
Abstract
Background:
Childhood neglect is a risk factor for subsequent mental health problems. However, research on the unique contribution of emotional and physical subtypes of neglect is lacking. Importantly, if emotional and physical neglect have different impacts on mental health, they must be examined separately to understand how to prevent and treat their effects.
Objective:
This study aimed to examine associations of emotional and physical neglect with depression, anxiety, stress, alcohol and drug use in 18- to 20-year-olds.
Methods:
Participants (N = 569, mean age = 18.9, 70% female) responded in an online survey to questions on childhood emotional and physical neglect, childhood abuse, symptoms of depression, anxiety and stress, and alcohol and drug use and problems. Procedures were approved by the University of Sydney Human Ethics Committee. Hierarchical linear regressions were performed, controlling for socio-demographic characteristics and other adverse childhood experiences.
Results:
Combined neglect was associated with depression (B = 2.895, p < 0.001), anxiety (B = 1.572, p = 0.003) and stress (B = 1.781, p = 0.001). However, a second model entering emotional and physical neglect as separate exposures revealed emotional neglect was driving this association with depression (B = 2.884, p < 0.001), anxiety (B = 1.627, p = 0.001) and stress (B = 1.776, p = 0.001), and that physical neglect was not associated with any outcome. Neither emotional nor physical neglect were associated with alcohol or drug use.
Conclusion:
Emotional neglect is a risk factor for mental health problems in early adulthood. Research that combines emotional and physical neglect into a single exposure may be obscuring relationships with mental health. Mental health prevention and treatment must screen for, and address, emotional neglect.
Introduction
Childhood maltreatment has consistently been identified as a major risk factor for the subsequent development of mental health and substance use (MHSU) problems (Gardner et al., 2019; Kisely et al., 2020). Childhood maltreatment is typically considered as encompassing any of the five following experiences before the age of 18 years: abuse (physical, sexual or emotional) or neglect (emotional or physical). Different types of maltreatment commonly co-occur and approximately 35% of those who experience any maltreatment will be exposed to more than one type (Edwards et al., 2003). Research on maltreatment has focused predominately on the deleterious effects of physical and sexual abuse. In contrast, neglect has received much less empirical attention, despite being more commonly experienced (Child Family Community Australia, 2017) and demonstrating severe effects on subsequent mental health. Indeed, neglect is associated with depression (Infurna et al., 2016; Spatz Widom et al., 2007), anxiety (Gardner et al., 2019), adolescent binge drinking (Shin et al., 2013), underage initiation of alcohol use (Dube et al., 2006), adolescent alcohol use frequency (Shin et al., 2009) and cannabis abuse (Abajobir et al., 2017).
The lack of attention to neglect is even more pervasive when considering specific subtypes of neglect, such as physical and emotional neglect. Physical neglect represents inadequate physical care, such as food, hygiene or medical care, while emotional neglect refers to a failure to meet the emotional needs of a child, such as support, affection and ensuring a child feels loved (Dube et al., 2003). When neglect is included in MHSU research, it is often focused solely on physical neglect. This is the case in large epidemiological datasets on which much evidence has been generated, such as the National Comorbidity Survey (Kessler et al., 1994), as well as a host of other studies (Oshri et al., 2017; Shin et al., 2009; Shin et al., 2013), particularly those that rely on Child Protective Service investigations. Alternatively, a combined measure of physical and emotional neglect has been used, and indeed Australian prevalence estimates are based on a combined category of neglect (Abajobir et al., 2017; Child Family Community Australia, 2017; Infurna et al., 2016). However, should these subtypes have different associations with MHSU, empirical evidence that fails to include emotional neglect, or distinguish between these two subtypes, may be obscuring the relationship with mental disorders.
From a theoretical perspective, the lack of focus on the effects of emotional neglect is surprising. Attachment disturbance provides insight into possible underpinnings of later psychopathology following maltreatment. Through repeated experiences of the provision (or lack) of support and comfort, a child develops an internal working model that determines expectations about attachment figures (see Schechter and Willheim, 2009). Fear of abandonment as well as parental inconsistency and distorted interactions can result in the insecure attachment styles of ambivalent, avoidant and disorganised attachment (see Sciarrino et al., 2018). Attachment insecurity is linked to child and adolescent difficulties in a range of areas known to be risk factors for mental disorder, such as problems with emotion regulation and interpersonal relationships, representations of the self, and internalising and externalising symptoms (Fearon et al., 2010; Madigan et al., 2013; Mikulincer and Shaver, 2012), and reflects the often transgenerational nature of maltreatment.
Subsuming physical and emotional neglect into one category carries two major assumptions: first, that these experiences co-occur and therefore it is difficult to meaningfully separate their unique effects; and second, that they exert the same impact on MHSU in the same manner. Regarding the first assumption, while there is a high degree of co-occurrence between all maltreatment types, empirical evidence does not uphold the assumption that emotional and physical neglect are more commonly co-occurring than other types. A community sample of US adults revealed that people who experienced emotional neglect were 12.2 times more likely to have experienced physical neglect, compared to those who had not experienced emotional neglect (Dong et al., 2004). However, odds were greater for overlap between physical abuse with emotional abuse, and emotional neglect with emotional abuse (odds ratios of 17.7 and 12.9, respectively). In addition, 30% of adults reporting maltreatment experienced both emotional and physical neglect (Witt et al., 2017). Thus, there is not strong support for the first assumption of a combined construct of emotional and physical neglect based on their co-occurrence.
Regarding the second assumption, that physical and emotional neglect have the same impact on mental health development, empirical evidence has produced mixed findings. Existing evidence from clinical patient samples retrospectively reporting neglect suggests emotional neglect may be more strongly associated with mental disorders than physical neglect. While associations were not significant for physical neglect, emotional neglect was associated with current depression, anxiety and substance use disorders among adult outpatients (Salokangas et al., 2020), and depression, social and trait anxiety, and worse self-esteem among adults with diagnosed social anxiety disorder compared to controls without any anxiety disorder (Kuo et al., 2011). Moreover, a systematic review found emotional, but not physical, neglect to be associated with mood and substance use disorders (Carr et al., 2013). Indeed, children raised in institutional care show higher rates of psychiatric and behavioural disorders than children never placed in institutional care (Zeanah et al., 2009). Institutional rearing typically meets a child’s basic physical needs but has inadequate resources to attend to their emotional needs, including availability of one specific caregiver.
Among non-patient samples, findings are mixed. Both emotional and physical neglect were predictive of early onset of alcohol use in a sample of adults (Dube et al., 2006) and significantly associated with virtually all lifetime substance use disorders in a nationally representative sample of 34,653 US adults (Afifi et al., 2012). A prospective longitudinal study among adolescents revealed both physical and emotional neglect predicted depression, posttraumatic stress disorder (PTSD), illicit drug use and smoking at 3 years follow-up (Cohen et al., 2017). However, other studies suggest emotional neglect may be more important for MHSU. A meta-analysis including both population-based, community samples and clinical samples found significantly stronger associations between emotional neglect and depression than physical neglect (Humphreys et al., 2020). In addition, emotional, but not physical neglect, was found to predict alexithymia (difficulty identifying and communicating emotion, a risk factor for mental disorder) in a community sample of 90 adults, and predicted worse functioning in subjects with high alexithymia (Aust et al., 2013). Finally, some community samples suggest physical neglect may be more strongly associated with MHSU disorders. While associations were not significant for emotional neglect, physical neglect increased the odds of lifetime alcohol dependence in a nationally representative sample of US adults (Fenton et al., 2013) and was associated with greater prevalence of clinically significant anxiety or depression among Finnish men (Rehan et al., 2017).
Thus, there is a substantial lack of consistency regarding the role of emotional and physical neglect for MHSU outcomes. Several gaps in our understanding are evident. First, only two of the reviewed studies controlled for other adverse childhood experiences (ACEs), such as parental psychopathology or domestic violence. Disruptions to early parenting are common to both exposures such as parental psychopathology and emotional neglect. While some of the impact of parental psychopathology on MHSU outcomes likely operates through neglectful parenting, other symptoms of parental psychopathology such as hostile or aggressive behaviour may impact child development in different ways. Given co-occurrence between these exposures, to understand the effect of neglect, it is important to control for these other traumatic childhood experiences. Second, there is a lack of data on young adult samples. This is important, as approximately three-quarters of all lifetime cases of mental disorders have their onset prior to age 24 (Kessler et al., 2005), highlighting the importance of prevention in young adulthood. Finally, there is a dearth of evidence on the impact of neglect on MHSU from an Australian context.
Importantly, if emotional and physical neglect are distinct in their co-occurrence and their impact on MHSU, conclusions based on a single category of neglect may be erroneous. Subsequent policy, research attention and community action may be misplaced. This study therefore aimed to determine (1) the co-occurrence between emotional and physical neglect among young Australian adults; (2) whether emotional and physical neglect are differentially associated with MHSU in a community sample of young adults, controlling for other ACEs; and (3) whether there are differences in MHSU outcomes when using a combined measure of neglect compared to separate exposures of emotional and physical neglect.
Methods
Sample and procedures
The current study is a secondary analysis of baseline data collected for the Australian arm of the International Study of Prosocial and Anti-social Behaviour (Basto-Pereira et al., 2019). Recruitment advertisements were circulated on Facebook and Twitter and via professional networks. Eligible participants were between the ages of 18 and 20 years old, fluent in English and residing in Australia. A total of 582 young adults participated. Thirteen participants were excluded due to incomplete data on the maltreatment variables, leaving a sample of 569 participants.
Participants provided written, informed consent online, then proceeded to an online, confidential survey that took 15–30 minutes to complete. Data were collected from November 2018 to June 2019. Participants who completed the survey were entered into a prize draw to win a $500 gift voucher. Procedures were approved by the University of Sydney Ethics Committee.
Measures
Maltreatment
Participants were asked about five types of maltreatment before the age of 18: emotional and physical neglect, and emotional, physical and sexual abuse. These items were sourced from the Family Health History Questionnaire (Dube et al., 2003; Felitti et al., 1998), which has demonstrated sound internal consistency (Ford et al., 2014).
Four of the maltreatment variables (emotional neglect, physical neglect, emotional abuse and physical abuse) were measured on a 5-point scale (1 = never true, 2 = rarely true, 3 = sometimes true, 4 = often true, 5 = very often true). Physical abuse also included a 5-point scale on the severity of spanking. For each category, scores were summed with higher scores indicating more frequent/severe experiences, and a dichotomous score was created to reflect the presence of absence of this experience (0 ‘no’, 1 ‘yes’). The threshold reflecting presence was 14 for emotional neglect, 8 for physical neglect, 12 for emotional abuse, and 8 for physical abuse, which corresponds to endorsing at least ‘rarely true’/‘a little hard’ on all items, or more frequently (sometimes, often/severely) on a subset of items. This has been used previously to define physical neglect and was applied to all maltreatment variables (excluding sexual abuse) to ensure consistency (Dube et al., 2003).
Emotional neglect was measured by seven items. Six items were reverse-coded and measured the frequency participants knew there was someone to take care of them/protect them, helped them feel important or special, they felt loved, their family looked out for each other, felt close to each other and was a source of support. One item was not reverse-coded: thinking their parents wished they had not been born. Physical neglect was measured by four items, assessing how often the participants did not have enough to eat, their parents were too drunk/high to take care of the family, they had to wear dirty clothes and that there was someone to take them to the doctor if they needed it (reverse-coded). Emotional abuse was measured by six items: people in the family called them things like lazy or ugly; said hurtful/insulting things to them; they believe they were emotionally abused; an adult living in their home swore, insulted or put them down; threatened to hit or throw something at them; and acted in a way that made the participant afraid they would be physically hurt. Physical abuse was measured by four items: how often an adult in the home pushed/grabbed/shoved/slapped/threw something at the participant, hit the participant so hard they had marks or were injured, and how often and how severely they were spanked.
Sexual abuse was assessed through four dichotomous questions asking whether an adult or someone at least 5 years older than the participant had ever, against the participant’s wishes, touched or fondled the participant’s body in a sexual way; was made to touch another’s body in a sexual way; whether the adult or person ever attempted to have, or actually had, any type of sexual intercourse with the participant. A dichotomous variable for any sexual abuse was created (0 ‘no’, 1 ‘yes’) whereby a ‘yes’ response to any of the above items against the participants wishes constituted sexual abuse, consistent with previous literature (Afifi et al., 2012).
A variable of combined neglect was created to mirror literature that fails to distinguish between the two subtypes. Scores on both the emotional and physical neglect items were summed, and a dichotomous variable was created to represent any neglect (0 ‘no’, 1 ‘yes’). The threshold for this variable was 22, consistent with the other maltreatment variables; that is, reflecting at least ‘rarely true’ on all items or more frequently (sometimes, often).
MHSU
Depression, anxiety and stress symptoms over the past week were measured using the respective subscales of the Depression Anxiety and Stress Scales (DASS) 21-item (Lovibond and Lovibond, 1995). Each subscale had seven items, with responses on a 4-point scale from 0 (did not apply to me) to 3 (applied to me very much or most of the time). Scores on each subscale were summed to create a total, ranging from 0 to 21, with higher scores representing poorer mental health. The DASS 21-item has shown good reliability and validity in non-clinical samples (Antony et al., 1998). Depressive symptoms measured emotions such as not being able to experience any positive feeling or difficulty working up the initiative to do things. Scores of 5–6 indicate mild symptoms, 7–10 indicate moderate symptoms, 11–13 indicate severe symptoms, and scores 14 and above are extremely severe. Anxiety symptoms measured feelings such as feeling scared without any good reason, and physical sensations such as being aware of dryness of the mouth. Scores of 4–5 indicate mild symptoms, 6–7 indicate moderate symptoms, 8–9 indicate severe symptoms, and scores 10 and above are extremely severe. Stress symptoms measured feelings such as finding it hard to wind down and feeling they were using a lot of nervous energy. Scores of 8–9 indicate mild symptoms, 10–12 indicate moderate symptoms, 13–16 indicate severe symptoms, and scores 17 and above are extremely severe.
Alcohol use and related problems was measured using the Alcohol Use Disorders Identification Test (AUDIT) (Saunders et al., 1993). Scores for each item were summed to create a total ranging from 0 to 40, with higher scores representing greater alcohol use and related problems. The AUDIT has sound test–retest reliability, sensitivity, specificity and internal consistency (de Meneses-Gaya et al., 2009). Scores of 8–14 indicate harmful alcohol use and scores 15 and above suggest the presence of alcohol dependence.
Drug use and related problems was measured using the 11-item Drug Use Disorders Identification Test (DUDIT) (Berman et al., 2003). Scores for each item were summed to create a total ranging from 0 to 44, with higher scores reflecting higher drug use and problems. The DUDIT has sound reliability and validity (Hildebrand, 2015). Drug-related problems are indicated for scores of six or more (males) or two or more (females).
Covariates
Socio-demographic covariates included gender (male, female, transgender, other gender identification), age, education (completed high school or not) and socio-economic status (SES). SES was a combination of years of education completed and profession for the caretaker with the highest level, or the participant themselves if they indicated they were financially independent. SES was categorised into low (routine or semi-routine occupations), medium (occupations requiring high school education or specialised skill) and high (managerial and professional occupations requiring college education) (Basto-Pereira and Farrington, 2019).
Other ACEs (excluding maltreatment items) were entered as dichotomous covariates. Items were from the Family Health History questionnaire (Felitti et al., 1998). These included the following experiences prior to the age of 18: a household member suffered from a mental illness, attempted suicide, was incarcerated, used street drugs or was a problem drinker; parents were separated/divorced; or the child was exposed to domestic violence in the home.
Analysis
Analyses were run using SPSS version 26. Multicollinearity for the ACEs and maltreatment variables was assessed and found to be acceptable. Phi correlation coefficients (ø) were calculated to determine the correlation between the dichotomous maltreatment variables. Hierarchical linear regressions were run for each outcome. Socio-demographic covariates were entered in a first block, followed by ACE covariates in a second block. In a final block, maltreatment variables were entered. Two models were compared: Model 1 entered sexual, physical and emotional abuse, and the combined variable of ‘Neglect’ (both physical and emotional neglect). Model 2 entered each of the five maltreatment variables (sexual, physical and emotional abuse, and physical and emotional neglect). Where emotional neglect was a significant predictor in these models, a second model was run whereby all other maltreatment variables were entered in block 3, and emotional neglect was entered in block 4. This was to examine the incremental variance accounted for by emotional neglect.
Results
Sample characteristics
The total sample size was 569 participants (70% female; 26% male; 2% transgender; and 2% did not identify as either male, female or transgender). The average age was 18.9 years (SD = 0.824). Participant SES revealed 13.4% were of low SES, 37.4% medium SES and 49.2% high SES. Almost all had completed secondary school (94%).
Table 1 shows the frequency and types of ACEs experienced, and mean scores and clinical levels on outcome measures. Living with someone who was depressed or mentally ill was the most common ACE, experienced by over half of the sample. Emotional abuse was the most commonly experienced form of maltreatment. Over 70% of the sample experienced at least one type of maltreatment, and of those experiencing any maltreatment, the average number of types experienced was 2.33 (SD = 1.16). The sample showed mild to moderate levels of mental health problems, and low risk of alcohol dependence and drug problems.
Descriptive statistics on predictor and outcome variables.
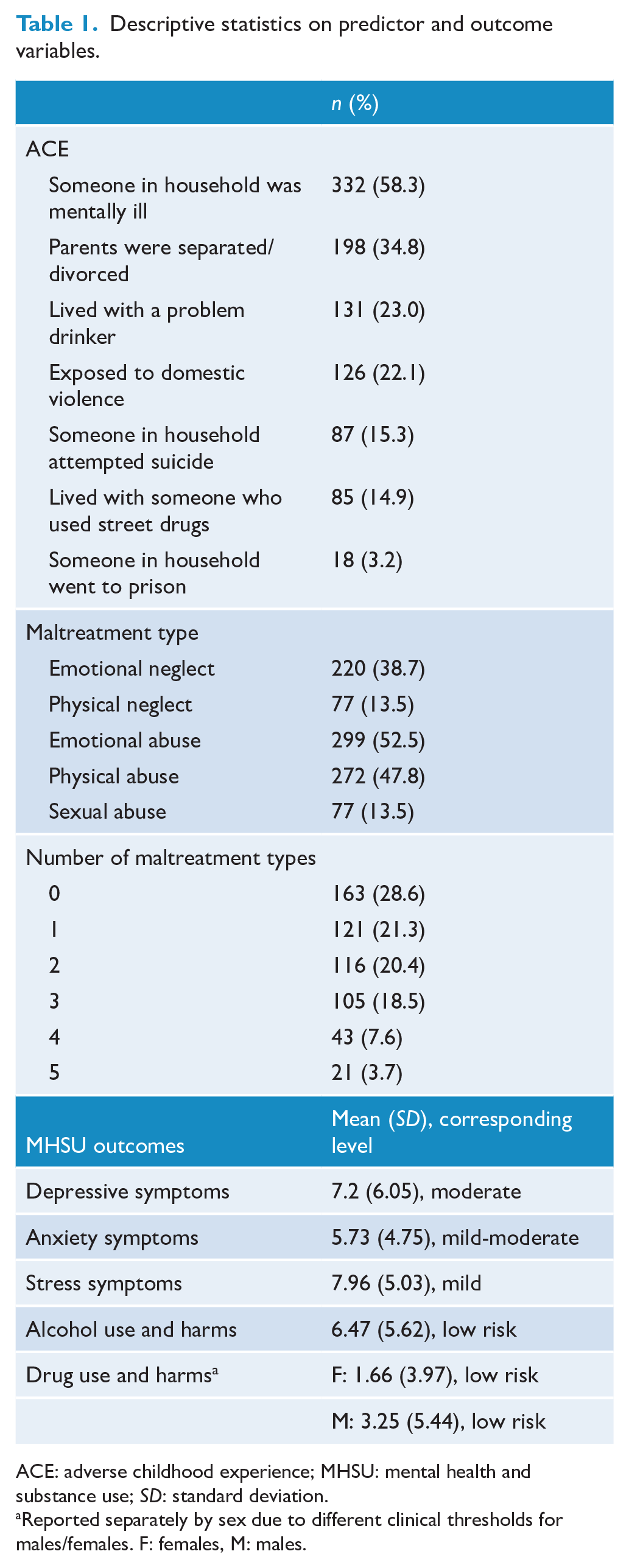
ACE: adverse childhood experience; MHSU: mental health and substance use; SD: standard deviation.
Reported separately by sex due to different clinical thresholds for males/females. F: females, M: males.
All maltreatment variables were significantly correlated (p < 0.001). Emotional neglect was most strongly correlated with emotional abuse (ø = 0.538), followed by physical neglect (ø = 0.340), physical abuse (ø = 0.266) and sexual abuse (ø = 0.161).
Experiencing both emotional neglect and emotional abuse was the most common co-occurrence of maltreatment types (n = 190, 33.4%), followed by experiencing both emotional neglect and physical abuse (n = 142, 25%), then emotional and physical neglect (n = 62, 10.9%), and emotional neglect and sexual abuse (n = 45, 7.9%).
Associations with MHSU
Tables 2–6 show the regression coefficients and variance explained for each MHSU outcome.
Linear regression predicting depression scores.
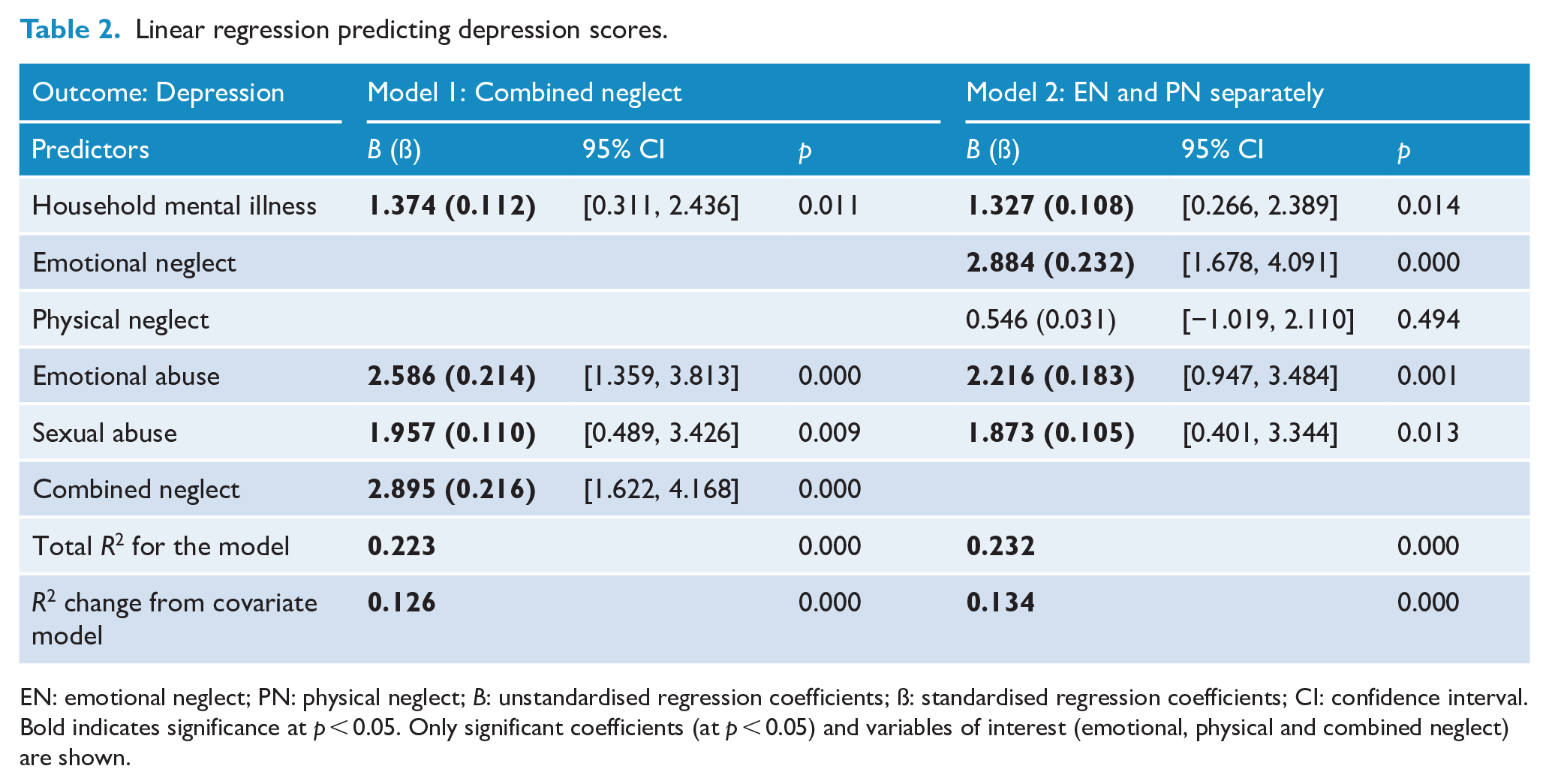
EN: emotional neglect; PN: physical neglect; B: unstandardised regression coefficients; ß: standardised regression coefficients; CI: confidence interval. Bold indicates significance at p < 0.05. Only significant coefficients (at p < 0.05) and variables of interest (emotional, physical and combined neglect) are shown.
Linear regression predicting anxiety scores.
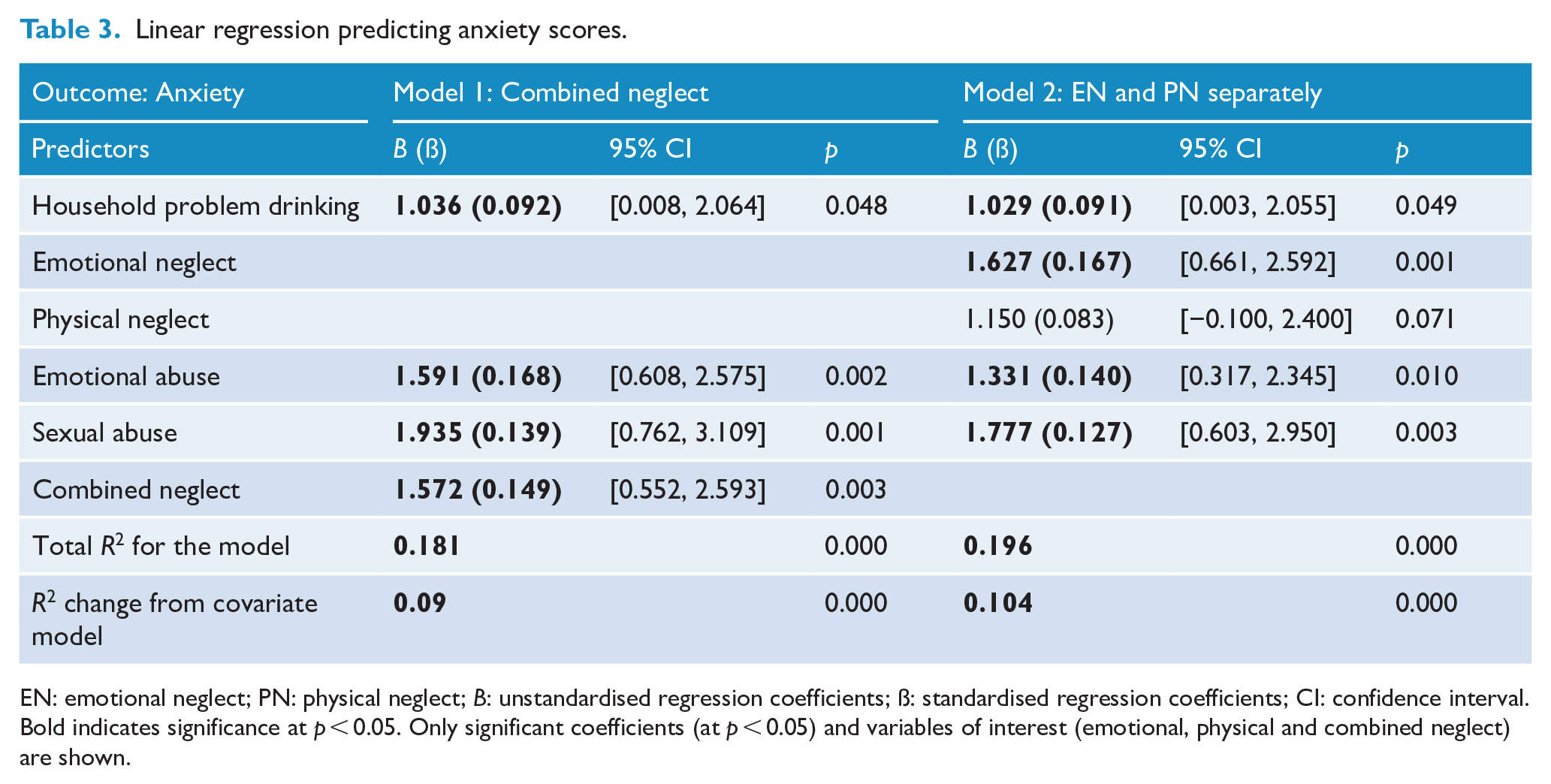
EN: emotional neglect; PN: physical neglect; B: unstandardised regression coefficients; ß: standardised regression coefficients; CI: confidence interval. Bold indicates significance at p < 0.05. Only significant coefficients (at p < 0.05) and variables of interest (emotional, physical and combined neglect) are shown.
Linear regression predicting stress.
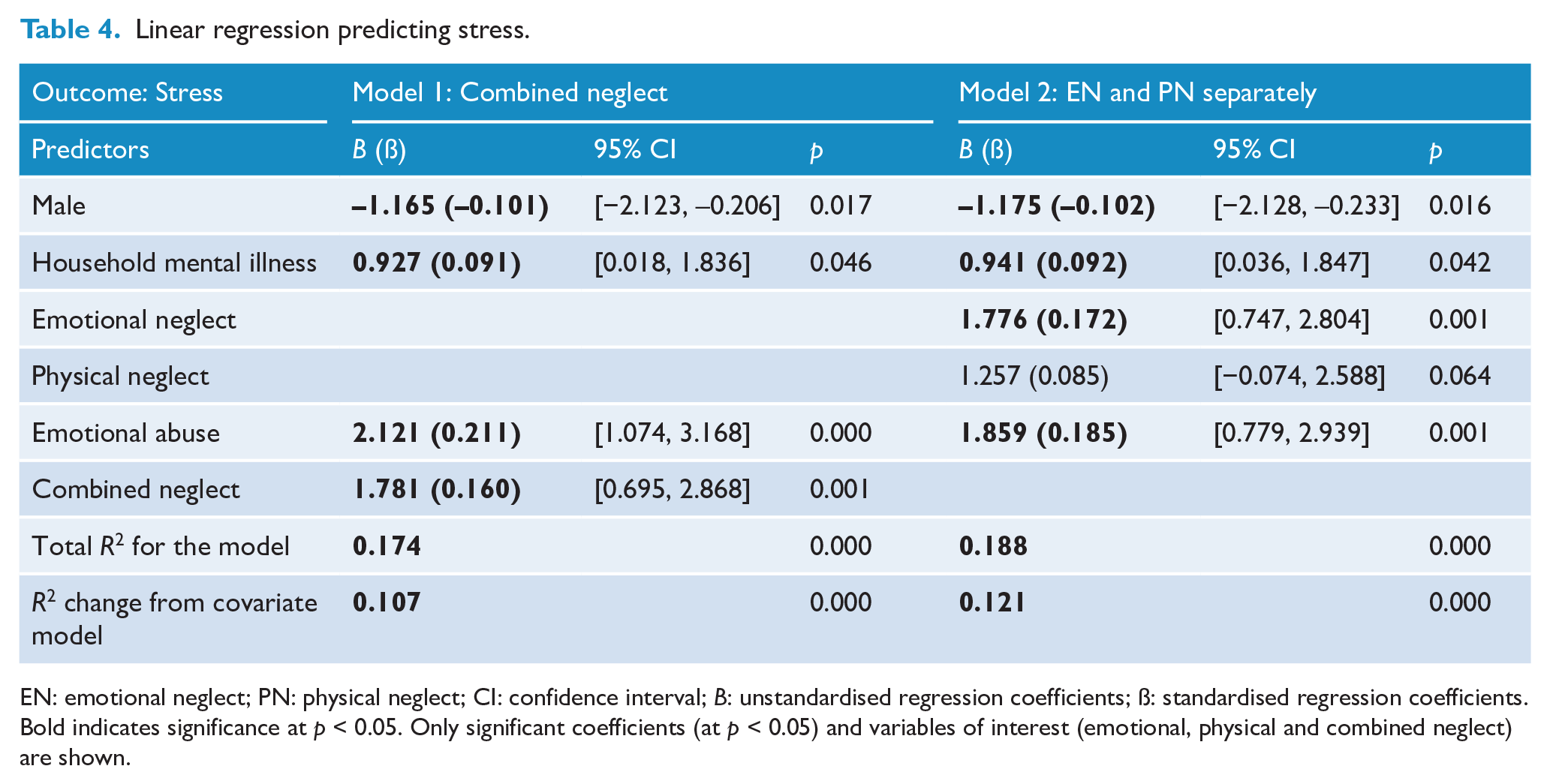
EN: emotional neglect; PN: physical neglect; CI: confidence interval; B: unstandardised regression coefficients; ß: standardised regression coefficients. Bold indicates significance at p < 0.05. Only significant coefficients (at p < 0.05) and variables of interest (emotional, physical and combined neglect) are shown.
Linear regression predicting alcohol use.
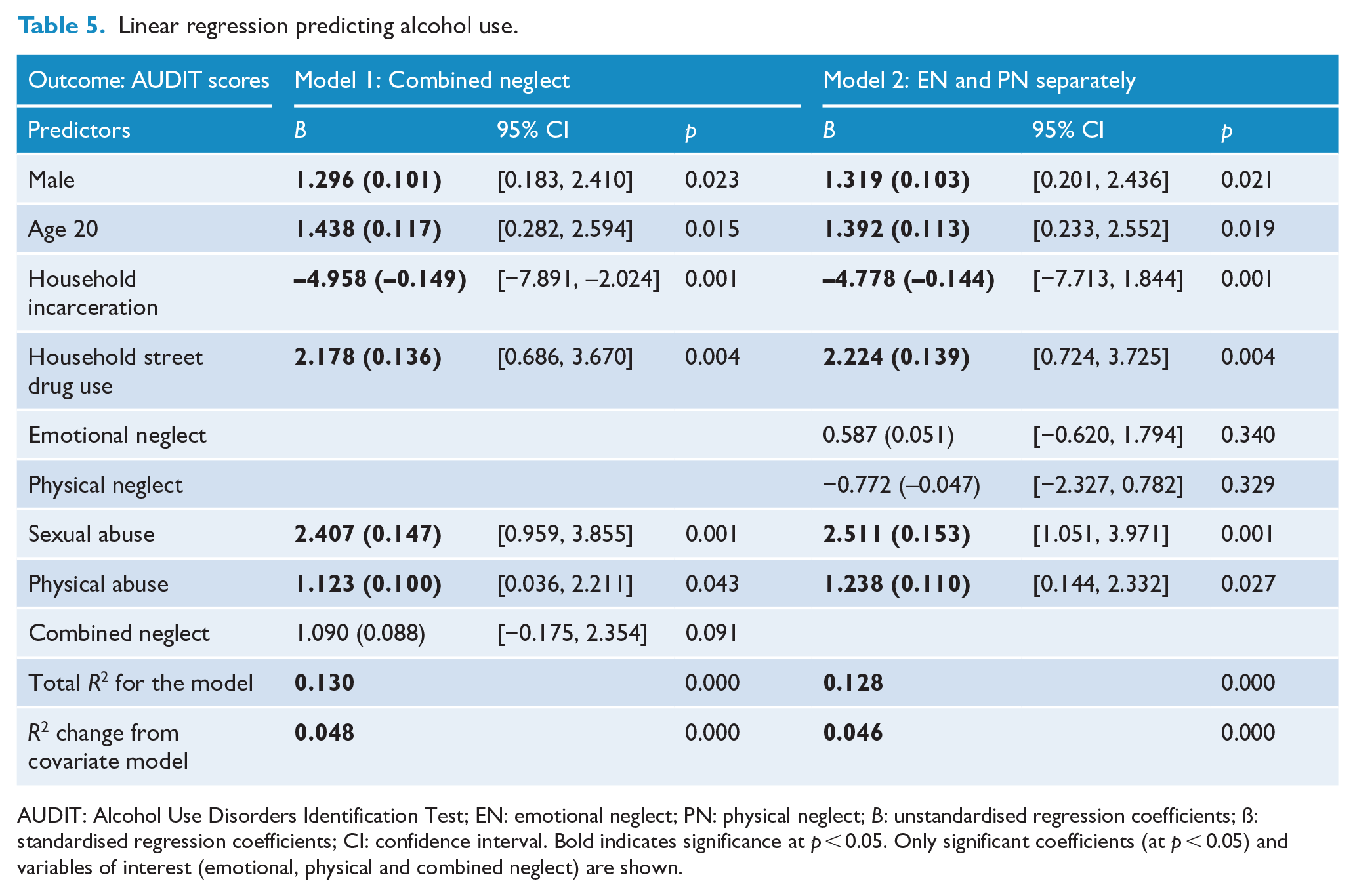
AUDIT: Alcohol Use Disorders Identification Test; EN: emotional neglect; PN: physical neglect; B: unstandardised regression coefficients; ß: standardised regression coefficients; CI: confidence interval. Bold indicates significance at p < 0.05. Only significant coefficients (at p < 0.05) and variables of interest (emotional, physical and combined neglect) are shown.
Linear regression predicting drug use.
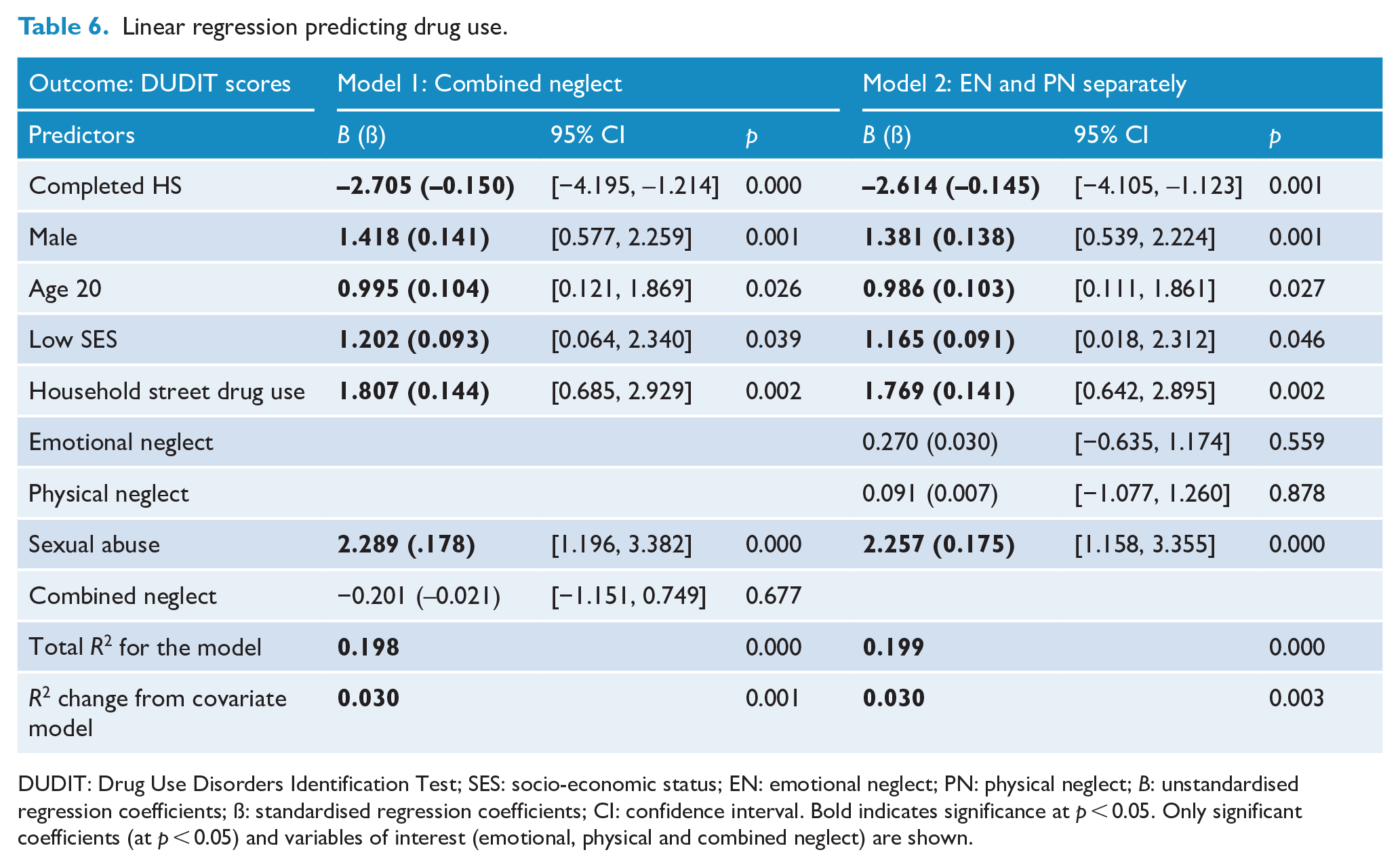
DUDIT: Drug Use Disorders Identification Test; SES: socio-economic status; EN: emotional neglect; PN: physical neglect; B: unstandardised regression coefficients; ß: standardised regression coefficients; CI: confidence interval. Bold indicates significance at p < 0.05. Only significant coefficients (at p < 0.05) and variables of interest (emotional, physical and combined neglect) are shown.
Depression
Both the socio-demographic (R2 = 0.046, p = 0.002) and ACE covariate (R2 = 0.052, p < 0.001) models significantly predicted depressive symptoms. After entering all covariates, emotional neglect accounted for 9.7% of the variance in depressive symptoms.
Using combined neglect for Model 1, the overall model accounted for 22.3% of the variance in depressive symptoms, p < 0.001. Living with a household member who was depressed or mentally ill significantly predicted depressive symptoms. Emotional abuse, sexual abuse and combined neglect were associated with greater depressive symptoms compared to those not exposed.
Entering emotional and physical neglect separately increased the variance explained (R2 = 0.232, previous R2 = 0.223). Emotional neglect, emotional abuse and sexual abuse were significant predictors of depressive symptoms. Physical neglect was not. Emotional neglect accounted for an additional 3.4% of the variance in depressive symptoms, above all covariates and other maltreatment types (p < 0.001).
Anxiety
The socio-demographic covariate model was not a significant predictor of anxiety symptoms (R2 = 0.028, p = 0.070). The ACE covariate model was significant (R2 = 0.092, p < 0.001). Emotional neglect accounted for an additional 6.3% of the variance in anxiety symptoms (p < 0.001), above covariates.
Using combined neglect for Model 1, the overall anxiety model accounted for 18.1% of the variance (p < 0.001). Living with someone who was a problem drinker predicted greater anxiety symptoms. Experiencing emotional abuse, sexual abuse and combined neglect were associated with increased anxiety symptoms.
Entering emotional and physical neglect separately increased the variance explained in anxiety symptoms (R2 = 0.196, previous R2 = 0.181). Emotional neglect, emotional abuse and sexual abuse significantly predicted increased anxiety symptoms. Physical neglect was not a significant predictor. Emotional neglect accounted for an additional 1.7% of the variance in anxiety scores, after controlling for all covariates and other maltreatment types (p = 0.001).
Stress
Both the socio-demographic (R2 = 0.031, p < 0.05) and ACE (R2 = 0.037, p < 0.01) covariate models significantly predicted stress symptoms. After entering all covariates, emotional neglect accounted for 7.6% of the variance in stress.
Using combined neglect for Model 1, the overall stress model accounted 17.4% of the variance and was significant (p < 0.001). Being male significantly predicted lower stress compared to females, while living with someone with a mental illness predicted greater stress. Emotional abuse and combined neglect predicted greater stress compared to not experiencing these maltreatment types.
Separating emotional and physical neglect, Model 2 accounted for more of the variance in stress (R2 = 0.188, previous R2 = 0.174). Emotional neglect and emotional abuse were significant predictors of stress. Physical neglect did not significantly predict stress. Emotional neglect accounted for an additional 1.9% of the variance in depressive symptoms, above and beyond all covariates and other maltreatment types (R2 = 0.019; p = 0.001).
Alcohol use
The socio-demographic block was not significant (R2 = 0.026, p = 0.098), though the ACE covariate model significantly predicted alcohol use (R2 = 0.082, p < 0.001). After covariates, emotional neglect accounted for 0.8% of the variance in alcohol use (p = 0.04). Using combined neglect, Model 1 accounted for 13% of the variance in alcohol use (p < 0.001). Being male predicted greater alcohol use compared to being female, as did being age 20 compared to age 18, and living with anyone who used street drugs. Living with someone who went to prison predicted less alcohol use than not. Physical and sexual abuse predicted increased alcohol use compared to no exposure. Emotional abuse and combined neglect were not significant predictors.
Entering emotional and physical neglect separately, Model 2 accounted for marginally less of the variance in alcohol use, but remained significant (p < 0.001). Significant predictors from Model 1 remained significant in Model 2. Emotional neglect, emotional abuse and physical neglect did not predict alcohol use.
Drug use
Both the socio-demographic (R2 = 0.103, p < 0.001) and ACE (R2 = 0.169, p < 0.001) covariate models significantly predicted drug use. After entering covariates in Blocks 1 and 2, emotional neglect did not significantly contribute to the drug use model (R2 = 0.002, p = 0.258).
Using combined neglect for Model 1, the drug use model accounted for 19.8% of variance in drug use (p = 0.001). Being male compared to female, being age 20 compared to age 18, having low SES compared to high SES, and living with anyone who used street drugs predicted greater drug use. Having completed high school predicted less drug use. Sexual abuse predicted greater drug use compared to no exposure and was the only significant maltreatment predictor of drug use.
Model 2 accounted for the same proportion of variance in drug use and was significant p = 0.003. All predictors from Model 1 remained significant. Emotional neglect, emotional abuse, physical abuse and physical neglect did not significantly predict drug use.
Discussion
To our knowledge, the current study represents the first examination of the mental health consequences of emotional neglect in a sample of young adults in Australia. Results highlight that emotional and physical neglect are distinct experiences. Indeed, emotional and physical neglect do not show the strongest correlation or most common co-occurrence among the different maltreatment types.
Results reveal neglect is associated with mental health outcomes, though due to emotional neglect in particular. When separated into distinct exposures, models explained more of the variance in each mental health outcome and emotional neglect was an important predictor of depression, anxiety and stress. In contrast, physical neglect was not. For mental health research, conclusions based on a combined category of neglect may lead to incorrect conclusions that physical neglect is important for mental health among young Australians, when instead, emotional neglect is driving the association. For substance use, neither emotional nor physical neglect were significant predictors.
This study aligns with previous work demonstrating emotional neglect to be associated with a range of mental disorders (Carr et al., 2013). Evidence for the association between physical neglect and mental health is weaker, with systematic reviews finding either null or weaker associations between physical neglect and mental health compared to emotional neglect (Carr et al., 2013; Humphreys et al., 2020). Evidence from clinical samples in particular more consistently demonstrates emotional, but not physical neglect, to be important for mental health (Kuo et al., 2011; Salokangas et al., 2020). The current study adds to the literature of emotional neglect and mental health in community samples, demonstrating that those exposed to emotional neglect show poorer mental health than those not exposed (Aust et al., 2013; Cohen et al., 2017).
The finding that neglect was not associated with alcohol and drug use was somewhat surprising, although there is substantial heterogeneity in the literature. Analysis of a nationally representative sample from the United States found both subtypes of neglect to predict drug and alcohol use disorders (Afifi et al., 2012), and that physical neglect was associated with increased odds of alcohol dependence (Fenton et al., 2013). In addition, a systematic review found emotional neglect to be associated with substance use disorders (Carr et al., 2013). However, only one of the above studies appropriately controlled for other maltreatment experiences (Fenton et al., 2013). After controlling for other maltreatment types and family dysfunction, analysis of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) found emotional neglect to only be predictive of depression, and not anxiety or substance use disorders (Taillieu et al., 2016). Thus, results of the current study add weight to the conclusion that neglect itself may not be significantly associated with substance use, but that failing to control for the experience of other ACEs may have erroneously inflated the importance of neglect for substance use in previous studies. In addition, the age of the sample and low level of problematic alcohol and drug use in the current sample may explain differences with previous research, as it is possible that neglect is associated with substance use disorders rather than consumption or harmful use. The current study helps to remedy the existing lack of data on neglect and substance use in young adult samples.
The current study supports accumulating evidence of distinct behavioural and neurobiological pathways to psychopathology depending on the type of maltreatment (threat/abuse vs deprivation/neglect). Children exposed to abuse or neglect show opposite patterns of activation during reward processing tasks (McLaughlin et al., 2019), and for neglected children, disruption in reward learning mediates the relationship between early deprivation and subsequent depression and social relationships (Sheridan et al., 2018). Abused children show alterations in fronto-amygdala regions involved in threat detection and aversive learning compared to neglected children who more consistently show changes in regions involved in executive function, cognitive control and social processing (McLaughlin et al., 2019). Deficits in cognition, in particular verbal ability, may be a neglect-specific pathway to psychopathology, as it was shown to link childhood deprivation, but not threat, to psychopathology (Miller et al., 2018). Of course, there are a multiplicity of factors other than maltreatment and a complex interplay between these factors that determine diagnostic outcomes in psychopathology. The current study provides an impetus to distinguish between types of deprivation, by demonstrating different mental health symptoms depending on the type of neglect. To do so will require a shift from a combined approach to neglect, which implicitly assumes that the types of deprivation affect development in the same manner, and thus tells us little about the mechanisms by which these exposures affect later outcomes.
For prevention and treatment of mental disorders, future research should replicate these findings with prospective samples and examine modifiable mechanisms linking emotional neglect to psychopathology. Emotional clarity has been shown to mediate the relationship between emotional neglect and depression among early adolescents (Jessar et al., 2017). Other evidence supports a role of narcissistic vulnerability and shame, and maladaptive schemas of vulnerability to harm (persistent sense of threats), self-sacrifice (prioritisation of others’ needs for fear of displeasing them) and shame, in mediating the relationship between emotional neglect and symptoms of depression and anxiety (Kealy et al., 2020; Wright et al., 2009). These mechanisms may provide targets to prevent and treat mental health problems among those exposed to emotional neglect, yet more longitudinal research, including intervention trials, is needed to examine efficacy of these as intervention targets.
The current study is not without limitations. The relatively small sample recruited through social media should not be considered representative of the target population. Future research should replicate this work in a more representative sample and in clinical samples. Second, the depression, anxiety and stress scales refer to symptoms over the past week; therefore, it is unclear how temporally stable these symptoms are for our sample. In addition, all data were self-reported, which is subject to desirability bias, although participants were assured their responses were confidential, and research shows self-report of maltreatment is more important for psychopathology than objective reports (e.g. child protective service reports) (Danese and Widom, 2020). There are also limitations to online surveys, as it is difficult to determine whether participants are attending. However, research shows that young people reliably answer online surveys and responses are valid (Ramo et al., 2011). In addition, the survey length was kept brief (15–30 minutes) to reduce likelihood of participant fatigue. Finally, maltreatment data were retrospective, which can be subject to problems with recall, and the data were cross-sectional. This limits our ability to rule out reverse causality, that is, that young adults with depressive symptoms may recall their childhood experiences in a negative light. However, there is good evidence that maltreatment is prospectively associated with mental health problems (Cohen et al., 2017; Spatz Widom et al., 2007), and improved memory recall is expected given the young age of participants and thus recency of childhood events. Nevertheless, prospective studies of Australian children exposed to maltreatment are needed to establish causality. In addition, family studies would provide an important examination of attachment patterns alongside maltreatment and the mental health of young Australians.
The current study demonstrates that emotional neglect is associated with depression, anxiety and stress in a sample of young adult Australians. It emphasises that emotional neglect is distinct from physical neglect, and that for mental health, these exposures must be considered separately. Future research should use prospective data to examine pathways from emotional neglect to mental health outcomes to identify targets for prevention and treatment of mental disorders.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Australian Government Research Training Programme scholarship to L.R.G.