
Abstract
Objective:
The relationship between alcohol and substance use and the risk of violence exhibited by patients with mental disorders is under-researched. This prospective cohort study aims to compare patients with severe mental disorders and with different substance use behaviors in terms of sociodemographic and clinical characteristics, hostility, impulsivity and aggressive behaviors. Furthermore, this study aims to assess differences in violent behaviors during a 1-year monitoring follow-up.
Methods:
A total of 378 participants with severe mental disorders from Italian residential facilities and from four Departments of Mental Health (244 outpatients and 134 residential patients) were enrolled. Participants were categorized as Persons with Current Substance Use, Persons with Former Substance Use and Persons with Non-Substance Use. All these patients underwent a complex multidimensional assessment, including the lifetime and current substance use; a subsample of outpatients was also assessed with a laboratory substance assay including the testing for specific substances. We assessed the differences among these three groups in hostility, impulsivity and aggressive behaviors.
Results:
The results of the close 1-year monitoring show a significantly higher risk of violence for patients with severe mental disorders Persons with Current Substance Use compared to Persons with Former Substance Use and Persons with Non-Substance Use. Persons with Current Substance Use showed significantly higher scores for irritability, negativism and verbal assault compared to Persons with Non-Substance Use. Persons with Former Substance Use showed significantly higher scores for lifetime history of aggressive behaviors compared with patients with Persons with Non-Substance Use.
Conclusion:
These findings suggest that patients with comorbid mental illness and substance use disorders should be referred for specific interventions to reduce aggressive behavior and ensure patient well-being and community safety.
Introduction
The common perception that mental disorders and violence are closely related as well as much of the stigma associated with mental illness may be related to a tendency to associate mental disorders with danger. However, this perception is not always supported by research, which has provided mixed results.
There is unanimous agreement that the co-occurrence of a severe mental disorder and substance use disorder markedly increases the risk of aggressive or violent behavior (Fazel et al., 2018; Iozzino et al., 2015). Several studies suggest that people who have severe mental disorders have high rates of comorbid substance use (Cotto et al., 2010), with prevalence rates of up to 47% in the United States (Regier et al., 1990) and 35% in Europe (Carrà et al., 2012). Understanding the additive or interactive effect of other well-known risk factors (such as diagnosis, age, sex, history of violence, impulsivity, hostility) for violence in people with comorbid severe mental illness and alcohol and substance use is therefore urgent, in particular in Italy, where recent national legislation (n. 81/2014) led to the closure of forensic mental hospitals and diversion of patients at low risk for reoffending to ordinary Departments of Mental Health.
This study assessed the associations between different levels of alcohol and substance use and violent behavior as assessed by Modified Overt Aggression Scale (MOAS) among patients with mental disorders. The specific aims were to (1) assess the sociodemographic and clinical characteristics of Persons with Current Substance Use (PCSU), Persons with Former Substance Use (PFSU), Persons with No Substance Use (PNSU); (2) explore differences in anger, impulsivity, hostility and previous violent behavior between PNSU, PFSU or PCSU; (3) assess differences in the frequency and severity of violent behavior during a 1-year follow-up (FU) period between PNSU, PFSU or PCSU; and (4) evaluate the main predictors of violent behavior across different levels of alcohol and substance use.
Methods
This study is part of the Violence Risk and Mental Disorders (VIORMED) project that involved four Departments of Mental Health in Northern Italy (De Girolamo et al., 2016, 2019). This prospective cohort study involved patients living in long-term residential facilities and outpatients who received treatment at different community mental health centers. Each Department of Mental Health included four community mental health centers that had approximately 3600 to more than 4400 patients (see Table S1). The residences were located in four cities in northern Italy; they have 24-hour coverage and generally host up to 20–25 patients.
Treating clinicians recruited residential patients in the index period of May 2013 to September 2013, and outpatients were recruited over a 6-month period in 2015. Study participants were recruited consecutively until the estimated sample size of approximately 450 patients was reached (ratio of cases and controls, 1:1). Inclusion criteria were a primary psychiatric diagnosis and age between 18 and 65 years. Cases (patients with a history of severe violence) were recruited first; selection was based solely on comprehensive, detailed documentation (as reported in clinical records) of a history of violent behavior; patients had to meet one or more of the following criteria: (1) at least one admission to a Forensic Mental Hospital for any violent act against a person; (2) at least one arrest for any violent act against a person; (3) a documented lifetime history of a violent act against a person in the last 10 years (as reported in clinical records); caused physical harm to the victim; or a history of armed robbery, pyromania or sexual violence. The control group, matched by age, sex and diagnosis, included patients who did not meet any of these three conditions.
Exclusion criteria included a primary diagnosis of an organic mental disorder, an intellectual disability, dementia or sensory deficit. In addition, patients with a primary substance use disorder were excluded because they are treated by addiction services and not by Departments of Mental Health. All participants provided written informed consent before the start of assessments. Ethical approval was granted by the ethical committees of the coordinating center (IRCCS Saint John of God, Fatebenefratelli) and the other recruiting centers.
Measures
Information was collected on selected sociodemographic, clinical and treatment-related characteristics. The Structured Clinical Interview for DSM-IV Axis I Personality Disorders (SCID-I) (First et al., 2002) and Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II) (First et al., 1997) were administered to confirm clinical diagnoses.
Symptom severity and psychosocial functioning were assessed with the Brief Psychiatric Rating Scale–Expanded (BPRS-E), (Ventura et al., 1993), the Specific Levels of Functioning (SLOF) (Montemagni et al., 2015) and the Personal and Social Performance Scale (PSP) (Morosini et al., 2000). Patient self-awareness about the disorders was assessed with the Insight Scale (IS) (Marková et al., 2003).
During the 1-year FU period, aggressive and violent behavior shown by patients was rated every 15 days with the MOAS (Margari et al., 2005), for a total of 24 evaluations for each patient. All MOAS evaluators were very familiar with the patients and had daily or very frequent contact with them.
Violence and impulsivity were evaluated with the following instruments: the Brown–Goodwin Lifetime History of Aggression (BGLHA), an 11-item questionnaire (Brown et al., 1979) assessing lifetime aggressive behavior across adolescence and adulthood; the Buss–Durkee Hostility Inventory (BDHI), a 75-item questionnaire developed to assess eight subscales related to hostility and negative affect (Buss and Durkee, 1957); the Barratt Impulsiveness Scale (BIS-11), a 30-item, 4-point Likert-type scale questionnaire assessing personality and behavioral impulsiveness, with scores of 30–120 (Fossati et al., 2001); the State-Trait Anger Expression Inventory 2 (STAXI-2), which includes six scales plus an Anger Expression Index, an overall measure of total anger expression (Spielberg, 1994).
Assessment of alcohol or substance use
Information about alcohol and substance use over the patient’s lifetime and during the past 12 months was collected from clinical records in order to define precise operational criteria. Based on their history, participants were classified into three groups by the treating clinicians: (1) PCSU characterized by episodes of alcohol and substance use (at least 21 episodes of use in the last year) resulting in individual health and psychosocial problems; (2) PFSU characterized by at least 21 episodes of use resulting in individual health and psychosocial problems (but not in the last 12 months); (3) PNSU. More details about the substances used and the frequency of use of PCSU are shown in Table S2.
Furthermore, the Multidrug Test (BSD711; Biosigma) was administered to a randomly selected subgroup of outpatients who had given written informed consent for urine testing. For financial reasons, the test could not be administered to the entire sample; therefore, the decision was made to randomize at least 50% of the outpatient sample. The Multidrug Test is an immersion rapid screening test that provides simultaneous qualitative detection of multiple drugs in urine samples. This test was administered once during the 1-year FU, with no previous notice, to further confirm the reliability of information about use behavior reported in the clinical records.
Finally, during the 1-year FU the treating psychiatrists completed a clinical monthly report with detailed information on alcohol and substance use for a subgroup of outpatients. This report was used to explore the association between episodic use and monitoring of violent behavior with the MOAS, which was conducted every 2 weeks.
Statistical analyses
Descriptive statistics were conducted with contingency tables for categorical variables and through the main statistical indexes, such as mean and standard deviation (SD), for quantitative variables. The distribution of categorical data among the three groups was compared with the χ2 test or exact Fisher’s test (when n < 5 in at least one cell). For quantitative data, Gaussianity assumption was verified with QQ-plots and box plots and Shapiro–Wilk and Kolmogorov–Smirnov tests. Depending on the distribution of variables (Gaussian or non-Gaussian), analysis of variance (ANOVA) or a nonparametric Kruskal–Wallis test was used. Moreover, analysis of covariance (ANCOVA) and generalized linear models (GLMs) were used to consider possible confounding of sociodemographic and clinical variables. Post hoc analyses were computed with Bonferroni correction.
Based on the work of Dazzi et al. (2016), a first confirmatory and a subsequent exploratory factor analysis were run on BPRS-E-E items to identify the main scale domains. Factor extraction was performed by varimax rotation, and the number of factors was determined through Kaiser’s criterion (i.e. eigenvalue ⩾ 1) and visual inspection of the scree plot. Factor loadings with the highest value (among extracted factors) were considered to contribute sufficiently to the overall variability accounted for by each factor (see Supplementary Table S3).
Participants who missed less than 10% of MOAS evaluations (i.e. up to two-time evaluations in all four subscales, therefore, for a total of 8 data points) were imputed by the moving average estimation method (MOAS of N = 7 participants, for a total of 35 data points, were imputed). Conversely, patients who missed more than 10% of MOAS evaluations (n = 15) were not considered in the analyses. For such a sample, the amount of missing values for each of the assessed sociodemographic and clinical variables was less than 10%.
Sociodemographic and clinical variables significantly associated with the study groups were assessed as potential predictors of aggressive behavior as measured by MOAS scores. Considering the skewed and zero-inflated distributions of the MOAS, GLMs with Tweedie distribution and log-link function were used.
Finally, mixed models with Tweedie distribution and log-link function were used to evaluate the longitudinal association between violent behavior, assessed with the MOAS, and symptoms, assessed through BPRS-E-E, both evaluated at two time points. These relationships were also adjusted for STAXI (state and trait anger scales). In order to achieve a temporal consistency between MOAS and BPRS-E-E evaluations, MOAS ratings at baseline and at the final timepoint were considered, respectively, as the average of the first four and of the last four observations (each covering 2 months of MOAS monitoring).
All tests were two-tailed and with statistical significance set at p = 0.05. All data were coded and analyzed using SPSS version 25 and R: language and environment for statistical computing (version 3.4.1, using cplm package).
Results
Sociodemographic and clinical characteristics
The total sample included 378 participants (134 residential patients and 244 outpatients). Another 10 residential patients and 27 outpatients were contacted, but refused to participate. Table 1 shows the sociodemographic characteristics of the sample based on a history of use behavior.
Sociodemographic characteristics of the sample.
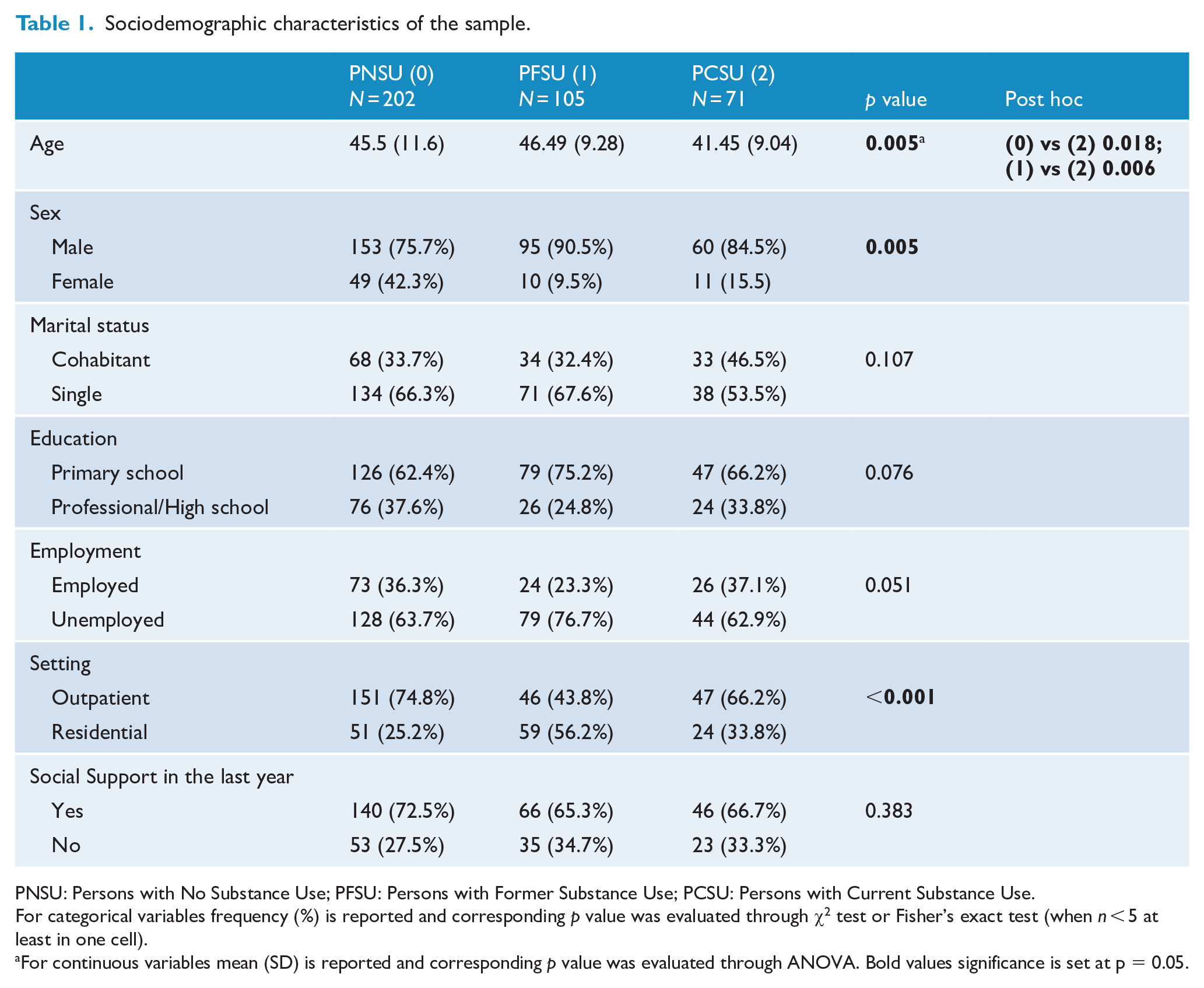
PNSU: Persons with No Substance Use; PFSU: Persons with Former Substance Use; PCSU: Persons with Current Substance Use.
For categorical variables frequency (%) is reported and corresponding p value was evaluated through χ2 test or Fisher’s exact test (when n < 5 at least in one cell).
For continuous variables mean (SD) is reported and corresponding p value was evaluated through ANOVA. Bold values significance is set at p = 0.05.
Overall, 53.4% of patients had no history of use (PNSU), whereas 27.8% had a former history (PFSU) and 18.8% had a current history (PCSU). Among PCSU alcohol (72.7%), cannabis (36.8%) and stimulants (28.4%) were the most prevalent substances. More specifically, considering daily use, alcohol use was the most prevalent followed by cannabis, benzodiazepines, stimulants, hallucinogens, opioids and sedative-hypnotics (see Table S2 for details).
The three groups showed significant differences for age (p = 0.005, with PCSU more likely to be younger than PNSU and PFSU) and sex (p = 0.005). Moreover, significant differences among the three groups were found for setting, with a different distribution of outpatients and residential patients (p < 0.001). These results were partially confirmed in the analysis performed separately for residential patients and outpatients (see Table S4).
The 116 outpatients who consented to the Multidrug Test were randomly assigned to two conditions: test (N = 59) and no test (N = 57). The findings of the Multidrug Test substantially supported the classification of the three groups, showing a significant association between PCSU, PFSU, PNSU and the multidrug categories (p < 0.001). In particular, all PNSU showed negative findings on the Multidrug Test and 64% of PCSU showed positive findings on the Multidrug Test.
The primary diagnosis (Table 2) showed a significant association with the three groups (p = 0.001): PCSU had a higher prevalence of patients with a primary diagnosis of a personality disorder, whereas for PNSU and PFSU, schizophrenia was the most frequent diagnosis. Cluster B personality disorders were the most frequent (56.6%) compared with cluster A (15.1%), cluster C (6.6%) and not otherwise specified (20%). The primary diagnosis showed a significant association with the three groups also, when separate analyses were performed for residential patients and outpatients (see Table S5).
Clinical characteristics of the sample.
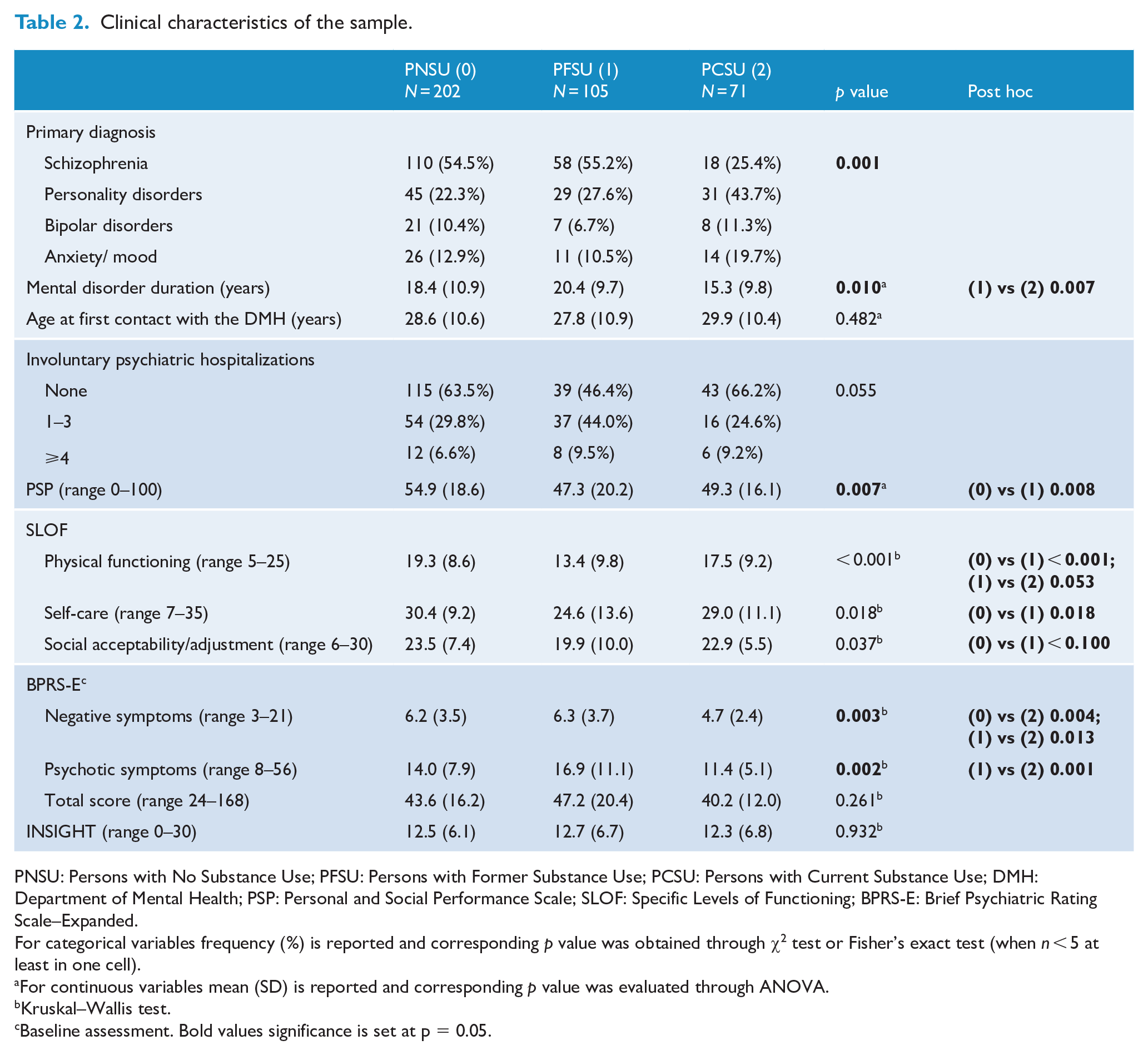
PNSU: Persons with No Substance Use; PFSU: Persons with Former Substance Use; PCSU: Persons with Current Substance Use; DMH: Department of Mental Health; PSP: Personal and Social Performance Scale; SLOF: Specific Levels of Functioning; BPRS-E: Brief Psychiatric Rating Scale–Expanded.
For categorical variables frequency (%) is reported and corresponding p value was obtained through χ2 test or Fisher’s exact test (when n < 5 at least in one cell).
For continuous variables mean (SD) is reported and corresponding p value was evaluated through ANOVA.
Kruskal–Wallis test.
Baseline assessment. Bold values significance is set at p = 0.05.
Significant differences were found for the duration of mental disorders (p = 0.010). Moreover, PFSU had lower PSP scores compared with PNSU (p = 0.008). Similar differences were found for the SLOF subscales: physical functioning, self-care and social acceptability (p < 0.001, p = 0.018 and p = 0.037, respectively). Separate analyses for residential patients and outpatients did not show these differences (except for SLOF social acceptability; see Table S5).
The BPRS-E-E items were analyzed with the following four-factor structure (obtained from factor analysis; see Table S3): negative symptoms, psychotic symptoms, affect-anxiety and activation. Table 2 reports BPRS-E-E significant differences between the groups (see Table S3 for more information): PCSU showed less severe negative symptoms than PNSU and PFSU (p = 0.004 and p = 0.013, respectively) and less psychotic symptoms than PFSU (p = 0.001). These results were confirmed in the separate analyses for both groups of patients, although, as expected, the BPRS-E-E scores of residential patients were higher than those of outpatients (data not shown).
Finally, no differences were found among the three groups for IS scores; similarly, no differences were visible between the two settings (see Table S5).
Hostility, impulsivity, anger and past aggressive behavior
Table 3 reports BIS total scores and BDHI significant differences between the groups (see Table S6 for more information). Compared to PNSU, PCSU showed higher scores in BDHI irritability (p = 0.006), negativism (p = 0.016) and total scores (p = 0.037). When residential patients and outpatients were analyzed separately, this result was partially confirmed for outpatients (see Table S6). Conversely, no significant differences were found for BIS scores.
Lifetime aggression, hostility, impulsivity and anger dimensions of the all sample.
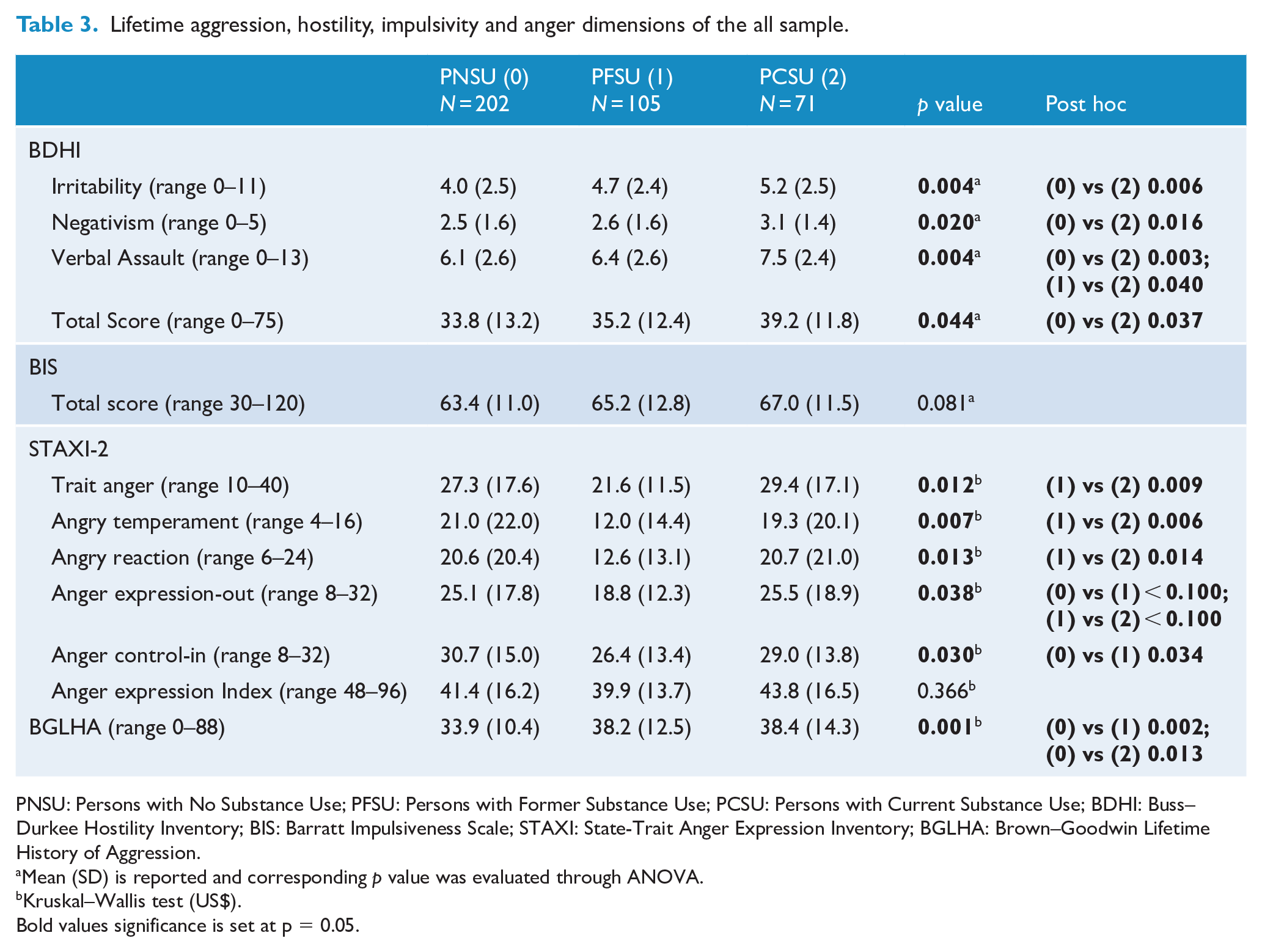
PNSU: Persons with No Substance Use; PFSU: Persons with Former Substance Use; PCSU: Persons with Current Substance Use; BDHI: Buss–Durkee Hostility Inventory; BIS: Barratt Impulsiveness Scale; STAXI: State-Trait Anger Expression Inventory; BGLHA: Brown–Goodwin Lifetime History of Aggression.
Mean (SD) is reported and corresponding p value was evaluated through ANOVA.
Kruskal–Wallis test (US$).
Bold values significance is set at p = 0.05.
Table 3 reports also STAXI-2 subscales that showed significant differences between the three groups (see Supplementary Materials for more information). PFSU showed lower scores than the PCSU on many STAXI-2 subscales. Moreover, significant differences were found among the three groups for anger expression-out (p = 0.038). These results were almost confirmed in the separate analyses for residential patients and outpatients (see Table S6).
Finally, the three groups showed different lifetime aggressive behavior, as shown by BGLHA scores (p = 0.001), with significantly higher scores for the PFSU and PCSU compared with PNSU (Table 3).
Figure 1 shows mean MOAS scores at 1-year FU. PCSU had significantly higher scores than the PNSU and PFSU on all four MOAS subscales (p = 0.001 for all) and for the total score (p < 0.001), showing more violent behavior than the other groups (see Table S7 and Table S8).
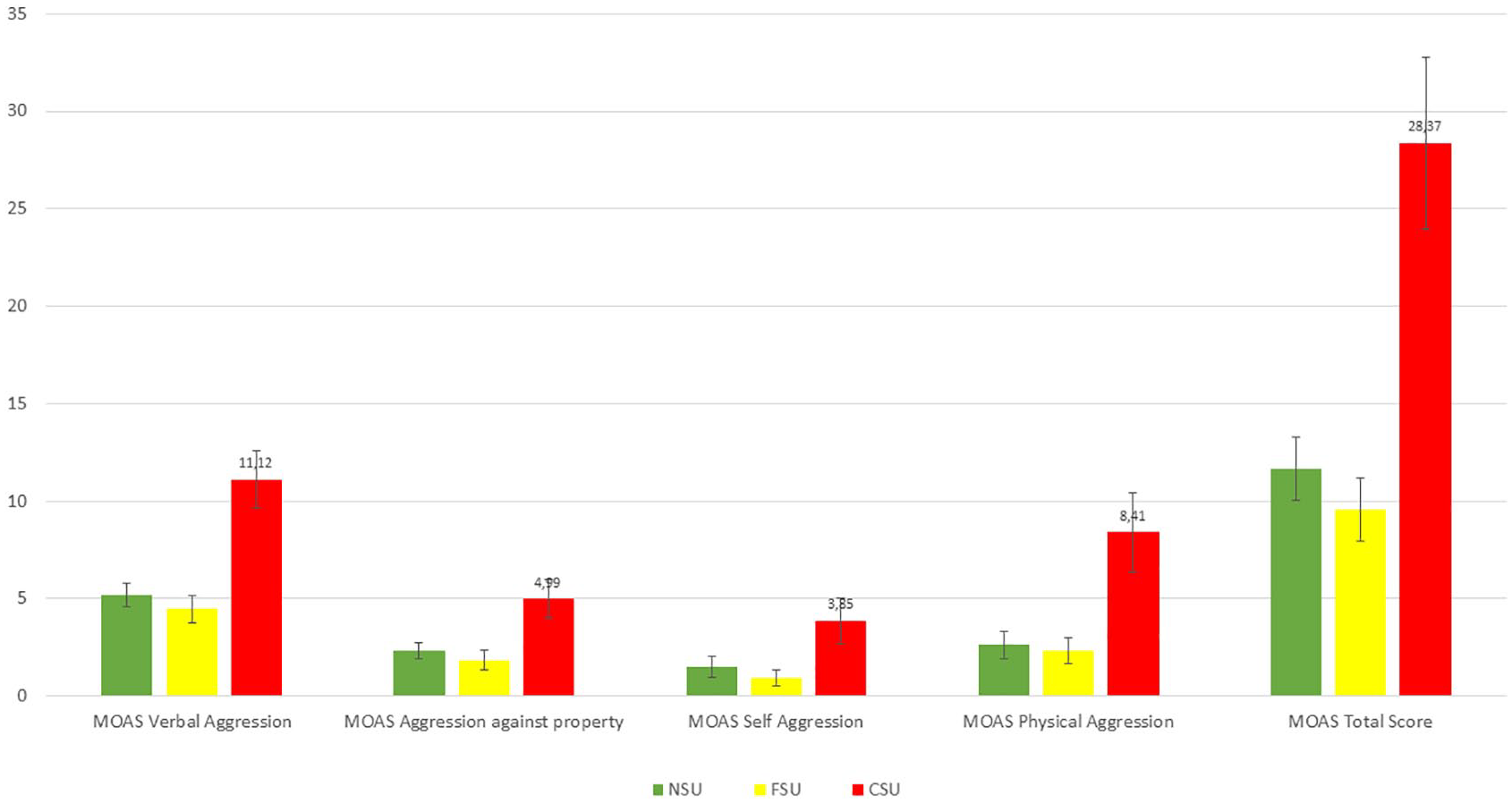
MOAS subscales and total scores during 1-year follow-up.
All sociodemographic and clinical variables that were significantly associated with the three groups (i.e. sex, age, diagnosis, illness duration, PSP, SLOF, BDHI scores, STAXI and BGLHA) were evaluated as predictors of MOAS total score by a multiple GLM, identifying (for significance and explained variability) the following three variables as best predictors: primary diagnosis, BPRS-E-E negative symptoms and BDHI total score. When the clinical differences between patients in the two settings (RFs and outpatients) were considered, a GLM with the interaction effect [predictor × groups × setting] was performed for each of the three best predictors (see Figure 2). As expected, the CSU group showed more violent behavior than the other groups, regardless of the predictors and setting (p < 0.004 for all three GLMs).
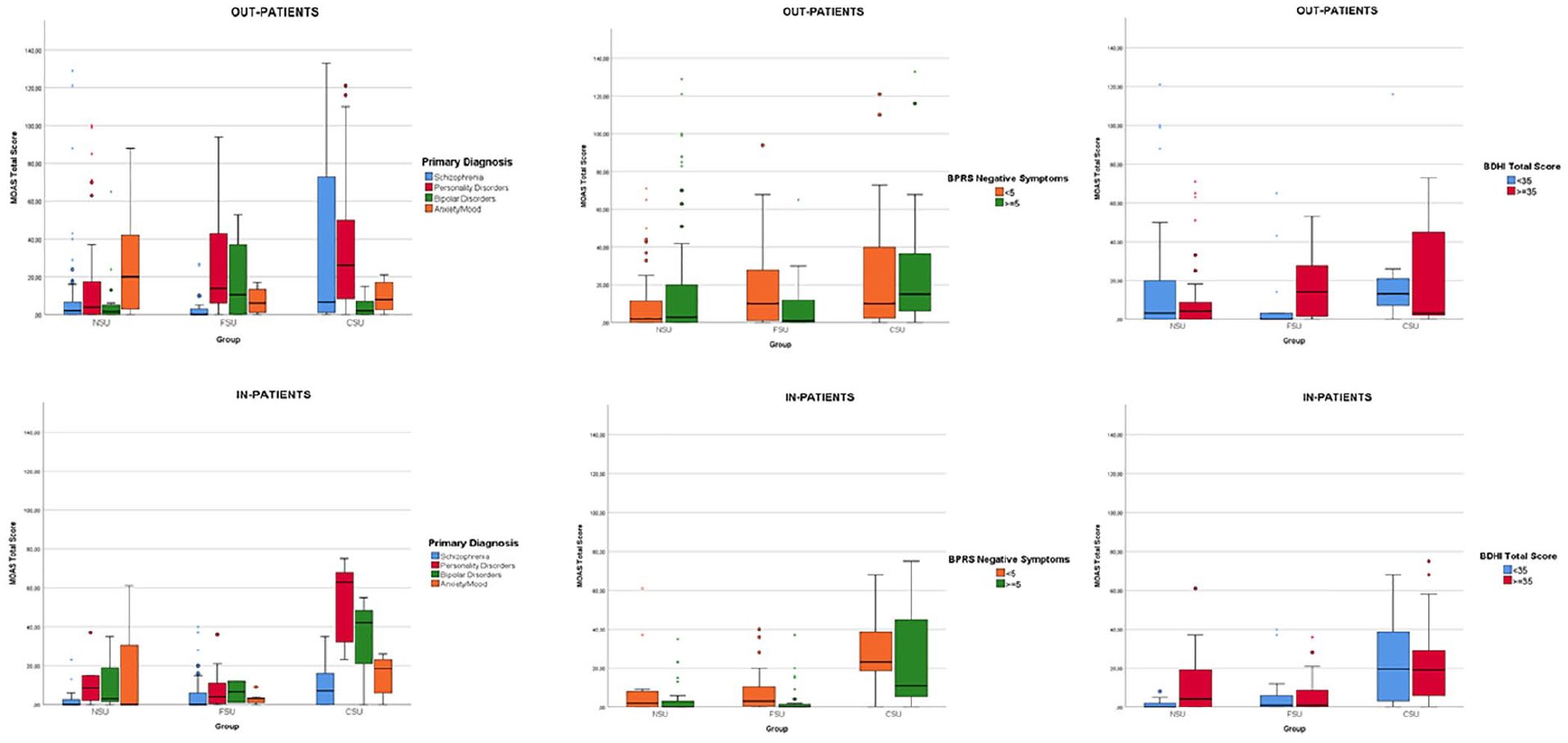
Graphical representation of the generalized linear models with the interaction effect [predictor × groups × setting].
Residential patients had higher MOAS scores. The main differences in diagnoses were found between outpatients PCSU compared to residential PCSU with personality disorders and bipolar disorder (Figure 2; panels A and B). Similarly, residential patients in the CSU group who had fewer BPRS-E-E negative symptoms showed higher levels of violence than outpatients in the CSU group (Figure 2; panels C and D).
Finally, clinical monthly reports of use episodes of a subgroup of outpatients were used to assess their periodic use behavior during the 1-year FU. A significant association was found between the three groups and use behavior for all 12 months, showing that frequent or occasional users were more prevalent for PCSU (see Table S9). These clinical monthly reports were also used to distinguish occasional and frequent users from non-users and to explore their violent behavior (assessed with the MOAS total score; see Figure S1 in Supplementary Materials): occasional and frequent users had systematically higher MOAS scores than patients who never used alcohol or substances during the 1-year FU.
Longitudinal association between violence and symptomatology
Table 4 shows that an increase of BPRS-E Activation item was associated with an increase of MOAS total score. On the other hand, an increase of BPRS-E Negative Symptoms and BPRS-E Psychotic Symptoms was associated with a decrease of MOAS total score. For the BPRS-E Activation, the observed association was due to a change in verbal aggression and aggression against people; for BPRS-E Negative Symptoms, the relationship was due to a change in verbal aggression, and for BPRS-E Psychotic Symptoms, the association was due to a change in all MOAS subscales. The associations observed above hold also adjusting for the three study groups. Moreover, adding STAXI (state anger and trait anger scales) in the mixed model, the longitudinal associations between MOAS Total score and BPRS-E subscales were all still statistically significant, with the exception of BPRS-E Psychotic symptoms (when adjusted for STAXI Trait anger). This last result showed a spurious association between MOAS Total Score and BPRS-E Psychotic Symptoms, driven by STAXI Trait anger.
Relationship between MOAS Total score and BPRS unadjusted and adjusted for STAXI: mixed models.
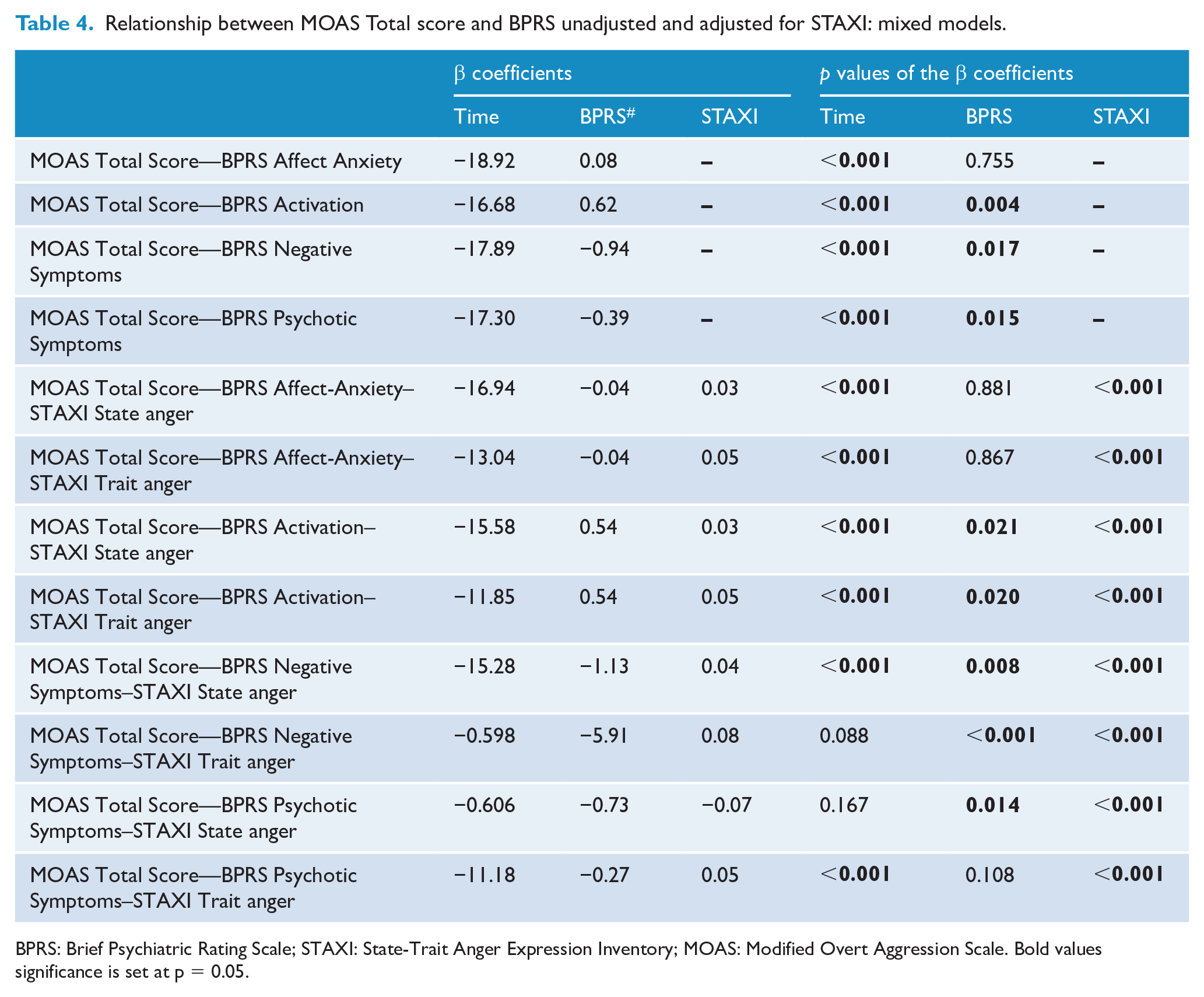
BPRS: Brief Psychiatric Rating Scale; STAXI: State-Trait Anger Expression Inventory; MOAS: Modified Overt Aggression Scale. Bold values significance is set at p = 0.05.
Discussion
This study assessed the clinical characteristics, frequency and severity of violent behavior among psychiatric patients with differing histories of use behavior.
Consistent with previous Italian data related to people with severe mental disorders (Carrà et al., 2015), we found that almost 20% of the sample was made up by patients in the PCSU group due to episodes of use in the last 12 months. Since no specific interventions addressing addictive behavior reduction are usually provided by mental health services in Italy, our findings confirm that current substance use among patients in treatment may be underestimated.
The Multidrug Test administered during the 1-year FU to a subgroup of outpatients showed that no positive test results were found for PNSU compared to a rate of 36.4% positive testing among of PCSU. PCSU were substantially more likely to be outpatients (66.2%) compared with residential patients (33.8%). The most prevalent substances used were alcohol, cannabis and stimulants. Because RFs are not high-security facilities and patients can go out during the daytime, occasional use of alcohol and substances is possible. Moreover, PCSU were younger than those in the other groups. Consistent with previous results (Cavalera et al., 2018; Dipartimento Politiche Antidroga, 2015), the mean age of patients seeking treatment for use behavior is lower compared with patients already in treatment, who may have stopped episodes of use. Participants with past and current use behavior were more likely male. Consistent with previous data (Duke et al., 2018), in Italy, patients with severe mental disorders and comorbid episodes of alcohol and substance use are significantly more often male.
Diagnostic and clinical patterns
As found in other studies (Mir et al., 2015), patients with personality disorders showed higher rates of past or current use behavior. This may be related to the high proportion (56.6%) of cluster B personality disorders: these patients share many clinical characteristics with those who show alcohol and substance use (Moss et al., 2015). In addition, consistent with previous European data (Candini et al., 2017), in this study, patients with schizophrenia showed a prevalence of PNSU (54.5%) that is low compared with North American or Northern European patients (Carrà et al., 2012).
PFSU had lower personal and social performance scores than PNSU: prolonged use behavior is usually associated with marked impairment of daily psychosocial functioning (Vonasch et al., 2017).
Hostility, impulsivity, anger and past aggressive behavior
As assessed by BDHI total score, PCSU showed more hostility than PNSU. These data highlight that use of alcohol and substances can amplify hostility and affect the way that patients relate to other people (McCormick and Smith, 1995). More specifically, considering PCSU data, alcohol use was the most prevalent and the most severe confirming that this kind of use can be related to aggressive behavior in patients with mental disorders (Iozzino et al., 2015).
As assessed by the BIS scale, impulsivity scores showed no significant differences, although mean scores followed the direction of BDHI results, indicating that PCSU were more likely to show impulsive behavior than the PFSU and PNSU.
According to STAXI-II scores, PNSU showed greater ability to control anger than PFSU (Garofalo and Wright, 2017). PCSU also showed higher scores for trait anger, angry reaction and angry expression-out compared with PFSU, suggesting that those who quit use behavior may be less prone to express anger than PCSU. Contrary to expectations, PNSU had higher scores for angry temperament compared with the PFSU and PCSU, and further study is warranted.
On the BGLHA, data confirm that the absence of use behavior, as found for PNSU reporting lower BGLHA scores, is associated with a decreased lifetime likelihood of violent behavior.
Behavior of patients with a different use history during 1-year FU
While there have been other studies focusing on the risk of violence among people with mental disorders (with and without former or current substance use) which have employed larger samples, no study has ever conducted such a detailed outpatients monitoring (every 2 weeks) of aggression and violence. Consistent with previous results (Chermack et al., 2014; Elbogen et al., 2016), the 1-year MOAS monitoring shows that PCSU were more likely to exhibit verbal aggression, aggression against property and aggression against people than PFSU and PNSU. As shown by MOAS subscales and total scores, PCSU show a significantly higher number of aggressive and violent behaviors compared with PNSU. As found by Schaffer et al. (2015), current use behavior is also a significant predictor of self-aggressive behavior among patients with mental disorders. The relationship between use behavior and MOAS scores was systematically confirmed by the clinical monthly reports for all 12 months.
Multiple GLM analysis also showed that PCSU were more likely to show violent behavior. Consistent with previous results (Bulgari et al., 2017), personality disorders and low negative BPRS-E symptoms must be considered, especially for residential patients with current use. Our findings suggest that specific interventions to reduce aggressive and violent behavior should be targeted toward patients with this clinical profile.
MOAS ratings and symptom patterns
We found a positive association between the BPRS-E Activation and the mean MOAS ratings, each covering 2 months either after baseline assessment or prior to the 1-year FU; on the other hand, a negative association was also found between BPRS-E Negative Symptoms and MOAS ratings, and these findings were confirmed controlling for STAXI. This again highlights the importance of general symptom patterns to modulate the onset or the decrease of aggressive and violent behavior and points to the importance of treatment to control behavioral activation in people with severe mental disorders.
Limitations
This study had some limitations. Since we did not assess the effect of medication and treatment adherence during the 1-year FU, we could not explore the relationships between these clinical variables and alcohol/substance use and the risk of violence.
Although a recent meta-analysis showed good reliability of clinical screening information compared with biologic testing (Large et al., 2012), not all patients who were offered the Multidrug Test accepted: in particular, CSU patients, as reported in clinical records, refused.
Conclusion
Patients who exhibit current use behavior are at higher risk for violent behavior in both the outpatient and residential settings. To assess the frequency and severity of aggressive and violent behavior by patients with severe mental disorders, the accuracy of reports by key informants is of paramount importance: from this perspective, it is worth noting that no study as the VIORMED has ever performed such a close monitoring of aggressive and violent behavior, with 24 ratings every 2 weeks over the course of 1 year. Although some studies have employed larger samples (Appelbaum et al., 2000; Steadman et al., 1998; Swanson et al., 2002, 2006), they have assessed extended time periods (generally 6 months), and this raises many questions in terms of potential recall biases which may flaw an accurate reporting of these events.
These data provide crucial cues for the development of specific treatment programs for health care staff (Carroll, 2007; Simpson et al., 2015). As for other European countries, the Italian mental health system has encouraged a closer relationship between mental health services and addiction services (Carrà and Johnson, 2009). More efforts toward a multi-layered approach between mental health services and addiction services may benefit both patient well-being and community safety and may significantly contribute to efforts to reduce the stigma attached to mental disorders.
Supplemental Material
FigS1 – Supplemental material for Substance use disorders and violent behaviour in patients with severe mental disorders: A prospective, multicentre study
Supplemental material, FigS1 for Substance use disorders and violent behaviour in patients with severe mental disorders: A prospective, multicentre study by Cesare Cavalera, Clarissa Ferrari, Giorgio Bianconi, Viola Bulgari, Valentina Candini, Giuseppe Carrà, Massimo Clerici, Giovanni Conte, Marta Cricelli, Maria Teresa Ferla, Laura Iozzino, Ambra Macis, Alberto Stefana, Alessandra Ornaghi and Giovanni de Girolamo in Australian & New Zealand Journal of Psychiatry
Supplemental Material
SUPPLEMENTARY_MATERIAL – Supplemental material for Substance use disorders and violent behaviour in patients with severe mental disorders: A prospective, multicentre study
Supplemental material, SUPPLEMENTARY_MATERIAL for Substance use disorders and violent behaviour in patients with severe mental disorders: A prospective, multicentre study by Cesare Cavalera, Clarissa Ferrari, Giorgio Bianconi, Viola Bulgari, Valentina Candini, Giuseppe Carrà, Massimo Clerici, Giovanni Conte, Marta Cricelli, Maria Teresa Ferla, Laura Iozzino, Ambra Macis, Alberto Stefana, Alessandra Ornaghi and Giovanni de Girolamo in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors wish to thank the following clinicians who provided valuable help for the realization of the project: Paola Artioli, MD; Silvia Astori, MD; Emanuele Barbieri, MSN; Annalisa Bergamini, MD; Francesca Bettini, MD; Monica Bonfiglio, MD; Silvia Bonomi, MD; Stefania Borghetti, M. D; Giulia Brambilla, MD; Paolo Cacciani, MD; Pierluigi Castiglioni, MD; Giorgio Cerati, MD; Andrea Cesareni, MD; Ezio Cigognetti, MD; Massimo Clerici, MD; Fabio Consonni, MD; Alessia Delalio, MD; Giacomo Deste, MD; Emanuela Ferrari, MD; Silvio Lancini, MS Ed; Luca Micheletti, MD; Donato Morena, MD; Antonio Musazzi, MD; Paola Vittorina Negri, MD; Roberta Paleari, MD; Ivano Panelli, MSN; Cristina Pedretti, M.S.N.; Rosa Perrone, MD; Monica Petrachi, MD; Elisabetta Polotti, MD; Francesco Restaino, MD; Enrico Rossella, MD; Emilio Sacchetti, MD; Daniele Salvadori, MD; Jacopo Santambrogio, MD; Simona Scaramucci, MD; Pasquale Scognamiglio, MD; Giuseppina Secchi, MD; Joyce Severino, MD; Valentina Stanga, MD; Cesare Turrina, MD; Alessandra Vecchi, MD; Alessandra Zanolini, MS Ed. The VIORMED-2 Group also includes Mattia Bava, MD; Giulia Gamba, MD; Assunta Martinazzoli, MD; Giuliana Mina, MD; Alessandra Ornaghi, MD; Bruno Travasso, MD.
Author Contributions
G.d.G., C.C., C.F., V.B., V.C., M.C., L.I., A.M., A.S. contributed to the conception or design of the work and to the acquisition, analysis or interpretation of data for the work. G.d.G., C.F., A.M. drafted and revised the work critically for important intellectual content. C.C., V.C., L.I. and G.d.G. edited the final manuscript. G.B., G.C., M.C., G.C., M.T.F., A.O. ensured that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have reviewed the process of data analysis and writing of the manuscript and approved the final article.
Data Availability
The full data set of the study is in process of being stored at the data archive of the University of Milan Bicocca (see = ![]() ). The University of Milan Bicocca is one of the participating sites to the project. The storage of data is in process and we will shortly receive a DOI for the precise identification of the data set.
). The University of Milan Bicocca is one of the participating sites to the project. The storage of data is in process and we will shortly receive a DOI for the precise identification of the data set.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was funded by the Lombardy Region, grant CUP E42I14000280002 for ‘DISTURBI MENTALI GRAVI E RISCHIO DI VIOLENZA: UNO STUDIO PROSPETTICO IN LOMBARDIA’ with DECRETO D.G. SALUTE N. 6848, date 16.7.2014.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.