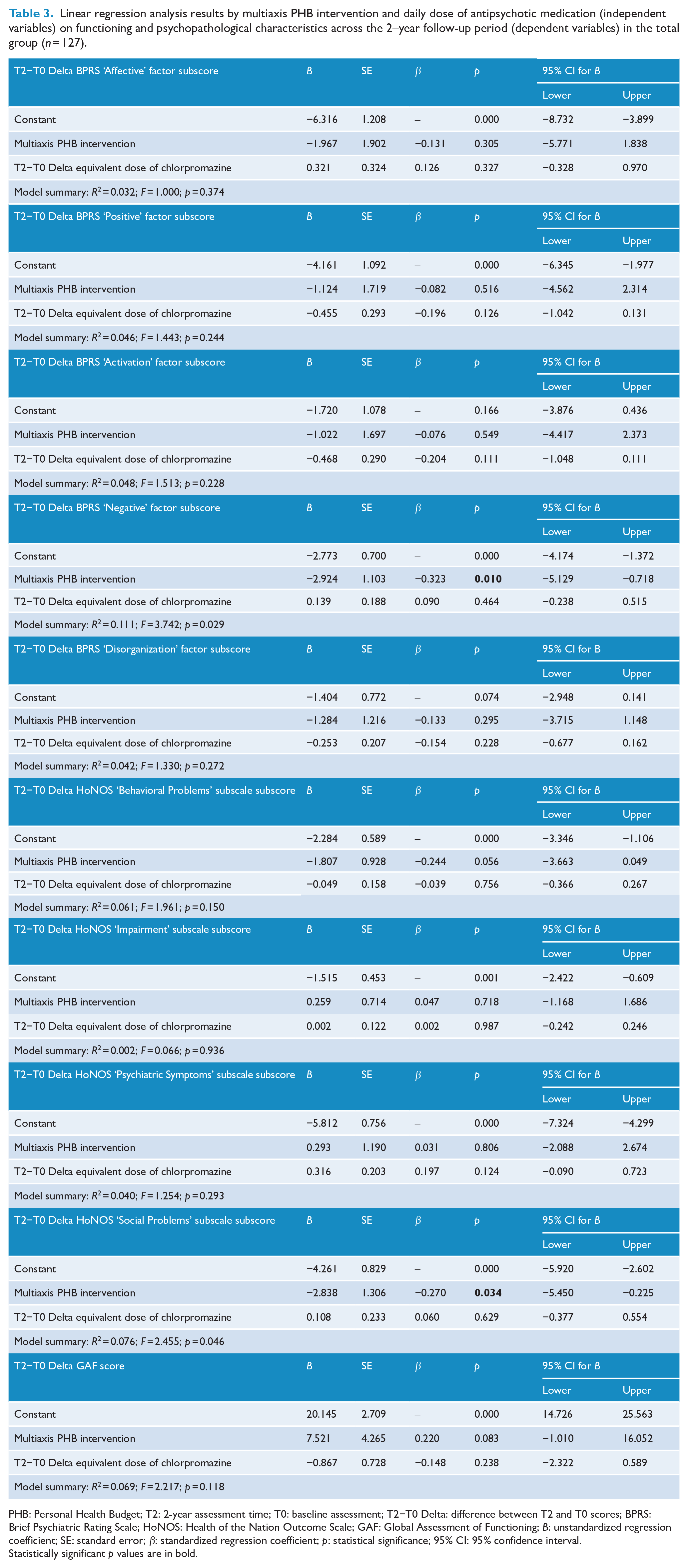
PHB: Personal Health Budget; T2: 2-year assessment time; T0: baseline assessment; T2−T0 Delta: difference between T2 and T0 scores; BPRS: Brief Psychiatric Rating Scale; HoNOS: Health of the Nation Outcome Scale; GAF: Global Assessment of Functioning; B: unstandardized regression coefficient; SE: standard error; β: standardized regression coefficient; p: statistical significance; 95% CI: 95% confidence interval.
Statistically significant p values are in bold.
Discussion
In the last two decades, empirical evidence showed that pharmacological treatment alone, despite clinical improvement, is not enough to prevent relapses and to ensure a stable functional recovery in patients with SMI both in the medium and in the long term (Drake and Whitley, 2014). In this respect, recent systematic reviews and meta-analyses suggested that integrated psychosocial interventions and intensive case management (together with pharmacotherapy) in SMI are more effective in reducing hospitalization and treatment drop-out, as well as in improving long-term functioning and social outcomes (Dieterich et al., 2017; Hunt et al., 2019). In this sense, psychosocial treatments can lead to a significant improvement in the patients’ quality of life, enhancing their interpersonal networks, social supports, socio-cognitive functions and self-esteem, so as to reach a fuller satisfaction of their unmet needs (Pelizza et al., 2020a). For these reasons, the PHB methodology has emphasized the necessity of offering community-based psychosocial interventions besides antipsychotic medications as a crucial part of the complex treatment of SMI (Varga et al., 2018).
In this context, the Italian PHB model may be considered as an innovative, integrated psychosocial rehabilitation approach aimed at creating an effective social and healthcare integration, placing the patients in their life environment and giving them an active role in the co-planning of their life projects (RER, 2016). In Italy, PHB has been intended as a new design of assistance, resulting in the promotion of the individual instead of certain services or service institutions as a way of personalizing care based on patient’s personal strengths and needs. Within this theoretical framework, the main aim of this study was to provide preliminary data about the beneficial effects of PHB methodology added to standard pharmacological therapy in patients with SMI.
Follow-up data
The findings of this research showed a significant improvement in functioning and in all the examined psychopathological and outcome parameters (i.e. BPRS and HoNOS scores) across the 2-year follow-up period. This suggests an overall beneficial effects of PHB (added to a standard pharmacotherapy) in ameliorating clinical, social and functional recovery of patients with SMI, confirming the promising add-on benefits of other supported employment interventions (e.g. IPS) within the Italian public mental health network (Pelizza et al., 2020b).
Linear regression analysis results also showed that a PHB multiaxial approach (but not the daily dose of antipsychotic medication) significantly predicted a specific improvement in negative symptoms and in social problems of patients with SMI after the 24 months of follow-up. In this sense, a multiaxis PHB approach (especially if combining interventions on employment and sociality [i.e. the two axes more commonly involved in our PHB treatments]) seems to be particularly useful in counteracting negative symptomatology and in favoring social inclusion in the community, and appears therefore to be preferred. These findings also support the results reported in other studies on PHB approach conducted in the United Kingdom and in the Netherlands (Slasberg et al., 2014; Webber et al., 2014), suggesting a positive impact of PHB interventions on psychological well-being in subjects with SMI. Specifically, in these studies, outcomes mainly included decreased severity in psychopathology, a better daily functioning, improved relationships and reduced drug misuse.
The success of PHB model has been attributed to both a ‘flexibility through partnership’ (creating a policy framework to enable decisions about how many resources each person should get within a cash-limited budget) and a ‘self-directed support’ (based on the individual being given a budget with which to plan his own care) (Jones et al., 2013). In this respect, it appears to be crucial for individuals affected by SMI (particularly those with problems that already restrict their ability to live the life they want) to have autonomy in choosing their own care.
Limitations
Several limitations of this research should be acknowledged. First, this study was a descriptive, retrospective cohort study with no control group. With this design, it was not possible to clearly attribute the observed improvements in outcome to PHB interventions, especially when patients were enrolled in treatment entry. Therefore, a longitudinal case–control design is needed to better examine PHB beneficial effects. However, for the 1-year period prior to this research, in a sample of 50 patients in ‘Treatment As Usual’ for SMI within the Parma Department of Mental Health (i.e. combining pharmacotherapy and a supportive case management) and with statistically similar sociodemographic and clinical characteristics, significantly greater percentages of drop-outs (n = 12 [24%] vs 10 [7.3%], χ2 = 7.78, p = 0.008) and new hospitalizations (n = 16/50 [32%] vs n = 20/137 [14.5%], χ2 = 6.49, p = 0.02) were found.
Second, participants provided with PHB intervention voluntarily accepted the PHB proposal. In this respect, although 91.3% of SMI patients accepted our PHB treatments, no specific (clinical/functional) comparison was made with the minority (n = 13) who did not agree with the intervention, and no potential systematic differences that might affect the interpretation of the results were examined. However, no statistically relevant inter-group difference on sociodemographic features (i.e. gender, age at entry, level of education, ethnic group and mother tongue) and duration of taking charge within CMHCs was found. Therefore, randomized controlled trials on effects and outcomes of PHB model are needed.
Third, in the present retrospective research, the follow-up duration was limited to 24 months. Thus, our findings should be replicated in long-term perspective studies.
Fourth, in this study, we eminently considered functional recovery, omitting to investigate personal recovery, which is a crucial dimension strictly associated with better long-term outcomes and quality of life (Poletti et al., 2019). Thus, future research extended beyond functional recovery to consider personal recovery of SMI subjects is needed. Moreover, qualitative methods to investigate the subjective experience of the individuals who experienced the PHB model of care are also useful to better analyze the beneficial effects of PHB interventions.
Fifth, in this study, outcome measures were all clinician-rated. Although raters were different from clinicians directly involved in providing PHB interventions, they knew that participants were receiving a PHB treatment and could be biased toward reporting a good outcome. Thus, further research including consumer-rated outcome measures to capture the participants’ perspective is needed.
Another weakness was the moderately limited sample size of the SMI group. This probably reduces the generalizability of our findings, which should be replicated in larger clinical populations with SMI.
Finally, in the current research, we considered a wide age range (18–50 years). Therefore, our findings should be replicated in more uniform age groups, such as in clinical populations of young people with SMI.
Conclusion
The findings of this study support the add-on benefits of PHB intervention to standard pharmacotherapy in terms of improving functioning and decreasing psychopathology severity in patients with SMI across a 2-year follow-up period. This improvement (especially in negative symptoms and in social problems) appears to be specifically enhanced by a PHB approach, based on the integration of professional knowledge and technical skills in order to provide person-tailored social/healthcare pathways within a caring community system. Therefore, the implementation of the PHB model in Italian public mental health services has a beneficial effect on people in treatment, does not seem to be in conflict with a standard pharmachological therapy for SMI and suggests that it may be clinically useful in addressing the hot issue of social retirement and unmet social needs. In the Italian context, PHB does not necessarily consist of new, extra-money, but rather a different and more rational way of allocating and spending health/social resources to meet specific personal needs and offer specialized care pathways within the belonging community.
Footnotes
Acknowledgements
The authors wish to thank all the patients who actively participated to the research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.