
Abstract
Objective:
Alcohol use disorder and social anxiety disorder are interconnected disorders that commonly co-occur. We report the first trial to assess whether integrated treatment for social anxiety and alcohol use disorder comorbidity improves outcomes relative to standard alcohol-focussed treatment.
Method:
Participants were recruited to a randomised controlled trial, and randomly allocated to one of two treatments, Integrated (n = 61) or Control (alcohol-focussed; n = 56). Assessment and treatment session were conducted at two sites in Sydney, Australia. Inclusion criteria were as follows: (1) clinical diagnosis of social anxiety disorder and (2) Diagnosis or sub-clinical symptoms of alcohol use disorder. Diagnoses were determined according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.). All participants (n = 117) received 10 sessions of cognitive behavioural treatment and motivational enhancement. The Integrated treatment simultaneously targeted social anxiety disorder, alcohol use disorder and the connections between these disorders. The Control treatment focussed on alcohol use disorder only. Outcomes were assessed at 6-month follow-up, with interim assessments at post-treatment and 3 months. Primary outcomes were social anxiety disorder severity (composite Social Phobia Scale and Social Interaction Anxiety Scale), alcohol use disorder severity (standard drinks per day and Severity of Alcohol Dependence Questionnaire) and quality of life (Short-Form Health survey) was assessed to capture the combined impairment of social anxiety and alcohol use disorder comorbidity.
Results:
At 6-month follow-up, both conditions showed significant reductions in social anxiety and alcohol use disorder symptoms, and improved quality of life. There was no evidence of between-condition differences for alcohol outcomes, with mean consumption reduced by 5.0 (0.8) and 5.8 (1.0) drinks per day following Alcohol and Integrated treatments, respectively. Integrated treatment achieved greater improvements in social anxiety symptoms (mean difference = −14.9, 95% confidence interval = [−28.1, −1.6], d = 0.60) and quality of life (mean difference = 7.6, 95% confidence interval = [1.2, 14.0], d = 0.80) relative to alcohol-focused treatment.
Conclusion:
These results suggest that integrated social anxiety and alcohol use disorder treatment enhances quality of life and social anxiety disorder symptom improvement, but not alcohol outcomes, compared to treatment focussed on alcohol use disorder alone.
Keywords
Introduction
Comorbidity, when two or more disorders co-occur, represents one of the most significant challenges to effective treatment provision and an urgent global priority for health research (Teesson et al., 2009; The Lancet, 2018). A common pattern of comorbidity identified in epidemiological studies is the co-occurrence of ‘internalising’ (i.e. depression and anxiety) disorders with problematic substance use, and substance use disorders (Kushner et al., 2008; Stewart et al., 2016). Social anxiety disorder (SAD) and alcohol use disorder (AUD) are two prevalent disorders that commonly co-occur leading to greater symptom severity, more functional impairment and higher service utilisation than either disorder alone (Schneier et al., 2010). Increasingly, the co-occurrence of anxiety and alcohol use disorders is being conceptualised as a clinically important relationship involving bidirectional connections between disorders (Anker and Kushner, 2019; Smith and Randall, 2012; Stewart et al., 2016). Alcohol is often available in social settings and social anxiety is associated with use of alcohol to self-medicate or cope with anxiety in social contexts (Cooper et al., 2014; Morris et al., 2005). Over time, use of alcohol to self-medicate can lead to progressively greater alcohol intake, which can in turn increase psychosocial problems, functional impairment and heighten stress and anxiety (Anker and Kushner, 2019; Koob and Le Moal, 2005). Left untreated, social anxiety and alcohol use can become engaged in a mutually reinforcing cycle that interferes with recovery from either condition (Baillie et al., 2010; Kushner et al., 2013; Smith and Randall, 2012; Stewart et al., 2016), and there is evidence that SAD is a strong predictor of return to drinking following treatment (Kushner et al., 2005).
A large body of evidence supports the effectiveness of cognitive behavioural therapy (CBT) for treating SAD (Olatunji et al., 2010). CBT is also a widespread treatment for AUD, yielding moderate effects compared to no/minimal treatment, although a recent systematic review concluded it was no more effective than other established AUD therapies, such as motivational interviewing (Magill et al., 2019). Effective approaches for managing SAD or AUD cannot be assumed to generalise to individuals with comorbid anxiety and AUDs, who are typically excluded from treatment trials (Smith and Randall, 2012). Among studies investigating the impact of comorbidity on treatment outcomes, some found the effectiveness of standard treatment to be unaffected (Marquenie et al., 2006; Schade et al., 2007); however, others showed that anxiety-AUD comorbidity reduced the effectiveness of standard treatments. Higher pre-treatment alcohol use was found to predict poorer recovery from social interaction anxiety following anxiety-focused psychotherapy (McEvoy and Shand, 2008) and concurrent SAD was associated with less alcohol use reduction and greater risk of relapse following standard treatment for AUD (Farris et al., 2012; Kushner et al., 2005; Schellekens et al., 2015).
Two previous trials have evaluated the potential advantages of concurrently addressing SAD and AUD in comorbid samples. Both of these trials involved separate, unintegrated delivery of manualised treatment for each disorder (Randall et al., 2001; Schade et al., 2005). One found that the benefits of intensive, dual-focussed treatment were limited to anxiety symptom improvement, while the other found equivalent anxiety outcomes but poorer alcohol outcomes compared to the AUD-focussed treatment. In both cases, the study sample was drawn from a severely dependent population, and it may be that dual-focussed treatment is more effective at lower levels of AUD severity (Randall et al., 2001). Furthermore, delivery of two parallel, unintegrated treatments may increase cognitive load, and provides no explicit guidance for managing the interconnections between SAD and AUD. While no trial to date has evaluated integrated treatment for SAD and AUD specifically, two studies have combined AUD treatment with transdiagnostic anxiety treatment in samples with comorbid generalised panic, social or generalised anxiety disorder (Kushner et al., 2013; Morley et al., 2016). These studies found that integrated treatment improved alcohol but not anxiety outcomes compared to routine treatment for AUD (Morley et al., 2016) or anxiety (Kushner et al., 2013). The latter authors noted that despite receiving integrated treatment, trial participants experienced worse treatment outcomes than would be expected for AUD patients without co-occurring anxiety disorders, highlighting the need for additional research to identify more effective approaches for comorbid presentations (Kushner et al., 2013).
We report the first randomised controlled trial to evaluate integrated treatment for co-occurring SAD and AUD. The 10-session treatment (Stapinski et al., 2015) integrates effective CBT and motivational enhancement protocols for treatment of SAD (Rapee et al., 2009) and AUD (Miller et al., 1992; Monti et al., 2002) to target SAD, AUD and the interconnections between these disorders. To facilitate integration of the therapeutic techniques and rationale, we selected a CBT model given it is supported for treatment of both SAD and AUD (Magill et al., 2019; Olatunji et al., 2010), presented within a motivational enhancement framework and therapeutic style in view of the large body of evidence supporting motivational interviewing in the treatment of AUD (Frost et al., 2018; Lundahl et al., 2013). Ten sessions of AUD-focused treatment (CBT and motivational enhancement) were selected as a control given it has demonstrated equivalent or better outcomes compared to parallel SAD-AUD treatment in trials to date (Randall et al., 2001; Schade et al., 2005). We hypothesised that both treatments would reduce SAD and AUD symptoms and functional impairment, with superior outcomes in the Integrated condition. In contrast to previous trials, we recruited participants with alcohol use problems across a continuum of severity, enabling us to test the secondary hypothesis that AUD severity would moderate between-treatment differences, with integrated treatment most beneficial at lower levels of alcohol dependence.
Methods
Study design
The study was a randomised controlled trial comparing integrated CBT and motivational enhancement for SAD and AUD, to CBT targeting AUD only. Trial procedures, pre-specified outcomes and sample size calculations are detailed in the study protocol (Baillie et al., 2013). The target sample size (n = 200) was conservatively designed to have 80% power to detect a moderate effect size of 0.5 between conditions, assuming 20% attrition. Subsequent power calculations applying methods (Spybrook et al., 2011) to take into account the analytic approach (multi-level analysis with a nested, repeated measures design) suggested that our original power calculation was overly conservative and indicated a target sample size of n = 129 (assuming 30% attrition). All study procedures were approved by the Ethics Review Committees at Macquarie University (HE28MAR2008-R05758) and the Sydney South West Area Health Services (HREC/09/RPAH/553). All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The trial was prospectively registered prior to participant recruitment in the Australian and New Zealand Clinical Trials Registry (ACTRN12608000228381). The funding source had no role in the design or execution of this study, nor its analyses, interpretation or decision to submit results.
Participants and recruitment
Participants were recruited through a variety of health services and public media. Eligible participants were 18 years or older, who met diagnostic criteria for SAD (formerly social phobia) as assessed by the Anxiety Disorders Interview Schedule for The Diagnostic and Statistical Manual of Mental Disorders (4th ed., DSM-IV) (ADIS-IV) (Brown et al., 1994), and consumed alcohol at hazardous or harmful levels, indicated by an Alcohol Use Disorders Identification Test (AUDIT) score >8 (Babor et al., 2001). This alcohol use entry criteria facilitated recruitment of participants with alcohol use problems along the continuum from hazardous use through to severe alcohol dependence, in order to test our secondary hypothesis that dependence level would moderate between-treatment differences. Exclusion criteria were (1) inability to provide locator information or participate in treatment; (2) need for detoxification (⩾20 on the revised clinical institute withdrawal assessment for alcohol scale [Sullivan et al., 1989]; participants were eligible for the study after completion of detoxification) (3) active psychosis or history of schizophrenia; (4) current active suicidal intent assessed by the Suicidal Behaviours Questionnaire–Revised (Osman et al., 2001); and (5) current injecting drug use or substance use dependence (other than alcohol and tobacco). Individuals meeting criteria for other comorbid disorders were eligible, provided SAD or AUD was considered the primary diagnosis.
Randomisation and masking
After baseline assessment, participants were individually randomised on a 1:1 basis to (1) Integrated CBT for SAD and AUD or (2) CBT targeting AUD only. Randomisation was stratified for antidepressant use (stabilised prior to study entry). The randomisation sequence was computer-generated by an independent research assistant, who prepared sequentially numbered, opaque, sealed envelopes for implementation.
Assessments
Self-report assessments used well-validated measures administered at baseline, post-treatment (within 1 month of completion) and at 3- and 6-month follow-up. SAD, AUD and other comorbid diagnoses were determined by structured clinical assessments using the ADIS-IV (Brown et al., 1994) administered at baseline and 3 months by trained graduate students and psychologists. Diagnosticians were blind to participants’ treatment allocation. The primary outcome for SAD was baseline to 6-month follow-up symptom change assessed by the composite Social Phobia Scale (SPS) and Social Interaction Anxiety Scale (SIAS) (composite total scores ranged from 0 to 160; Mattick and Clarke, 1998). Primary outcomes for AUD were change from baseline to 6-month follow-up on the number of Australian standard drinks (10 g of alcohol) per drinking day assessed using the Timeline Follow-Back method (Sobell et al., 1988) and scores on the Severity of Alcohol Dependence Questionnaire (SADQ; range 0–100) (Stockwell et al., 1994), a well-validated measure of dependence spanning physical and affective withdrawal symptoms, craving, consumption and impaired control. Given the focus of the trial on treatment of comorbidity, a fourth primary outcome was included to capture the combined impairment of SAD-AUD comorbidity, assessed by overall quality of life on the mental health subscale of the Short-Form Health survey (SF12) (Ware et al., 1996). Secondary outcomes were days out of role assessed by the Short Disability Assessment Schedule (Von Korff et al., 2008); depression symptoms assessed by the Depression Anxiety Stress Scales (DASS) (Lovibond and Lovibond, 1993) and clinician-rated SAD and AUD severity on the ADIS-IV (Brown et al., 1994). Inter-rater reliability and diagnostician blinding were confirmed (see Supplementary Material). High inter-rater reliability was observed for the presence of SAD and AUD (100%), and disorder severity ratings (SAD: intraclass correlation coefficient [ICC] = 0.94; AUD: ICC = 0.90). To corroborate assessment of alcohol use, biochemical markers serum aspartate aminotransferase (AST) and gamma-glutamyltransferase (GGT) were assessed at baseline.
Procedure
The CONSORT flow diagram is shown in Figure 1. All assessment and treatment session were delivered at one of two sites in Sydney, Australia: the Emotional Health Clinic, Macquarie University, and Drug Health Services at Royal Prince Alfred (RPAH) Hospital. Potential participants were screened via telephone, then invited to a structured interview (ADIS-IV; Brown et al., 1994) to confirm eligibility and diagnostic status. Study procedures (Baillie et al., 2013) were explained to eligible individuals and written consent obtained from all participants. After baseline assessment, all participants received an initial motivational enhancement session, followed by a 4-week stabilisation period, during which they focussed on reducing or abstaining from alcohol. To assist with initial alcohol reduction, they were also referred for medical review (including full blood count and liver function) and to assess suitability for optional alcohol pharmacotherapy (naltrexone or acamprosate). Two check-in calls were conducted to provide encouragement over the stabilisation period. At the end of 4 weeks, self-reported SAD symptoms were re-assessed to differentiate these from transient alcohol-induced anxiety. Eligible participants were individually randomised to receive 90-minute sessions of Integrated or Alcohol-focussed CBT. The two treatments were delivered individually by the same pool of clinical psychologists, who ranged from recent graduate to experienced clinician and were supervised by experienced clinicians (A.J.B. or C.S.). In view of the complexity and severity of comorbid presentations, supplementary safety net sessions could be used at the therapist’s discretion to manage crises or deterioration in functioning. Participants were encouraged to make up missed sessions but were given a maximum of 5 months to complete treatment. Post-treatment and follow-up assessment dates were calculated from the end of all treatment sessions, or the equivalent timepoint for participants who discontinued treatment. Participants were reimbursed AUD$25 for completing the 3- and 6-month follow-up.
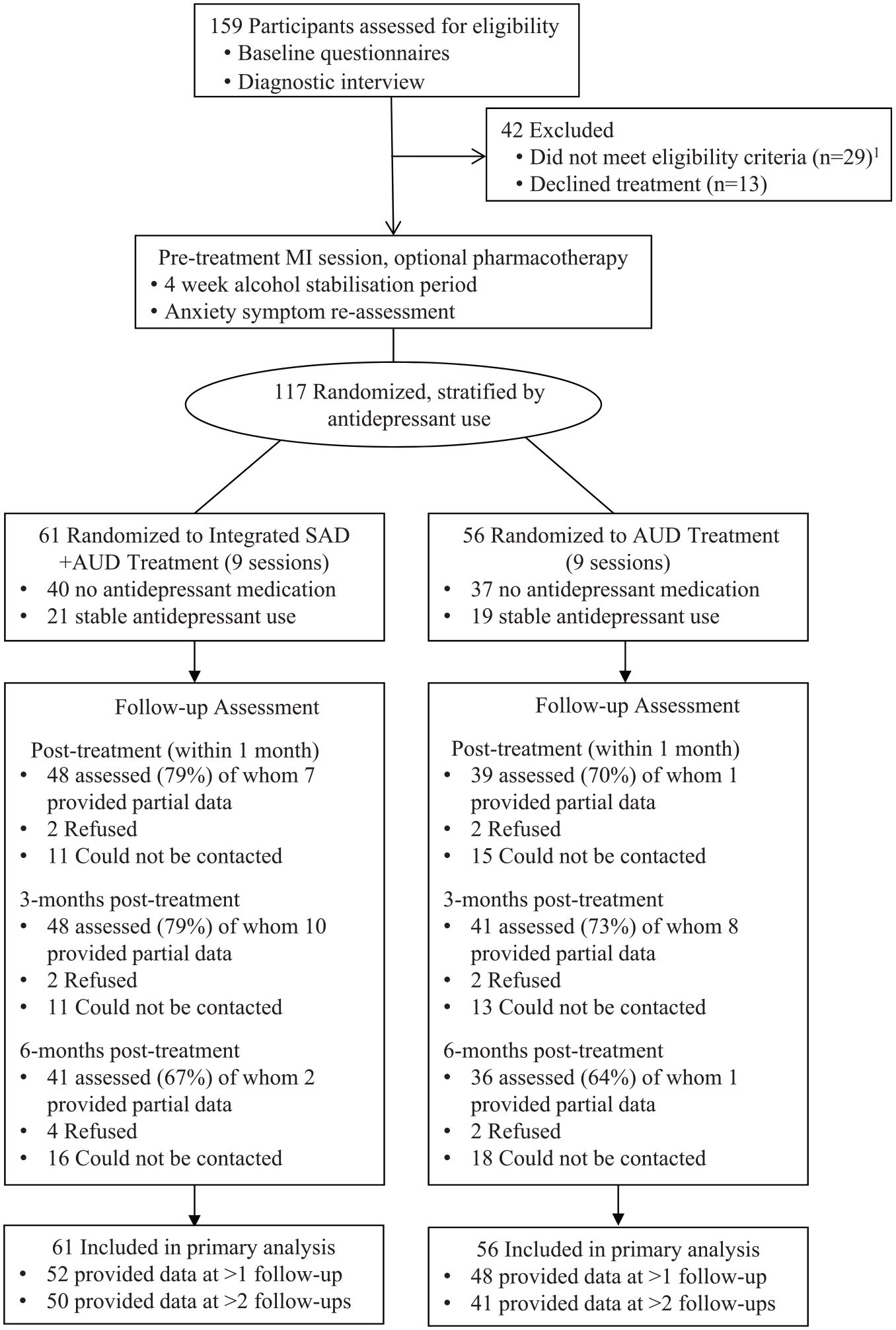
CONSORT diagram showing flow of participants through the trial.
Interventions
Detailed therapist manuals, session checklists and client workbooks were developed for both treatments to facilitate administration by non-specialist psychologists and are available on request. All participants received a preparatory alcohol-focussed motivational interviewing (MI) session (based on Motivation Enhancement Therapy [Miller et al., 1992]), followed by nine weekly CBT sessions. Each session integrated CBT skills within an over-arching motivational interviewing framework, provided opportunities for graded mastery and focussed on small successes to maintain motivation. The Integrated treatment was informed by our review of SAD-AUD comorbidity (Baillie et al., 2010; Stapinski et al., 2015) and synthesised established CBT approaches for SAD (Rapee et al., 2009) and AUD (Monti et al., 2002), to target both disorders and the interconnectedness between these disorders. The core treatment components, theoretical background and clinical application are described in full elsewhere (Stapinski et al., 2015). The Alcohol-focused treatment was based on widely used CBT and motivation enhancement interventions for AUD (Miller et al., 1992; Monti et al., 2002). When anxiety-provoking contexts were identified as potential trigger situations for drinking, coping strategies were explored but there was no focus on treating anxiety. Treatment fidelity and competence assessment indicated high adherence to allocated treatment protocols (see Supplementary Material).
Statistical analysis
All analyses were conducted using Stata v.13.1. Normality assumptions were examined, and analyses with transformed data reported where these showed substantive difference from analyses using raw data. Primary analyses involved multi-level mixed effects analysis, a rigorous method for modelling change over time (Gueorguieva and Krystal, 2004; West et al., 2014), and applied an intention-to-treat approach, with all 117 randomised participants included in their allocated condition. Models used baseline measurements as the reference point to estimate participant-specific starting points and change over time. Treatment was dummy-coded (Alcohol = 0, Integrated = 1), and condition by time interactions were examined to assess between-condition differences in treatment response over time. Missing data were accommodated using maximum likelihood estimation. All models included a random intercept and were adjusted for gender due to the differential distribution between conditions. The most appropriate model and covariance structure were determined using model fit statistics (see Supplementary Material). Within and between-condition effect sizes (Cohen’s d) were calculated from the model estimated Condition and Condition × Time coefficients (Feingold, 2013). Sensitivity analyses examined whether between-condition differences in implementation of safety net sessions affected results, and analyses using multiply imputed data explored whether attrition influenced results (see Supplementary Material).
Results
Recruitment, retention and participant characteristics
A total of 295 adults contacted the study for initial screening, of these 220 were invited to a diagnostic interview. Figure 1 shows flow through the trial for the 159 people who attended a diagnostic assessment. The final sample size of 117 reflected the challenges of conducting research with complex comorbid presentations and a lower than expected recruitment rate. Full baseline data were available for 116 of the 117 randomised participants; 85% provided data for at least one assessment post baseline. Number of assessments completed did not differ by condition, t(115) = −0.45, p = 0.65. At baseline, all participants met criteria for SAD, with a mean composite social anxiety score for the total sample of 84.0 (standard deviation [SD] = 25.0). All but two participants (98%) also met criteria for AUD, and the sample reported drinking on average 17.7 days in the past month (SD = 8.8), 10.1 standard drinks per drinking day (SD = 5.7) and mean scores on the SADQ of 17.2 (SD = 10.2). Sample characteristics are shown in Table 1. Gender distribution was substantially different between randomly allocated conditions with more females in the Alcohol-focussed treatment condition (48%) than in the Integrated (26%) condition. There were no between-condition differences in baseline scores on any primary or secondary outcomes measures (see Table 2).
Baseline characteristics of the total sample and by treatment condition (integrated vs alcohol-focused).
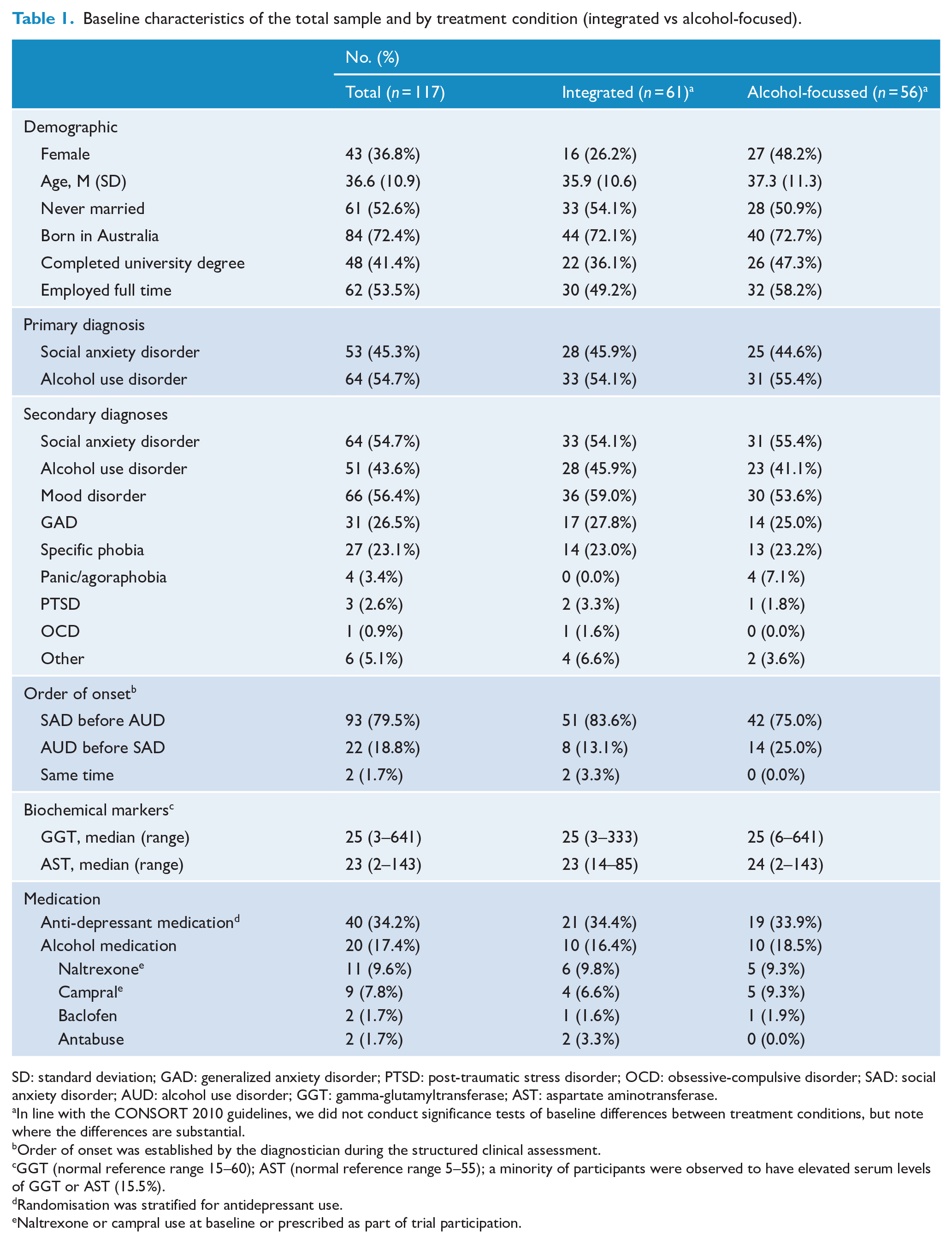
SD: standard deviation; GAD: generalized anxiety disorder; PTSD: post-traumatic stress disorder; OCD: obsessive-compulsive disorder; SAD: social anxiety disorder; AUD: alcohol use disorder; GGT: gamma-glutamyltransferase; AST: aspartate aminotransferase.
In line with the CONSORT 2010 guidelines, we did not conduct significance tests of baseline differences between treatment conditions, but note where the differences are substantial.
Order of onset was established by the diagnostician during the structured clinical assessment.
GGT (normal reference range 15–60); AST (normal reference range 5–55); a minority of participants were observed to have elevated serum levels of GGT or AST (15.5%).
Randomisation was stratified for antidepressant use.
Naltrexone or campral use at baseline or prescribed as part of trial participation.
Marginal means a for primary and secondary outcomes by treatment condition (integrated vs alcohol-focused).
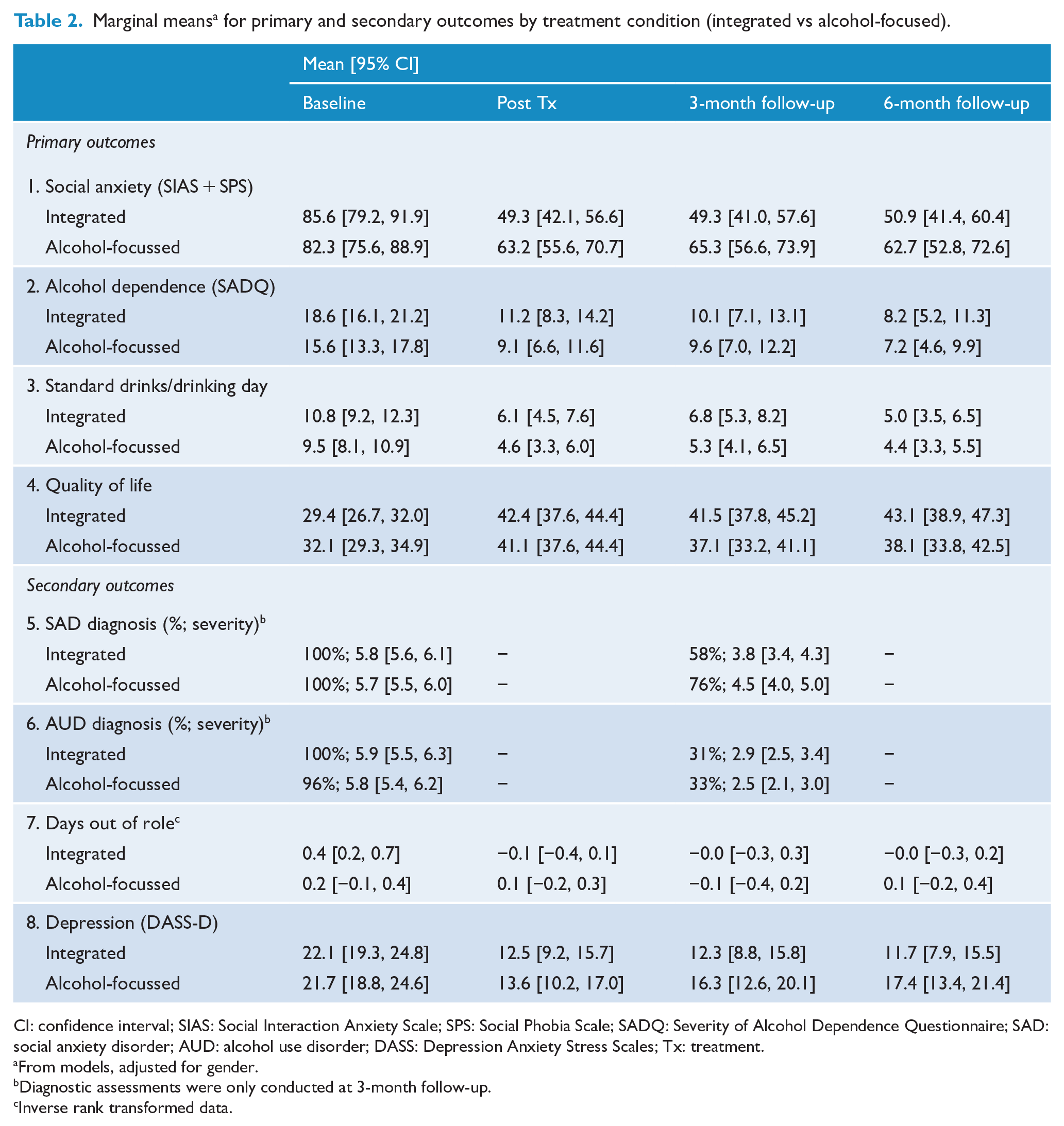
CI: confidence interval; SIAS: Social Interaction Anxiety Scale; SPS: Social Phobia Scale; SADQ: Severity of Alcohol Dependence Questionnaire; SAD: social anxiety disorder; AUD: alcohol use disorder; DASS: Depression Anxiety Stress Scales; Tx: treatment.
From models, adjusted for gender.
Diagnostic assessments were only conducted at 3-month follow-up.
Inverse rank transformed data.
Pre-treatment stabilisation period
Participants demonstrated moderate success reducing their alcohol intake during the 4-week stabilisation period, reducing on average 2.5 (95% confidence interval [CI] = [−3.6, −1.4]) points on the SADQ. There was a corresponding reduction of 6.4 points (95% CI = [−9.6, −3.2]) on the SAD symptom measure; however, participants continued to report SAD symptoms within the clinical range (M = 77.3, 95% CI = [72.5%, 82.1]; 74% within clinical range, compared to 80% at baseline [Peters, 2000]).
Treatment compliance
Treatment sessions were primarily delivered at the Emotional Health Clinic (76%), 17% of the sample attended treatment at RPA Drug Health Services, and 7% switched between sites (for convenience reasons) over the course of treatment. Treatment completion (>80% of sessions) was 70% for Integrated treatment and 64% for Alcohol-focussed treatment and did not differ between conditions, χ2(1) = 0.51, p = 0.47. Safety net sessions (beyond the standard 10) were required for more participants allocated to Integrated treatment (26%) than Alcohol treatment (11%), χ2(1) = 4.60, p = 0.03, thus a sensitivity analysis explored the impact on treatment outcomes.
Primary outcomes
Primary results are reported in Table 3, and marginal means in Table 2. All models co-varied gender; however, there was no evidence of an association with any primary or secondary outcome.
Mixed model repeated measures results: primary outcomes.
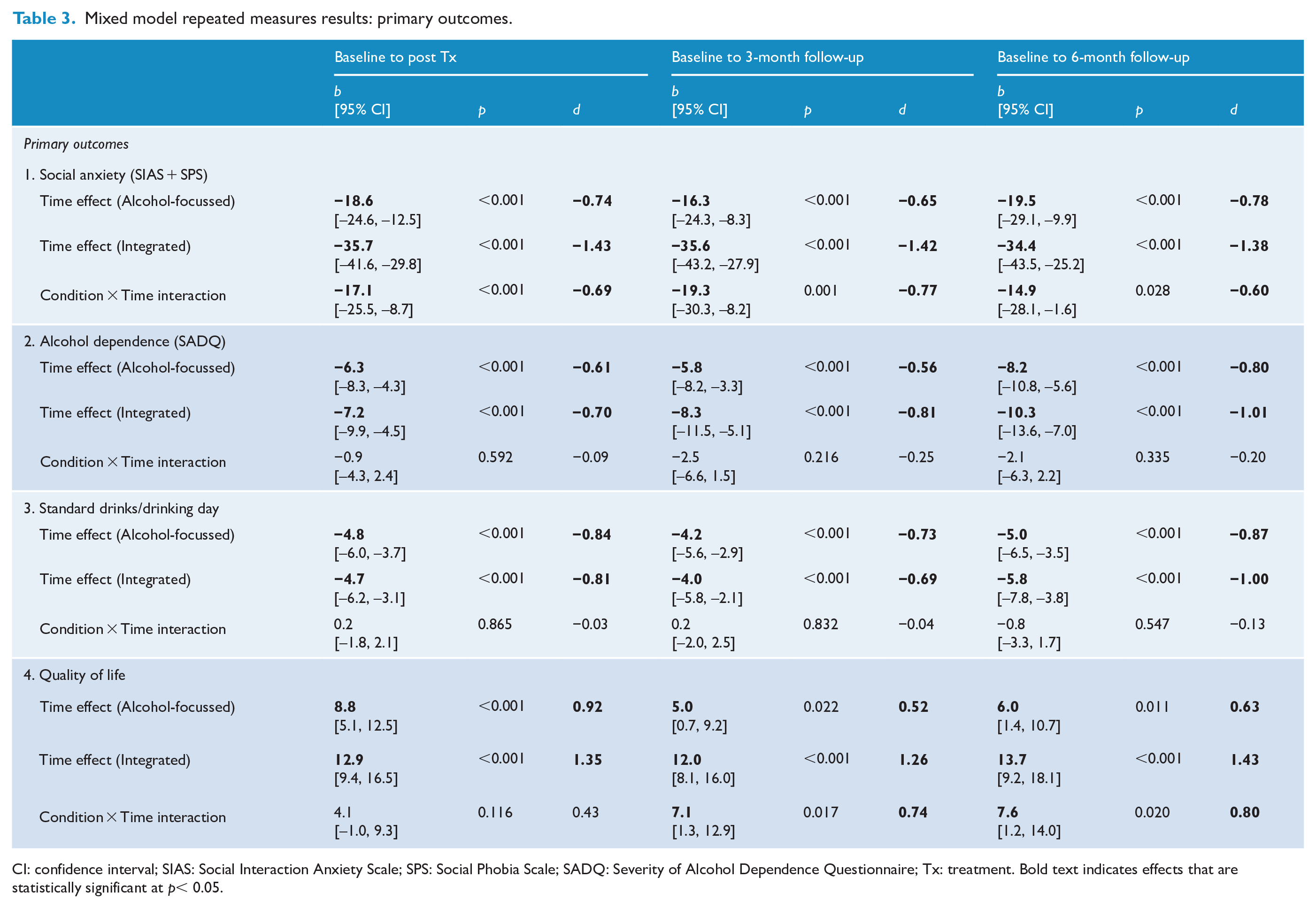
CI: confidence interval; SIAS: Social Interaction Anxiety Scale; SPS: Social Phobia Scale; SADQ: Severity of Alcohol Dependence Questionnaire; Tx: treatment. Bold text indicates effects that are statistically significant at p< 0.05.
Social anxiety disorder
In both conditions, SAD symptoms reduced from baseline to post-treatment, and these gains remained evident at 3- and 6-month follow-up (see Table 3). There was a condition by time interaction at all timepoints, with greater symptom reduction in the Integrated treatment from baseline to post-treatment (d = 0.69), 3-month (d = 0.77) and 6-month follow-up (d = 0.60).
Alcohol use disorder
Across conditions there was a sustained reduction in consumption and alcohol dependence symptoms, with largest reductions at 6-month follow-up. There was no evidence of a condition by time interaction at any timepoint, indicating both treatments were similarly effective for AUD.
Quality of life
Quality of life improved from baseline to post-treatment in both conditions, and these improvements were sustained at 3- and 6-month follow-up (see Table 3). A condition by time interaction was evident, with participants allocated to receive Integrated treatment reporting a greater increase in quality of life from baseline to 3 months (d = 0.74), and 6-month follow-up (d = 0.80).
Secondary outcomes
Secondary outcome results are reported in Table 4, and marginal means are shown in Table 2.
Mixed model repeated measures results: secondary outcomes.
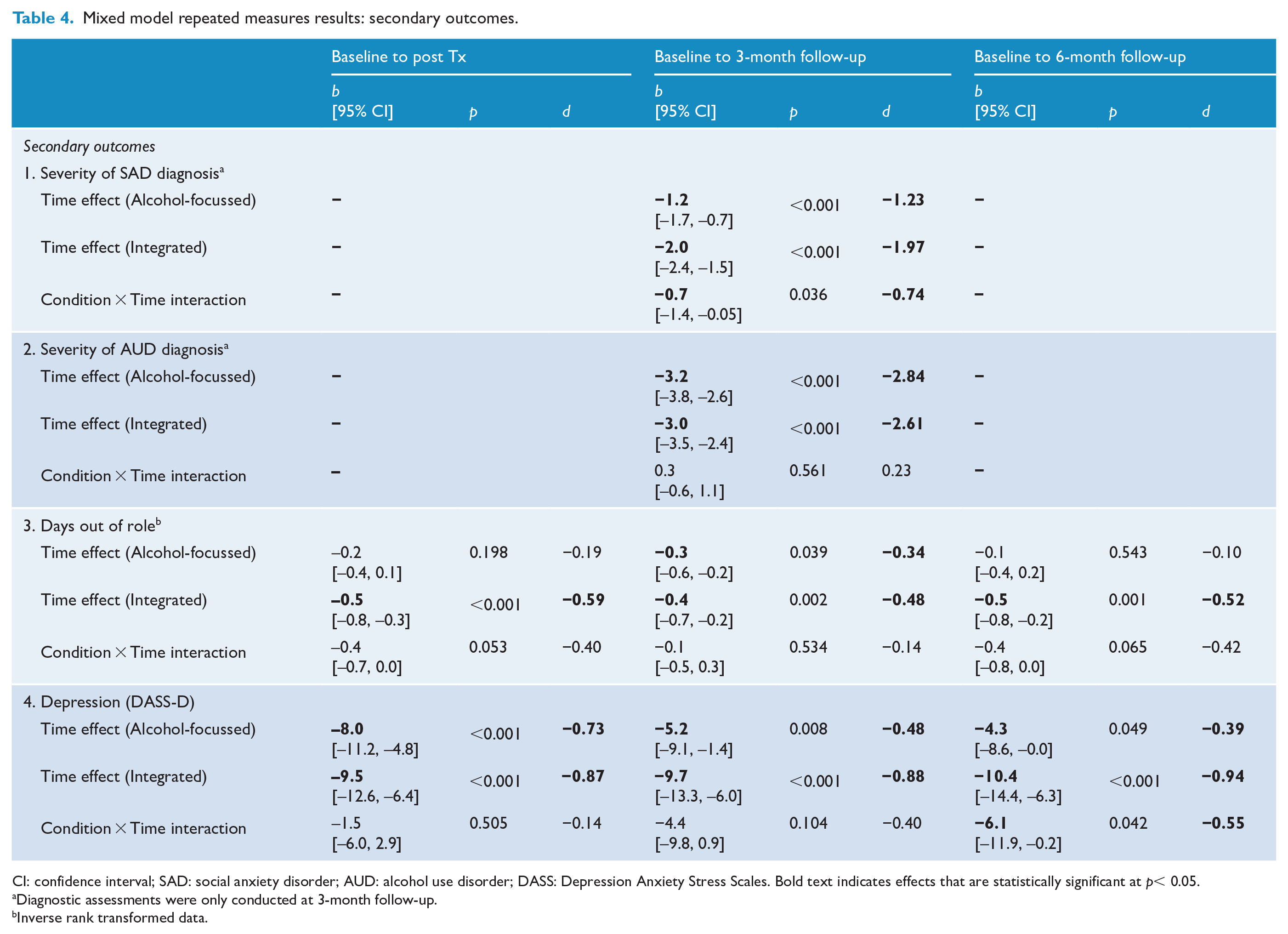
CI: confidence interval; SAD: social anxiety disorder; AUD: alcohol use disorder; DASS: Depression Anxiety Stress Scales. Bold text indicates effects that are statistically significant at p< 0.05.
Diagnostic assessments were only conducted at 3-month follow-up.
Inverse rank transformed data.
Clinician-rated diagnostic severity
Clinician-rated SAD diagnostic severity reduced significantly from baseline to 3-month follow-up. A condition by time interaction was observed, indicating greater reduction for participants allocated to Integrated treatment (d = 0.74). Clinician-rated AUD diagnostic severity also reduced from baseline, but there was no evidence of a condition by time interaction, aligning with self-report results indicating the treatments were similarly effective for AUD.
Days out of role
There was a significant and sustained reduction in inverse rank transformed days out of role for the Integrated condition, and for the Alcohol condition, a significant reduction in days out of role at the 3-month follow-up only. There was no evidence of a condition by time interaction at any timepoint.
Depression
Sustained reductions in depression symptoms from baseline were observed in both conditions. A significant condition by time interaction at 6-month follow-up suggested some depression symptom rebound in the Alcohol condition, with greater maintenance of treatment gains in the Integrated condition (d = 0.55).
Severity of dependence as a moderator of treatment outcome
There was no evidence that baseline severity of dependence predicted differential response to treatment for any outcome (all p values > 0.22), with the exception of alcohol dependence. A condition by time by baseline dependence severity interaction effect was observed at 3-month follow-up only (mean difference −0.36, 95% CI = [−0.68, −0.05], p = 0.03). Contrary to our hypotheses, at this timepoint higher dependence severity was associated with better outcomes in the Integrated treatment relative to Alcohol-focussed treatment.
Sensitivity analyses
There was no evidence of differential attrition by treatment allocation. Attrition was associated with younger age, and higher drinks per day during treatment. Sensitivity analyses with imputed data and adjusting for delivery of safety net sessions confirmed our findings, with no substantive difference to conclusions derived from principal analyses (see Supplementary Tables S1–S4).
Discussion
Results of the study suggest that integrated treatment for comorbid SAD and AUD achieved superior gains for some outcomes compared to standard Alcohol-focussed treatment. Integrated treatment was associated with greater reduction in social anxiety symptoms, and this between-treatment difference was sustained at 6-month follow-up (mean difference −14.9, d = 0.60). Clinician-rated SAD severity showed a similar pattern. The Integrated treatment was also associated with greater improvements in quality of life compared to Alcohol-focussed treatment (d = 0.80). There was a delayed benefit for depression symptoms, with superior outcomes for Integrated compared to Alcohol-focussed treatment at 6-months follow-up (d = 0.55), supporting the stronger effects for Integrated treatment on overall quality of life.
We hypothesised that providing participants with strategies to manage SAD symptoms would facilitate greater reduction in alcohol consumption compared to Alcohol-focussed treatment; however, there was no evidence that Integrated treatment enhanced gains on any alcohol outcomes. Both treatments were associated with a significant and sustained reduction in drinking and AUD severity, with mean reductions of 5 and 5.8 standard drinks consumed per drinking day in the Alcohol-focused and Integrated conditions, respectively. The largely equivalent alcohol outcomes observed for the two treatments in this study may reflect their different strengths: while Integrated treatment addressed both disorders and the interconnections between them, the Alcohol treatment had a singular focus and dedicated comparatively greater time to alcohol reduction. It is noteworthy that participants in the Integrated treatment were encouraged to seek out previously avoided social interactions. A previous study reported worse alcohol outcomes for parallel SAD and AUD treatment, which they attributed in part to use of alcohol during exposure to social contexts as part of SAD treatment disorder (Randall et al., 2001). Therefore, it is encouraging that in our study, participants allocated to Integrated treatment reduced social avoidance without a corresponding increase in alcohol intake. Participants in the Integrated condition were more likely to require safety net sessions, which may reflect the additional challenges and affective intensity associated with facing previously avoided anxiety-provoking situations. Over the longer term, the capacity to more effectively manage anxiety symptoms may mitigate the increased risk of alcohol relapse that has been previously associated with SAD-AUD comorbidity (Kushner et al., 2005). On the other hand, it is possible that to prevent alcohol relapse, what is most critical is to decouple the link between anxiety symptoms and drinking behaviour, for example, by challenging inaccurate expectancies about the beneficial effects of alcohol. This view has been argued by Kushner et al. (2013), who found better alcohol outcomes following CBT targeting transdiagnostic anxiety and alcohol compared to AUD treatment plus relaxation training in a mixed anxiety disorders and AUD sample. In our study, both the Alcohol-focussed and Integrated treatments targeted alcohol expectancies, including expectancies regarding the social enhancement and tension reducing properties of alcohol. Thus, the similar alcohol outcomes observed across conditions may reflect effective decoupling of the anxiety-drinking connection for both treatments.
Our study found no evidence that more severely dependent individuals fared worse in the Integrated condition, in fact there was weak evidence at 3-month follow-up that higher AUD severity was associated with better alcohol outcomes in the Integrated relative to Alcohol-focussed treatment. This finding was unexpected, as we hypothesised that more severely dependent participants would benefit more from an undivided treatment focus on strategies to reduce alcohol consumption. Evidence of comparatively greater AUD symptom reduction following integrated treatment may suggest that at higher levels of alcohol dependence severity, there is even greater need to address the connection between SAD and AUD, perhaps because the two problems are more deeply intertwined, or because social anxiety symptoms present a greater impediment to change when alcohol dependence is high. These hypotheses will be explored in subsequent analyses of the mechanisms that mediate and moderate treatment change in this comorbid sample.
This study represents the first evaluation of an integrated treatment for SAD and AUD. Consistent with previous research (Schneier et al., 2010), 80% of the sample reported onset of SAD prior to AUD. Reflecting the severity and complexity of diagnostic comorbidity, most participants met criteria for an additional mood and/or anxiety disorder. Despite this complexity, both treatments were associated with significant improvements in AUD symptoms, with 67% and 69% of participants no longer meeting diagnostic criteria for AUD following Alcohol-focussed and Integrated treatment, respectively. In the Integrated condition, 42% of the sample were also SAD diagnosis free, a rate comparable to treatment focussed on social anxiety alone (Rapee et al., 2009). Given the lower than expected recruitment rate, replication of these findings in a larger trial is needed to confirm the benefits of integrated treatment. Nonetheless, our study provides preliminary evidence that an integrated SAD and AUD treatment can improve SAD, depression and quality of life outcomes compared to standard single-disorder treatment. Given the significant functional impairment that is associated with SAD, it is unsurprising that the greater social anxiety symptom improvements following Integrated treatment were associated with corresponding improvements in quality of life. People with SAD typically experience significant impairment spanning social, personal and occupational functioning, for example, they have difficulty dating and forming friendships, are more likely to be single and experience higher rates of unemployment and reduced work performance compared to people without SAD (Ruscio et al., 2008; Wittchen et al., 2000). The level of impairment is even greater when people have SAD in combination with other disorders (Ruscio et al., 2008). Given the level of impairment associated with SAD, integrated treatment offers clear advantages over alcohol-focussed treatment for people suffering both disorders by reducing the severity of social anxiety symptoms, improving quality of life and ultimately reducing depression, with the same number of treatment sessions. Unlike previous investigations of SAD and AUD treatment delivered in parallel (Randall et al., 2001), this study found no evidence that dual-focussed treatment delivered in an integrated format weakened the efficacy of AUD treatment. It will be useful for future research to explore whether integrated treatment may offer other advantages such as better alignment with clients’ perceptions of interconnection between disorders, and engaging clients who may minimise their AUD severity or are unmotivated to seek treatment purely for alcohol use problems.
These findings must be interpreted in the context of the study limitations. Most importantly, recruitment to the trial was lower than expected, reflecting the increased challenges of research with this complex comorbid population. Recruitment via secondary services proved impractical, which is consistent with the low rates of treatment-seeking for AUD, with a median delay to seek treatment of 18 years reported in Australia (Chapman et al., 2015). For people with SAD-AUD comorbidity, treatment-seeking may be further complicated by uncertainty about where to seek treatment, or past experiences of being ineligible for standard single disorder treatment services until their comorbid condition has resolved or stabilised (Kay-Lambkin et al., 2004). Due to the challenges recruiting participants from treatment services, the majority of participants were recruited from the community via advertisements and media coverage. Therefore, although the sample may be representative of the broader community, our study does not necessarily indicate a clear pathway for translation of integrated treatment to services operating within the dominant single-disorder model. Second, the study is limited by data attrition over the follow-up period; however, we are reassured by the results of sensitivity analyses in multiply imputed data, which suggested our conclusions were robust to the potential impact of response attrition. Third, we used the mental health subscale of SF12 quality of life scale in an attempt to capture the combined impairment associated with SAD-AUD; however, we acknowledge that a measure that specifically assesses the additive or multiplicative impact of comorbidity would be preferable. Fourth, the randomised conditions differed in gender distribution and proportion of participants requiring safety net sessions. To account for these differences, all analyses included sex as a covariate, and sensitivity analyses confirmed that treatment effects were not attributable to differences in implementation of safety net sessions. In addition, treatment was administered by clinical psychologists, which may not reflect the training level of staff in community-based services. To facilitate administration by non-specialist psychologists, detailed client workbooks, therapist manuals and implementation guides have been developed (Stapinski et al., 2015), and evaluation of treatment delivery in a naturalistic health care setting is an important next step. Finally, the exclusion of participants with comorbid substance use dependence limits the generalisability of the findings. Given the positive results, adaption of the Integrated treatment for other substances and for persons using multiple substances is an important future direction.
Conclusion
This study tested two treatments delivered to participants with comorbid SAD and AUD: 10 sessions of CBT and motivational enhancement focused on AUD only, compared to 10 sessions of integrated CBT and motivational enhancement targeting AUD, SAD and the connections between these disorders. Our results showed that both treatments were associated with reductions in social anxiety symptoms, alcohol consumption and severity of alcohol dependence. For busy clinicians, this indicates there are benefits of delivering alcohol-focussed CBT and motivational enhancement to patients with SAD-AUD comorbidity, and they can reasonably expect to see some improvement in both AUD and SAD symptoms. However, our study indicated there are advantages to an integrated SAD-AUD treatment approach, which achieved comparable alcohol outcomes and superior social anxiety, depression and quality of life outcomes compared to treatment focussed on AUD alone.
Supplemental Material
Stapinski_et_al_Supplementary_Material – Supplemental material for Randomised controlled trial of integrated cognitive behavioural treatment and motivational enhancement for comorbid social anxiety and alcohol use disorders
Supplemental material, Stapinski_et_al_Supplementary_Material for Randomised controlled trial of integrated cognitive behavioural treatment and motivational enhancement for comorbid social anxiety and alcohol use disorders by Lexine A Stapinski, Claudia Sannibale, Mirjana Subotic, Ronald M Rapee, Maree Teesson, Paul S Haber and Andrew J Baillie in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of Erin Kelly, Sonia Haggman, Chris Winkler and Zayra Millan who delivered treatment sessions; Kristen Tulloch, Jocelyn Elliot, Bianca Lee, Travis Wearne, Mia Romano, Sylvia Derdeyan and Carla Ross for research assistance; Les Davidson for assistance with co-ordination at the Royal Prince Alfred Hospital Drug Health Services; and Lauren McLellan for assistance with reliability coding. We are extremely grateful to all the participants who took part in this study.
Authors’ Contribution
A.J.B., C.S., M.T., R.M.R. and P.S.H. designed the study and obtained funding support. A.J.B. was chief investigator of the trial. L.A.S. was project manager, conducted the data analysis with assistance from A.J.B. and prepared the first draft of the manuscript. M.S. provided research assistance. All authors contributed to interpretation of the results, reviewed and edited the final manuscript.
Clinical Trial Registration
This work was prospectively registered on 2 May 2008 in the Australian New Zealand Clinical Trials Registry ACTRN12608000228381.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: The authors developed the integrated treatment programme for comorbid social anxiety and alcohol use disorders. The programme is not distributed for profit.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Health and Medical Research Council (grant number: APP1004744, APP1041129).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.