
Abstract
Objective:
The prevalence of mental illness among those in prison is much higher than in the community; however, very few studies have examined whether rates have changed over time, in line with increasing self-reported rates in the community.
Methods:
This study compares the prevalence of self-reported mental illness, self-harm and suicidal thoughts/behaviours, and drug and alcohol use across three waves (2001, 2009 and 2015) of health surveys involving men and women in New South Wales prisons and compared these rates with published community-level findings.
Results:
The prevalence of those reporting any mental health diagnosis increased significantly across the three surveys, even after adjustment for socio-demographic and criminal justice variables that also changed over time. Individuals surveyed in 2015 were more likely to report a mental health diagnosis than those surveyed in 2001 (adjusted odds ratio = 2.66, 95% confidence interval = [2.16, 3.27]). The prevalence of self-harm and suicidal thoughts and behaviours remained stable across the three surveys, while self-reported regular drug use decreased over the period. Women experienced a far greater burden of mental illness than men across all three surveys and experienced more growth in the prevalence of most psychiatric disorders.
Conclusion:
These findings have important implications for public and prison health systems given the poor social, health and criminal justice outcomes of those imprisoned with mental illness, both in custody and post-release.
Rates of mental illness in people imprisoned in Australia are higher than in the general population (Butler et al., 2006), a finding that is consistent with prison mental illness prevalence studies worldwide (Fazel and Seewald, 2012). Individuals in prison with mental illness are a highly vulnerable group who experience higher levels of disadvantage and ill-health prior to incarceration and more adverse social and health outcomes post-release than those without (Cutcher et al., 2014).
Accounting for the high prevalence of mental illness in prisons is complex. Mental illnesses across the diagnostic spectrum have been found to be associated with both violent and non-violent offending (Chowdhury et al., 2021; Stevens et al., 2015), and particular symptoms, such as paranoia and delusional beliefs, have been shown to be important in driving some offending behaviour (Coid et al., 2013, 2016). As well as having a direct impact on the likelihood of offending, mental illness is associated with a number of factors that may increase the risk of criminal justice contact such as substance use (Kopak, 2021) and socio-economic indicators such as homelessness, unemployment and financial hardship, suggesting a process of the ‘criminalisation’ of the socially disadvantaged (Baldry and Russell, 2017). Even among those who offend, those with mental illness have higher rates of conviction and incarceration (Stewart et al., 2020) and return to prison sooner after release (Cloyes et al., 2010; Stewart and Wilton, 2014).
Despite consistent findings regarding elevated rates of mental illness in prisons, prevalence estimates vary widely between studies. This is likely due, in part, to methodological heterogeneity, but may also reflect global variations in population rates of mental disorder and differences in policing, legal, health and prison systems (Fazel et al., 2016). The degree to which prevalence rates change over time in response to changes in the drivers of prison mental health burden is also unclear; just as with comparisons across jurisdictions, attempts to directly compare prevalence across time may be limited by variations in study methodology (Collishaw et al., 2004).
Bradley-Engen et al. (2010) examined the rates of individuals admitted to Washington State (USA) prisons with serious mental illness and co-occurring substance abuse between 1998 and 2006 and found that while the number of individuals admitted with serious mental illness increased during this time, admission base rates remained relatively stable. Fazel and Seewald’s (2012) updated meta-analysis found no statistically significant increase in rates of psychosis or major depression in prisons since their 2002 review, with the authors suggesting that this may be accounted for by higher rates of diversion away from the criminal justice system and improving standards of care for individuals with mental disorder who offend. However, a recent study conducted in Finland (Jüriloo et al., 2017) found a 10-fold increase in the number of incarcerated people with psychosis between 2005 and 2016 despite an overall decrease in prisoner numbers. Contrasting findings may of course indicate that trends in prevalence over time differ between jurisdictions.
General population trends in mental illness prevalence should also be considered when attempting to determine factors impacting rates in prison. A systematic review and meta-analysis of studies between 1978 and 2015 examining the global prevalence of adult mental illness excluding psychotic disorders (Richter et al., 2019) found a small but significant increase (odds ratio of 1.18) over time. Studies specifically examining psychotic disorders have reported relatively stable incidence rates over time (Kirkbride et al., 2012; Sutterland et al., 2013). In Australia, National Health Survey data show that the proportion of those reporting any mental or behavioural condition has been increasing, from around one in ten in 2001 to one in five in 2017–2018 (Australian Bureau of Statistics (ABS), 2001, 2018). Again, methodological differences, particularly with regard to sampling and defining/measuring mental illness, are likely to play a role in explaining differences between studies.
To date, no studies have directly examined the prevalence of mental illness in prison over time using data from repeated surveys. National data published at regular intervals by the Australian Institute of Health and Welfare (AIHW, 2010, 2019) on the health of people in prison has seen an overall upward trend in the rates of prison entrants reporting ever having been diagnosed with a mental health or substance use disorder, although no direct statistical analysis of this trend has been undertaken. The current study examines data from three large prison health surveys conducted in New South Wales (NSW) over a 15-year period, to determine whether the rates of mental illness in custody are increasing, in line with increases in self-reported mental illness in the general population and the apparent trend in national prison surveys. Any increase in the prevalence of mental illness in prisons over time has important implications for planning and resourcing both local health and prison services given the poorer health and criminal justice outcomes of this group.
Method
Sample
The current study compared three survey samples: the 2001 NSW Inmate Health Survey (Butler and Milner, 2003), the 2009 NSW Inmate Health Survey (Indig et al., 2010) and the 2015 Network Patient Health Survey (Justice Health and Forensic Mental Health Network, 2017). Each survey obtained a random sample stratified by age, sex and Aboriginal and/or Torres Strait Islander background, determined by the demographic distribution of the prisoner population. Women and Aboriginal and/or Torres Strait Islander individuals were oversampled for planned stratified analyses.
Participants were recruited from all operating adult prisons in NSW (excepting one in 2015 which did not grant research access for security reasons). Prior to each survey, a list of all individuals in custody and basic demographic information was obtained from correctional electronic records. A fixed sampling fraction was developed proportional to the size of the population of each prison, and a random sample was drawn according to sample and stratification targets.
Exclusion criteria for the 2001 survey consisted solely of insufficient English to comprehend the survey questions; the 2009 survey added lack of capacity to consent (i.e. due to intellectual disability or mental illness) and the 2015 survey extended the criteria to exclude those who posed a safety or security risk.
Written consent was obtained from participants in all surveys. The survey response rate was 85% in 2001, 85.4% in 2009, and 76% in 2015. Participating individuals had $10 deposited into their prison account post-participation.
A small number of participants who participated in more than one interview for the purpose of longitudinal analysis had data retained from the first survey in which they participated only (n = 123). In addition, 45 cases with missing essential demographic and mental health data were removed from the 2001 sample. The final total sample size was 2874: 869 from the 2001 survey, 964 from the 2009 survey and 1041 from the 2015 survey.
Measures
Surveys collected cross-sectional data on the health status of the NSW prison population. A range of physical health measurements and tests were undertaken by health staff and an interview covering demographic information, physical and mental health, drug and alcohol use and sexual health was conducted, in-person in 2001 and 2015, and via computer-assisted telephone interviewing in 2009.
Items that were the same or sufficiently similar across the three surveys were selected for analysis from socio-demographic, criminal justice, mental health and drug and alcohol domains. A new variable was created for each item and responses recoded where necessary to enable comparison.
Socio-demographic variables examined were gender, Aboriginal and/or Torres Strait Islander status, age, country of birth, marital status, and, at the time of incarceration, unemployment and homelessness (defined as ‘sleeping rough’, having no fixed address or having unsettled/temporary lodgings). Education level was not examined due to differences across surveys (i.e. ‘age left school’ vs ‘highest year of school completed’).
Criminal justice variables examined were legal status (remand/sentenced), first time in custody and violent offence (based on the most serious offence currently charged with or convicted of, with violence defined as assault, homicide or other acts intended to cause physical injury).
Mental health variables examined were lifetime mental health problems (ever told by a psychiatrist, doctor or clinician that they had a mental disorder), history of psychiatric admission in the community, current use of psychiatric medication and having ever been diagnosed with: depression, schizophrenia, bipolar disorder, anxiety, psychopathy/personality disorder, alcohol or drug problems/dependence, attention-deficit disorder or attention-deficit hyperactivity disorder (ADD/ADHD). Post-traumatic stress disorder (PTSD) was not examined as it was only specifically asked about in the 2015 survey. Three suicide/self-harm variables were examined: lifetime history of suicidal ideation, suicide attempts and self-harm (excluding suicide attempts). Variables were also created for comorbidity (both mental health diagnosis and history of illicit drug use), dual diagnosis (both a mental health diagnosis and alcohol/substance use disorder diagnosis), serious mental illness (schizophrenia, psychosis or bipolar disorder) and more than one mental health diagnosis.
Substance use variables covered lifetime substance use (ever having used illicit drugs), any illicit drug use in prison, and, in the 12 months before prison, regular (daily/almost daily) use of: cannabis, heroin, cocaine, MDMA/ecstasy and tranquilisers/sleeping pills. Amphetamine/ice use was only compared between 2009 and 2015 due to the wording of the 2001 survey not being sufficiently similar. A ‘hazardous drinker’ variable reflected a score of 8 or above on the Alcohol Use Disorders Identification Test (AUDIT; Saunders et al., 1993), which focused on alcohol use in the 12 months prior to custody.
Australian general population data were obtained to enable descriptive comparisons of trends in mental health and illicit drug use over the same period. An aggregate measure of mental health prevalence was obtained from published reports of the National Health Surveys completed by the ABS in 2001, 2007–2008 and 2014–2015 (ABS, 2001; 2008; 2015) in which participants were asked if they had any mental health or behavioural conditions that had lasted, or were expected to last, for at least 6 weeks. It is important to note that the 2014–2015 survey had an increased focus on mental and behavioural conditions in comparison with previous surveys which may have led to higher rates of reporting such conditions.
National rates of illicit drug use were obtained from the AIHW’s National Drug Strategy Household Surveys, completed in 2001, 2010 and 2016.
Statistical analysis
Data for each prison survey were weighted according to that year’s prison census to adjust for the oversampling of women and Aboriginal and/or Torres Strait Islander participants. The 2001 and 2009 surveys were also weighted for age to account for incidental oversampling of older and younger participants, bringing the samples as close as possible to the published composition of the prison population in the relevant year.
SPSS Statistics 27 was utilised to obtain descriptive statistics and chi-square analyses were conducted to test for differences between survey years for socio-demographic, criminal justice and drug and alcohol variables. A figure was produced to compare rates of mental illness and drug use across the survey years between the prisoner samples and the Australian general population. The weighted prevalence of mental health and self-harm variables was calculated by year and odds ratios obtained on a univariate basis for the overall sample and for men and women separately. Multivariate logistic regression was conducted for the overall sample to adjust for key factors found to have significantly changed across surveys.
Ethics approval
Ethical approval was granted by the Justice Health and Forensic Mental Health Network Human Research Ethics Committee (Ref: G365/14), the Corrective Services NSW Ethics Committee (Ref: D15/227697) and the Aboriginal Health and Medical Research Council Ethics Committee (1080/15).
Results
Socio-demographic and criminal justice characteristics
The unweighted and weighted prevalence of men and women, Aboriginal and/or Torres Strait Islander participants and median age for each survey year is presented in Table 1. The socio-demographic and criminal justice characteristics of the survey samples, weighted for age, gender and Aboriginal and/or Torres Strait Islander status are presented in Table 2. There was no significant difference in the gender ratio from 2001 to 2015. There was a significant increase in the proportion of Aboriginal and/or Torres Strait Islander individuals, from 15.1% in 2001 to 24.1% in 2015 (χ2 (2) = 24.19, p < 0.001) and those over the age of 40 (χ2 (4) = 36.33, p < 0.001).
Key sample characteristics and results of sampling strategies.
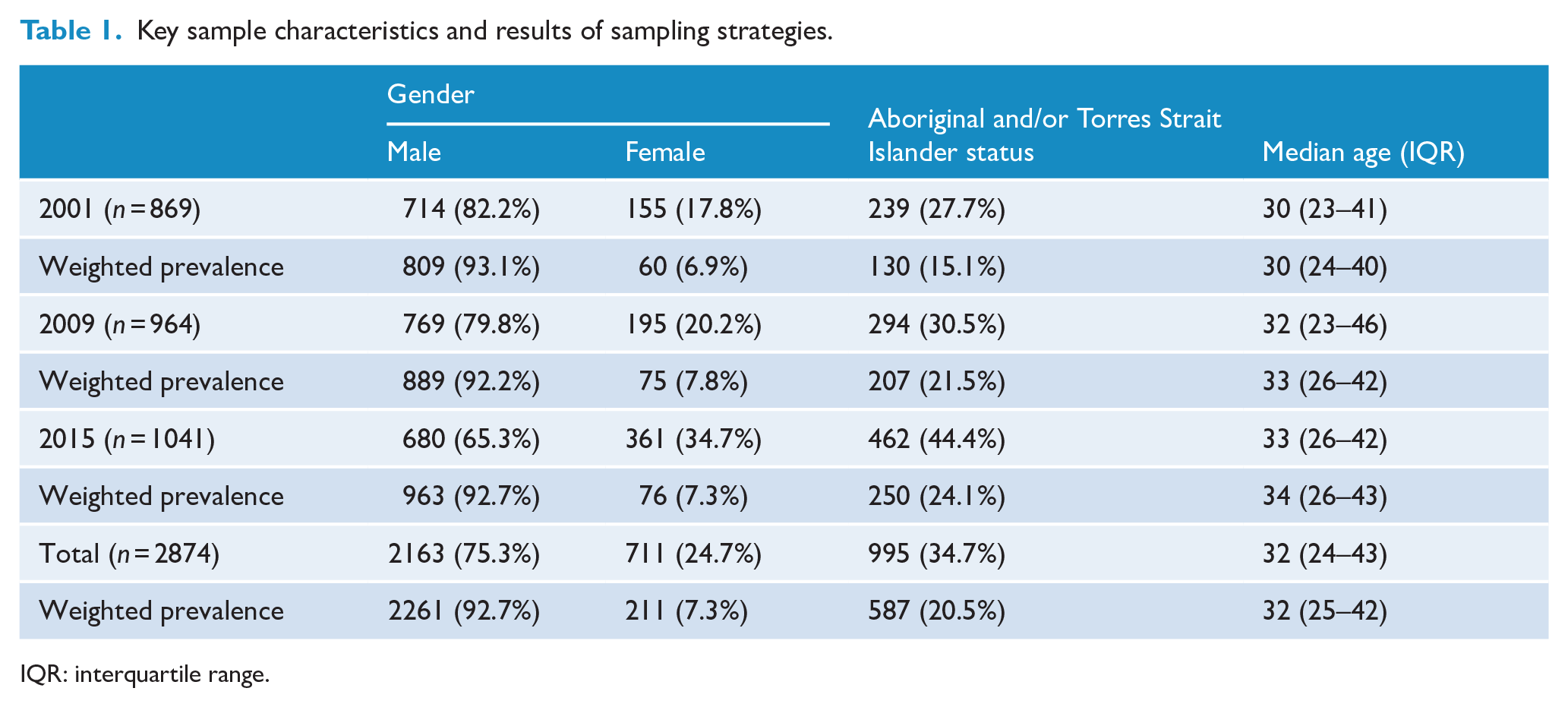
IQR: interquartile range.
Socio-demographic and criminal justice characteristics of the surveys.
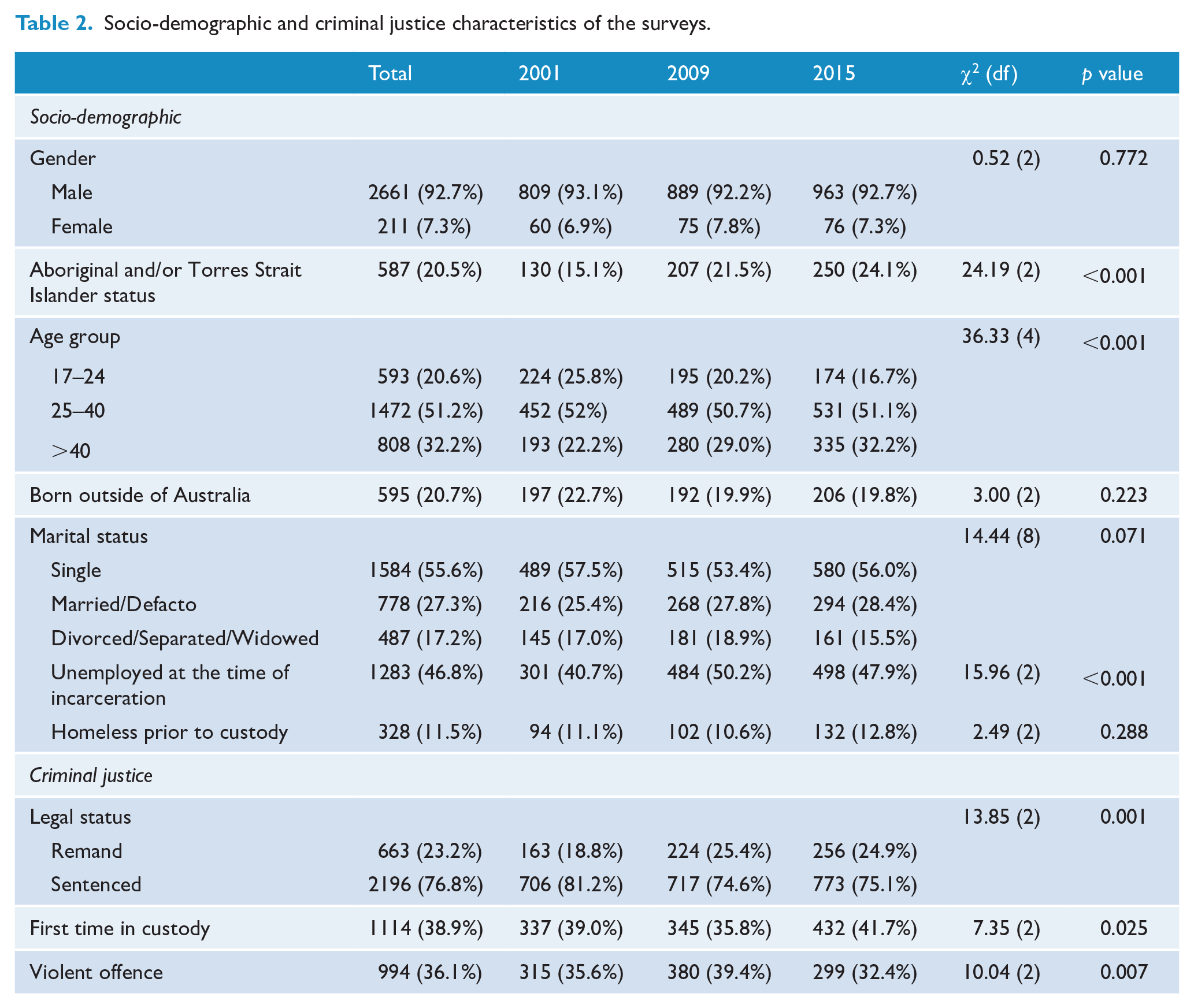
Respondents were significantly more likely to have been unemployed at the time of incarceration in 2009 (50.2%) and in 2015 (47.9%) compared to 2001 (40.7%; χ2 (2) = 15.96, p < 0.001), whereas rates of homelessness prior to custody remained stable at around one in ten. The number of individuals on remand increased across surveys (χ2 (2) = 13.85, p = 0.001), and the proportion of those who were in custody for the first time dropped from 39% in 2001 to 35.8% in 2009 before increasing to 41.7% in 2015 (χ2 (2) = 7.35, p = 0.025). The proportion of individuals with a violent offence increased from 35.6% in 2001 to 39.4% in 2009, before dropping to 32.4% in 2015 (χ2 (2) = 10.04, p = 0.007).
Prevalence of drug and alcohol use over time
A significant decrease in self-reported regular use of all substances in the 12 months prior to custody was observed between 2001 and 2009 (Figure 1). The most commonly used drug was cannabis (49.4% in 2001, decreasing to 24.8% in 2009), followed by heroin (34.2% declining to 9.5%). Cocaine use dropped from 21.8% to 6.9%, MDMA/ecstasy use dropped from 9.4% to 6.8% and misuse of tranquilisers/sleeping pills declined from 14.2% to 6.6%. Between 2009 and 2015, there was an increase in the reported regular use of all drugs, excepting amphetamines/ice which decreased from 45.9% in 2009 to 37.2% in 2015, and MDMA/ecstasy, which further declined to 4.9% by 2015. Where increases were seen, they were not a return to 2001 levels. Cannabis use increased from 24.8% in 2009 to 37% in 2015. Heroin use increased from 9.5% to 14%, cocaine use from 6.9% to 8.3% and misuse of tranquilisers/sleeping pills from 6.6% to 9.1%.
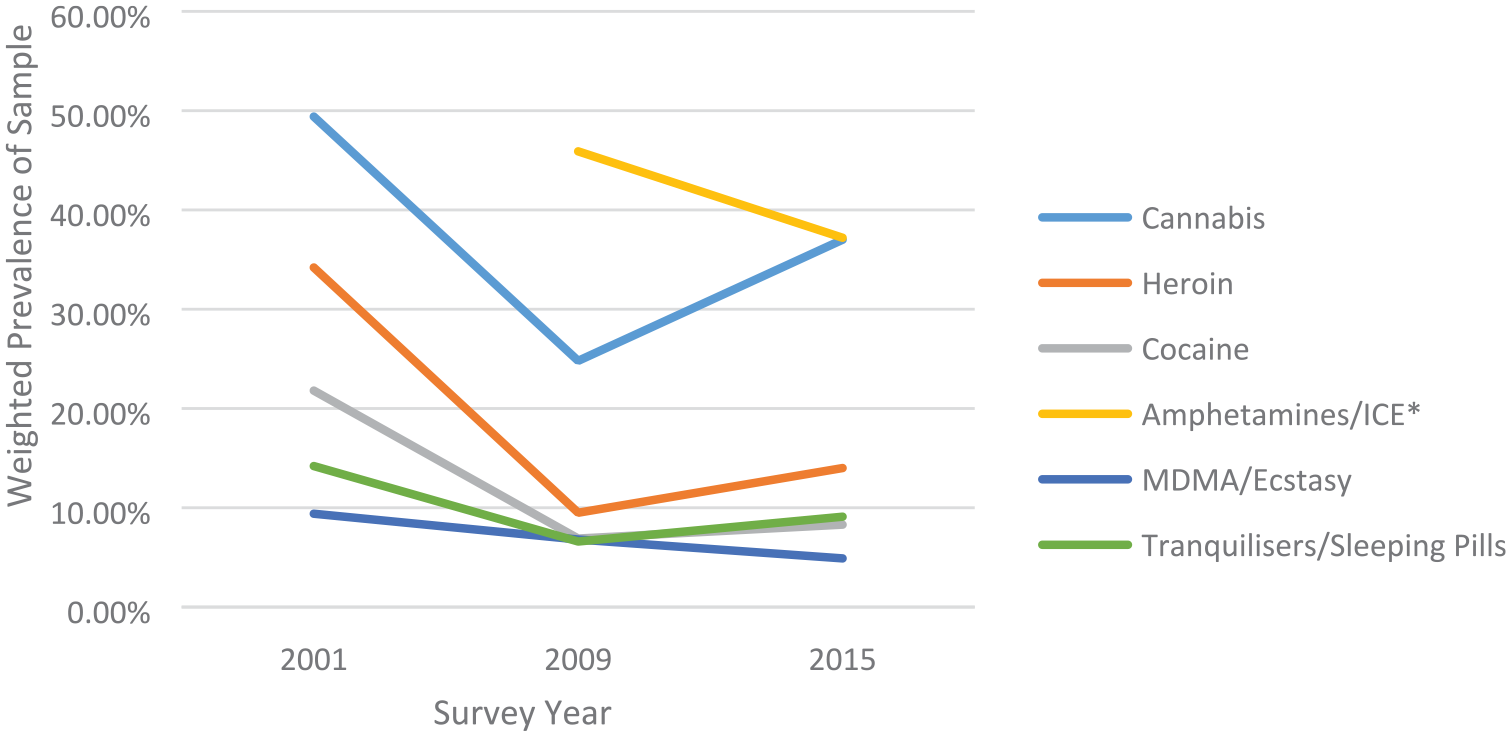
Regular drug use in the 12 months prior to custody, by survey year.
The opposite pattern was observed for problematic alcohol use, with an increase in the proportion of those classified as a ‘hazardous drinker’ between 2001 and 2009 (45.2–57.8%), declining back to 46.9% by 2015.
Prevalence rates for drug and alcohol variables over time and chi-square analyses are presented in Supplementary Table 1.
More than four in five individuals across the three surveys reported ever having used illicit drugs – approximately double the general population rate (Figure 2; AIHW, 2002, 2011, 2017). A slight increase from 2001 to 2009 was observed in the prison survey data (from 81.3% to 86.7%) before a decrease was then seen in 2015 (82.1%) as compared with a consistent but modest upward trend in the community sample.
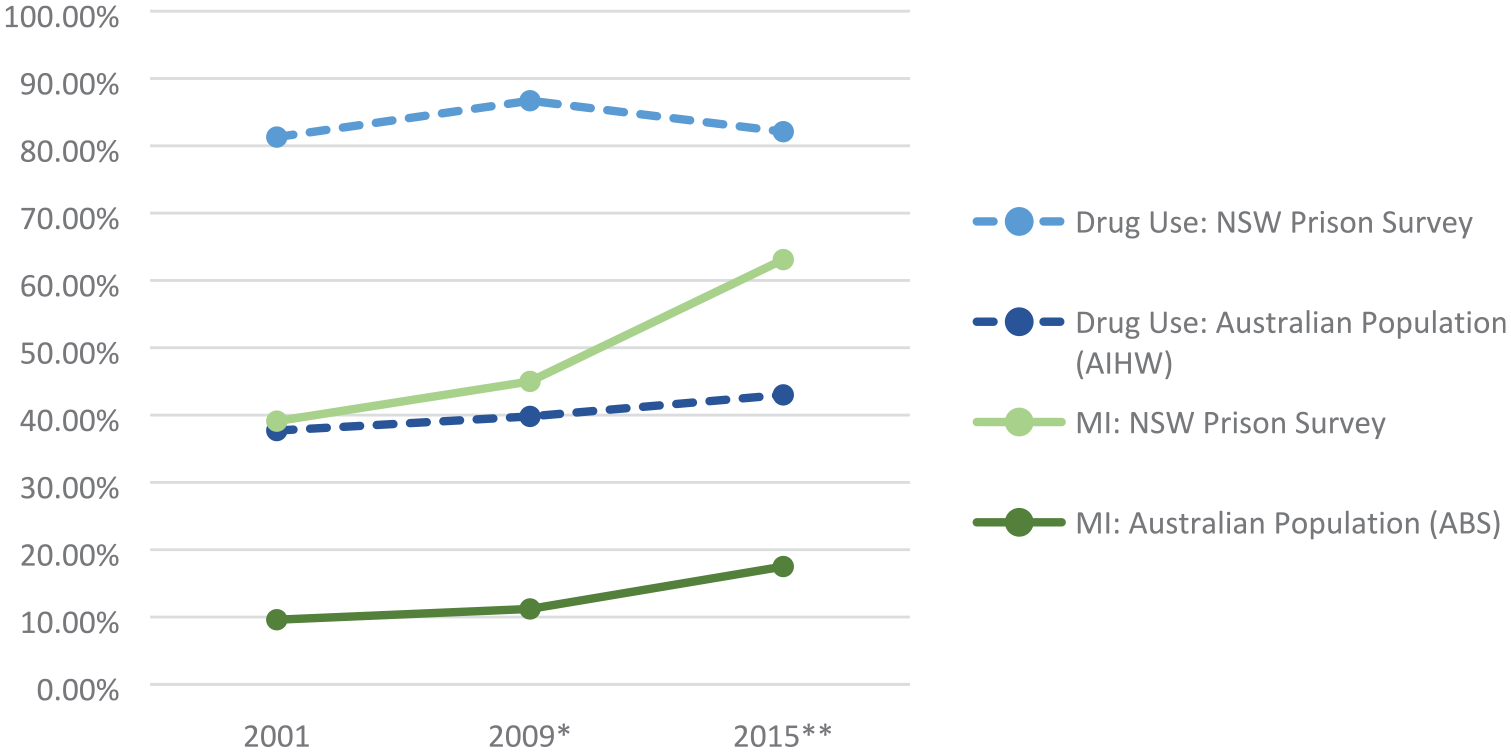
Prevalence of lifetime drug use and mental illness in NSW prisons and Australian community over time.
Prevalence of self-reported mental illness over time
The proportion of those reporting any mental health diagnosis steadily increased (Table 3), from 39.1% in 2001 to 63.1% in 2015 (odds ratio [OR] = 2.66, 95% confidence interval [CI] = [2.20, 3.20]). In 2015, participants were two and a half times more likely to report more than one mental health diagnosis (OR = 2.50, 95% CI = [2.03, 3.07]), and to be taking psychiatric medication (OR = 2.51, 95% CI = [1.99, 3.18]) than they were in 2001. Significant increases in all self-reported diagnoses between 2001 and 2015 were observed, with the exception of psychopathy/personality disorder.
Mental health variables over the three surveys – overall sample.
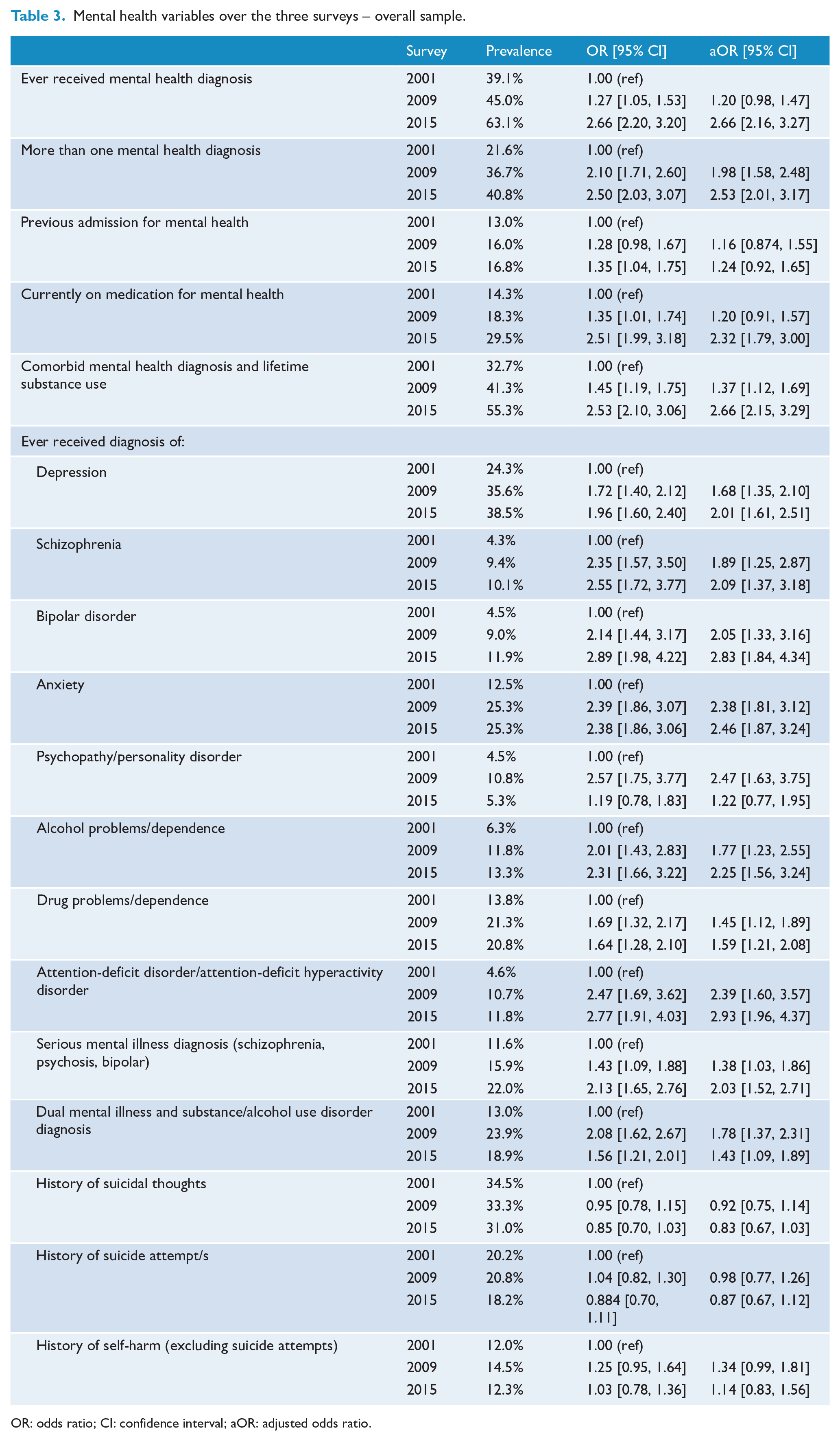
OR: odds ratio; CI: confidence interval; aOR: adjusted odds ratio.
Findings of increased prevalence remained significant after adjusting for socio-demographic and criminal justice factors that had also changed over time (Aboriginal and/or Torres Strait Islander status, age, legal status, unemployment status, violent offence and first time in custody). Even after adjustment, for example, participants were twice as likely to report a diagnosis of serious mental illness in 2015 than in 2001 (adjusted odds ratio [aOR] = 2.03, 95% CI = [1.52, 2.71]).
Those in custody reported substantially higher rates of lifetime mental health diagnosis than the general population (Figure 2). Both groups demonstrated an increased prevalence of mental illness over time, with individuals in prison being 1.6 times more likely to report a mental health diagnosis in 2015 (63.1%) than they were in 2001 (39.1%) and those in the general population being 1.8 times more likely to report a mental health diagnosis in 2015 (17.5%) than in 2001 (9.6%).
Prevalence of comorbidity and self-harm over time
The prevalence of mental health/drug and alcohol comorbidity significantly increased from around one third of the 2001 sample (32.7%) to over half in 2015 (55.3%), such that participants were two and a half more times more likely to report comorbidity in 2015 (OR = 2.53, 95% CI = [2.10, 3.06]). Participants were also more likely to report dual diagnosis over time (OR = 2.08, 95% CI = [1.62, 2.67] in 2009; OR = 1.56, 95% CI = [1.21, 2.01] in 2015).
Around one-third of each of the samples reported a history of suicidal thoughts (Table 3). Approximately one in five reported previously attempting suicide and approximately one in eight reported a history of self-harm. No significant change over time was observed for the self-harm variables.
Mental illness prevalence and gender
Across all surveys, women reported higher rates of all diagnoses than men except for schizophrenia, alcohol problems/dependence and ADD/ADHD and were more likely to report more than one mental health diagnosis, a history of psychiatric admission and current use of psychiatric medication (Supplementary Tables 2 and 3).
Around half of women (52.6%) reported a lifetime mental health diagnosis in 2001, increasing to over three-quarters (76.8%) in 2015 (OR = 2.98, 95% CI = [2.03, 4.38]). The prevalence for men increased from 38.2% in 2001 to 62.1% in 2015 (OR = 2.64, 95% CI = [2.12, 3.29]).
The most commonly reported diagnosis for both men and women was depression (Figures 3 and 4), with rates increasing by 2015 (OR = 1.95, 95% CI = [1.53, 2.47] for men; OR = 2.38, 95% CI = [1.65, 3.45] for women). The rates of anxiety also increased by 2015 and were particularly pronounced for women (OR = 5.53, 95% CI = [3.49, 8.75] vs OR = 2.20, 95% CI = [1.64, 2.94] for men).
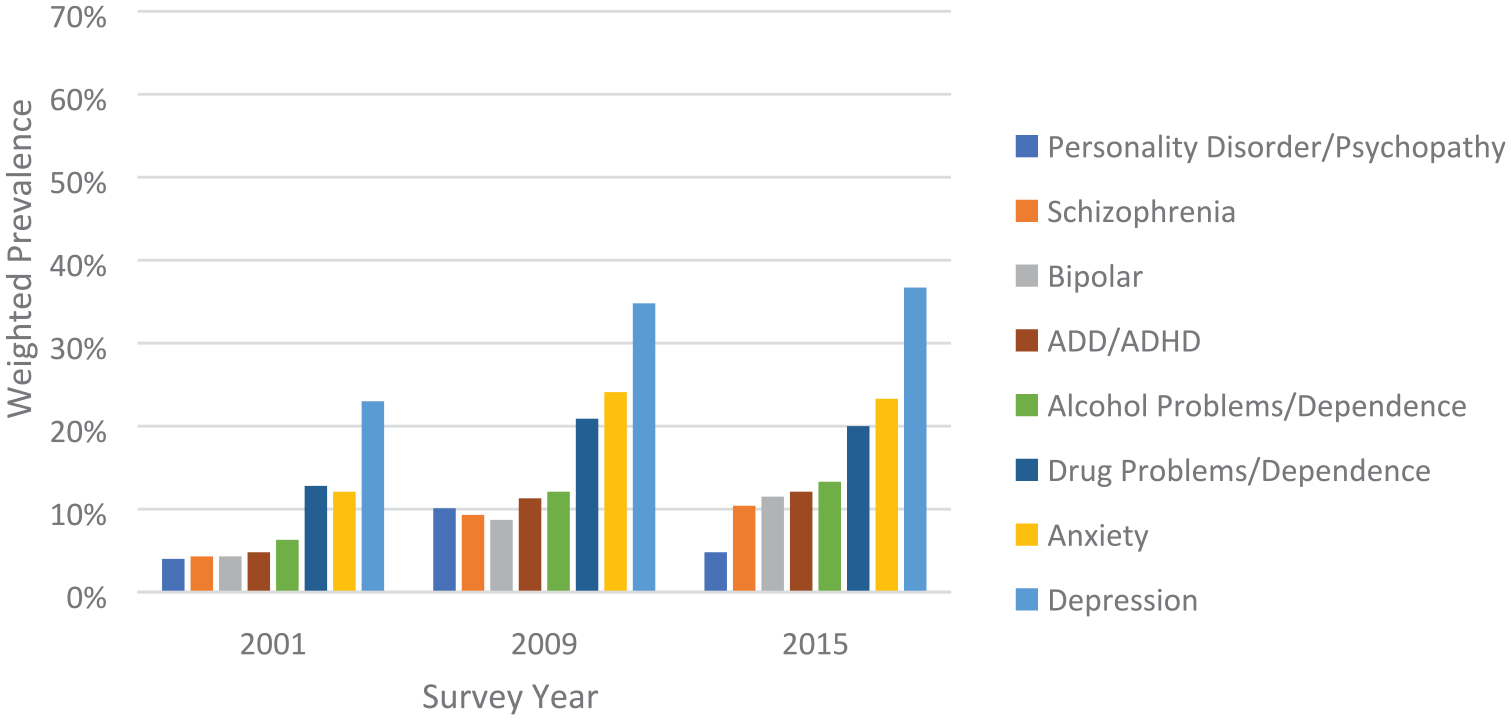
Self-reported mental health diagnoses by survey year for men.
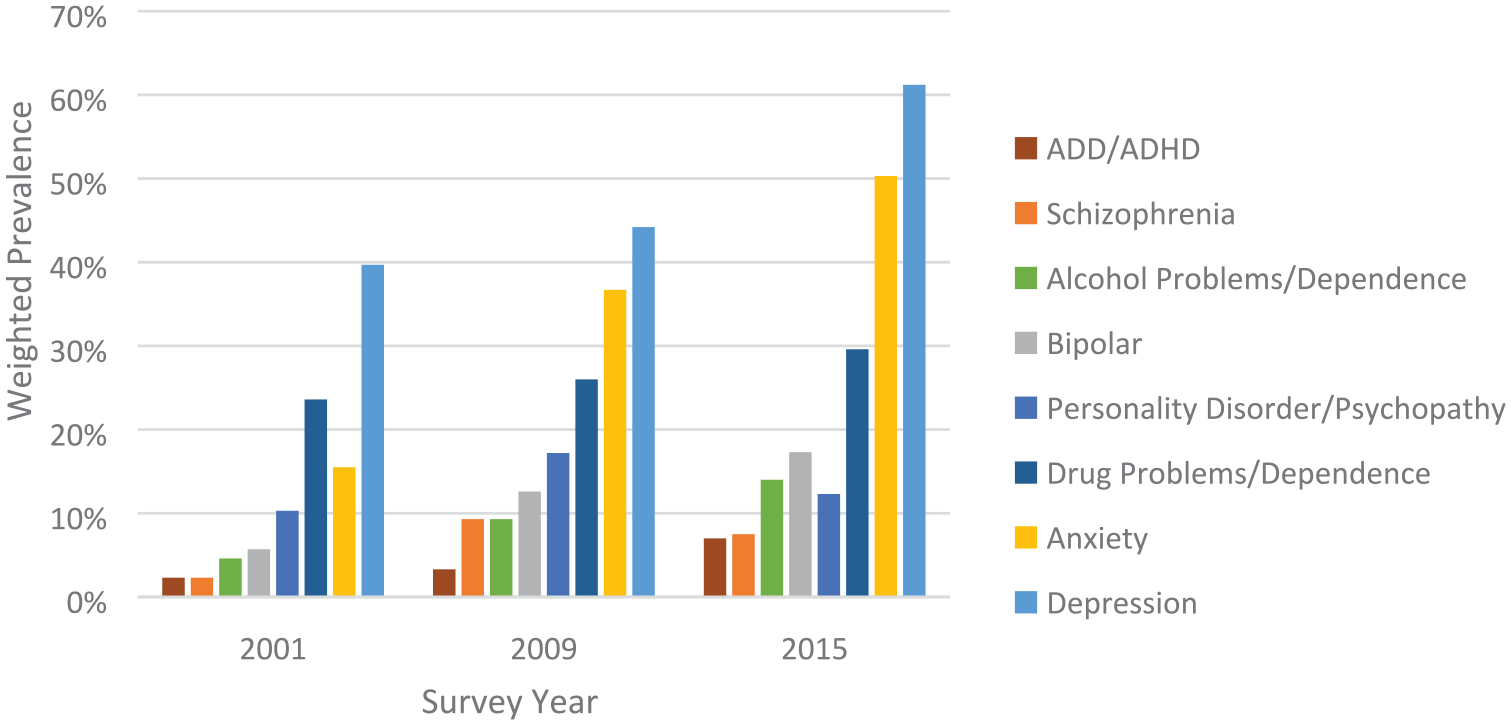
Self-reported mental health diagnoses by survey year for women.
While an equal proportion of men and women reported a lifetime diagnosis of schizophrenia in 2009, a higher proportion of men reported this diagnosis in 2001 and 2015. Prevalence increased over time, with men being around 2.5 times more likely to report a diagnosis in 2015 than in 2001 (OR = 2.53, 95% CI = [1.62, 3.94]) and women being around 3.5 times more likely to report a diagnosis (OR = 3.47, 95% CI = [1.20, 10.07]).
Survey participants were not asked about a diagnosis of PTSD prior to 2015 so differences over time could not be determined. In 2015, the prevalence was 10.4% of the overall sample, 20.1% of women and 9.7% of men.
Women were more likely than men to report mental health/drug and alcohol comorbidity across all surveys; however, a steeper rise in prevalence was observed in men: while women were twice as likely to report comorbidity in 2015 than they were in 2001 (64.4% vs 46.6%; OR = 2.07, 95% CI = [1.43, 2.99]), men were two and a half times more likely to report comorbidity (54.5% vs 31.6%; OR = 2.60, 95% CI = [2.08, 3.24]). Dual diagnosis was also higher among women, staying stable at around a quarter across the surveys while the proportion of men with dual diagnosis increased between 2001 and 2009 (OR = 2.26, 95% CI = [1.70, 3.02]). Despite dropping in 2015, prevalence still remained significantly higher than in 2001 (OR = 1.61, 95% CI = [1.19, 2.19]).
While the prevalence of historical suicidal ideation, suicide attempts and self-harm remained stable for both men and women over time, rates among women were consistently higher.
Discussion
In directly comparing three health surveys conducted in NSW prisons over a 15-year period, the current study demonstrates that the prevalence of self-reported mental illness has been increasing over time, in line with the increase seen in the general population. Both men and women in custody experienced an increasing mental health burden across the full spectrum of diagnoses. These findings have implications for the level of resources needed in prisons to meet increasing levels of mental health need and add urgency to efforts focused on addressing the criminalisation of mental illness.
Main findings
Significant changes occurred in the socio-demographic and criminal justice profile of those in NSW prisons between 2001 and 2015. Our findings reflect an ageing prison population with increasing numbers of individuals on remand, which, aside from potentially impacting the rates of mental illness in custody, has important implications for healthcare provision. Notably, there was a significant increase over time in the proportion of Aboriginal and/or Torres Strait Islander people in custody, with more than a quarter of those incarcerated identifying as Aboriginal and/or Torres Strait Islander in 2015 despite making up only 2.9% of the NSW general population (ABS, 2016), highlighting the importance of addressing the enduring overrepresentation of Indigenous people in custody.
The proportion of those reporting any mental health diagnosis, a serious mental illness diagnosis and more than one diagnosis all increased significantly between 2001 and 2015. Increases in nearly all self-reported diagnoses were observed, even after adjustment for socio-demographic and criminal justice factors that had also changed over time. When compared with published general population figures over a comparable period, individuals in prison reported much higher rates of mental illness, consistent with previous research (Butler et al., 2006). Both the prison and community samples demonstrated a pattern of increasing prevalence over time. While no previous studies have directly compared repeated prison surveys, the results of the current study contrast with findings suggesting little change in the prevalence of mental illness in prisons worldwide between 2002 and 2010 (Fazel and Seewald, 2012). This reinforces the benefits, and justifies the investment in, undertaking repeated cross-sectional surveys.
It is possible that the increasing rates of mental disorder both in the community and in prison reflect a growing awareness of mental illness and higher rates of diagnosis rather than an increase in underlying mental ill health. Health service utilisation among Australians with mental and substance use disorders increased between 2006–2007 and 2011–2012 (Harris et al., 2015), which may partly account for an increase in diagnoses. The number of individuals receiving Medicare-subsidised mental health services has also been consistently increasing since the introduction of the Better Access to Mental Health Care initiative in 2006 (AIHW, 2021). However, the use of these services is determined by socio-economic and geographical factors, and the most disadvantaged and remote communities (from which many of those involved with the criminal justice system come) have much lower rates of service utilisation (Meadows et al., 2015). Hence, this is unlikely to fully account for the increased rate of self-reported mental illness we observed in our sample.
Substance use problems are almost ubiquitous among those in contact with the criminal justice system and in the current study participants reported lifetime use of illicit drugs at a rate double that of the general population (AIHW, 2002, 2011, 2017). Interestingly, while the prevalence of diagnosed drug or alcohol problems/dependence and dual diagnosis increased significantly in prison between 2001 and 2015, the proportion of those reporting regular use of any substance in the 12 months prior to custody decreased in line with a broader pattern of decreasing substance use in the community (AIHW, 2020b). Increasing diagnoses in the context of reducing rates of self-reported drug use may reflect an increasing recognition that drug and alcohol problems represent a diagnosable health condition and consequently we may be observing an increase in diagnostic rates rather in the actual rates of substance use. Individuals in custody may also be more likely to receive a diagnosis of substance use disorder, with one survey finding that prison entrants were more likely to have seen a drug and alcohol professional during a previous prison term than they were in the community (AIHW, 2019).
The proportion of individuals in prison with a history of suicidal thoughts and behaviour is much higher than in the community; around one third of our sample reported a history of suicidal thoughts in contrast to 13.3% in the community (Slade et al., 2009), and around one-fifth reported a previous suicide attempt as opposed to 3.3% in the community. That the prevalence of those reporting histories of self-harm and suicidal thoughts/behaviour remained stable over time in the context of increasing rates of mental illness is an interesting finding given the strong association between the two. This may provide additional support for the idea that the rising rates of self-reported mental illness may reflect increasing rates of diagnosis rather than mental illness per se.
Findings for men and women
Reflecting higher rates of mental illness among women both in the general population (AIHW, 2020a), and in custody (Sirdifield et al., 2009; Tyler et al., 2019), women in this study reported higher rates of most psychiatric diagnoses, psychiatric hospitalisation, prescribed medication and self-harm than their male counterparts. They also demonstrated stronger growth in the prevalence of nearly all diagnoses between 2001 and 2015, even for the two diagnoses where prevalence was higher in men (schizophrenia and ADD/ADHD). The one diagnosis where growth was stronger for men over time was drug problems/dependence. However, despite rates in this diagnosis remaining stable for women, a greater proportion of women than men reported drug problems/dependence across all surveys. It has previously been reported that women in prison are more likely than men to have substance use disorders (Indig et al., 2016), which contrasts starkly with the fact that, in the general population, men have more than twice the rate of substance use disorder than women (ABS, 2008). This speaks to the ‘gender gap’ in imprisonment: with men forming the vast majority of the prison population, only the most disadvantaged women in the community are incarcerated. The mental health needs of women in prison are clearly very high and, as the current study suggests, are only increasing with time. This, along with a growing female prison population, highlights the particular importance of prioritising the mental health needs of women in prison and strategies to prevent their incarceration.
Strengths/limitations
To our knowledge, this is the first study to examine the prevalence of mental illness in a prison population over time by directly comparing results from repeated surveys employing comparable methodologies and to compare trends with published community-level data. Furthermore, trends over time for men and women were examined separately, an important addition given the relative dearth of prison research focusing on or including sufficient numbers of women.
While the questions examined across the three prison surveys were largely consistent, some changes in measurement did occur over time. The wording of some items and response choices differed between surveys, and while we only compared questions that we deemed sufficiently similar, we are unable to gauge the impact of any change in wording on responses. Where survey items were not present or consistent across surveys, we were unable to make comparisons, meaning that trends in the prevalence of important factors (e.g. PTSD diagnosis or methamphetamine use) were unable to be determined.
Finally, mental illness prevalence in the current study was estimated based on self-report and findings may have differed if diagnostic interviews had been employed. This self-report method, however, was consistent across surveys, and so any errors arising from it are unlikely to have influenced the upward trend that was observed.
Conclusions/implications
Mental illness is a growing concern both in the community and in prison. While the high prevalence among those in prison is well established, the current study suggests that rates are increasing over time. More research is required to replicate this finding in other jurisdictions and to investigate the underlying causes of the increase. From a public health perspective, the implications of an increasing proportion of those in custody suffering mental illness are far-reaching considering the poorer health and social outcomes and increased risk of recidivism and reincarceration for this group when released. Prison presents an opportunity for the identification and treatment of this under-serviced, high-need group, and prison mental health services must be adequately resourced and supported to do this. While we do not propose prison as a therapeutic intervention, certain aspects of prisons are likely to be conducive to improved mental state such as the imposition of a structured routine, along with provision of regular meals, opportunities for sleep, reduced access to illicit substances and alcohol, and potentially increased access to mental health treatment. Evidence suggests that those entering prison with existing mental health and substance use problems can experience improvements in mental health and reduction of symptoms over a period in custody (Dirkzwager and Nieuwbeerta, 2018). While some of the apparent improvement seen is likely to be related to mental distress peaking at the beginning of incarceration, it can also be seen as an indictment of community mental healthcare provision and the absence of opportunities for successful diversion. Under-resourced and under-supported community-based mental health services, along with inadequate numbers of inpatient mental health beds, can mean that those experiencing mental health crises are at increased risk of ending up in contact with the criminal justice system. It is also likely that the potential to be gained from mental health court diversion is not being realised currently. Albalawi et al. (2019) found that almost three quarters of those coming before the courts in NSW with a diagnosis of psychotic illness were given punitive sanctions rather than treatment orders, and another study found that only 57.3% of those eligible for diversion were actually granted diversion by magistrates in NSW (Soon et al., 2018). These studies also found inequity in access, with lower rates of diversion among Aboriginal and/or Torres Strait Islander individuals and those with comorbid substance use problems.
Finally, supporting the continuity of mental health care between prison and the community post-release is important, given that those with mental illness are at increased risk of experiencing multiple incarcerations (Baillargeon et al., 2009). Intervention during the early post-release period for those with mental illness can increase contact with community mental health services and reduce the risk of reincarceration (Hawthorne et al., 2012; Hopkin et al., 2018). Collaboration between prison and community mental health services to support successful transitions is vital.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221104411 – Supplemental material for The prevalence of self-reported mental illness among those imprisoned in New South Wales across three health surveys, from 2001 to 2015
Supplemental material, sj-docx-1-anp-10.1177_00048674221104411 for The prevalence of self-reported mental illness among those imprisoned in New South Wales across three health surveys, from 2001 to 2015 by Christie C Browne, Daria Korobanova, Natalia Yee, Sarah-Jane Spencer, Trevor Ma, Tony Butler and Kimberlie Dean in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.