
Abstract
Alcohol-use disorders were among the most common mental disorders identified in the two largest USA population based epidemiological studies assessing drug- and alcohol-use disorders: the US Epidemiological Catchment Area (ECA [1]) study and the National Comorbidity Survey (NCS [2]). The ECA study estimated the lifetime prevalence of DSM-III alcohol-use disorders at just under 14%%. There was a higher prevalence of alcohol-use disorders in the National Comorbidity Survey, with 24%% meeting lifetime criteria for alcohol dependence and 10%% meeting criteria for an alcohol-use disorder in the past 12 months.
Alcohol-use disorders in the ECA were strongly related to gender with 24%% of men and 5%% of women having had an alcohol-use disorder at some time in their lives, and 12%% of men and 2%% of women had such a disorder in the previous year. The same pattern was observed in the NCS [3].
One in three in the ECA sample (36%%) had used an illicit drug at sometime in their lives, most often cannabis. Drug-use disorders were diagnosed in 6%% of the population. Cannabis-use disorders affected 4%%, stimulant disorders 2%%, sedative disorders 1%% and opioid disorders 0.7%%. Men had higher rates of drug-use disorders than women (8%% vs 5%%). The highest rate was in the 18–29 years age group (14%% overall, 16%% among men and 11%% among women).
The lifetime prevalences of drug-use disorders in the NCS were somewhat higher than in the ECA: any drug-use disorder, 8%%; cannabis, 4%%; cocaine, 3%%; other psychostimulants, 2%%; anxiolytics, 1%%; and heroin, 0.4%%. The prevalence of drug-use disorders in the past year was 3.6%%. As in the ECA, men were more likely than women to be dependent on drugs (5%% male vs 2%% females in the past year).
Until recently, Australia was reliant on data from these USA studies and other smaller studies of specific areas (e.g. [4]). In 1997, the Australian Bureau of Statistics was funded by the Commonwealth Mental Health Branch to undertake the National Survey of Mental Health and Wellbeing (NSMHWB [5–7]), a survey of the mental health of a representative sample of the Australian adult population. The survey provides the first national Australian data on the prevalence and patterns of alcohol- and other drug-use disorders among Australian men and women in the past year. In this paper we summarise the main findings on the prevalence and correlates of disorders related to the use of alcohol and illicit drugs. The emphasis is on the broad findings and their implications for the treatment of drug- and alcohol-use disorders.
Method
Henderson et al. [6] have described the survey methods and presented the basic findings of the survey; here, we briefly review the assessment of alcohol- and other drug-use disorders. More detailed information on the survey method and the prevalence and correlates of ICD-10 alcohol- and drug-use disorders is provided elsewhere [8],[9], as are the implications of mental health survey data for drug and alcohol and mental health services [10],[11]. The survey contains limited information on tobacco use and these results are reported elsewhere [8].
The NSMHWB sample was based on a stratified, multi-stage probability sample of persons aged 18 years and older in the Australian population. The overall response rate was 78%% and there were 10 641 participants. Alcohol- and drug-use disorders [12] were assessed by a modified version of the Composite International Diagnostic Interview (CIDI [13]). The CIDI assessments of alcohol- and other drug-use disorders have excellent inter-rater reliability and test–retest reliability [14]. There are fewer studies of validity, although results have shown good levels of agreement between the CIDI and clinicians [15] and the CIDI and Present State Examination [16].
Questions from the NSMHWB concerning the use of alcoholic beverages asked about age of onset, frequency, recency and quantity of drinking. Alcohol-use disorders (harmful use and dependence) were assessed in those individuals who had consumed more than 12 standard drinks in the last 12 months. A standard drink was defined as 10 g of alcohol.
With regard to drugs, respondents were asked separate questions about their use of illicit drugs and ‘extramedical use’ of prescribed drugs. Specifically, whether drugs and medicines had been used ‘in larger amounts than was prescribed or for a longer period than was prescribed’ or used ‘more than five times when they were not prescribed for you, to get high, to relax, or to make you feel better, more active, or alert’. Respondents were assessed for drug-use disorders (ICD-10 harmful use or dependence) if they had used drugs more than five times in the past 12 months.
Additional questions covered age of onset of use, frequency and recency of use. The drug groups covered were selected to reflect the most widely used drugs among Australian adults, as indicated in the Australian National Drug Strategy Household surveys [17]. They included: cannabis (marijuana and hashish); amphetamines, ecstasy and other stimulants that can be obtained by medical prescription; tranquillisers and other sedatives that can be obtained by medical prescription; opioids such as heroin and opium and other opioids that can be obtained on medical prescription.
The ICD-10 criteria for disorders (harmful use and dependence) are reported in this paper. ICD-10 harmful use criteria require a pattern of substance use that causes damage to health. The damage may be physical or mental. ICD-10 dependence criteria require the presence of three or more of the following: a strong desire to take the substance; impaired control over the use; a withdrawal syndrome on ceasing or reducing use; tolerance; a disproportionate amount of the user's time is spent obtaining, using and recovering from use; and continued use despite associated problems. The problems should have been experienced at some time during the previous year for at least 1 month.
Results
Alcohol-use disorders
The majority of Australian adults (83%% of males and 63%% of females) reported that they had consumed at least 12 drinks of alcohol in the preceding year. One in 15 (6.5%%) had had an alcohol-use disorder in the past 12 months (3.0%% with harmful use and 3.5%% with dependence). More males than females had an alcohol-use disorder within the past 12 months (9.4%% vs 3.7%%, respectively). Figure 1 shows that the prevalence of alcohol-use disorders decreases steadily with increasing age: it was highest among 18–34-year-olds (10.6%%) and lowest among those over 55 years (4.4%%).
Prevalence (%%) of alcohol-use disorders by age and gender: ▪, male; □, female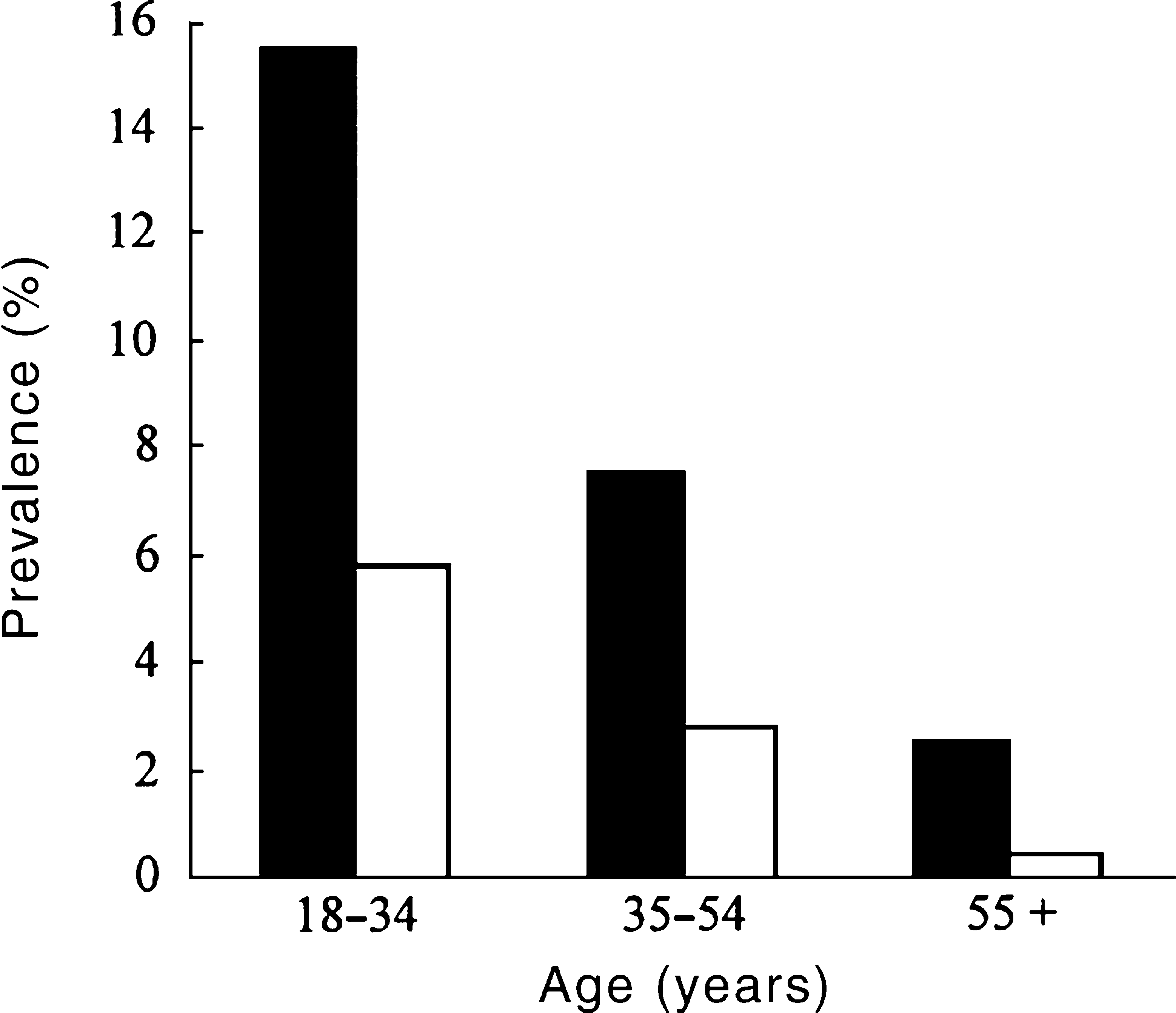
Alcohol-use disorders were more prevalent among the unemployed than the employed (12.7%% vs 7.8%%), those who had never married (13.0%%) compared with those who were separated or divorced (9.4%%) or those who were married (4.5%%), and those born in Australia (7.1%%) and other English-speaking countries (6.2%%) compared with those born in non-English-speaking countries (3.3%%). There were no substantial differences in the prevalence of alcohol-use disorders between those living in capital cities (6.5%%) and those living outside the capital cities (6.4%%).
Proportions of those with ICD-10 dependence upon alcohol and other drugs reporting symptoms of dependence
Comorbidity
There was considerable comorbidity between alcohol-use disorders and other mental disorders (Fig. 2). Just under half of females with an alcohol-use disorder (48%%) met criteria for an anxiety, affective or drug-use disorder. In comparison, among females who did not have an alcohol-use disorder, 15%% had at least one mental disorder.
Comorbidity of mental disorders among males and females: □, anxiety; ▪, affective; ▪, drug; ▪, any two comorbid; ▪, all three comorbid; ▪, no other disorder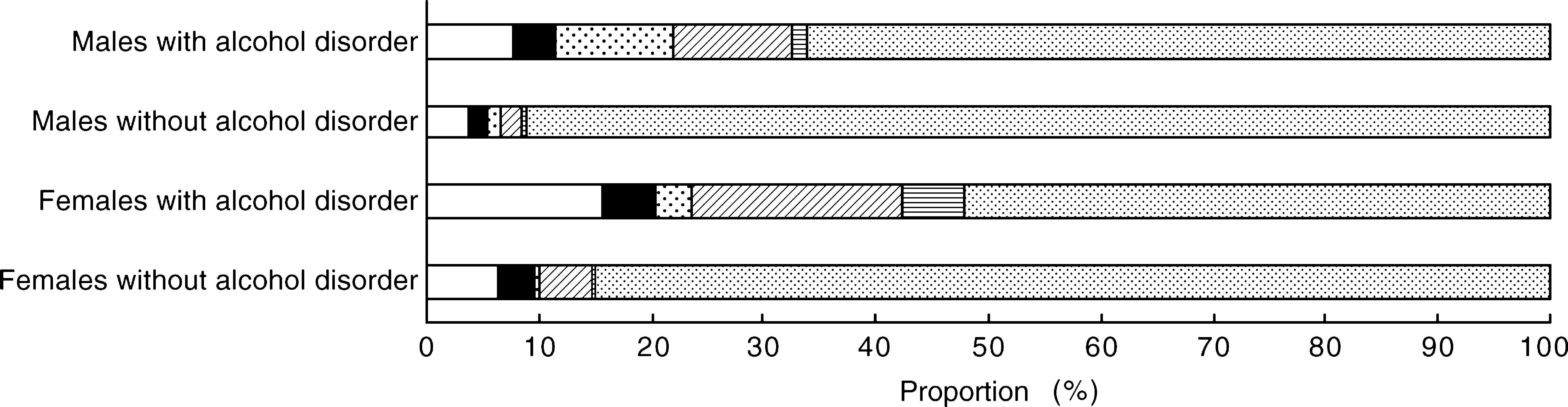
A third (34%%) of males with an alcohol-use disorder met criteria for another mental disorder. Of men who did not have an alcohol-use disorder, 9%% had at least one mental disorder. Women with an alcohol-use disorder were somewhat more likely than men to have a comorbid mental disorder, as shown in the patterns of comorbidity in Figure 2. Over a third (39%%) of individuals with alcohol-use disorders had a comorbid physical disorder.
Treatment seeking
Twenty-eight per cent of those with an alcohol-use disorder sought assistance from a health professional within the last year. Rates of help seeking among those with an alcohol-use disorder were higher among females (39%%) than males (23%%). General practitioners were the most commonly consulted professionals (29%% of women and 18%% of men). Smaller proportions sought help from psychiatrists (3%% of males and 6%% of females) or psychologists (4%% of males and 8%% of females). Other mental health professionals were consulted by 7%% of men and 11%% of women with an alcohol-use disorder. Psychologists were 19 times more likely to see individuals with comorbid anxiety and affective disorders than individuals with alcohol-use disorders alone. Psychiatrists were 7 times more likely and general practitioners 4.7 times more likely.
Other drug-use disorders
One in eight males (12.5%%) and one in 14 females (6.9%%) reported that they had used at least one of the drug classes (cannabis, stimulants, sedatives and opioids) more than five times in the past year. Cannabis use was the most common, reported by 10.3%% of males and 4.3%% of females. Use of stimulants, sedatives and opioids were reported by 1.3–1.9%% of males, and 0.6–2.3%% of females.
Drug-use disorders affected about one in 45 persons in the past 12 months. An estimated 2.2%% of the Australian adult population had a drug-use disorder (0.2%% with harmful use and 2.0%% with dependence) involving at least one of the controlled substances in the last 12 months. Cannabis accounted for most drug-use disorders: 1.7%% of the sample qualified for a 12-month diagnosis of a cannabis-use disorder. Sedative-use disorders were next, affecting 0.4%% of the study population; 0.3%% met criteria for a stimulant-use disorder, and 0.2%% met criteria for an opioid-use disorder in the past 12 months (Figure 3).
Prevalence (%%) of substance-use disorders by gender: □, male; □, female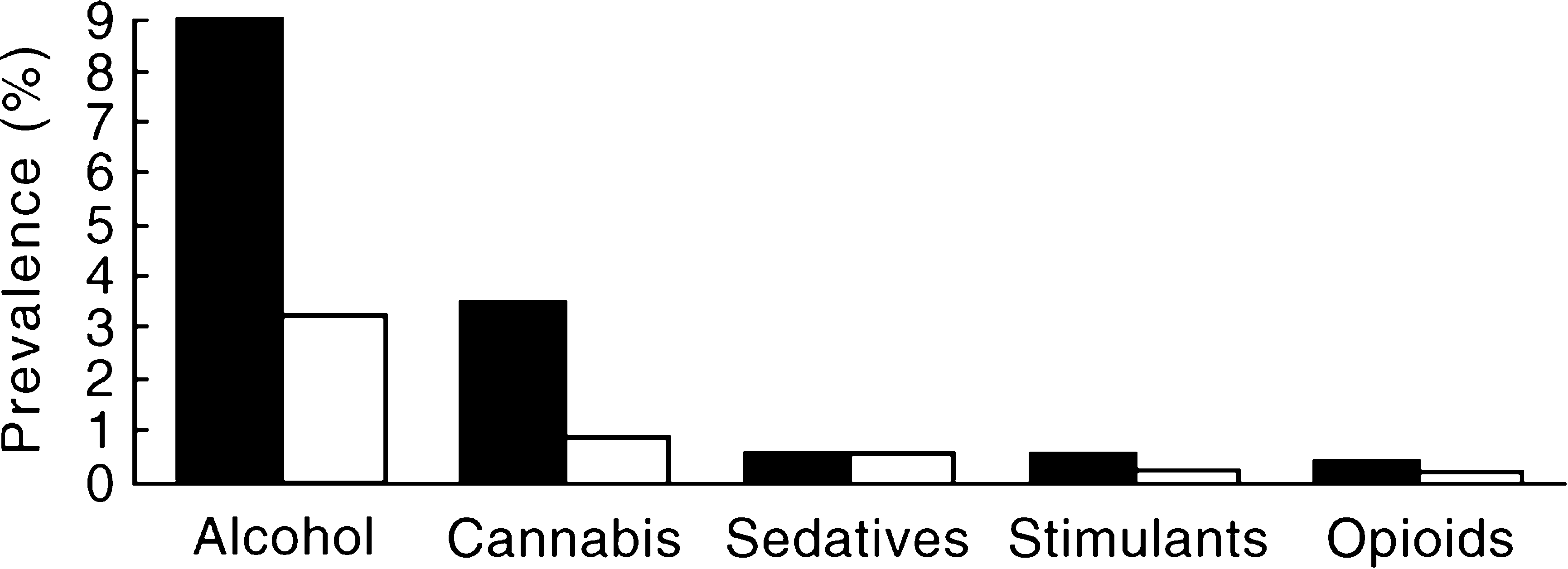
The prevalence of drug-use disorders was higher among males (3.2%%) than among females (1.3%%; Fig. 4). The prevalence of drug-use disorders decreased steadily with increasing age: drug-use disorders were highest among 18–34-year-olds (4.9%%) and lowest among those over the age of 55 years (0.8%%; Fig. 4).
Prevalence (%%) of drug-use disorders by age and gender: ▪, male; □, female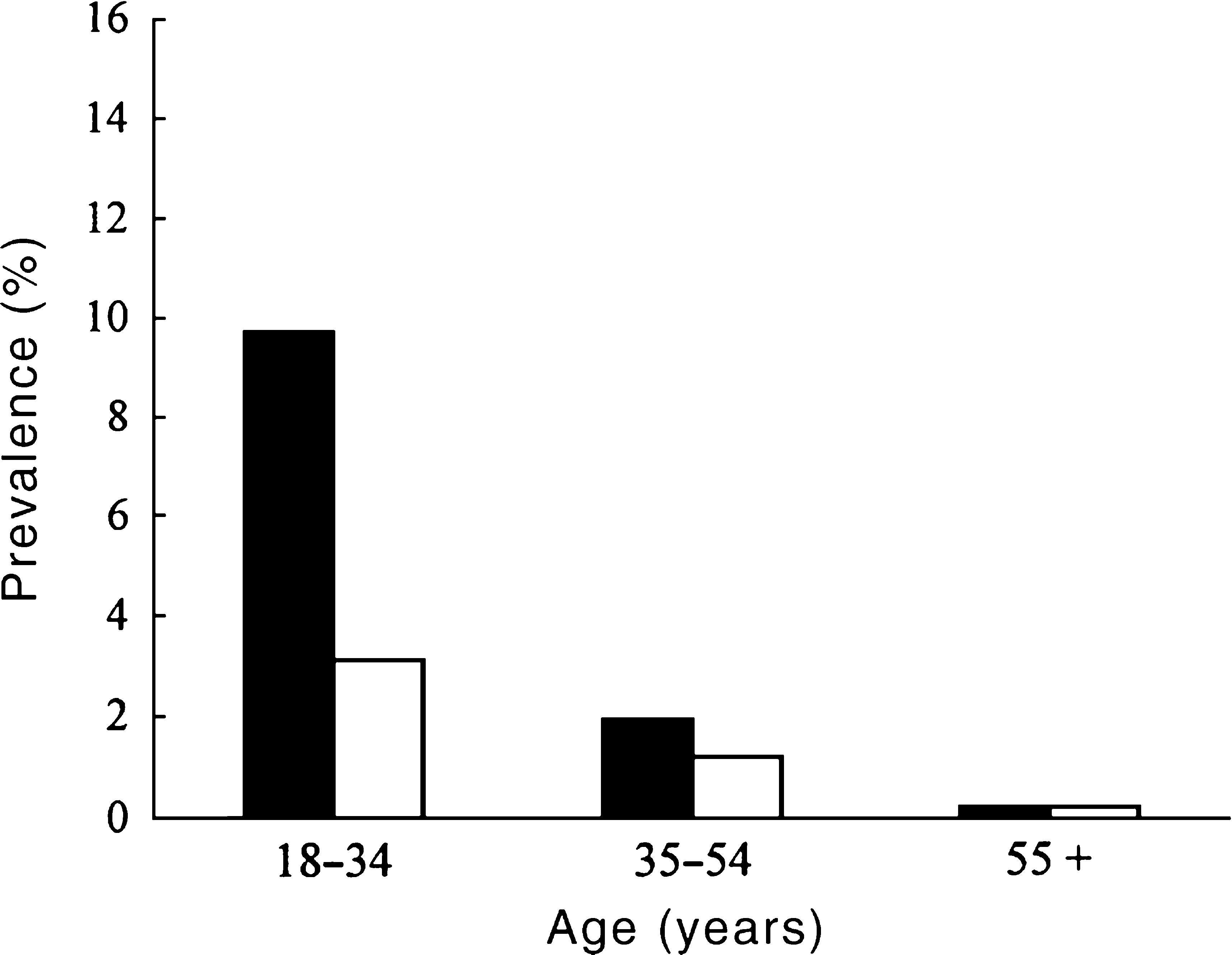
Drug-use disorders were more prevalent among the unemployed than the employed (7.8%% vs 2.1%%), those who had never married (6.3%%) compared with those who were separated or divorced (2.6%%) or those who were married (1.0%%), and those born in Australia (2.5%%) compared with those born in other English-speaking countries (1.4%%) and non-English-speaking countries (1.4%%). Drug-use disorders were also more common among persons living in capital cities (2.4%%) than outside capital cities (1.8%%).
The overwhelming majority of persons meeting criteria for drug dependence, regardless of drug class, reported that they had impaired control over their drug use (92–100%%) and either withdrawal symptoms or use of the drugs to avoid withdrawal (72–96%%; Table 1). Few of those individuals meeting criteria for stimulant dependence reported a desire or compulsion to use (17%%). Withdrawal symptoms were commonly reported by those dependent upon any drug (72–96%%) as against only half (50%%) of those who were alcohol dependent.
Comorbidity
There was considerable comorbidity between drug-use disorders and other mental disorders (Fig. 5). Two-thirds of females with a drug-use disorder (65%%) met criteria for an anxiety, affective or alcohol-use disorder. These rates were considerably elevated compared with females without drug-use disorders, 12%% of whom had an other mental disorder.
Comorbidity of mental disorders among males and females: □, anxiety; ▪, affective; ▪, drug; ▪, any two comorbid; ▪, all three comorbid; ▪, no other disorder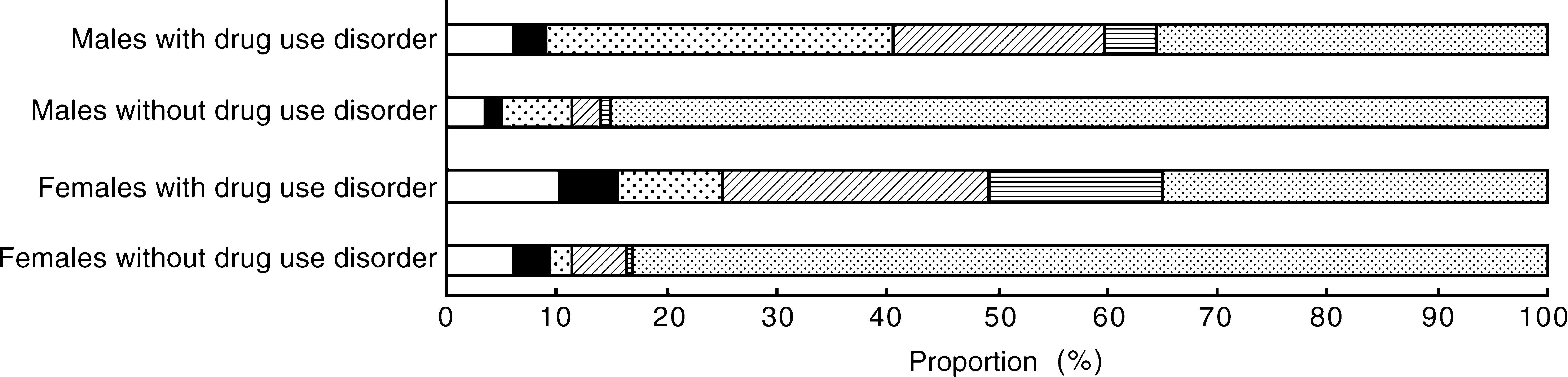
Nearly two-thirds of males with a drug-use disorder (64%%) met criteria for another mental disorder. By comparison, in men without a drug-use disorder only 11%% had another mental disorder. Four in 10 individuals with a drug-use disorder (42%%) had a comorbid physical disorder.
Treatment seeking
One-third of those with a drug-use disorder (36%%) had sought professional assistance in the past 12 months. Rates of help seeking were higher among females (56%%) than males (28%%). As with alcohol-use disorders, general practitioners were the most commonly consulted professionals (46%% of women and 27%% of men with a drug-use disorder). Relatively fewer people sought help from other professionals: 8%% of males and 14%% of females consulted a psychiatrist, and 4%% of men and 14%% of women consulted a psychologist. Other mental health professionals were consulted by 16%% of men and 19%% of women with a drug-use disorder.
Discussion
The prevalence of alcohol-use disorders in the past year in the NSMHWB were generally similar to the NCS and ECA studies [1],[2]. This was despite the use of different classification systems [18] (DSM-III in the ECA and DSM-III-R in the NCS) as against ICD-10 in this report. The findings of all these studies are consistent in showing that a substantial proportion of the adult population meets criteria for alcohol and other drug-use disorders. The correlates of these disorders were also similar in the different surveys. All studies found that the disorders were more common in males and young adults and that persons with the disorders had high rates of other comorbid mental disorders.
A consistent result was that men had higher rates than women of alcohol- and most drug-use disorders in all age groups. These gender differences may be due to much higher rates of exposure to heavy alcohol and drug use among males than females [1]. However, social changes may be reducing the differences between younger men and women. Tolerance of female drinking and more opportunities for young women to drink under more liberal licensing laws may have contributed to higher rates of drinking among young women [19]. The sex ratios for alcohol-use disorders reflect these changes: the ratio was 2.1 among those aged 18–34 years compared with 8.8 among those aged over 55 years.
There was a steady decrease in the prevalence of both alcohol- and drug-use disorders with increasing age. One possible explanation is decreased exposure to alcohol with age and historical differences between birth cohorts in exposure to alcohol use in youth and early adulthood [19]. The reasons for the decline in other drug-use disorders is less well studied; however, the same explanations are equally plausible, as older adults have had fewer opportunities to use drugs than younger adults.
Implications of comorbidity
Individuals who had an alcohol- or drug-use disorder in the NSMHWB had high rates of other mental disorders. Among females, half of those with an alcohol-use disorder and two-thirds of those with a drug-use disorder met criteria for another mental disorder. Among males, a third of those with an alcohol-use disorder and two-thirds of those with a drug-use disorder had another mental disorder.
This finding is consistent with other studies [1],[2] and has a number of implications for the treatment and management of alcohol- and drug-use disorders and other mental disorders. Mental disorders complicated by alcohol- and other drug-use disorders, and vice versa, have been recognised as having a poorer prognosis than those of patients without such comorbid disorders. Such disorders are also more likely to become chronic and disabling, and they result in greater service utilisation [20],[21]. Specialist mental health services need to better recognise and treat individuals with mental disorders comorbid with alcohol-and drug-use disorders. This is especially the case with anxiety and affective disorders, since substantial minorities of persons with these disorders who seek treatment in mental health services will have alcohol-and other drug-use disorders. Specialist drug and alcohol services also need to better recognise the most prevalent disorders that are most amenable to treatment, namely the anxiety and affective disorders [11].
Reducing the population impact of alcohol- and drug-use disorders
The NSMHWB found, as did the ECA and NCS, that only a minority of those who meet criteria for an alcohol and drug-use disorder had sought professional help for their disorder. Treatment seeking was related to gender with females being more likely to seek assistance than males and treatment was most likely to be sought from general practitioners.
The survey findings do not necessarily mean that 6.5%% of Australian adults need specialist treatment for alcohol-use disorders. Specialist treatment is one response that should form part of a general public health approach to reducing alcohol and other drug-use disorders. Public health policies that reduce the availability and increase the price of alcohol may also reduce the prevalence of alcohol-use disorders [22]. Public education about the risks of alcohol use may help to prevent some alcohol-use disorders, while advice on self-help strategies may obviate the need for professional assistance in a substantial proportion of younger milder cases [10].
The survey results show that the majority of individuals who seek assistance seek it from their general practitioners. Screening and brief advice for excessive alcohol consumption in general practice and hospital settings has been shown to reduce consumption and the problems caused by alcohol [23–25]. The survey accordingly identifies a need to improve the capacity of general practitioners to identify alcohol-use disorders by routine screening for hazardous and harmful alcohol use and to give advice on cutting down or stopping alcohol use and, when appropriate, referring persons with more severe disorders to specialist services. Screening is of considerable importance for males, who, according to the present survey, are less likely than females to seek assistance.
Controlled evaluations of treatment have demonstrated that approximately one-third of patients remain abstinent over a year, one-third show reductions in their drinking, while the drinking in the remaining third is largely unchanged [26]. There is also good evidence that treatment for alcohol dependence has a net economic benefit. Studies of insured persons [27],[28] show a substantial reduction in health care expenditure between the 3 years before and the 3 years after alcohol treatment. More recently, new pharmacological treatments such as acamprosate and naltrexone have proven effective in preventing relapse in people with alcohol dependence [29],[30]. While the efficacy of treatment has been demonstrated, there are currently no rational processes for deciding who of the 6.5%% of Australians with alcohol-use disorders should receive specialist treatment [10].
At present, specialist addiction services often involve protracted periods of detoxification and in-patient treatment. There is evidence from well-controlled studies [31] that in unselected patients with alcohol problems there is at most a small difference in outcome between inpatient treatment and simple assessment and advice to stop drinking. This indicates that residential or inpatient treatment is not routinely required for all persons with moderate to severe alcohol-use disorders, many of whom can in fact be successfully managed as outpatients. Further, it is not an effective use of scarce treatment resources.
The treatment response to illicit drug use is complicated by their illegality. The illegality prevents the use of the control policies that have been recommended to reduce alcohol-related health problems (namely increased taxation, and decreased legal availability). The major policies to reduce the availability of illicit drugs have been law enforcement efforts to interdict drugs at the customs barrier, prevent their distribution and reduce demand for drugs by prosecuting or diverting illicit drug users into treatment [32].
The major health policies aimed at reducing drug-use disorders have been mass media campaigns to discourage the use of illicit drugs. Among those who are not discouraged, efforts have been made to reduce some of the harmful consequences of drug use. Injecting drug users have been given clean needles and syringes, and educational programs designed by user groups have been used to communicate information about how to reduce drug-related harms.
Withdrawal symptoms were commonly reported by those dependent upon any illicit drugs (72–96%%) as against half (50%%) of those who were alcohol dependent. Consistent with this finding, detoxification is one of the interventions most often sought by dependent heroin users [33],[34]. This is a palliative treatment for opioid withdrawal that provides heroin users with a respite from drug use and provides an opportunity for outreach and education [33].
Drug substitution treatment substitutes a longer-acting, usually orally-administered, opioid drug for the shorter-acting heroin typically used by injection. It aims to stabilise the dependent heroin user so that they become more accessible and amenable to rehabilitation. Drug substitution is among the most popular forms of treatment with heroin users [34].
There has been a major increase in the provision of treatment for drug-use disorders in Australia, especially heroin users, with the numbers of such individuals enrolled in methadone treatment increasing from 800 in 1985 to 24 000 in 1999. This is a substantial proportion of those identified in this study as heroin dependent, however, the fact that the NSMHWB was a general population survey means that it is likely to under-represent the extent of heroin dependence in Australia. Methadone maintenance therapy is the most common form of drug substitution worldwide and to date it has been the only type of opioid substitution treatment that is routinely provided in Australia. It has been shown to be a good investment of community resources [35].
Conclusions
Alcohol- and other drug-use disorders are a major mental health issue for Australia. Men are at higher risk than women of developing these disorders because of their greater exposure to heavy drinking, although this may be changing. Drug-use disorders are much less common than alcohol-use disorders but they still affect around 2.2%% of Australians. They show similar patterns to alcohol dependence, with young men overrepresented because of their higher exposure to illicit drug use than young women or older people.
The prevalence of these disorders can be reduced by a range of public health strategies including efforts to reduce the availability of alcohol and public education about the risks of alcohol use. General practitioners who see the majority of persons with these disorders need to be better equipped to diagnose and intervene. Specialist treatment is required for persons with more severe alcohol and drug-use disorders that have resisted efforts at self help. Such treatment has substantial benefits for affected individuals and the community.
Footnotes
Acknowledgements
The design, development, and conduct of the National Survey of Mental Health and Wellbeing was funded by the Mental Health Branch of the Commonwealth Department of Health and Aged Care. The development and testing of the computerised survey instrument was undertaken by the WHO Collaborating Centre in Mental Health at St Vincent's Hospital, Sydney. The fieldwork and implementation of the Survey, the enumeration, compilation and initial analyses of the data were undertaken by the Australian Bureau of Statistics. Neil Buhrich and Andrew Baillie provided helpful comments on earlier drafts.