
Abstract
Over the last decade excessive or binge drinking among young people has become a major public health concern. While much focus and concern has rested with underage drinking, recent reports suggest that in fact the most excessive drinkers are young adults [1, 2]. Using guidelines from the National Health and Medical Research Council (NHMRC) [3], based on short-term (accident/injury) and long-term risks (cancer, liver cirrhosis, and alcohol dependence), young adults are again the highest drinkers, with around one in seven 20–29-year-olds drinking at rates that put them at moderate to high risk for long-term alcohol-related problems [4, 5].
One explanation for excessive drinking by many young adults may be that these young people already have an alcohol use disorder, that is, alcohol abuse or dependence. Recent evidence suggests that, in Australia, young adults have the highest rates of alcohol use disorders compared to other age groups [6]. Lifetime rates of DSM-IV alcohol use disorders in young adults (under 29 years of age) evident in two major US epidemiological studies range from 27 to 29% for men, and 7 to 15% for women [7, 8]. Data from the Australian National Survey of Mental Health and Well-Being (NSMHWB) [6] suggest that almost 16% of men and 6% of women aged 18–36 years met criteria for alcohol abuse or dependence in the previous 12 months. These rates are consistent with, but slightly higher than, those found in the two US studies in which 12% of men and 2% of women met criteria for an alcohol use disorder in the past 12 months [7, 8].
While alcohol consumption and the risk of dependence are positively associated [9], patterns of drinking vary among those with alcohol use disorders [10] and, because quantity of alcohol consumption is not a criterion for a diagnosis of alcohol use disorder in either the DSM-IV or the ICD-10, one cannot simply assume that all heavy drinking is done by those with an alcohol use disorder. To date there has been little research examining the association between risky drinking (as defined by the NHMRC guidelines in terms of quantity) and alcohol use disorders. Yet in terms of enabling, designing, and providing appropriate health care and management of alcohol-related problems to youth, this question is of considerable importance. The present study sought to describe the association between excessive or high-risk drinking and the presence of an alcohol use disorder in young adults.
Methods
Procedure and sample
Data were collected from young adults aged 24–25 years as part of the Victorian Adolescent Health Cohort Study. A detailed description of the design and methods is given in a previous publication [11], and therefore is only briefly outlined here. The cohort was selected in 1992 using a two-stage procedure with schools as the primary sampling units and classes (within schools) as the secondary sampling units. This paper is based on analyses of data obtained in the eighth wave of the study when the cohort members were aged 24–25 years.
Of the 2032 students selected for the cohort, 1943 (96%) participated at least once during the first six waves. In wave 8, 1520 (75% of those selected and 78% of wave 1–6 participants) were interviewed between May 2001 and March 2003. Reasons for non-completion at wave 8 were refusal (n = 269), not contactable (n = 147) and death (n = 7). The mean (SD) age was 24.1 (0.6) years at wave 8. Omitting the seven cases due to death, the total number of participants for these analyses was n = 1936.
Measures
Alcohol use
Recent alcohol use was assessed by asking participants on which days they had drunk alcohol in the past week. Amount of alcohol consumed on Friday, Saturday, Sunday, and the most recent week day (of Monday, Tuesday, Wednesday and Thursday) was recorded by asking participants what types of alcohol they consumed, the container that it was consumed from (e.g. a “pot” of beer in Victoria is 285 mL), and how many of each combination of alcohol and container were consumed. To reduce respondent burden in completing a lengthy interview, the one detailed weekday report was extrapolated to other weekdays if drinking occurred (e.g. if they indicated drinking on Monday and Tuesday, it was assumed that the same amount was consumed on each of these 2 days), enabling the estimation of total alcohol consumption for the week prior to the survey. Those who reported 12 or more drinking occasions in the past 12 months were classified as ‘drinkers’.
We used the NHMRC drinking guidelines [3] to classify the participants according to their risk drinking status. The guidelines define short-term alcohol-associated risk in terms of an excessive volume consumed in a single day, and the associated risks are intoxication and impaired judgement leading to accidents, injury and death [3]. Short-term risk is specified in the following manner: low risk, <5 drinks for female subjects and <7 drinks for male subjects per drinking day; risky or moderate risk, 5–6 drinks for female subjects and 7–10 for male subjects per drinking day; high risk, ≥7 drinks for female subjects and ≥11 drinks for male subjects per drinking day. Long-term risk is defined by the total amount of alcohol consumed in a typical week and the risk is associated with health problems caused by chronic alcohol consumption (such as cardiovascular problems or liver disease). Long-term risk is specified in the following manner: low risk, <15 drinks per week for female subjects, <29 per week for male subjects; risky or moderate risk, 15–28 drinks per week for female subjects, 29–42 drinks per week for male subjects; high risk, ≥29 drinks per week for female subjects, ≥43 drinks per week for male subjects. Although the NHMRC guidelines use the term ‘risky’, for ease of expression we will refer to that category as ‘moderate’.
There is evidence that individuals who fall in the high-risk drinking categories often consume considerably more than the levels indicated in the category [12]. Therefore to capture the maximum alcohol consumption in 1 day by young people that falls above the high-risk NHMRC level, we categorized maximum alcohol consumed into the following groupings of standard drinks: 0–5, 6–10, 10–15, 16+.
Assessment of DSM-IV alcohol abuse and dependence
The Composite International Diagnostic Interview (CIDI) was used to assess alcohol use disorders (abuse and dependence) as per the DSM-IV (1994). Alcohol use disorders were assessed in those individuals who reported that they had consumed more than 11 standard drinks in the last 12 months. To receive a DSM-IV diagnosis of alcohol abuse participants must fulfil one of the following criteria: recurrent failure to fulfil major role obligations at work, school, or home, recurrent use in physically hazardous situations, recurrent alcohol-related legal problems, continued use despite persistent social or interpersonal problems. To obtain a DSM-IV diagnosis of alcohol dependence, participants must fulfil at least three of the following criteria: tolerance as indicated by increasing amounts of alcohol needed to become intoxicated, withdrawal as indicated by a number of physiological symptoms on cessation of alcohol use, use for longer or in larger amounts than intended, persistent desire or unsuccessful attempts to cut down, excessive amounts of time spent obtaining, using or recovering from alcohol, important social, occupational or recreational activities given up because of alcohol use, and continued use despite knowledge of physical or psychological harm caused by alcohol. In DSM-IV, alcohol abuse and dependence are mutually exclusive hierarchical diagnoses, such that alcohol abuse is diagnosed only in those not meeting diagnosis for alcohol dependence.
Analysis
More than 20% of the original Victorian Adolescent Health Cohort Survey (VAHCS) participants were not interviewed in wave 8 data and a minority provided data at all waves. The results of ‘complete case’ analyses based on only those with complete data at all waves could potentially be biased. Analyses were therefore performed using the method of multiple imputation [13] to allow for missing data on outcomes and predictor variables. This method has advantages over simpler imputation methods such as mean substitution and last observation carried forward, both in its potential to reduce bias and in the appropriate accounting of variance due to uncertainty about the true unobserved values. Under this method several copies of the dataset are created using a modelling process that imputes a value for each missing item, and final analyses are obtained by combining the results obtained by applying standard complete-data methods to each of the imputed datasets. Imputed values are randomly drawn using a modelling process that allows for uncertainty in the model parameters, and includes predictive information from related variables that may or may not have missing values themselves. In this study, a multivariate normal model was used to impute the missing data to create five different complete datasets used for the analyses of this paper. Variables measuring alcohol and drug use, and variables known to be associated with alcohol and drug use, from all eight waves of the VAHCS study were included in the imputation model, along with key sociodemographic covariates (child sex, parental education and ethnicity, parental marital status, urban vs rural residence). Imputation was performed using the NORM package for Windows [14] (http://www.stat.psu.edu/∼jls/misoftwa.html), and the mi commands in Stata [15] were used to analyse the imputed data.
The percentages of participants who were classified into each category of risky drinking and alcohol abuse and dependence were calculated with 95% confidence intervals (CI). Multinomial logistic regression was used to investigate the nature of the relationship between alcohol disorder diagnosis status (as a covariate) and the outcomes risky short-term drinking and risky long-term drinking, controlling for gender. The categories of the alcohol disorder variable were: alcohol use with no disorder (reference category), alcohol abuse and alcohol dependence. Tests of interaction were implemented to investigate whether the nature of the relationship between alcohol disorder status and the high-risk drinking outcomes differed between male and female subjects. Non-drinkers were excluded from the multinomial regression analyses. Logistic regression was used to examine the association between gender and a diagnosis of having a diagnosis of alcohol abuse or alcohol dependence.
Results
Drinking patterns
The majority (86%) of participants were classified as current drinkers, reporting ≥12 drinking occasions in the past 12 months (Table 1). In the previous week, 41% of the total sample drank at rates that were moderate or high risk for short-term harm. A markedly larger proportion of female than male subjects were in the non-drinking category (20% compared with 8%) and a larger proportion of male subjects fell into the high short-term risk category; half of the male subjects reported consuming ≥7 standard drinks on 1 day in the past week. The frequency of moderate- to high-risk long-term-risk drinking was substantially lower than the frequency of moderate- to high-risk short-term-risk drinking. Around 1 in 7 male subjects and 1 in 17 female subjects reported alcohol consumption at levels considered to be of high long-term risk. Thirty-six percent (95%CI = 32–40) of male drinkers and 21% (95%CI = 18–24) of female drinkers reported drinking on ≥3 days in the past week.
NHMRC measures of risky short-term and long-term alcohol use
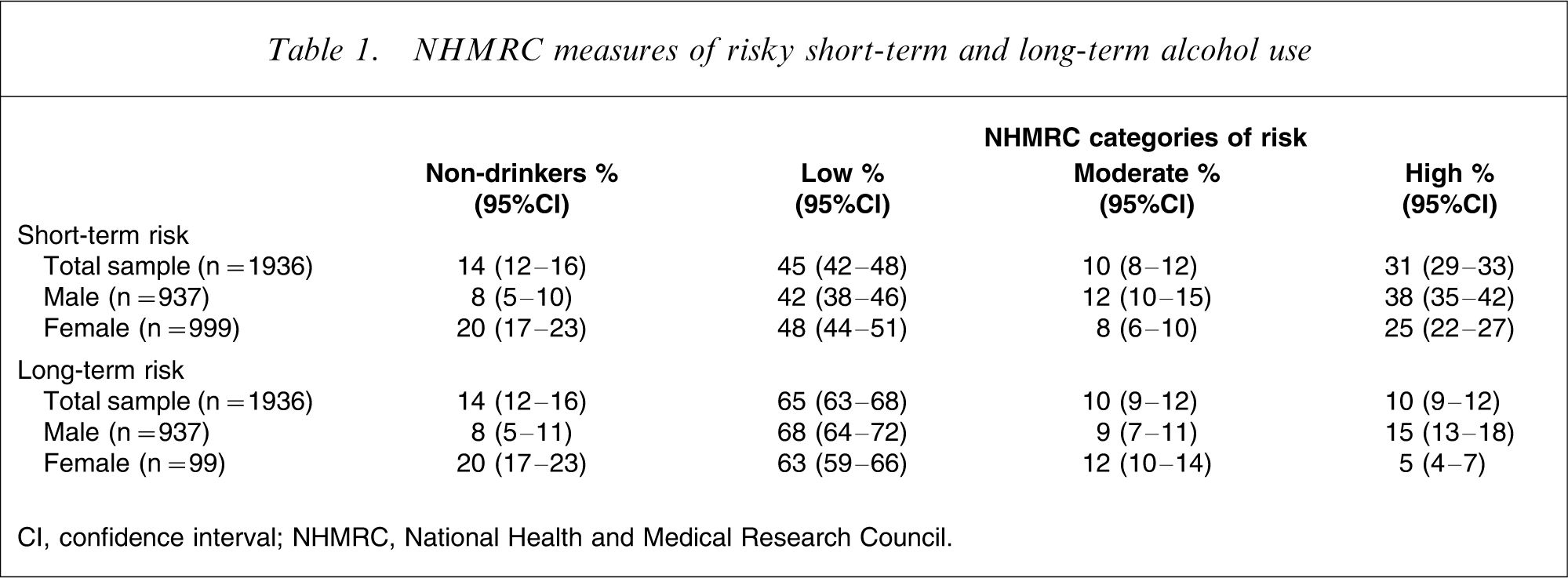
CI, confidence interval; NHMRC, National Health and Medical Research Council.
Alcohol use disorders
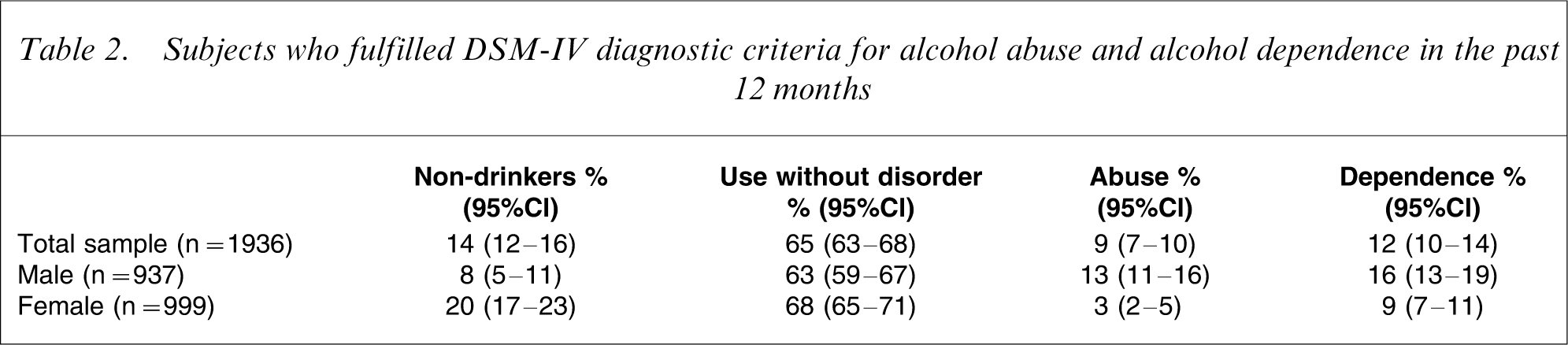
An estimated 8% of the total sample met DSM-IV criteria for alcohol abuse, and 12% met DSM-IV criteria for alcohol dependence in the past 12 months (Table 2). The odds of abuse were more than fourfold higher (odds ratio (OR) = 4.2, 95%CI = 2.7–6.5) and the odds of dependence were twofold higher (OR = 2.0, 95%CI = 1.5–2.7) among male than female subjects.
Subjects who fulfilled DSM-IV diagnostic criteria for alcohol abuse and alcohol dependence in the past 12 months
We examined the maximum volume of alcohol consumed on one occasion in the past week. Overall, 54% (95%CI = 51–58) of drinkers who did not gain a diagnosis of alcohol abuse or dependence reported a maximum alcohol consumption of <5 standard drinks and only 16% (95%CI = 14–18) reported consuming ≥16 standard drinks on one occasion. In contrast, for those who met criteria for an alcohol use disorder, only 29% (95%CI = 24–35) reported a maximum alcohol use of <5 standard drinks, and 36% (95%CI = 31–41) reported consuming ≥16 standard drinks in one session in the past week.
Association between alcohol use disorders and alcohol consumption among drinkers
Of those drinking at high short-term risk levels, 13% (95%CI = 10–16) were diagnosed with alcohol abuse, and 23% (95%CI = 19–28) were diagnosed with alcohol dependence. Of those drinking at high long-term risk levels, 16% (95%CI = 11–22) were diagnosed with alcohol abuse, and 33% (95%CI = 25–41) were diagnosed with alcohol dependence. The results of fitting multinomial logistic regression models to examine the association between alcohol use disorders and short-term risky drinking and long-term risky drinking are shown in Tables 3 and 4, respectively. The results of interaction tests suggested that there was no strong evidence that the relationship between alcohol use disorders and risky drinking status differed between male and female drinkers, all p > 0.05.
NHMRC risky short-term alcohol use
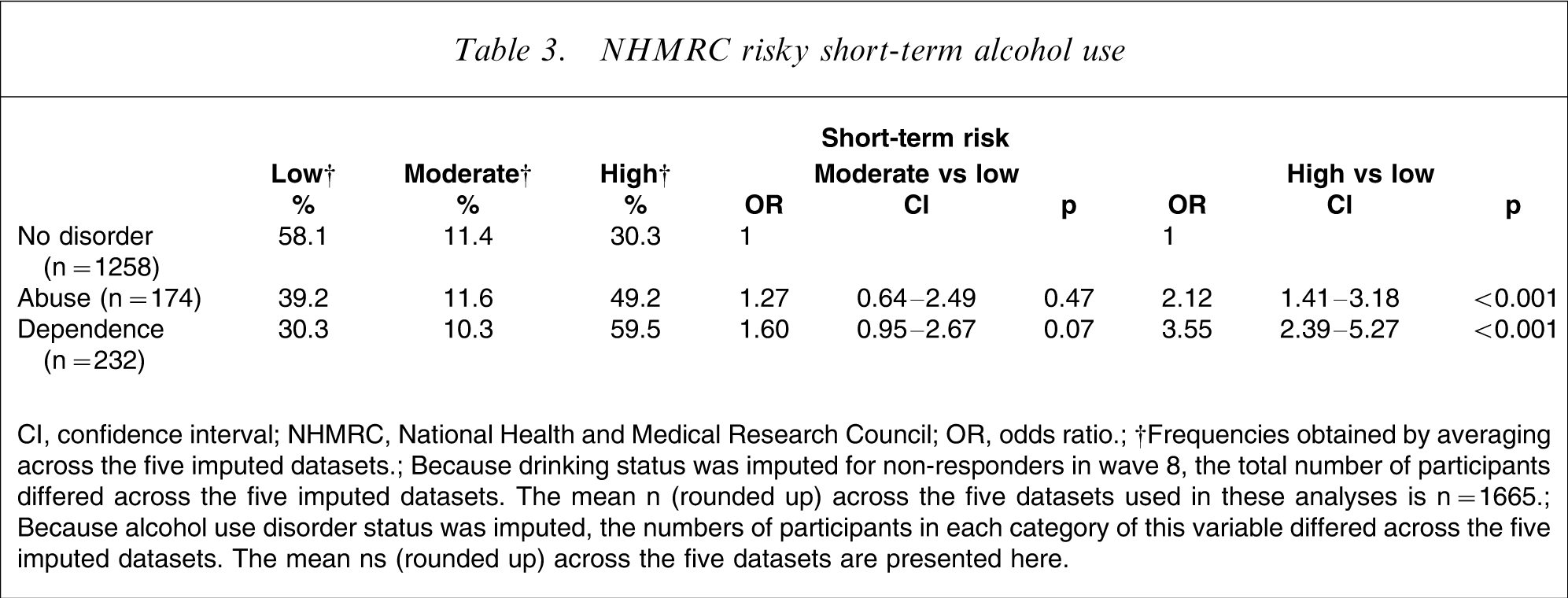
CI, confidence interval; NHMRC, National Health and Medical Research Council; OR, odds ratio.
†Frequencies obtained by averaging across the five imputed datasets.
Because drinking status was imputed for non-responders in wave 8, the total number of participants differed across the five imputed datasets. The mean n (rounded up) across the five datasets used in these analyses is n = 1665.
Because alcohol use disorder status was imputed, the numbers of participants in each category of this variable differed across the five imputed datasets. The mean ns (rounded up) across the five datasets are presented here.
NHMRC risky long-term alcohol use
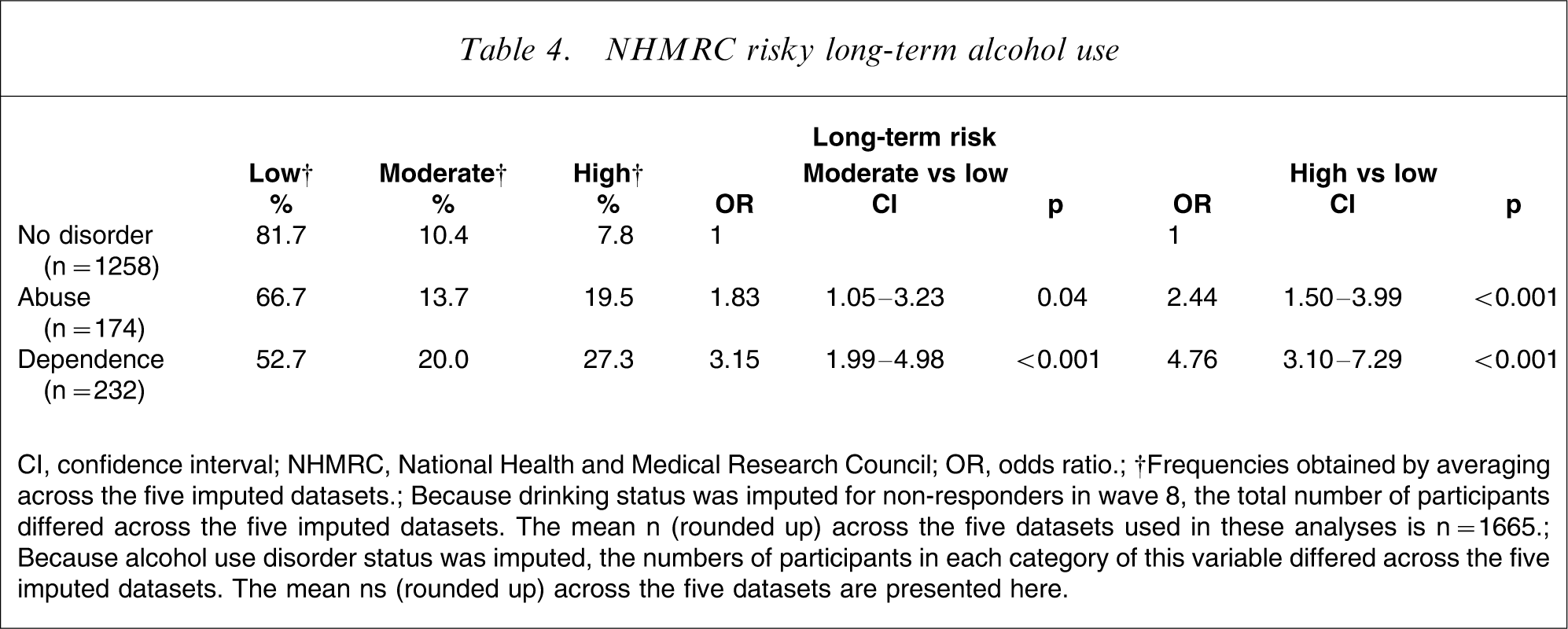
CI, confidence interval; NHMRC, National Health and Medical Research Council; OR, odds ratio.
†Frequencies obtained by averaging across the five imputed datasets.
Because drinking status was imputed for non-responders in wave 8, the total number of participants differed across the five imputed datasets. The mean n (rounded up) across the five datasets used in these analyses is n = 1665.
Because alcohol use disorder status was imputed, the numbers of participants in each category of this variable differed across the five imputed datasets. The mean ns (rounded up) across the five datasets are presented here.
Approximately two-fifths of drinkers without an alcohol use disorder drank at moderate- to high-risk levels for short-term harm. There appeared to be only weak evidence of an association between a diagnosis of abuse or dependence and being in the moderate short-term-risk drinking category (as opposed to low-risk drinking). The odds of high short-term-risk drinking (as opposed to low short-term risk) were 2.12-fold larger for those with alcohol abuse and 3.55-fold larger for those with alcohol dependence relative to drinkers without a diagnosis of alcohol use disorder.
In terms of long-term harmful drinking (weekly consumption), more than half of those with alcohol abuse or dependence reported alcohol consumption in the low long-term risk category. A stronger association between longer-term risk drinking and diagnoses of abuse or dependence was evident than for short-term risk drinking. For those with a diagnosis of abuse the odds of drinking at moderate long-term risk levels (as opposed to low risk) were 1.83-fold higher than for drinkers with no alcohol use disorders, and the odds of drinking at high-risk levels (as opposed to low risk) were 2.44-fold higher compared to drinkers without an alcohol disorder. For those with a diagnosis of dependence the odds were 3.15-fold higher that they would drink at moderately risky levels for long-term harm and 4.76-fold higher for drinking at high-risk levels for long-term harm compared to drinkers without an alcohol disorder.
Discussion
Two out of five of the 24–25-year-olds in this sample drank at rates that are moderate to high risk for short-term harm. Fewer young adults, one in five, drank persistently at moderate to high risk for long-term harms. The presence of an alcohol use disorder accounted for, at most, only a minimal amount of excessive drinking bouts. Longer term moderate- and high-risk consumption was more common in those with an alcohol use disorder, yet fewer than half of those with an alcohol use disorder actually fell into these long-term harm categories. Therefore, the high rates of risky alcohol consumption in young adults as found in both the present study and previous research [6–8], cannot simply be attributed to the co-occurrence of high rates of alcohol use disorders in young people. The majority of moderate- and high-risk drinking is done by those who do not meet criteria for an alcohol use disorder.
The prevalence of alcohol use disorders in this age group is higher overall than both the NSMHWB [6] and other international epidemiological surveys [7, 8], but consistent with the gender patterns in those studies. The prevalence of alcohol use disorder was markedly greater for male than female subjects. The prevalence of moderate and high long-term-risk drinking in this sample is considerably higher than reported in the National Drug Strategy Survey [4]; a difference that may be attributable to a lower response rate (50%), national sampling and a larger age range (20–29 years) in the latter study.
Some potential limitations of this study should be noted. First, there is some evidence that the CIDI may overdiagnose alcohol use disorders in community samples [16] thereby elevating population estimates of alcohol use disorders. Nevertheless, despite the possible elevation of estimates, we found that most risky drinking occurs in those without an alcohol use disorder. At present, self-report in community studies remains the best method for capturing a complete picture of alcohol use disorders in young adults [17]. Second, the alcohol-use diary, on which the short-term and long-term risk categories were based, assessed alcohol use only in the last 7 days and actual volumes for the weekend and one weekday with extrapolation to other weekdays as necessary. Although justified by the limited extent to which individuals can accurately report on patterns and volume of alcohol consumption over longer time periods [18], there would inevitably have been variation from week to week with some resultant measurement error.
Excessive drinking once or twice a week is common for young adults, including many of those without alcohol abuse or dependence. It is likely that social factors underlie much of this excessive consumption. Excessive drinking by young adults tends to occur on the weekends in social settings of excessive use among like-minded peers [19]. One distinction found in the present study between non-problem drinkers and those with an alcohol use disorder was the quantities consumed during a drinking session. For example, while consuming >5 standard drinks in a session is common practice among young adults, more than one-third of those with alcohol dependence consumed >15 standard drinks in one session within the last week. Therefore, from a clinical perspective, young adults with alcohol use disorders may appear to have a similar drinking pattern to their non-problem drinking peers: They drink to excess during drinking sessions, but do not drink consistently or steadily throughout the week and are unlikely to show symptoms of withdrawal or report the social narrowing typically associated with tertiary alcohol use disorders [12]. It is important for clinicians to focus on the quantity of alcohol consumed rather than the number of drinking days when diagnosing alcohol use problems in young adults.
Footnotes
Acknowledgements
We acknowledge the funding support from the Alcohol Education and Rehabilitation Fund, the National Health and Medical Research Council and the Victorian Health Promotion Foundation.