
Abstract
Objective:
This study presents rates of suicide thoughts and behaviours of police and emergency services personnel around Australia. In addition, it examines personal (i.e. mental health, substance use) and working environment risk and protective factors.
Method:
A stratified random sample of personnel from 33 Australian emergency services organisations were invited to participate in a mental health and wellbeing survey. In total, 14,868 Australian ambulance, fire and rescue, police and state emergency services employees participated and self-reported any suicidal thoughts, plans and/or attempts in the 12 months prior to the survey or at any stage in their life. Logistic regressions assessed factors associated with suicidal thoughts and behaviours.
Results:
Employees reported notably higher rates of suicidal thoughts and plans than the general Australian adult population, but not attempts. Male, single/divorced, non-heterosexual or longer-serving employees reported higher rates of suicidal thoughts and behaviours across each sector. Perceptions of stigma regarding mental health conditions from others in the workplace, negative impact of work on one’s private life and low meaning of work were associated with suicidal thoughts, while bullying significantly differentiated who planned and attempted suicide from those who reported suicidal thoughts only. Higher resilience and social support were associated with lower suicidal thoughts, while intermittent explosive anger and illegal drug use were associated with higher rates of suicidal thoughts. Post-traumatic stress disorder symptoms significantly differentiated who planned suicide, while misuse of prescription drugs and psychological distress differentiated who attempted suicide from those who only reported suicidal thoughts.
Conclusion:
Amid inherently stressful occupations, it is important that workplaces function in a way that supports their personnel. Access to mental health services should be promoted and readily available to personnel.
Research suggests that, at the start of their careers, police and emergency services personnel (i.e. police, ambulance, firefighters and state emergency services workers) are mentally healthy (Hodgins et al., 2001). Yet, longer periods of service are associated with higher levels of psychological problems (e.g. psychological distress, post-traumatic stress disorder (PTSD); Carleton et al., 2018). Higher rates of psychological distress may be a consequence of the inherent stressful nature of working in an emergency services role and a poorly functioning workplace (Meyer et al., 2012). The propensity among police and emergency services personnel to experience distress due to working conditions is concerning due to its association with an increased risk of contemplating and planning suicide among police and emergency services personnel, as well as other harmful behaviours (e.g. substance use; Carleton et al., 2018; Harvey et al., 2016; Stanley et al., 2015; Sterud et al., 2008; Violanti, 2004).
Reducing employee suicidal thoughts and behaviours is a major goal for many emergency services organisations worldwide. Yet, within an Australian context, there is a lack of research assessing suicide risk among personnel (Varker et al., 2018). Retrospective mortality studies have found Australian emergency personnel to be largely at a heightened risk of suicide completions when compared with adults in other occupations (Milner et al., 2017). However, studies assessing the prevalence of suicidal thoughts and behaviours (i.e. plans, attempts) among this population are non-existent, with no wide-scale national studies conducted within the region. In addition, studies assessing factors associated with negative outcomes which are targetable through interventions have yet to occur.
The exposure to traumatic and/or life-threatening incidents, and injuries or deaths of colleagues are commonly experienced while working in emergency services occupations, and can be particularly stressful when repeatedly experienced (Gershon et al., 2002; Kimbrel et al., 2016). Indeed, Violanti (2004) found that traumatic work exposures are associated with an increased risk of developing PTSD symptoms, which in turn was associated with a heightened risk of suicidal ideation. However, there are additional stressors which may influence mental health, such as poor workplace communication, heavy workload, workplace discrimination and/or harassment (Meyer et al., 2012; Skeffington et al., 2017; Sterud et al., 2008). In a national survey of Norwegian ambulance personnel, symptoms of depression, job related emotional exhaustion and bullying were associated with higher levels of suicidal ideation (Sterud et al., 2008). Further research is needed to explore how workplace experiences influence suicidal thoughts and behaviours among personnel.
While a negative working environment may have direct effects on mental health, it may also have more insidious effects through inhibiting positive help-seeking behaviours. Without appropriate treatment and support, mental health problems can cause problems at work and at home, and result in loss of employment or, in worst-case scenarios, suicide (Bloodgood, 2006; Chae and Boyle, 2013). Perceptions of being seen as weak and negative career consequences from signalling the need for help are cited as particular aspects of stigma that may prevent help-seeking (Hom et al., 2016). Research into police has found that individuals are more likely to seek help when they perceive support within their environment (Heffren and Hausdorf, 2016). Thus, there is a complex interaction between various workplace factors that may exacerbate or protect against suicide.
This study provides findings from the first national survey of Australian police and emergency services personnel, and the largest to date worldwide. The survey acted to inform strategies to reduce the risk of suicide among emergency personnel. In addition to presenting the prevalence of suicidal thoughts and behaviours, this study builds on prior research by assessing the relationships between suicidal thoughts and behaviours and a variety of personal (e.g. mental health conditions, resilience, substance use) and workplace (e.g. perceived bullying, support, stigma) factors. Specifically, it examines which factors differentiate those who think about suicide from those who have acted on their suicidal thoughts (Klonsky and May, 2014). Research to date has only established correlates of suicidal thoughts and attempts among emergency personnel, rather than assess which factors may signify an increased risk of acting on suicidal thoughts.
Method
Participants and procedure
Thirty-three emergency services organisations from around Australia participated in the survey, with a total of 14,868 employees partaking (police = 8088; ambulance = 3473; fire and rescue = 2975; state emergency service = 332). The survey looked to assess the prevalence of mental health conditions of personnel, and experiences within the workplace, such as trauma, stigma, support and bullying. The survey was advertised as a mental health and wellbeing survey and was both commissioned and advocated by prominent Australian mental health advocacy group, Beyond Blue. Employees were contacted via email and could voluntarily complete the survey online or through physical copies, which took around 25 minutes to complete. The characteristics of the sample are summarised in Table 1.
Sample characteristics.
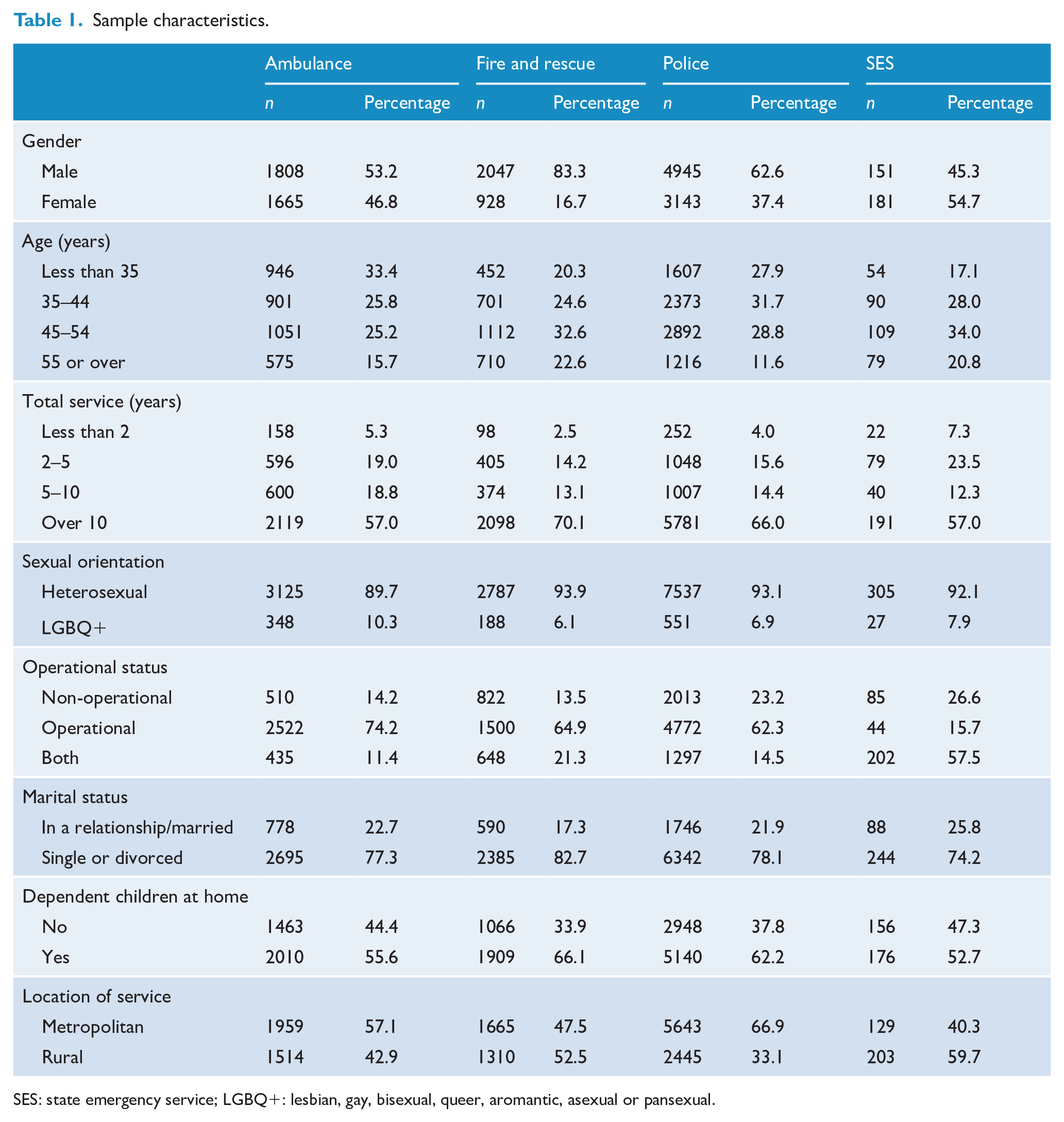
SES: state emergency service; LGBQ+: lesbian, gay, bisexual, queer, aromantic, asexual or pansexual.
Each agency provided information on the demographic composition of their workforce, from which a stratified random sample of their current employees was selected (or full censuses in smaller agencies). In total, there was a 22% response rate in this study. The profile of survey participants was compared to several sources, such as the 2016 Census of Population and Housing and the Productivity Commission’s Report on Government Services to examine sample representativeness and to inform weighting strategies. Although response bias is difficult to determine, the characteristics of the sample were compared to the known demographic characteristics of employees in the sector. Overall, response bias was found to be low, and more information regarding calculations is presented in Supplemental Material and prior research (Lawrence et al., 2018). In short, those with mental health issues were not more likely to participate early in the study, and there was no significant association between response rates and rates of mental health conditions in individual agencies. When compared to known demographic characteristics of personnel in the sector, survey respondents were slightly more likely to be female, older and in non-operational roles. No differences were found in terms of country of birth, educational status, marital status or number of children.
Measures
Suicidal thoughts and behaviours
Six questions in total were used to assess suicidal thoughts and behaviours. Participants were asked whether they had seriously thought about taking their own life, planned to take their life or attempted suicide in the past 12 months or any stage in their life, and could answer in a yes/no format. Questions were available in a conditional manner, such that questions regarding suicide plans were offered only if an employee had reported thinking about suicide. Furthermore, attempts could only be reported if employees had previously indicated planning a suicide attempt. Employees could also indicate whether they preferred not to answer each question in order to minimise socially desirable responding which may cause inaccuracies in prevalence figures. These questions were derived from the 2007 National Survey of Mental Health and Wellbeing (NSMHWB; Australian Bureau of Statistics [ABS], 2007).
Psychological distress
The Kessler-10 questionnaire was used to measure symptoms of depression and anxiety in the 30 days prior to the survey (Kessler et al., 2002). There are 10 items in total which measure emotional states using a five-item Likert-type scale (1 = None of the time, 5 = All of the time). Higher scores on the measure represent a greater likelihood of experiencing a mental health condition. The scale has been shown to perform well in screening for mood and anxiety disorders (Furukawa et al., 2003) and had excellent internal consistency (α = 0.92)
Intermittent explosive anger
The 2007 NSMHWB (ABS, 2007) included four items to measure symptoms of anger in the prior 4 weeks. The scale had acceptable internal consistency in the current survey (α = 0.77) and in prior studies (α = 0.72–0.81), and individuals diagnosed with intermittent explosive disorder scored higher on the measure than those without the disorder in prior research (Barrett et al., 2013).
PTSD symptoms
To assess symptoms of PTSD, an adapted version of the PCL-5 (PTSD Checklist for DSM-5) PTSD screening scale was used (Blevins et al., 2015). This shortened version aimed to encapsulate the core criteria for a diagnosis of PTSD, such as experiencing repeated and unwanted memories or nightmares about stressful experiences, flashbacks and strong physical reactions in the 4 weeks prior to the survey. Additional questions were included to reflect the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) diagnostic criteria for PTSD (American Psychiatric Association, 2013), such as symptoms having to last for a minimum of 1 month and be associated with clinically significant distress or functional impairment. The PCL-5 screening scale has been shown to have strong psychometric properties (Blevins et al., 2015), and the adapted version had good internal consistency in the current survey (α = 0.89). Higher total scores on the scale represent likely experiencing more symptoms of PTSD.
Resilience
A shortened three-item version of the Brief Resilience Scale (Smith et al., 2008) was used to measure aspects of resilience, or the ability to bounce back from adversity, using a five-point Likert-type scale (1 = Strongly disagree, 5 = Strongly agree). The full measure had good psychometric properties in prior research (Smith et al., 2008) and good internal consistency in the current sample (α = 0.88). Higher scores on the scale represent higher self-reported resilience.
Social support
Social support was measured through the use of an adapted version of the 2-Way Social Support Scale (Shakespeare-Finch and Obst, 2011). Seven items in total assessed emotional support received, with four items retained from the original scale and an additional three items created to assess support specific to work (e.g. ‘My family/friends understand my job demands’). Higher scores on the scale represent receiving higher perceived support from others. The adapted scale was shown to have good levels of internal consistency in the current sample (α = 0.87).
Psychosocial working environment
Eight items were extracted from the second version of the Copenhagen Psychosocial Questionnaire (COPSOQ-II) to assess employees’ working environments (Pejtersen et al., 2010): meaning of work, work/family conflict (i.e. work negatively impacting one’s private life), supervisor support and recognition of work and fairness. Four additional items were developed to measure exposure to emotionally disturbing situations, the ability to take time off following traumatic incidents and work/life balance. Items were measured on a five-point Likert-type scale (1 = Never, 5 = Always). Items had acceptable psychometric properties in prior research (Pejtersen et al., 2010), and all items had acceptable internal consistency in this study (α = 0.77). Higher scores on each sub-scale represent more frequent negative experiences within one’s working environment.
Bullying
One question was used to assess the frequency of perceived bullying within the workplace in the 12 months prior to the survey (1 = Never, 6 = Almost daily). If participants indicated experiencing some bullying, a second question was made available to assess the stress that bullying causes them (1 = No stress, 6 = Extreme Stress). Both items were combined to create a total bullying score with higher scores representing more frequent and stressful bullying.
Stigma
Three items adapted from the Depression Stigma Scale (Griffiths et al., 2004) were used to assess an employee’s perceptions that others within their organisation hold stigma regarding mental health issues. Shame surrounding one’s own mental health issues was captured through three questions from the Self-Stigma of Depression Scale (SSDS; Barney et al., 2010), which were only available to employees who reported a lived experience with mental health issues. Items were measured on a five-point Likert-type scale (1 = Strongly disagree, 5 = Strongly Agree). If participants on average agreed or strongly agreed with items on each scale, they were deemed to have high stigma, while disagreeing indicated low stigma. Perceived (α = 0.74) and self-stigma (α = 0.84) items had acceptable to good internal consistency in this study. Higher scores on the scales represent higher stigma regarding mental health.
Organisational commitment
Five items were developed to assess an employee’s perception of how committed the organisation they work for is to promoting positive mental health and supportiveness of colleagues and management towards those with mental health issues. All items were measured on a five-point Likert-type scale (1 = Strongly disagree, 5 = Strongly agree), with higher scores on the scale representing higher perceived organisational commitment. The items had acceptable internal consistency (α = 0.79).
Binge drinking and drug use
Binge drinking was classified based on the National Health and Medical Research Council (NHMRC, 2009) alcohol consumption guidelines, which was consuming five or more standard drinks on one occasion. Participants were asked how frequently they binge drink (never, less than monthly, monthly, weekly, daily or almost daily). Participants were also asked whether they had consumed illegal drugs in the 12 months prior to the survey and/or prescription drugs (either not prescribed or used in a non-prescribed manner).
Sleep quality
Two questions were used to assess employees’ sleep quality, adapted from the Pittsburgh Sleep Quality Index (Buysse et al., 1989): the number of hours of sleep they got on average (1 = Less than 5 hours, 7 = More than 9 hours) and how often they sleep well (1 = Almost always, 5 = Almost never). Good-quality sleep was characterised by sleeping well ‘often’ or ‘always’ for 7 or more hours. Sleeping 6 hours or less and sleeping well ‘not often’ or ‘almost never’ represented poor sleep quality in this study.
Analytical approach
Prevalence of suicidal thoughts and comparisons to Australian adults
Rates of suicidal thoughts, plans and attempts were calculated within and across sectors, with data weighted to represent demographic characteristics of the population. Chi-square tests of proportions were conducted to assess whether rates of thoughts and behaviours across sectors were significantly different from rates among the general population identified in the 2007 NSMHWB of Australian adults (ABS, 2007) and also whether there were any differences in terms of age or gender.
Associations with suicidal thoughts and behaviours
Several logistic regressions were performed to determine associations between personal and workplace factors and suicidal thoughts in the past 12 months. Using a sub-sample of employees who indicated suicidal thoughts, two additional regressions were performed to assess which factors were associated with suicide plans and attempts. That is, the first model looked at risk factors for suicidal ideation among all employees, and two further models were fitted looking at risk factors for suicide planning and attempts among those who reported suicidal thoughts in the past 12 months. Due to the lower number of suicide attempts, Firth’s (1993) bias-adjusted estimate of parameters was used. Interquartile odds ratios (ORs) were calculated for continuous predictor variables to allow for comparison with categorical variables and compensate for the scale-dependent characteristic of the statistic (Mackinnon, 1992). Model performance was assessed through the inspection of positive predictive value (PPV), area under curve, sensitivity and specificity statistics, with the probability cut-off for classification of an event set to 0.10. All analyses were conducted using the SAS version 9.4 software through the surveylogistic procedure.
Assessing the impact of participants who skipped suicide questions on regression results
This study groups participants who skipped suicide-related questions as not having suicidal thoughts and behaviours for all analyses to provide conservative estimates. Complementary analyses present suicide rates when excluding these participants and also grouping them with ‘yes’ respondents. Several regressions were performed to assess the sensitivity of the associations between predictors and suicidal thoughts and behaviours to the exclusion of the ‘prefer not to say’ participants from the sample. In addition, regressions were performed when grouping the ‘prefer not to say’ participants with participants endorsing suicidal thoughts in the prior 12 months. However, they were not grouped with participants reporting suicidal behaviours in models predicting suicide plans and attempts. This is due to the significant disparity in rates of behaviours when grouping them with participants who reported suicide plans and attempts, and the low base rates of such behaviours, which may distort associations. Responses were not imputed due to the inherent difficulties in predicting suicidal thoughts and behaviours.
Results
Prevalence of suicidal thoughts and behaviours among emergency personnel
Rates of suicidal thoughts and behaviours among the surveyed emergency personnel are reported in Table 2. Roughly 5.3% (n = 802) of employees indicated experiencing suicidal thoughts in the prior 12 months, while 2.0% (n = 320) reported plans and 0.3% (n = 50) attempted. Lifetime rates were notably higher, with 12.3% (n = 2016) thinking about suicide, 5.7% (n = 943) planning and 1.9% (n = 309) attempting. A total of 8.0% (n = 1117) of employees preferred not to answer suicide-related questions. Excluding these participants did not result in significantly different rates of thoughts and behaviours (Supplementary Table 1). When assuming participants who skipped suicide questions have a history of suicidal thoughts and behaviours, rates were substantially higher (e.g. Suicidal thoughts, plans and attempts in the prior 12 months were 13.3%, 10.7% and 9.3%, respectively).
Proportion and odds of employees indicating suicidal thoughts and/or behaviours by service and demographic factors.
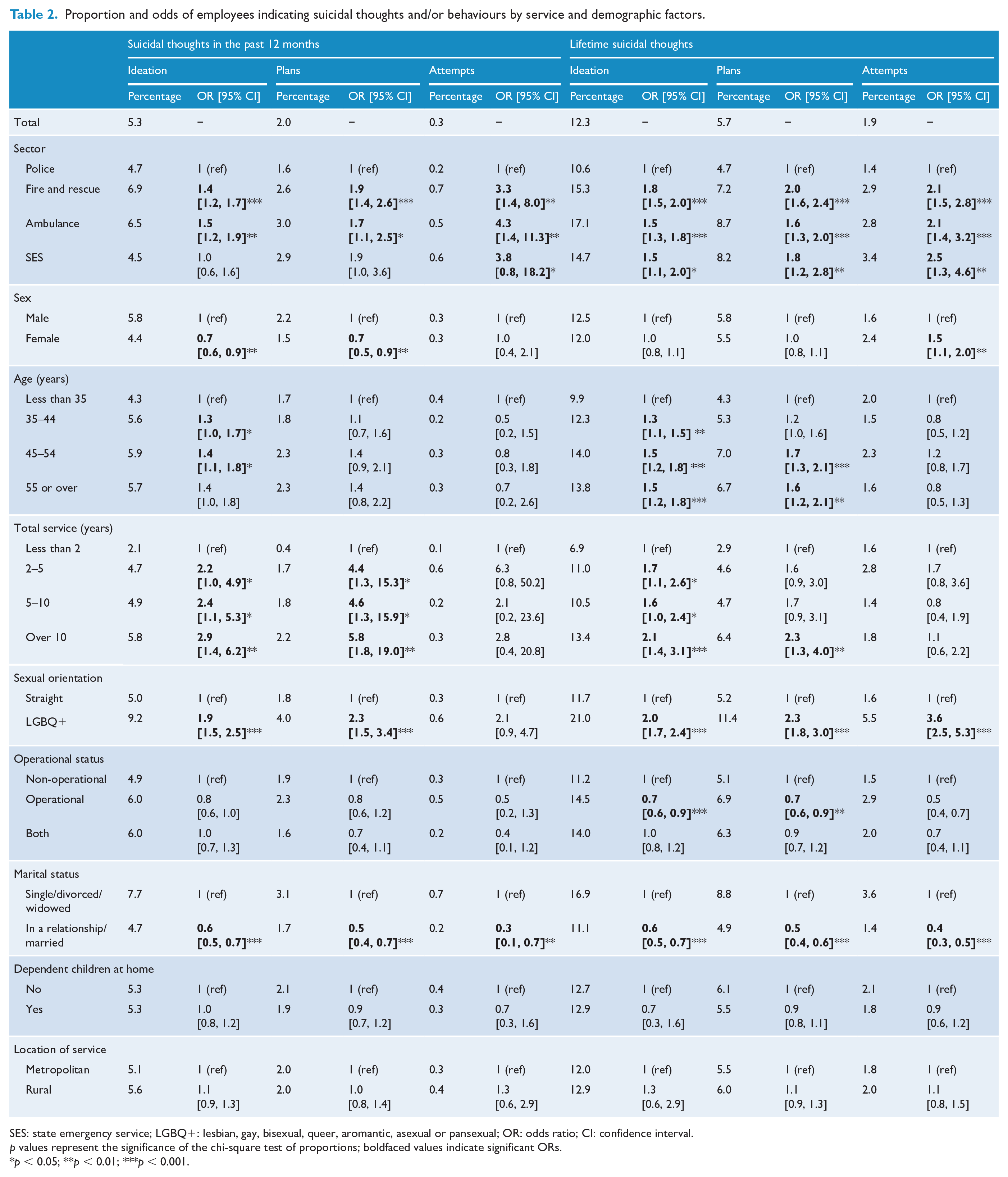
SES: state emergency service; LGBQ+: lesbian, gay, bisexual, queer, aromantic, asexual or pansexual; OR: odds ratio; CI: confidence interval.
p values represent the significance of the chi-square test of proportions; boldfaced values indicate significant ORs.
p < 0.05; **p < 0.01; ***p < 0.001.
Characteristics of employees who preferred not to answer suicide questions
Employees that preferred not to answer suicide questions were more likely to report high psychological distress (62.6%, 95% confidence interval [CI] = [59.0, 66.3]) than employees who reported not thinking about suicide (23.8%, 95% CI = [22.8, 24.8]), and lower rates than employees who reported suicidal thoughts (77.7%, 95% CI = [73.8, 81.4]). They were also more likely to hold high levels of shame regarding their mental health (49.8%, 95% CI = [45.2, 54.5]), compared to 36.7% (95% CI = [33.7, 39.9]) of those who indicated suicidal thoughts and 31.9% (95% CI = [30.0, 33.7]) of those reporting no suicidal thoughts. In addition, they were significantly more likely to perceive stigma from others within the workplace (38.2%, 95% CI = [34.4, 42.0]) compared to those with no suicidal thoughts (23.9%, 95% CI = [22.9, 25.0]). There was no significant difference between occupations or genders, while employees under 35 years of age tended to skip suicide-related questions less often.
Comparisons between emergency services employees and Australian adults
Table 3 presents the rates of suicidal thoughts, plans and attempts among emergency services personnel and Australian adults (ABS, 2007). Emergency services personnel reported significantly higher rates of suicide thoughts, χ2(1, 23,709) = 95.63, p < 0.001, and plans, χ2(1, 23,709) = 69.69, p < 0.001, in the prior 12 months, but not attempts, χ2(1, 23,709) = 2.76, p = 0.097. They also indicated significantly higher rates of suicidal thoughts and plans across all age groups and gender when compared with Australian adults. Australian adults under the age of 35 years reported significantly higher rates of suicide attempts, χ2(1, 23,709) = 6.52, p = 0.012. However, the NSMHWB included a higher proportion of adults under the age of 25, who had higher rates of suicide attempts in that survey. Supplementary Table 2 presents the rates of suicidal thoughts and behaviours among broader age groups (i.e. 25–34 years and 54–65 years), and cross-tabulations between age and gender.
Suicidal thoughts and behaviours among police and emergency services employees in the 12 months prior to the survey, as compared with Australian adults, by age and sex.
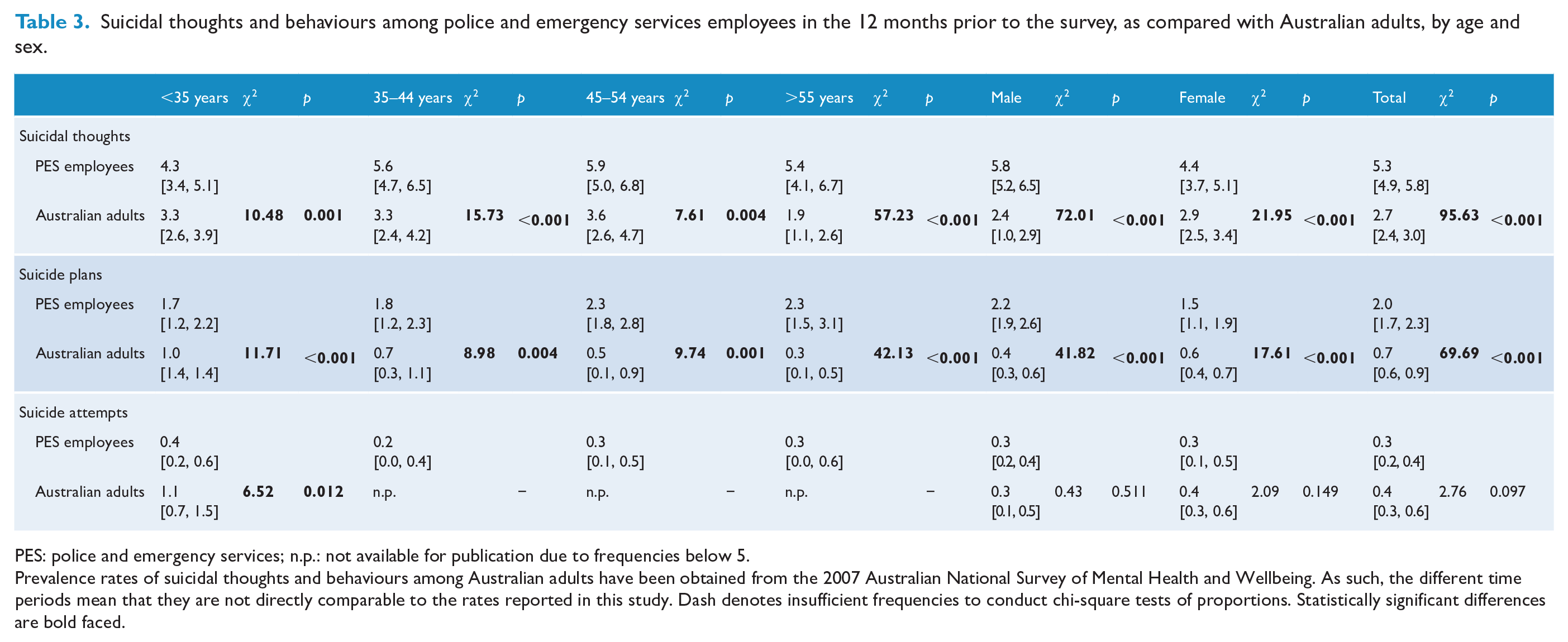
PES: police and emergency services; n.p.: not available for publication due to frequencies below 5.
Prevalence rates of suicidal thoughts and behaviours among Australian adults have been obtained from the 2007 Australian National Survey of Mental Health and Wellbeing. As such, the different time periods mean that they are not directly comparable to the rates reported in this study. Dash denotes insufficient frequencies to conduct chi-square tests of proportions. Statistically significant differences are bold faced.
Prevalence of suicidal thoughts and behaviours: lifetime and in the prior 12 months
Occupation and operational status
Proportions of employees reporting suicidal thoughts and behaviours in each sector are reported in Table 2 and Supplementary Table 3. Police employees had the lowest rates of thoughts and behaviours, while fire and rescue and ambulance personnel reported significantly higher lifetime rates and in the prior 12 months. Employees currently in operational roles were significantly less likely to report lifetime suicidal thoughts (OR = 0.74, 95% CI = [0.64, 0.86], p < 0.001) and plans (OR = 0.73, 95% CI = [0.59, 0.91], p = 0.004) than non-operational employees, while there was no significant difference in the prior 12 months. There was no significant difference in rates between metropolitan and rural services.
Age and length of service
Older employees tended to report marginally higher rates of lifetime suicidal thoughts and plans, and suicidal thoughts in the 12 months prior to the survey. There was a stepwise increase in suicidal thoughts and behaviours in the prior 12 months by the length of service, with 5.8% (OR = 2.94, 95% CI = [1.39, 6.22], p = 0.004) of employees serving over 10 years reporting suicidal thoughts, compared to only 2.1% of employees serving less than 2 years. Longer service was also associated with higher rates of lifetime suicidal thoughts and plans. There was no significant association between length of service and lifetime suicide attempts.
Gender and sexual orientation
Female employees reported significantly lower rates of suicidal thoughts (OR = 0.75, 95% CI = [0.61, 0.91], p = 0.005) and plans (OR = 0.66, 95% CI = [0.48, 0.90], p = 0.010), but not attempts (OR = 0.95, 95% CI = [0.44, 2.06], p = 0.897) in the prior 12 months. Furthermore, there was no significant difference between genders in rates of lifetime thoughts and plans. Female employees reported higher rates of lifetime suicide attempts when compared with male employees (OR = 1.50, 95% CI = [1.11, 2.02], p = 0.008). Compared to employees with heterosexual orientation, non-heterosexual employees (i.e. lesbian, gay, bisexual, queer, aromantic, asexual or pansexual [LGBQ+]) reported higher rates of lifetime suicidal thoughts, plans and attempts, and higher rates of thoughts and plans in the 12 months prior to the survey.
Marital status and children
Employees who were not in a relationship reported significantly higher rates of lifetime suicidal thoughts and behaviours and in the 12 months prior to the survey. Having dependent children at home was not associated with significantly different rates of suicidal thoughts and behaviours.
Prevalence of suicidal thoughts and behaviours in the prior 12 months in each occupation
Table 4 presents the rates of suicidal thoughts and behaviours for each sector in the past 12 months, across a range of demographic factors. Non-heterosexual employees consistently reported higher rates of suicidal thoughts and behaviours in each occupation. Employees that were not in relationships were more likely to report suicidal thoughts and behaviours in each occupation.
Rates and odds [95% CI] of suicidal thoughts and behaviours in the past 12 months by employees in each sector, by demographic and work characteristics.
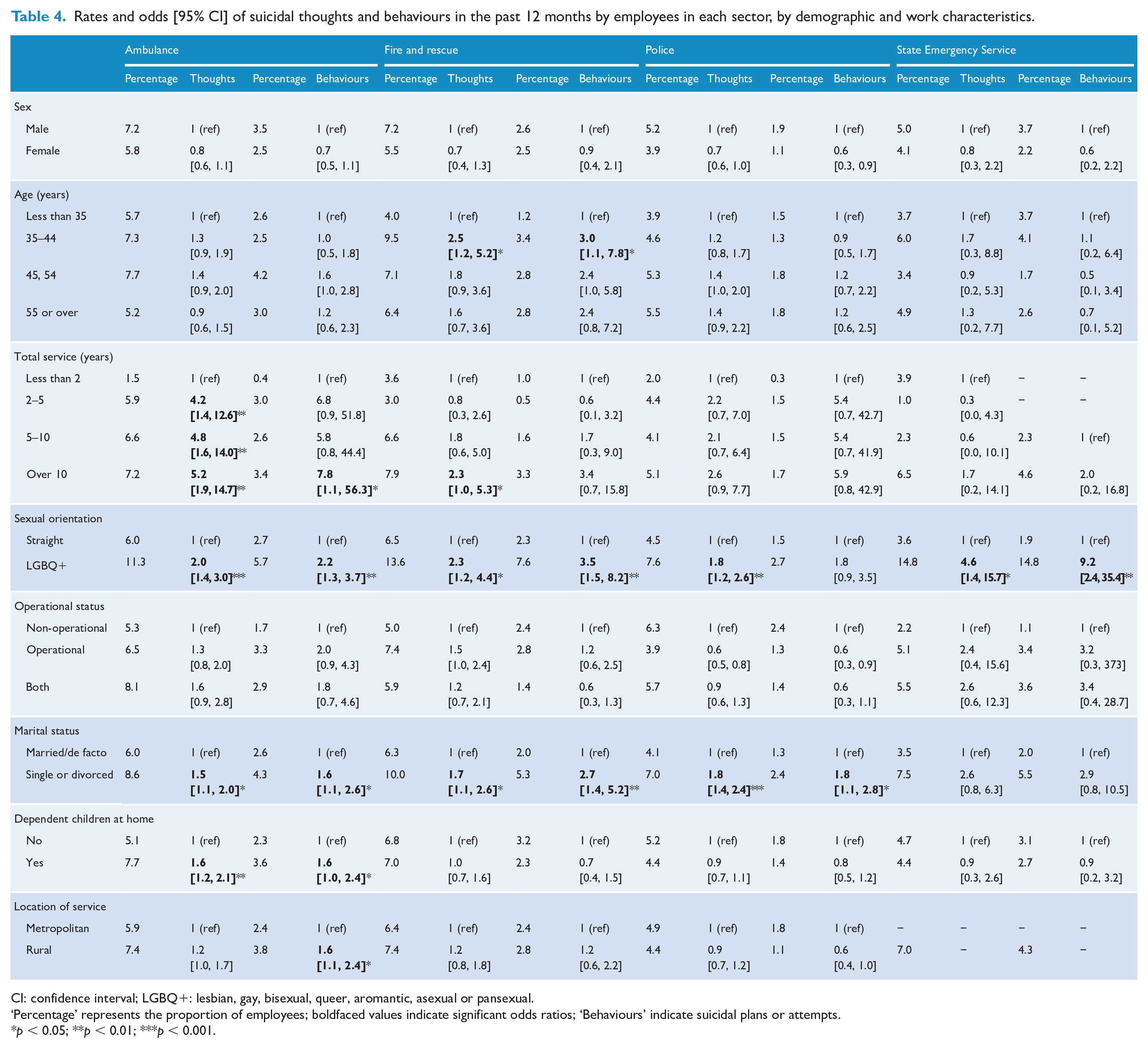
CI: confidence interval; LGBQ+: lesbian, gay, bisexual, queer, aromantic, asexual or pansexual.
‘Percentage’ represents the proportion of employees; boldfaced values indicate significant odds ratios; ‘Behaviours’ indicate suicidal plans or attempts.
p < 0.05; **p < 0.01; ***p < 0.001.
Factors associated with suicidal thoughts and behaviours
Workplace factors
Multivariate logistic regressions were performed to assess how workplace factors were associated with suicidal thoughts and behaviours in the prior 12 months (Table 5). Higher rates of bullying (OR = 1.38, 95% CI = [1.22, 1.57], p < 0.001), perceived stigma (OR = 1.24, 95% CI = [1.12, 1.28], p < 0.001), work/family conflict (OR = 1.79, 95% CI = [1.58, 2.02], p < 0.001) and low meaning of work (OR = 1.31, 95% CI = [1.16, 1.48], p < 0.001) were associated with higher rates of suicidal thoughts. Among employees reporting suicidal thoughts, only more stressful and frequent bullying was significantly associated with suicide plans (OR = 1.46, 95% CI = [1.15, 1.86], p < 0.001) and attempts (OR = 1.68, 95% CI = [1.06, 2.65], p = 0.012). Tolerance of predictors was above 0.4 and variance inflation factor (VIF) coefficients were below 2.4 in both samples, indicating acceptably low multicollinearity (Hair et al., 2010).
Multivariate associations between workplace factors, suicidal thoughts in the past 12 months and the transition from thoughts to behaviours.
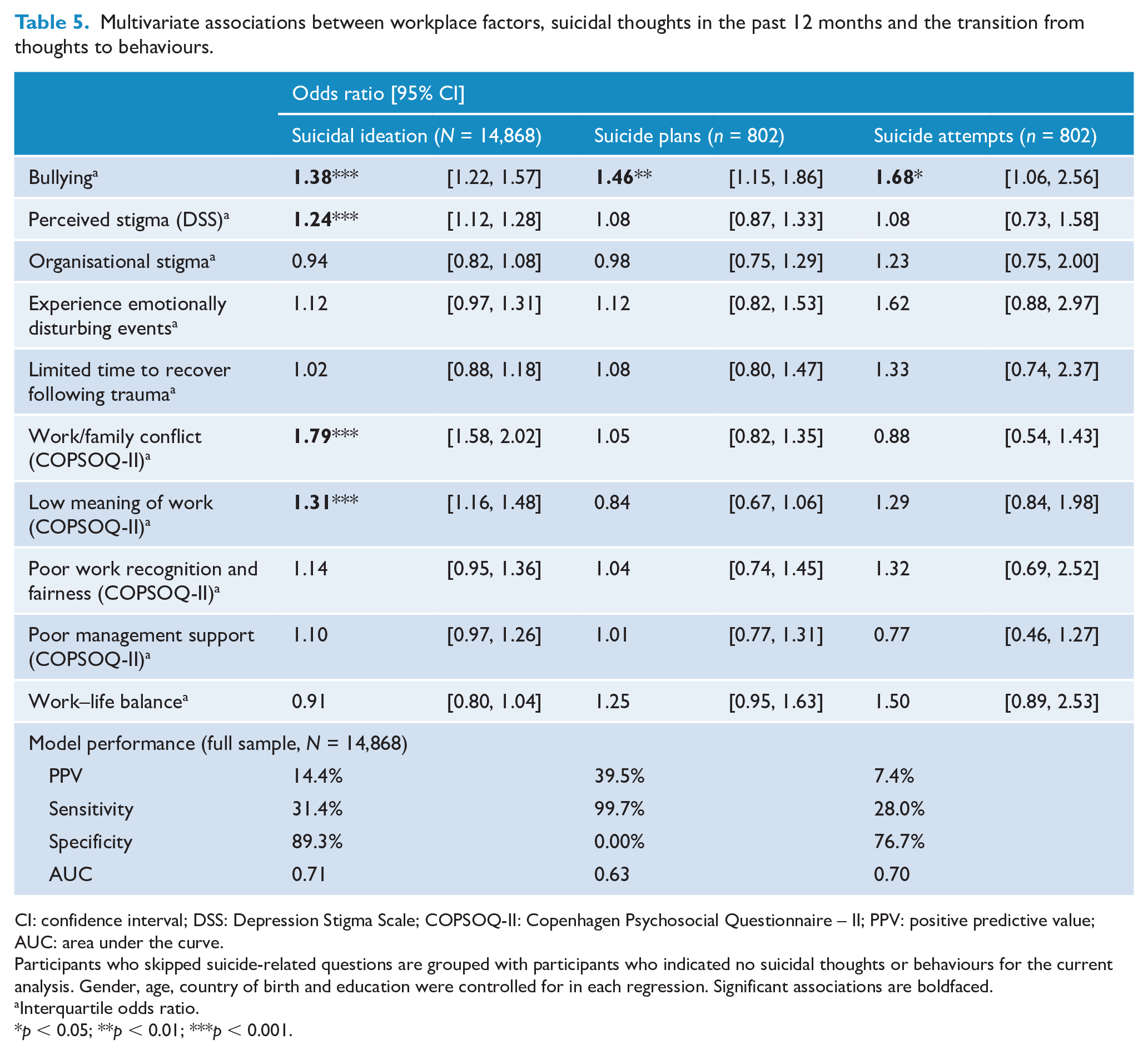
CI: confidence interval; DSS: Depression Stigma Scale; COPSOQ-II: Copenhagen Psychosocial Questionnaire – II; PPV: positive predictive value; AUC: area under the curve.
Participants who skipped suicide-related questions are grouped with participants who indicated no suicidal thoughts or behaviours for the current analysis. Gender, age, country of birth and education were controlled for in each regression. Significant associations are boldfaced.
Interquartile odds ratio.
p < 0.05; **p < 0.01; ***p < 0.001.
Personal factors
Receiving social support (OR = 0.61, 95% CI = [0.54, 0.70], p < 0.001) and perceived resilience (OR = 0.62, 95% CI = [0.40, 0.94], p = 0.025) were associated with lower suicidal ideation, with higher psychological distress (OR = 2.02, 95% CI = [1.75, 2.34], p < 0.001) and PTSD symptoms (OR = 1.50, 95% CI = [1.32, 1.70], p < 0.001) being associated with higher rates of suicidal thoughts in the prior 12 months (Table 6). High intermittent explosive anger (OR = 1.35, 95% CI = [1.07, 1.68], p = 0.010), illegal drug use (OR = 2.36, 95% CI = [1.66, 3.35], p < 0.001) and prescription drug misuse (OR = 1.83, 95% CI = [1.36, 2.39], p < 0.001) were also significantly associated with increased rates of suicidal ideation. Among a sub-sample reporting suicidal thoughts, a higher number of PTSD symptoms was associated with higher rates of suicide plans (OR = 1.33, 95% CI = [1.05, 1.69], p = 0.018), while higher psychological distress (OR = 2.70 95% CI = [1.64, 4.45], p < 0.001) and prescription drug misuse (OR = 2.63, 95% CI = [1.24, 5.59], p = 0.012) were significantly associated with suicide attempts. Supplementary Tables 4 and 5 present the associations with plans and attempts among the full sample of employees, and Supplementary Table 6 presents the correlations between predictors. Tolerance of predictors in each model was above 0.3 and VIF below 3.3.
Multivariate associations between personal psychological factors, suicidal thoughts in the past 12 months and the transition from thoughts to behaviours.
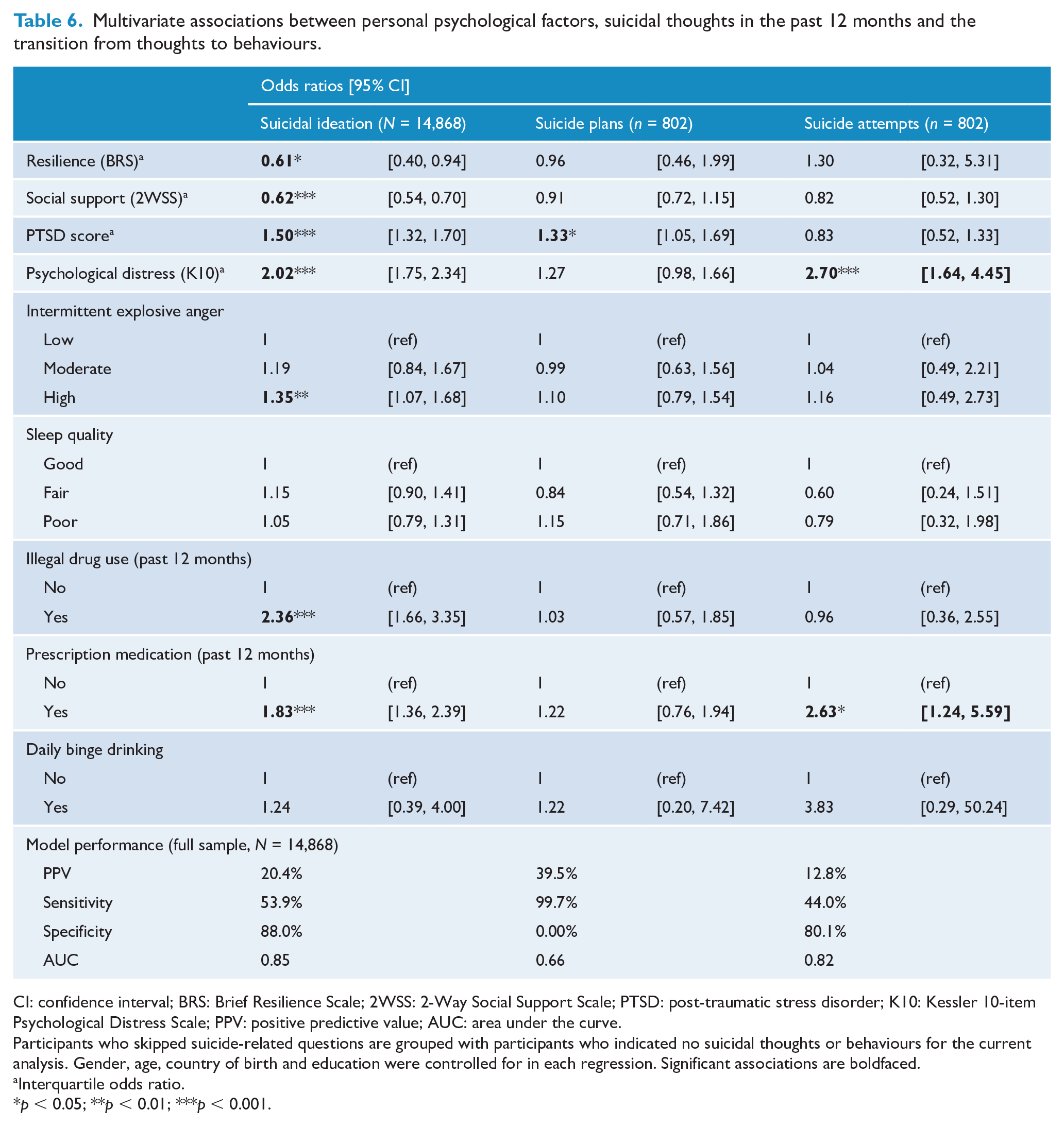
CI: confidence interval; BRS: Brief Resilience Scale; 2WSS: 2-Way Social Support Scale; PTSD: post-traumatic stress disorder; K10: Kessler 10-item Psychological Distress Scale; PPV: positive predictive value; AUC: area under the curve.
Participants who skipped suicide-related questions are grouped with participants who indicated no suicidal thoughts or behaviours for the current analysis. Gender, age, country of birth and education were controlled for in each regression. Significant associations are boldfaced.
Interquartile odds ratio.
p < 0.05; **p < 0.01; ***p < 0.001.
Impact of employees who skipped suicide-related questions on regression results
Excluding employees who skipped suicide-related questions from the analyses did not result in significantly different associations with suicidal thoughts, plans and attempts and model performance. When grouping them with participants who reported suicidal thoughts, however, daily binge drinking (OR = 3.65, 95% CI = [1.78, 7.48], p < 0.001) and perceived organisational commitment (OR = 0.82, 95% CI = [0.75, 0.90], p < 0.001) became significantly associated with suicidal thoughts in the prior 12 months.
Model performance
Model performance with only workplace factors was poor, with PPV and sensitivity being low when predicting suicidal thoughts and behaviours (Tables 5 and 6). On the other hand, the model with mental health and substance use factors was associated with significantly higher PPV and sensitivity, indicating improved model performance. However, a large portion of incidents were not detected by the models, indicating that other factors may be important in determining suicide risk. For instance, 44.0% of suicide attempts in the prior 12 months were detected through the model based on personal factors, and roughly 87.2% of the time produced false positives.
Discussion
This study presents the most comprehensive assessment of suicidal thoughts and behaviours among Australian police and emergency services personnel to date. Rates of suicidal thoughts and plans were higher than those of the Australian adult population, while rates of attempts were too low to allow for a decisive conclusion. Across the four sectors assessed in this study, police employees reported the lowest rates of suicidal thoughts and behaviours. This is consistent with findings from prior research which identified police as having lower rates of suicidal thoughts and behaviours than other emergency and non-emergency occupations (Carleton et al., 2018; Loo, 2003; Milner et al., 2017). Particular experiences within sectors and the way their workplaces operate may act as protective factors against suicide, such as camaraderie between police officers, and specific experiences relating to suicide while on duty (i.e. breaking news to family members of an individual who completed suicide). Indeed, Mercy et al. (2001) found that exposure to suicidal behaviour of a friend/acquaintance was associated with lower rates of suicide attempts in the general population. Further research is needed to explore protective elements of working as a police officer that could be translated to other populations.
Consistent with prior research, this study found that symptoms of PTSD and psychological distress had a strong association with suicidal thoughts and also significantly differentiated which employees acted on their suicidal thoughts (Violanti, 2004). These findings build on Sterud et al. (2008), who found symptoms of depression and anxiety to be associated with higher levels of suicidal ideation. According to prominent escape theories, suicidal ideation may potentially represent a desire to escape from distressing thoughts and feelings, albeit maladaptive (Baumeister, 1990). Other behaviours such as alcohol and drug use may also alleviate feelings of distress and could account for the significant relationship with suicidal thoughts and behaviours in the current study (Tiffany, 1990).
The current study identified a variety of workplace factors associated with suicidal thoughts and behaviours. Consistent with Sterud et al. (2008), this study found bullying to be associated with higher rates of suicidal thoughts and behaviours, while negative impacts of work on one’s private life were associated with higher rates of suicidal thoughts only. Building on these findings, individuals who perceived high levels of stigma within their working environment were more likely to think about suicide. Those who perceive stigma may be less likely to seek help from others, and rely on maladaptive coping mechanisms, such as desiring suicide (Baumeister, 1990; Nock and Prinstein, 2004). Predictive models based on workplace factors were, however, relatively poor in detecting who acted on their suicidal thoughts. Therefore, individual differences in responses to stressful working environments may still remain important.
Examination of demographic variables revealed several characteristics associated with suicidal thoughts and behaviours. Consistent with prior research, employees in relationships reported lower rates of suicidal thoughts and behaviours and likely reflect the positive impact of social support away from the workplace (Carleton et al., 2018; Sterud et al., 2008). Further supporting prior research, there was no significant difference in lifetime suicidal thoughts between males and females, although the higher rate of thoughts and plans in the prior year among male employees contrasts with Sterud et al. (2008). Employees with an LGBQ+ sexual orientation reported notably high rates of lifetime and recent suicidal thoughts and behaviours than heterosexual employees, which is consistent with findings from wider populations (Hass et al., 2010). This suggests that certain personnel may be in particular need of mental health services and support.
An important finding from this study is that employees who preferred not to answer suicide-related questions held higher rates of shame regarding mental health issues, consistent with findings from studies of other high-risk populations (Podlogar and Joiner, 2020). This may represent an unwillingness to speak to others regarding their own mental health issues and inhibits adaptive help-seeking behaviours (Rüsch et al., 2014). They were more likely to perceive stigma from others, which is consistent with findings from Hom et al. (2016), who found that stigma-related issues were significant barriers to care among firefighters with suicidal thoughts and behaviours. Reducing the stigma surrounding mental health may therefore be an effective target for interventions.
Limitations and directions for future research
A limitation of this study is that it was a cross-sectional survey. Although it allowed for a comprehensive assessment of a variety of mental health and workplace factors, it prevents the identification of causal relationships. Thus, it is difficult to determine whether workplace factors cause distress, or whether an employee perceives greater adversity in the workplace as a symptom of a mental health condition. Longitudinal research may assist in identifying factors associated with short-term fluctuations in suicidal thoughts and behaviours (Ben-Zeev et al., 2012; Kyron et al., 2018) and also in identifying employees with pervasive mental health issues at risk of self-injury (Czyz and King, 2015; Kyron et al., 2019 Restifo et al., 2015). Understanding how symptoms change over time may assist in enhancing the prediction of which employees are at risk of suicide and also which factors could be targeted during interventions. Another limitation of this study is the differing periods in which risk factors and outcomes were assessed. For instance, the PTSD scale measured symptoms in the prior 4 weeks, while suicide-related questions asked about thoughts and behaviours in the prior 12 months or at any stage in the individual’s life. It is therefore difficult to determine whether risk factors temporally precede the development of suicidal thoughts and behaviours.
It is important for future research to simultaneously assess factors distally related to mental health outcomes and those proximally related (Stuart, 2008). Personality characteristics may predispose an individual to experience heightened negative affect following stressful incidents (Mroczek and Almeida, 2004) and be associated with higher workplace stress and suicidal ideation in emergency personnel (Pienaar et al., 2007; Sterud et al., 2008). Furthermore, emergency personnel may have higher pain tolerance and a reduced fear of death, which lends itself to attempting suicide (Chu et al., 2016). Further research is needed to explore these domains.
Conclusion
This study looked to address the shortage of studies assessing suicidal thoughts and behaviours among emergency personnel, particularly within an Australian context. Poorer mental health and some aspects of the working environment were associated with higher rates of suicidal thoughts and behaviours. Therefore, there are various pathways to improve outcomes during workplace interventions. The growing amount of research into the mental health of emergency personnel has allowed for a more cohesive picture of contributing factors. However, given the high prevalence of mental health conditions among emergency personnel and the stressful nature of jobs in the sector, attention should be focussed on building working environments and cultures that promote mental health and wellbeing.
Supplemental Material
Supplementary_information – Supplemental material for Prevalence and predictors of suicidal thoughts and behaviours among Australian police and emergency services employees
Supplemental material, Supplementary_information for Prevalence and predictors of suicidal thoughts and behaviours among Australian police and emergency services employees by Michael J Kyron, Wavne Rikkers, Andrew C Page, Patrice O’Brien, Jennifer Bartlett, Anthony LaMontagne and David Lawrence in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_material – Supplemental material for Prevalence and predictors of suicidal thoughts and behaviours among Australian police and emergency services employees
Supplemental material, Supplementary_material for Prevalence and predictors of suicidal thoughts and behaviours among Australian police and emergency services employees by Michael J Kyron, Wavne Rikkers, Andrew C Page, Patrice O’Brien, Jennifer Bartlett, Anthony LaMontagne and David Lawrence in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_Table – Supplemental material for Prevalence and predictors of suicidal thoughts and behaviours among Australian police and emergency services employees
Supplemental material, Supplementary_Table for Prevalence and predictors of suicidal thoughts and behaviours among Australian police and emergency services employees by Michael J Kyron, Wavne Rikkers, Andrew C Page, Patrice O’Brien, Jennifer Bartlett, Anthony LaMontagne and David Lawrence in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_Table_1 – Supplemental material for Prevalence and predictors of suicidal thoughts and behaviours among Australian police and emergency services employees
Supplemental material, Supplementary_Table_1 for Prevalence and predictors of suicidal thoughts and behaviours among Australian police and emergency services employees by Michael J Kyron, Wavne Rikkers, Andrew C Page, Patrice O’Brien, Jennifer Bartlett, Anthony LaMontagne and David Lawrence in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The current research was conducted by The University of Western Australia in partnership with Roy Morgan Research on behalf of Beyond Blue, and their help has been greatly appreciated. The authors acknowledge and appreciate the participation of the individual agencies and people who work in police and emergency services who contributed to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by Beyond Blue and the Bushfire and Natural Hazards Cooperative Research Centre.
Ethical Approval
All procedures were approved by The University of Western Australia Human Research Ethics Committee, The Sydney Local Health District Ethics Review Committee, Tasmanian Health and Medical Human Research Ethics Committee, Ambulance Victoria Research Committee, Victoria Police Human Research Ethics Committee and St John Ambulance Western Australia Research Advisory Group.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.