
Abstract
Objectives:
Protests, riots and revolutions have long been a part of human history and are increasing globally, yet their impact on mental health remains largely unknown. We therefore systematically reviewed studies on collective actions and mental health.
Method:
We searched PubMed, Web of Science, PsycINFO and CINAHL Plus for published studies from their inception until 1 January 2018. Study quality was rated using the Newcastle–Ottawa Scale.
Results:
We identified 52 studies (n = 57,487 participants) from 20 countries/regions. The prevalence of post-traumatic stress disorder ranged from 4% to 41% in riot-affected areas. Following a major protest, the prevalence of probable major depression increased by 7%, regardless of personal involvement in the protests, suggestive of community spillover effects. Risk factors for poorer mental health included female sex, lower socioeconomic status, exposure to violence, interpersonal conflicts, frequent social media use and lower resilience and social support. Nevertheless, two studies suggested that collective actions may reduce depression and suicide, possibly due to a collective cathartic experience and greater social cohesion within subpopulations.
Conclusion:
We present the first systematic review of collective actions and mental health, showing compelling evidence that protests even when nonviolent can be associated with adverse mental health outcomes. Health care professionals therefore need to be vigilant to the mental and psychological sequelae of protests, riots and revolutions. Further research on this emerging sociopolitical determinant of mental health is warranted.
Keywords
Background
In the past few decades, collective actions such as protests, riots and revolutions (Tarrow, 2011) have taken place in over 180 countries, accounting for 99% of the world’s population (Banks and Wilson, 2017) (Figure 1). They continue to increase globally (Ortiz et al., 2013; Stephan and Chenoweth, 2008), yet the mental health consequences of collective actions remain largely unknown. By contrast, the mental health impact of other large-scale population events such as natural disasters, human-made disasters, terrorist attacks and armed conflicts have been much better documented (Charlson et al., 2019; Galea et al., 2005; Galea and Maxwell, 2009; Goldmann and Galea, 2014; Norris et al., 2002a; North, 2014; North and Pfefferbaum, 2002; Perlman et al., 2011). These studies indicate significant levels of both psychopathology and resiliency in the face of mass community trauma, but the relevance of collective actions to health care professionals remains unclear. As the nature of collective actions differs from other major population events, a separate field of inquiry is needed. We therefore systematically reviewed studies on collective actions and mental health around the world.
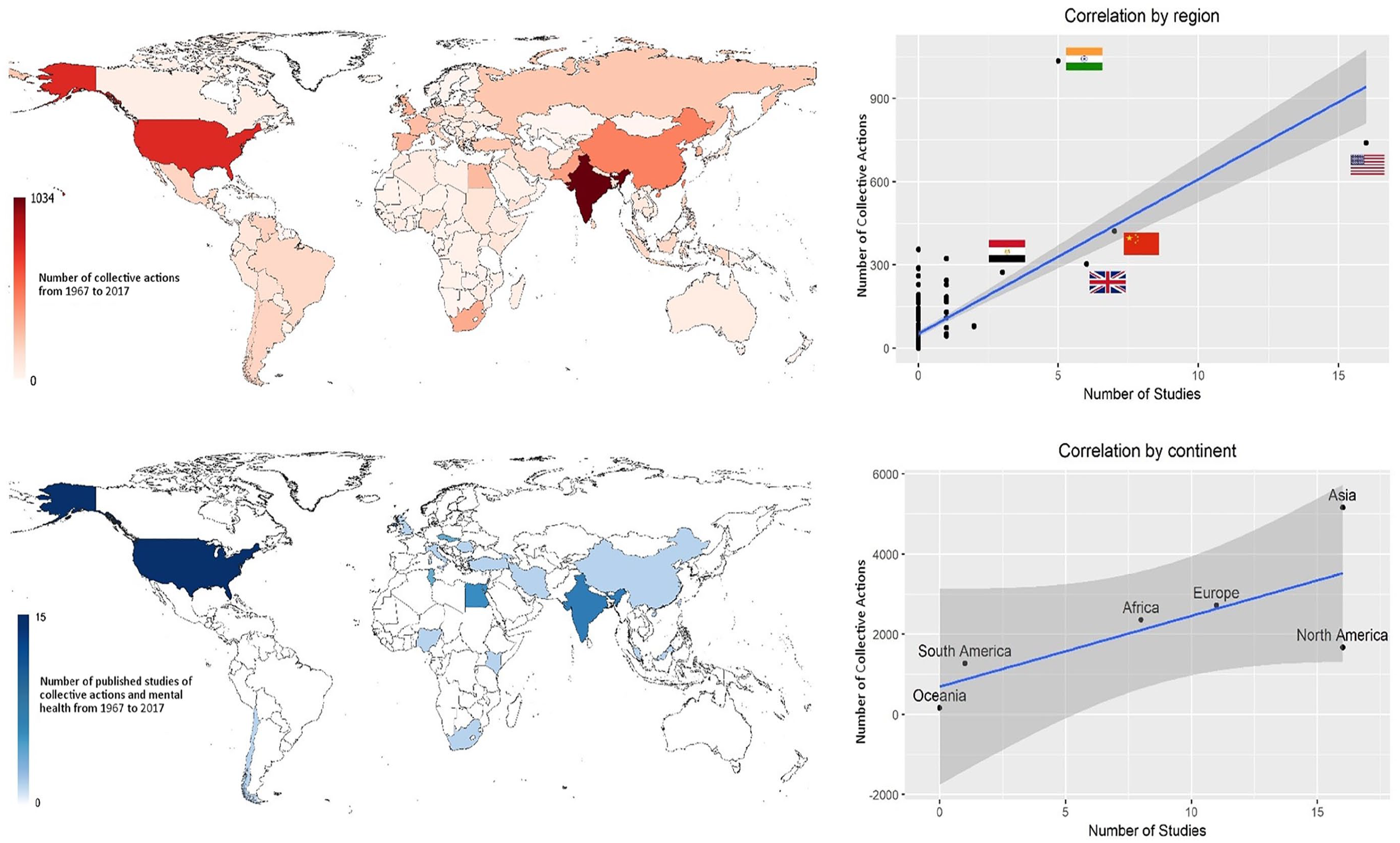
Number of collective actions from 1967 to 2017 (upper panel), number of published studies of collective actions and mental health from 1967 to 2017 (lower panel) and correlation between the number of collective actions and the number of published studies (right panels). Data source for the number of collective actions: Banks and Wilson (2017).
Methods
Search strategy and selection criteria
We pre-specified our methods in a study protocol registered in PROSPERO (PROSPERO 2015:CRD42015029732), and followed the Preferred Reporting Items for a Systematic Review and Meta-analysis (PRISMA) guidelines (Liberati et al., 2009). We included studies reported in English and published in peer-reviewed journals. Studies of all designs, qualitative and quantitative, cross-sectional and longitudinal, were included.
The inclusion criterion for the outcome was that the study measured mental health, either by reporting psychiatric diagnoses, admissions, prescriptions, symptoms or distress of individuals who were directly or indirectly influenced by an identified collective action. We excluded studies based on labour disputes as these aimed to change the distribution of resources or roles within an organisation. Incidents that involved prolonged, paramilitary conflicts organised by states or state-like actors were also excluded.
PubMed, Web of Science, PsycINFO and CINAHL Plus were searched for studies published from the inception of each database until 1 January 2018. Reference lists of retrieved articles were reviewed to identify additional studies. Terms that capture diverse types of collective action, such as ‘protest’, ‘civil disorders’, ‘demonstration’, ‘revolution’ or ‘campaign’ were searched, along with social movements employing collective actions as a tool, using ‘social movement’, ‘political movement’ and ‘socio-political movement’. These were used in combination with terms such as ‘mental health’, ‘mental disorders’, ‘behavioral symptoms’ and ‘psychological’ to identify potential articles addressing collective action and mental health outcomes. An example of the detailed search strategy is presented in Table 1.
Electronic search strategy for PubMed.
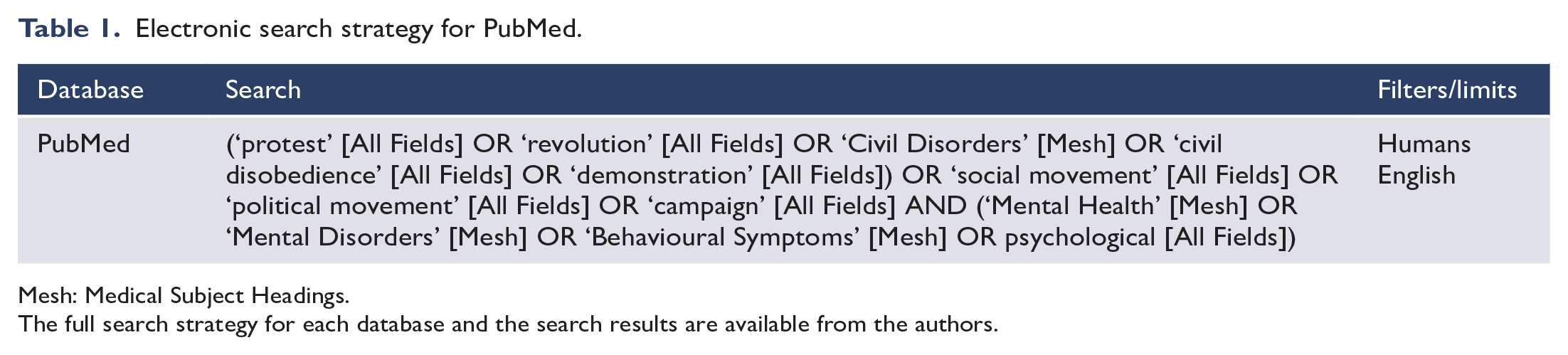
Mesh: Medical Subject Headings.
The full search strategy for each database and the search results are available from the authors.
Once studies were retrieved, two authors independently screened the articles to be included and any disagreement was resolved by consensus. Titles were examined in the first round and abstracts in the second round of screening to determine whether the articles met the inclusion criteria. After the first two rounds of screening, full texts of articles were carefully assessed, and those that met the exclusion criteria were removed.
Two authors constructed a data extraction form, and the first and second author independently completed the form for all included studies. For each article, location, date and duration, type of the collective action, level of violence (death, looting, arson, gun and tear gas use), study design, study population, sampling methods, sample size, analytic methods, exposure and outcome measurement, social support, media exposure, resilience and funding information were extracted.
Evidence grading
Three authors independently rated the methodological quality of all included studies using the Newcastle–Ottawa Scale (NOS), which is recommended by the Cochrane collaboration for the appraisal of non-randomised studies (Higgins and Green, 2012a). The NOS was modified for the quality assessment of cross-sectional studies with reference to previous adaptations (Anglin et al., 2013; Patra et al., 2015).
Synthesis of results
Findings were summarised by mental health outcomes. In accordance with recommendations for systematic reviews, we focused first on findings from longitudinal studies and when none were available then cross-sectional studies with high NOS scores were reviewed (JAMA, 2018). When assessing the prevalence of mental health outcomes, we prioritised findings based on random samples drawn from the general population.
Results
Description of studies
The initial search yielded 18,181 articles. After applying the inclusion and exclusion criteria and searching the reference lists of included studies, we identified a total of 52 studies (Figure 2). These included 6 longitudinal, 8 time series, 3 serial cross-sectional, 22 cross-sectional, 8 case series and 5 qualitative studies, involving a total of 57,487 participants (excluding time series and qualitative studies that did not specify sample size). In total, our review identified reports from 20 countries/regions, including the United States (16 studies), Hong Kong SAR (six), India (five), Northern Ireland (five), Egypt (three), Czechoslovakia (two), Tunisia (two) and one each from Chile, China, Georgia, Iran, Israel, Italy, Kenya, Malaysia, Nigeria, Romania, South Africa, Turkey and the United Kingdom (Figure 1). The Spearman correlation coefficients between the number of collective actions and the number of published studies from 1967 to 2017 were 0.40 (p < 0.001) by region and 0.75 (p = 0.08) by continent (Figure 1). Half of the studies covered riots, 14 were on protests and 9 studied revolutions. The collective actions ranged in time from the 1965 Watts riots to the 2015 Baltimore Protests. Tables 1–3 and Supplemental Tables S1–S4 summarise the study designs and main findings from five decades of research.
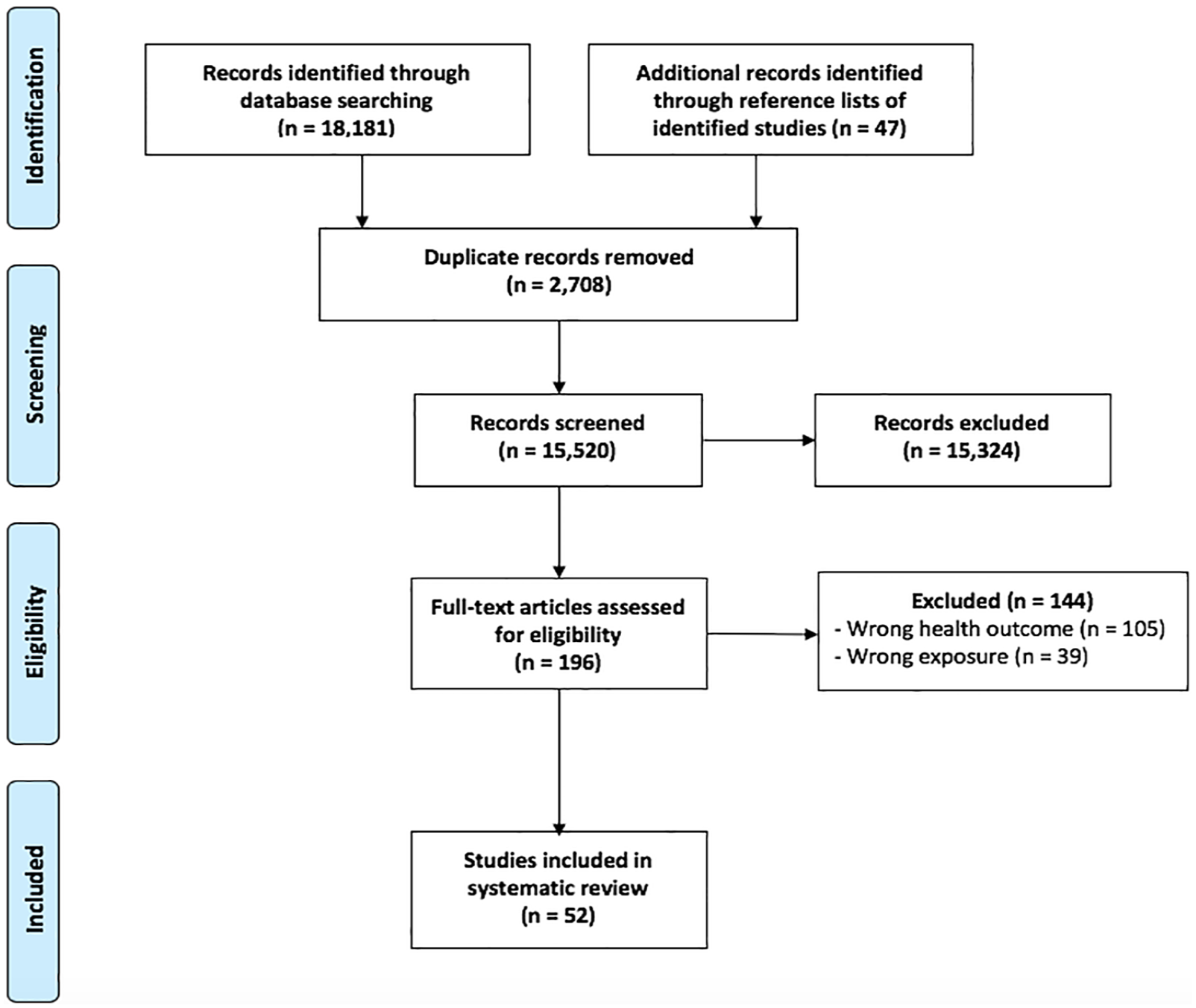
PRISMA flow diagram for studies on collective actions and mental health.
Sample characteristics
Thirteen studies used random samples, some drawn from the general population (Hou et al., 2015; Lau et al., 2016, 2017; Ni et al., 2016, 2017), others by sex (Kubicka et al., 1995, 1998), from health facilities (Bamrah et al., 2013), schools (Castillo-Carniglia et al., 2017), or affected communities (Greenley et al., 1975; Hanson et al., 1995; Obilom and Thacher, 2008; Sasao and Chun, 1994). Sample sizes ranged from 5 to 37,319 (median 343). The majority of studies (n = 36) were conducted after the collective action, while seven started before the collective action (Brown et al., 1994; Fraser, 1971; Garbarino et al., 2012; Klee and Gorwitz, 1970; Kubicka et al., 1995, 1998; Lyons, 1972), and six studies included assessments before, during and after the collective action (Castillo-Carniglia et al., 2017; Fishbain et al., 1991; Greenley et al., 1975; Ni et al., 2016, 2017; Yimgang et al., 2017).
Assessment of mental health outcomes
Depressive sequelae were the most frequently assessed outcome, recorded in a third (n = 18) of all studies, followed by post-traumatic stress disorder (PTSD) (n = 11) and anxiety disorder/anxiety symptoms (n = 11). Other outcomes included psychiatric admissions and prescriptions, psychological distress, substance abuse and suicide (Table 2).
Published studies on collective actions and mental health.
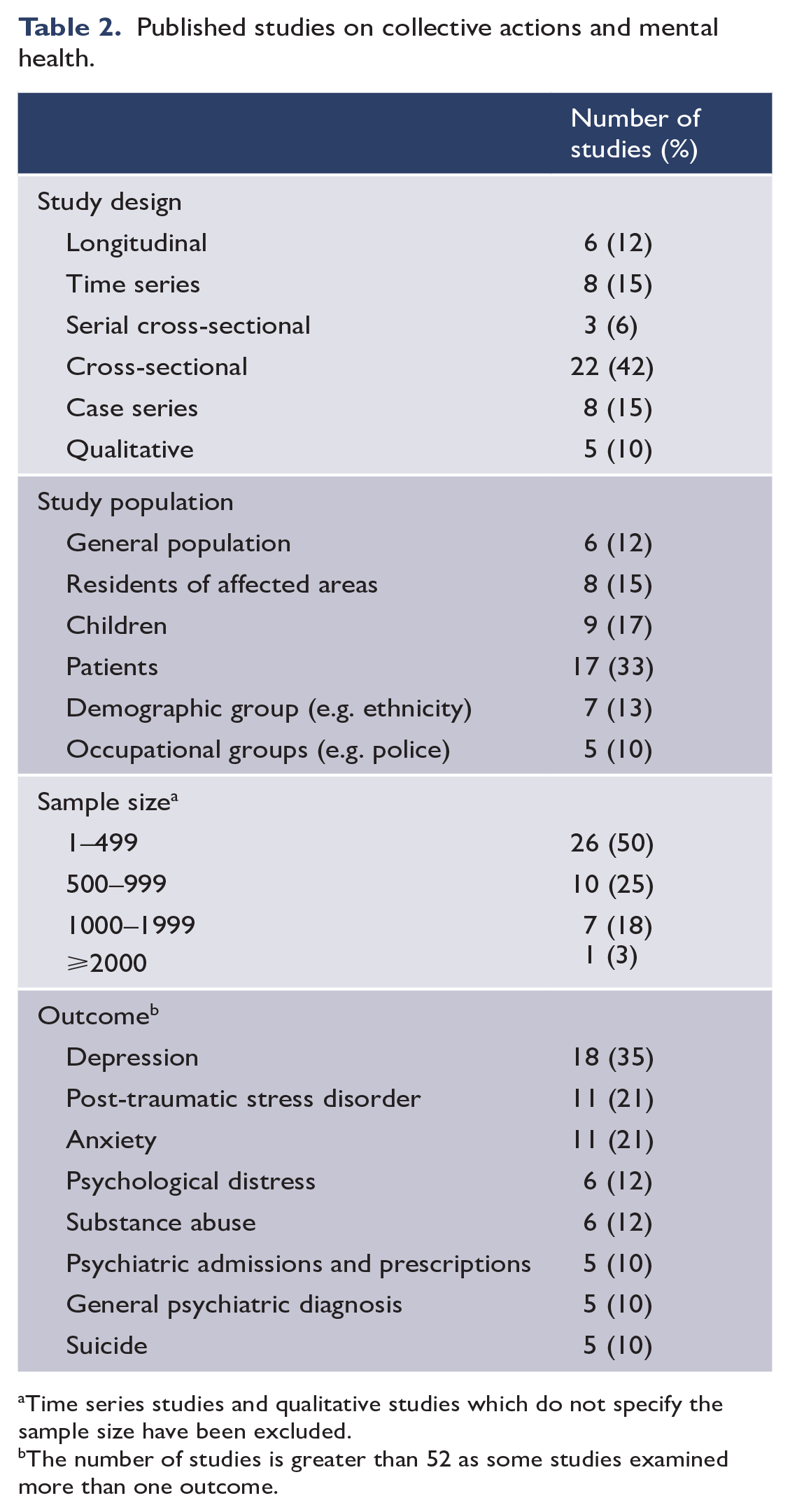
Time series studies and qualitative studies which do not specify the sample size have been excluded.
The number of studies is greater than 52 as some studies examined more than one outcome.
Depressive sequelae
Prevalence
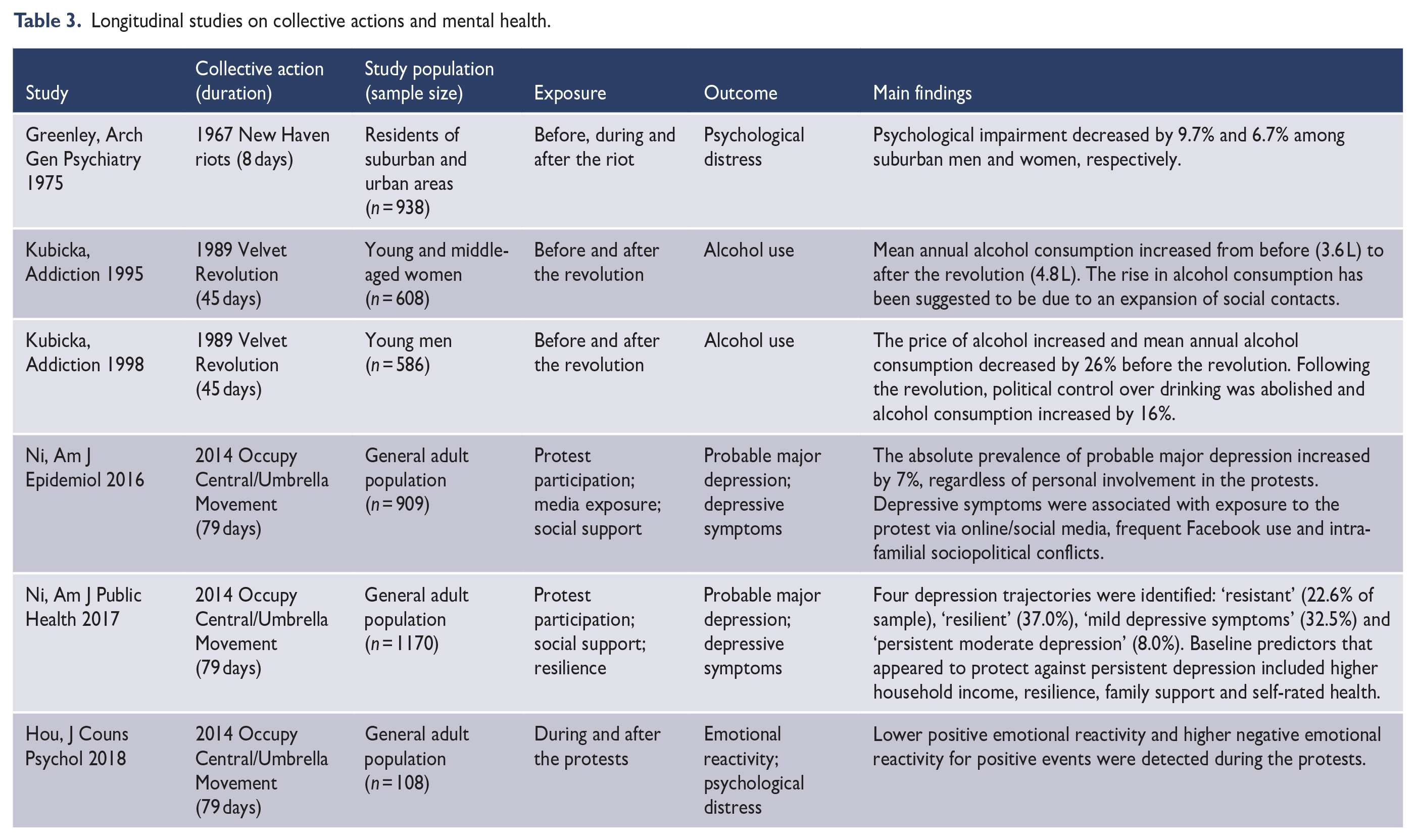
Five studies (Hou et al., 2015; Lau et al., 2016, 2017; Ni et al., 2016, 2017) used probability samples in the general population to assess the prevalence of depression following a collective action. However, all of these studies focused on Hong Kong’s 2014 Occupy Central/Umbrella Movement. Using pre-event data from a population-representative cohort, the prevalence of probable major depression was 1.5% before the Occupy Central/Umbrella Movement. Following the Movement, the prevalence increased to 6.7% (first month), 6.3% (second month), 6.8% (third month) and 8.5% (sixth month) (Ni et al., 2016) (Table 3). Based on the same cohort, four depression trajectories were identified before, during and 1 year after the Occupy Central/Umbrella Movement: ‘resistant’ (22.6% of sample), ‘resilient’ (37.0%), ‘mild depressive symptoms’ (32.5%) and ‘persistent moderate depression’ (8.0%) (Ni et al., 2017). These findings contrast studies from Northern Ireland. Findings based on three districts with varying degrees of exposure to the 1969 Northern Ireland riots found no differences in anti-depressant prescriptions (Fraser, 1971), and indeed a decline in health care utilisation for depression (Lyons, 1972).
Longitudinal studies on collective actions and mental health.
Correlates of depressive sequelae
The negative impact of exposure to collective action appears to vary with the level of violence. For collective actions associated with fatalities, proximity to violence was an important predictor for depression. During the 2011 Arab Spring, the prevalence of depression among children in schools closer to Tahrir Square (a focal point of the revolution) was 62% (Moussa et al., 2015). Living in riot-affected areas was also associated with depression risk (Coudreaut et al., 1995; Fraser, 1971; Tan and Simons, 1973; Yimgang et al., 2017). By contrast, participation in nonviolent collective actions was not associated with depressive sequelae (Lau et al., 2017; Ni et al., 2016). Case series have identified other risk factors for depression following collective actions, including media coverage, unemployment and poor social cohesion (Brown et al., 1994; Coudreaut et al., 1995; Tan and Simons, 1973). These have been corroborated by subsequent studies where exposure to collective actions via television (Galovski et al., 2016; Lazarescu et al., 1993) or social networking platforms (Lau et al., 2016, 2017; Ni et al., 2016) was associated with more depressive symptoms.
Sociodemographic factors such as female sex, lower socioeconomic status and not having children were also associated with more depressive symptoms (Lau et al., 2017; Moussa et al., 2015; Ni et al., 2017). Other risk factors included poorer resilience, pre-existing health conditions, and the loss of personal and social resources (Brown et al., 1994; Hou et al., 2015; Ni et al., 2017). Lower baseline family support and family harmony were predictors of persistent depression following the Occupy Central/Umbrella Movement (Ni et al., 2017), while conflicts with family members (Lau et al., 2017; Ni et al., 2016) were also associated with more depressive symptoms. Qualitative studies have suggested that if the collective action is not able to achieve its aims, hopelessness could result in depression (Matthies-Boon, 2017).
PTSD
Prevalence
Four studies have assessed the prevalence of PTSD after collective actions (Galovski et al., 2016; Hanson et al., 1995; Obilom and Thacher, 2008; Wang et al., 2011). All the studies were cross-sectional, so the incidence and course of PTSD following collective actions remain unknown. The prevalence of PTSD drawn from probability samples ranged from 4.1% of residents after the 1992 Los Angeles riots (Hanson et al., 1995) to 41% of residents in Nigeria’s riot-affected areas (Obilom and Thacher, 2008). Studies have also examined the prevalence of PTSD among specific groups such as teachers (Stuber et al., 1997), children (Kumar and Fonagy, 2013; Moussa et al., 2015), patients (Coudreaut et al., 1995; Ouanes et al., 2014), medical and paramedical professionals (Ouanes et al., 2012), police officers (Harvey-Lintz and Tidwell, 1997) and victims of looting and arson (Kim-Goh et al., 1995). The prevalence of PTSD among these groups ranged from 6.7% in teachers (Stuber et al., 1997) to 75% in victims of looting and arson (Kim-Goh et al., 1995).
Correlates of PTSD
Exposure to violence was most consistently associated with increased risk of PTSD: direct victims of looting, arson and physical injury demonstrated the highest levels (Kim-Goh et al., 1995; Obilom and Thacher, 2008; Unuvar et al., 2017). Witnessing a personal attack (Kumar and Fonagy, 2013; Obilom and Thacher, 2008), being in close proximity to violence (Moussa et al., 2015) and the level of media exposure (Galovski et al., 2016) were also associated with PTSD risk. Demographic characteristics such as female sex and lower socioeconomic status were associated with increased risk of PTSD among school children (Moussa et al., 2015). In the context of racial (2014 Ferguson Protests in Missouri, USA) or ethnoreligious riots (2002 Gujarat Riots in India), social identity was associated with PTSD symptoms (Galovski et al., 2016; Patel and Nath, 2013).
Anxiety
Prevalence
Four studies assessed the prevalence of anxiety after a collective action in the general population (Hou and Bonanno, 2018; Hou et al., 2015; Lau et al., 2016, 2017) and seven in special groups (Bamrah et al., 2013; Dhavale et al., 2002; Garbarino et al., 2012; Lazarescu et al., 1993; Lyons, 1971; Matthies-Boon, 2017; Moussa et al., 2015). Two studies in the general population followed the 2014 Hong Kong Occupy Central/Umbrella Movement, although different anxiety scales were used. Immediately after the Movement, 10.5% of the general population had probable anxiety (7-item General Anxiety Disorder scale) (Lau et al., 2017). In a separate study 2 months later, 47.4% were found to have moderate-to-severe anxiety (State-Trait Anxiety Inventory) (Hou et al., 2015). A time series analysis of patients in a psychiatric clinic showed an increase in anxiety symptoms after the 1989 Romanian Revolution (Lazarescu et al., 1993). Symptoms of anxiety were common among subgroups, including 69% of general practice patients during the 1969 Northern Ireland riots (Lyons, 1971), 55% of children in primary schools near protest sites (Moussa et al., 2015) and nearly half of selected young political activists after the 2011 Arab Spring in Egypt (Matthies-Boon, 2017). Anxiety symptoms were reported for 34% of children attending schools in riot-affected areas in Bombay, India (Dhavale et al., 2002), and in 37% of internally displaced people and 44% of HIV patients in health facilities after the 2007–2008 Kenyan crisis (Bamrah et al., 2013).
Correlates of anxiety
As with depression, anxiety symptoms were correlated with younger age, female sex, lower socioeconomic status (Moussa et al., 2015), being single, and without children (Lau et al., 2017), personal and social resource loss (Hou et al., 2015), political uncertainty (Matthies-Boon, 2017), and exposure to media coverage (Lazarescu et al., 1993).
Other outcomes
Alcohol consumption increased among men and women after Czechoslovakia’s 1989 Velvet Revolution, although this has been attributed to a loosening of political control over drinking rather than the revolution itself (Kubicka et al., 1995, 1998). A school-level aggregated panel design showed that changes in marijuana use following Chile’s 2011 Occupy School movement were due to secular trends rather than the collective actions (Castillo-Carniglia et al., 2017). Findings related to reactive psychosis have been mixed. Reactive psychosis increased among patients during the 1989 Romanian Revolution (Lazarescu et al., 1993). In contrast, the 1969 Northern Ireland riots did not appear to impact reactive psychosis (Lyons, 1971) and was associated with fewer suicides (Lyons, 1972).
Appraisal of studies
Five of the six longitudinal studies received the maximum NOS score (Greenley et al., 1975; Kubicka et al., 1995, 1998; Ni et al., 2016, 2017); all six were assessed to be of ‘good quality’ (cutoff: NOS score ⩾ 7 out of maximum 9) (McPheeters et al., 2012; Patra et al., 2015) (Supplemental Table S5). Of the 22 cross-sectional and serial cross-sectional studies, 5 received the maximum score of 6 (Castillo-Carniglia et al., 2017; Hanson et al., 1995; Hou et al., 2015; Lau et al., 2017; Sasao and Chun, 1994) and 3 had a NOS score of 5 (Galovski et al., 2016; Moussa et al., 2015; Obilom and Thacher, 2008) (Supplemental Table S6).Studies with lower scores generally did not control for confounders such as sociodemographics.
Discussion
To our knowledge, this is the first systematic review of collective actions and mental health. Depression and PTSD are the two most commonly studied mental health outcomes for collective actions, disasters and armed conflicts (Charlson et al., 2019; Goldmann and Galea, 2014). Notably, the prevalence of depression and PTSD following collective actions both in the general population and among victims of violence appear comparable to those experiencing natural disasters, terrorist attacks and armed conflicts (Charlson et al., 2019; Goldmann and Galea, 2014; Hanson et al., 1995; Hou et al., 2015; Kim-Goh et al., 1995; Ni et al., 2016, 2017; Obilom and Thacher, 2008). Risk factors for psychopathology following collective actions included individual characteristics (e.g. female sex, low socioeconomic status, psychological resilience, health status, social support), the nature of the event itself (e.g. exposure to violence, media coverage, level of engagement) and post-event circumstances (e.g. loss of personal and social resources, unemployment) (Goldmann and Galea, 2014; Hanson et al., 1995; Kumar and Fonagy, 2013; Lau et al., 2017; Moussa et al., 2015; Ni et al., 2016, 2017; Norris et al., 2002a, 2002b; North and Pfefferbaum, 2013).
There is some evidence that collective actions may also be associated with better mental health (n = 2; 4% of all studies) such as reduced depression and suicides (Greenley et al., 1975; Lyons, 1972). This finding may be explained by collective actions serving as a cathartic experience when people collectively express grievances (Curran, 1988). Furthermore, greater social cohesion among subpopulations, either supporting or opposing the cause of the collective action, could strengthen social ties, which in turn could buffer the adverse impact of the stressful environment (Curran, 1988; Kawachi and Berkman, 2001; Lyons, 1973).
For natural disasters and terrorist attacks, the threat of harm or death is a key mediator of mental health consequences (Goldmann and Galea, 2014). Yet collective actions can still exact a substantial, pervasive and persistent toll on mental health even in the absence of large-scale violence such as fatalities, looting or arson (Hou et al., 2015; Ni et al., 2016, 2017). Nonviolent collective actions must therefore influence health via alternative mechanisms. Stressors and stress appraisal processes are potential explanation for the mental health impact of protests (Ni et al., 2017). Stressors are operationalised as environmental demands that challenge a person’s adaptive capacity, while stress reactivity refers to a greater risk of mental disorder following stress exposure (Hammen, 2015; Porta, 2014). The importance of stress reactivity in the development of psychiatric disorders has been recognised by its inclusion as the first domain of the Research Domain Criteria matrix (Insel et al., 2010). Thus, risk factors for mental health disorders following collective actions could be interpreted as the product of exposure and the person’s stress reactivity (Hammen, 2005; Ni et al., 2017). Collective actions can generate stressors via interpersonal conflicts and the disruption of health services (Ni et al., 2016; Yimgang et al., 2017). Social media may also act as a stressor due to interactions with other online users holding different ideological views (American Psychological Association, 2016; Bakshy et al., 2015). This could account for the association of social media use (Ni et al., 2016) and ‘unfriending’ (Lau et al., 2016) with depressive sequelae in the 2014 Occupy Central/Umbrella Movement. Protective factors may operate via stress appraisal processes, where higher baseline resilience (a measure of ability to cope with stressors) was associated with fewer depressive sequelae (Ni et al., 2017). Similarly, the protective role of social support might be explained by the stress buffering function of social ties (Goldmann and Galea, 2014; Kawachi and Berkman, 2001).
Limitations
This review is subject to several limitations. First, all identified studies were observational, so causality between the collective action and mental health outcomes cannot be directly inferred (Amenta et al., 2010; Giugni, 1998). It is difficult to ascertain whether changes in mental health were due to the circumstances that led to the collective action or to the collective action itself. Nevertheless, we have highlighted encouraging examples of longitudinal studies (Table 3) with before, during and after data for collective actions (Castillo-Carniglia et al., 2017; Fishbain et al., 1991; Greenley et al., 1975; Ni et al., 2016, 2017; Yimgang et al., 2017), which represent an advance from the preponderance of cross-sectional studies mostly conducted after the event in the literature thus far. Second, collective actions are disparate and our review may have omitted relevant studies. However, we used a combination of terms to identify different types of collective actions and accessed multiple bibliographic databases to broaden our search strategy. Third, there could also be publication bias as the majority of published studies were on riots and revolutions (Earl et al., 2004). As riots and revolutions commonly involve violence and deaths, they are more likely to reveal significant associations with adverse mental health. Fuller reporting of studies that find null or positive associations is needed, as well as research on nonviolent forms of collective actions given emerging evidence that they can also influence mental health (Hou et al., 2015; Lau et al., 2016, 2017; Ni et al., 2016, 2017). Fourth, comparisons between studies are limited by the heterogeneity of collective actions and the samples, a limitation that also applies to the disaster literature (Nandi et al., 2009). Due to the heterogeneity of the identified studies, a meta-analysis may not be appropriate (Higgins and Green, 2012b; Page et al., 2016). Fifth, this heterogeneity and the limited numbers of studies reduce the generalisability of our findings. This could be addressed by developing a standardised exposure assessment for collective actions, analogous to the Traumatic Exposure Severity Scale for disaster-related trauma (Elal and Slade, 2005). Sixth, the studies employed different measures of mental health, which made cross-study comparisons difficult. Future studies should assess mental health using diagnostic interviews or validated standardised scales (Galea and Maxwell, 2009). Finally, while the Cochrane collaboration recommends the NOS for the quality assessment of non-randomised studies (Higgins and Green, 2012a), the NOS was designed for cohort and case–control studies only. Nevertheless, the NOS has been modified with reference to previous reviews for the appraisal of cross-sectional studies (Anglin et al., 2013; Patra et al., 2015).
Implications for future research
Despite the extensive history and prevalence of collective actions around the world, our systematic review only identified 52 relevant studies of mental health outcomes (Figure 1). By comparison, there are more than 280 studies of PTSD following disasters (Nandi et al., 2009), 129 on conflicts (Charlson et al., 2019) and more than 150 studies have been conducted on the mental health consequences of the 11 September terrorist attacks (Perlman et al., 2011). The sparse documentation on collective actions has been attributed to their rapidly evolving and sporadic nature (Slone, 2003). Yet these methodological challenges also apply to disasters and armed conflicts (Galea and Maxwell, 2009).
As the majority of the population is resilient to a traumatic event, it would be more informative to examine trajectories of mental health rather than the population average (Bonanno et al., 2011). Longitudinal studies show that individuals exhibit remarkable resiliency following collective actions or disasters (Ni et al., 2017; Norris et al., 2009). We identify a lack of studies that assess potential mechanisms using theoretical frameworks relevant to mental health outcomes. One relevant framework is the social support deterioration model, which posits that declines in perceived social support after a population event mediate the immediate and delayed psychopathology (Kaniasty and Norris, 1993). The social support deterioration model is most applicable to human-induced events and thus could be relevant to collective actions (Kaniasty and Norris, 2009; Rochford and Blocker, 1991). Indeed, collective actions have the potential to exacerbate ideological divisions (Fraser, 1971; Ni et al., 2016) where disputes with family members over politics, rather than actual participation in protests, were associated with depressive sequelae during the 2014 Occupy Central/Umbrella Movement (Lau et al., 2017; Ni et al., 2016). In order to test the social support deterioration model, future studies should document social dynamics, together with other potential mediators, before, during and after an event as these could be as important in the long-term course of mental health as the event itself (Ajdukovic, 2004; Ni et al., 2017). Emerging methods could also be incorporated, for example, biological markers of stress (Hoyt et al., 2018), harnessing the social media as a form of mental health surveillance (Gruebner et al., 2016) and applying time-varying analytic approaches to disentangle underlying mechanisms (Galea and Maxwell, 2009; Slone et al., 2000).
None of the identified studies examined interventions to improve mental health following a collective action. Future research on interventions targeting risk factors for psychopathology and enhancing resilience is warranted. Psychological first aid, cognitive-behavioural therapy (CBT) and exposure-based therapy have been recommended in the disaster setting (Neria et al., 2009; North and Pfefferbaum, 2013). Interpersonal psychotherapy may also be promising since it could specifically address the social disruptions that are frequently observed in collective actions (Markowitz and Weissman, 2004; Ni et al., 2016, 2017).
Conclusion
Our review shows that the mental health outcomes following collective actions can be comparable to natural disasters, terrorist attacks or armed conflicts (Charlson et al., 2019; Goldmann and Galea, 2014; Hanson et al., 1995; Hou et al., 2015; Kim-Goh et al., 1995; Ni et al., 2016, 2017; Obilom and Thacher, 2008). Health care professionals therefore need to be vigilant to both the short- and medium-term psychiatric sequelae of collective actions. They should be particularly aware of potential community spillover effects, where even those who did not take part in the collective action can experience psychiatric sequelae (Galovski et al., 2016; Lau et al., 2017; Lazarescu et al., 1993; Ni et al., 2016). The Constitution of the World Health Organization (1995) states that ‘health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition’. This underlines the importance for all sides to find a peaceful resolution. On the other hand, studies have also suggested positive mental health influences of collective actions (Greenley et al., 1975; Lyons, 1972). Given the extensive research on disasters and conflicts, studies of collective actions may benefit from drawing upon the disaster- and conflict-related literatures, which have been summarised in classic reviews and texts (Charlson et al., 2019; Galea et al., 2005; Goldmann and Galea, 2014; Norris et al., 2002a, 2002b; North and Pfefferbaum, 2002). However, given the qualitative differences between collective actions, disasters and armed conflicts, tailored studies for collective actions are needed. Despite the increase in collective actions globally and their documented mental health consequences (Ortiz et al., 2013), collective actions have often been overlooked as a sociopolitical determinant of mental health. The literature has just begun to assess the mental health impact of collective actions and the underlying mechanisms. Research in this emerging field of inquiry would therefore be timely (Ni et al., 2020).
Supplemental Material
Appendix_clean_Jan9_ver2 – Supplemental material for Mental health during and after protests, riots and revolutions: A systematic review
Supplemental material, Appendix_clean_Jan9_ver2 for Mental health during and after protests, riots and revolutions: A systematic review by Michael Y Ni, Yoona Kim, Ian McDowell, Suki Wong, Qiu Hong, Irene OL Wong, Sandro Galea and Gabriel M Leung in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We thank Irene Wong, Candi Leung, and Cynthia Yau for technical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: General Research Fund (RGC GRF Grant #17609818), Research Grants Council, University Grants Committee of Hong Kong and Seed Fund for Basic Research for Resubmission of GRF/ECS Proposals 2017/18, University Research Committee, The University of Hong Kong.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.