
Abstract
Objective:
Emergency workers, such as fire-fighters, are routinely exposed to potentially traumatic events. While a number of studies have examined the occurrence of post-traumatic stress disorder, the role of multiple traumas on other mental health sequelae, such as depression and alcohol misuse, among emergency workers remains unclear. This study aimed to assess the prevalence of post-traumatic stress disorder, depression and alcohol misuse in a sample of current and retired fire-fighters and examine their relationship with cumulative trauma exposure.
Method:
A cross-sectional survey was completed by current (n = 488) and retired (n = 265) fire-fighters from Fire and Rescue New South Wales, Australia. Demographic and occupational information was collected, including the number of fatal incidents fire-fighters reported attending across years of service. Validated, self-report measures were used to determine probable caseness for post-traumatic stress disorder, depression and heavy drinking.
Results:
Among current fire-fighters, rates of post-traumatic stress disorder and depression were 8% and 5%, respectively, while 4% reported consumption of more than 42 alcoholic drinks per week. Retired fire-fighters reported significantly greater levels of symptomatology, with the prevalence estimates of post-traumatic stress disorder at 18% (p = 0.001), depression at 18% (p < 0.001) and heavy drinking at 7%. There was a significant positive linear relationship between the number of fatal incidents attended and rates of post-traumatic stress disorder, depression and heavy drinking.
Conclusion:
Fire-fighters suffer from high rates of mental disorders, with rates of post-traumatic stress disorder, depression and heavy drinking continuing to rise in a linear manner with each additional trauma exposure. The level of psychiatric morbidity among retired fire-fighters appears to be particularly high. Our findings have important implications for the ongoing debates surrounding the detection of mental disorders in high-risk occupations and for policy considerations around the welfare of current and retired emergency workers.
Introduction
Emergency workers perform a vital role in our society. They protect the rule of law, ensure our safety and provide assistance in emergencies. However, there is an increasing realisation that emergency work can come at a personal cost and that the regular exposure to trauma inherent in the role may be creating a large burden of mental health problems (McFarlane and Bryant, 2007). There are a range of mental health conditions that can occur in the aftermath of traumatic exposure, including depression, anxiety, post-traumatic stress disorder (PTSD), adjustment disorder, increased physical complaints and substance use (Farmer et al., 2000; Fear et al., 2010; Knudsen et al., 2013; Milliken et al., 2007; Paykel et al., 1996; Salyards et al., 2013). However, most studies examining the mental health of emergency workers have focused solely on PTSD, with a recent meta-analysis of 16 studies suggesting that 7% of current fire-fighters suffer from PTSD (Berger et al., 2012). While this represents a prevalence of PTSD far in excess of that seen in the general population (Creamer et al., 2001), an exclusive focus on PTSD risks under-estimating the full mental health impact of trauma exposure among emergency workers.
Studies of military personnel, who are similarly exposed to regular trauma as part of their work, have demonstrated other disorders such as depression and alcohol misuse to be substantially more prevalent than PTSD (Fear et al., 2010; Iversen et al., 2009). The few studies that have considered mental disorders other than PTSD among emergency workers have suggested a similar pattern, with one study of fire-fighters reporting more than 40% engaged in hazardous drinking behaviours (Haddock et al., 2012). Comparisons with the research data on military personnel also highlight a relative neglect of the long-term impacts of cumulative trauma exposure (Harvey et al., 2012) and consideration of what happens after an emergency worker retires. Recent studies have demonstrated that retired military personnel have higher levels of depressive, anxious and PTSD symptoms compared to those still serving (Hatch et al., 2013; Iversen et al., 2005). The reasons for this are not clear, although are likely related to the impact of cumulative trauma exposure over a whole career and the loss of social networks, roles and support after retirement (Harvey et al., 2011). While two studies have examined the prevalence of depression and PTSD in retired fire-fighters (Chiu et al., 2010, 2011), direct comparisons between current and retired fire-fighters and considerations of the above causal and confounding pathways are yet to be published.
Much of the epidemiology around emergency worker mental health has accumulated from studies following single major traumatic events, such as aircraft disasters (Huizink et al., 2006; Pietrzak et al., 2014) and bushfires (McFarlane, 1989). However, typically fire-fighters are exposed to multiple critical incidents across their careers. As the risk of developing PTSD increases with the number of exposures to traumatic events (Brewin et al., 2000), it is important to consider the impact of cumulative trauma exposure among emergency workers. However, the small number of studies that have examined this question have produced mixed findings. Wagner et al. (1998) found that the number of distressing missions undertaken by fire-fighters predicted PTSD symptoms, but Meyer et al. (2012) reported that the number of critical incidents attended by fire-fighters did not predict diagnosis of PTSD. While some preliminary investigations have shown that fire-fighters exposed to a greater number of trauma types had an increased risk of mood and alcohol use disorders (Kaufmann et al., 2013), others have found that there was no association between the number of critical incidents attended by fire-fighters and common mental disorders (Meyer et al., 2012). Resolving these discrepancies is crucial in developing a better understanding of the risks faced by emergency workers and in formulating policy and intervention responses that can focus on those at greatest risk.
This study aimed to assess the prevalence of a variety of mental health and alcohol use disorders (PTSD, depression and heavy drinking) in current and retired fire-fighters from one of the largest urban fire services in the world. It also aimed to examine the impact of cumulative trauma exposure on the development of mental health and alcohol use disorders. We hypothesised that retired fire-fighters would have greater levels of psychiatric symptomatology than current fire-fighters and that rates of mental health and alcohol use disorders would increase with repeated trauma exposure.
Methods
Participants
Participants were drawn from Fire and Rescue New South Wales (FRNSW), Australia. All procedures were approved by the Human Research Ethics Committee at the University of Sydney (Ref. No. 03-2009/11607), and participants provided informed consent. FRNSW is the seventh largest urban fire service in the world and responds to fire-fighting, rescue and hazardous material emergencies across Sydney and surrounding regional areas. Current and retired fire-fighters were recruited in two waves between November 2009 and October 2010. As one of the main aims of this study was to produce accurate prevalence estimates, an initial sample (called the ‘prevalence sample’) was recruited in a manner to maximise response rates and reduce sample bias. Researchers visited a selection of both metropolitan and regional fire stations and approached all on-duty fire-fighters to participate in this study. At the same time, all registered retired fire-fighters were contacted via mail with a request to participate in the study. In order to maximise the available sample size and power for analyses of association, which are less sensitive to error from sample bias than prevalence analyses (Knudsen et al., 2010), a second wave of recruitment was undertaken to form an ‘enriched sample’. An online version of the survey was emailed to all FRNSW employees and made available via a number of websites. As this study was focused on full-time fire-fighters, data from voluntary fire-fighters were excluded.
Measures
Demographics and trauma exposure
All participants were asked to provide basic sociodemographic (gender, age) and occupational (employment status, fire-fighter rank, years of experience) information. Participants who were no longer employed by FRNSW were asked to state their year of retirement. In addition, all participants were asked how frequently they had attended serious incidents involving one or more fatalities since joining FRNSW, with the following options: 0, 1–5, 6–10, 11–20, 21 or more. This information was used to calculate the number of serious incidents involving fatalities attended per year of service.
PTSD
A self-report questionnaire based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) Criterion A for PTSD and the Post-traumatic Diagnostic Scale (PTDS) were used to detect cases of probable PTSD. The PTSD DSM-IV Criterion A questionnaire directly reflected DSM-IV Criterion A for PTSD (American Psychiatric Association [APA], 1994) and was similar to that used in previous studies with fire-fighters (Haslam and Mallon, 2003). Participants were instructed to think of the most personally distressing event they had attended as a fire-fighter before answering three questions. These questions assessed whether or not participants felt they were ‘personally threatened in terms of serious injury or death’ (Q1.1.) or witnessed another person being threatened (Q1.2). Participants were then asked whether they had experienced ‘any fear, horror or helplessness’ (Q2) as a result of the distressing event. Participants who answered ‘yes’ to either Q1.1 or Q1.2 and ‘yes’ to Q2 were considered to have met DSM-IV Criterion A for PTSD. The PTDS is a validated self-report questionnaire and has demonstrated high diagnostic agreement with the Structured Clinical Interview (SCID) for PTSD (Foa et al., 1997). The PTDS comprises 49 items that assess severity of PTSD symptoms according to DSM-IV Criteria. Only items 17–38, which correspond to symptoms of re-experiencing (Criterion B), avoidance (Criterion C) and hyper-arousal (Criterion D), were included in this study. Participants indicated the frequency with which they had experienced a particular symptom in the last month using a 4-point scale ranging from 0 (‘Not at all or only one time’) to 3 (‘5 or more times a week/almost always’). Participants who scored a total of 15 or higher on the PTDS were considered to have moderate to severe PTSD symptoms (Sheeran and Zimmerman, 2002). A participant must have met DSM-IV Criterion A for PTSD and have moderate to severe PTSD symptoms to be classified as a probable PTSD case.
Depression
The Symptom Checklist Core Depression Scale (SCL-CD6) was used to detect cases of probable depression. The SCL-CD6 is a valid brief (6-item) scale of depression and predicts use of antidepressant drugs and hospitalisation with a depressive episode (Hanson et al., 2014). Participants indicated the extent to which a particular symptom had caused them discomfort in the past week using a 4-point scale ranging from 1 (‘Not at all’) to 5 (‘Extremely’). The SCL-CD6 is typically used with a 5-point scale. To ensure that we were able to utilise the validated cut-off score, responses were rescaled to ensure a total score out of 30. Participants who scored a total of 17 or higher on the SCL-CD6 were considered to have moderate to severe depression symptoms (Hanson et al., 2014).
Hazardous alcohol consumption
The Alcohol Use Disorders Identification Test–Consumption (AUDIT-C) was used to measure alcohol consumption. The AUDIT-C is a sound screening tool and has been demonstrated to be as effective as the full AUDIT (Reinert and Allen, 2007). The AUDIT-C comprises three items that were scored in accordance with previous research with military populations, another high-risk group with a culture of heavy drinking (Henderson et al., 2009). Weekly alcohol consumption was calculated by multiplying the number of days per week an alcoholic drink was consumed with the number of alcoholic drinks consumed on a typical day. ‘Unsafe drinking’ was defined as consuming more than 21 alcoholic drinks per week, and ‘heavy drinking’ was defined as consuming more than 42 alcoholic drinks per week.
Poor subjective wellbeing
The Satisfaction with Life Scale (SWLS) was used to gain a measure of the impact of any mental disorder on subjective wellbeing. The SWLS consists of five items, and participants indicated their agreement with positive statements about their life using a 7-point scale ranging from 1 (‘Strongly disagree’) to 7 (‘Strongly agree’). Based on normative data from Western populations (Pavot and Diener, 1993), participants who scored 19 or lower on the SWLS were considered to have poor subjective wellbeing.
Analysis
Data was analysed using STATA statistical software, version 12.1. As noted above, the initial ‘prevalence’ sample was used to estimate the prevalence of and overlap between the mental and alcohol use disorders as it was likely to be less biased than the final enriched sample. Differences in demographics and trauma exposure between current and retired fire-fighters were tested using Fisher’s exact tests or t-tests. Differences in the prevalence of mental and alcohol use disorders in current and retired fire-fighters were examined, in addition to the overlap between the disorders. The high correlation between employment status (current or retired) and other key predictors of mental disorder, such as age and level of exposure to cumulative trauma, prevented the use of multivariate logistic regression to examine the independent impact of retirement on mental health. Univariate logistic regression was used to provide a measure of the relative difference in prevalence rates. The final enriched sample, which was larger but with a greater chance of sampling bias, was used for analyses focused on associations. The associations between the type and number of mental and alcohol use disorders, and poor subjective wellbeing were initially assessed. In addition, logistic regression was used to examine the associations between the number of fatal incidents attended across all years of service/per year of service and the prevalence of mental and alcohol use disorders. Sex, age, rank and employment status (current or retired) were used as covariates. As only a very small number of the final enriched sample had not attended any fatal incidents across all years of service, the group that had attended one to five fatal incidents was used as the reference point for this analysis.
Results
A total of 341 current fire-fighters were recruited during direct visits to metropolitan and regional fire stations. Given the nature of fire-fighter duty, with emergency call-outs happening during recruitment and participation, it was difficult to estimate the exact response rate, but total staffing figures for a subset of stations visited suggest a response rate of 84%. As the focus of this study was on full-time fire-fighters, data collected from volunteer fire-fighters present at stations during recruitment (n = 67, 19.6%) were excluded, leaving a final prevalence estimate sample of 274 current fire-fighters. Of the 1408 retired fire-fighters who received a copy of the survey via mail, 354 (25.1%) responded. Of these respondents, 97 (27.4%) who indicated that they were previously volunteer fire-fighters were excluded, leaving a final prevalence estimate sample of 256 retired fire-fighters. These prevalence estimate samples were enriched with data collected from additional current and retired fire-fighters via an identical online questionnaire. As outlined in Table 1, the final sample size of the enriched data was 753 fire-fighters. As expected, retired fire-fighters tended to be older, more experienced, of a higher rank and to have been exposed to a greater overall number of potentially traumatic events (p < 0.05 for all).
Demographic characteristics of prevalence and enriched samples.
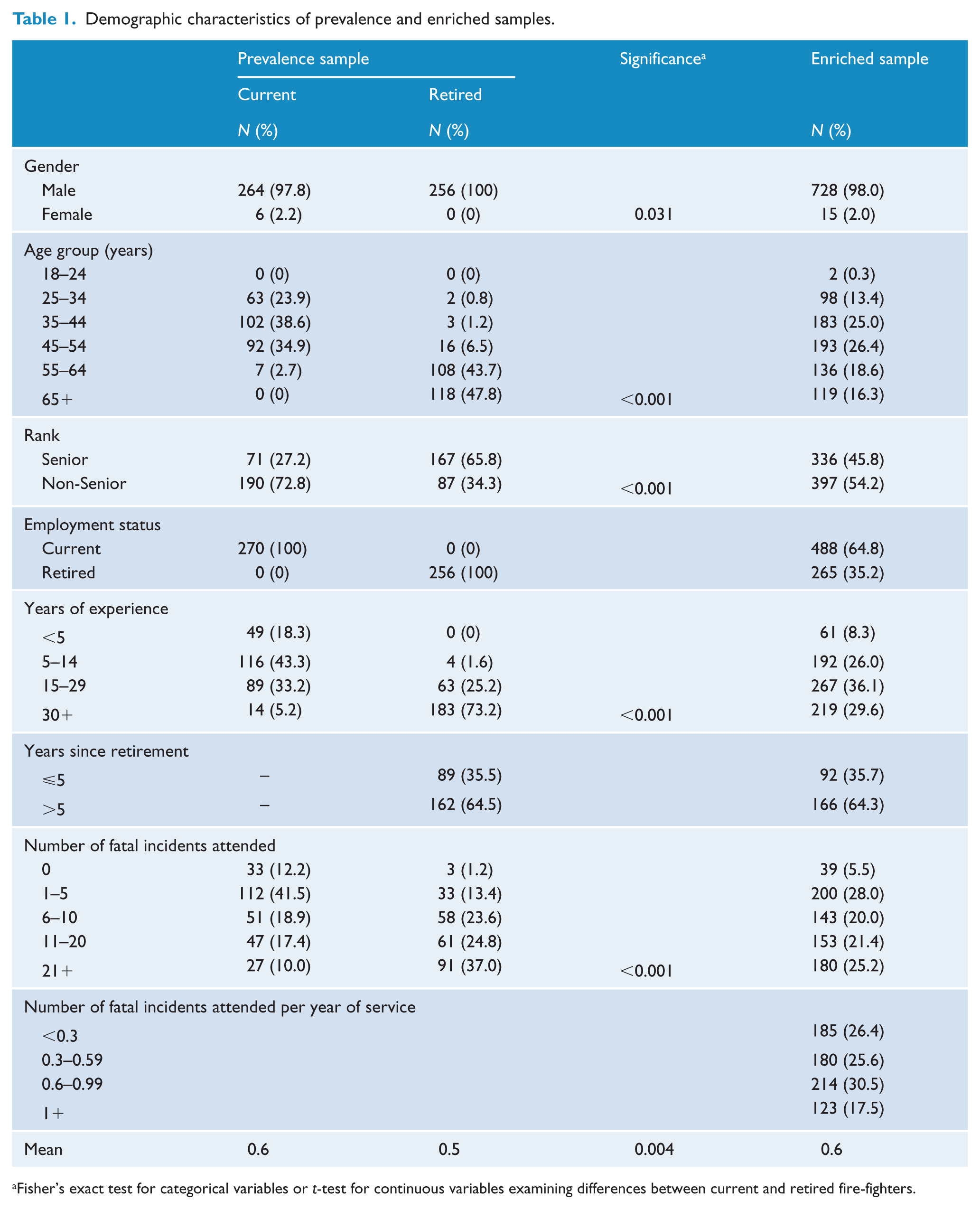
Fisher’s exact test for categorical variables or t-test for continuous variables examining differences between current and retired fire-fighters.
The estimated prevalence of mental disorders and heavy drinking in current and retired fire-fighters is shown in Table 2. Probable PTSD and depression were prevalent in the sample, with 13% and 11% of surveyed fire-fighters reporting at least moderate levels of symptoms. Heavy drinking (more than 42 alcoholic drinks per week) was reported by 6% of surveyed fire-fighters; however, 24% of the sample reported engaging in unsafe drinking (more than 21 alcoholic drinks per week; data not reported). Retired fire-fighters reported significantly higher rates of probable PTSD (unadjusted odds ratio [OR] = 2.61; 95% confidence interval [CI] = [1.47, 4.64]; p = 0.001) and depression (unadjusted OR = 4.31; 95% CI = [2.27, 8.22]; p < 0.001). However, there was no significant difference in heavy drinking between current and retired fire-fighters (unadjusted OR = 1.83; 95% CI = [0.85, 3.96]; p = 0.123). Overall, 13% of current and 27% of retired fire-fighters reported being afflicted by at least one mental or alcohol use disorder. When comparing subgroups of retired fire-fighters, there were no significant differences in rates of mental and alcohol use disorders between recently (within the last 5 years) retired and long-retired fire-fighters (p > 0.05 for all). However, there was a non-significant trend towards recently retired fire-fighters reporting higher rates of probable PTSD than long-retired fire-fighters (p = 0.07).
Prevalence estimates of mental disorders for current and retired fire-fighters.

PTSD: post-traumatic stress disorder; CI: confidence interval.
Table 3 displays the estimated overlap between different mental disorders and heavy drinking in the enriched sample of fire-fighters. Overall, the levels of overlap were high. There was a high rate of comorbidity between probable PTSD and depression, with more than half of those suffering from one disorder also meeting the criteria for the other. Both of these mental disorders were also moderately comorbid with heavy drinking.
Overlap among mental and alcohol use disorders in all fire-fighters.
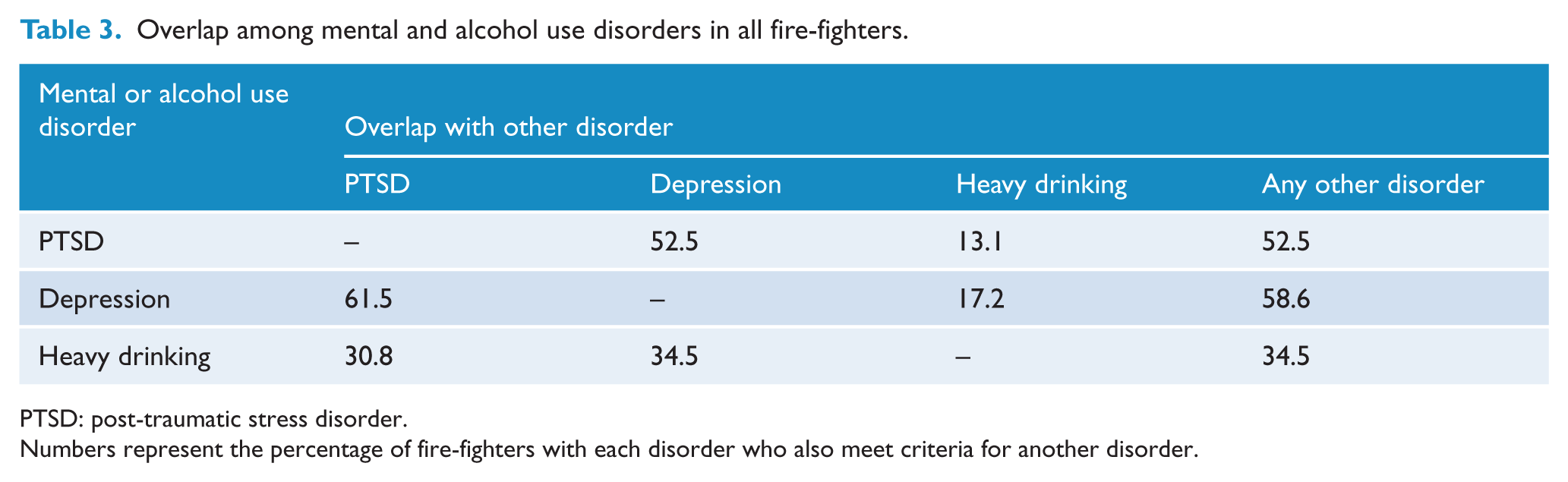
PTSD: post-traumatic stress disorder.
Numbers represent the percentage of fire-fighters with each disorder who also meet criteria for another disorder.
The impact of mental and alcohol use disorders on subjective wellbeing in the enriched sample of fire-fighters is shown in Figure 1. More than half of the fire-fighters suffering from either probable PTSD or depression were classified as having poor subjective wellbeing. Heavy drinking had a similar, but slightly reduced impact, with 43% of fire-fighters engaging in heavy drinking reporting poor subjective wellbeing. As the number of mental disorders increased, the percentage of fire-fighters classified as having poor subjective wellbeing also increased. For example, only 11% of fire-fighters free from any mental or alcohol use disorders had poor subjective wellbeing, whereas 72% of fire-fighters afflicted by two or more mental disorders reported poor subjective wellbeing.
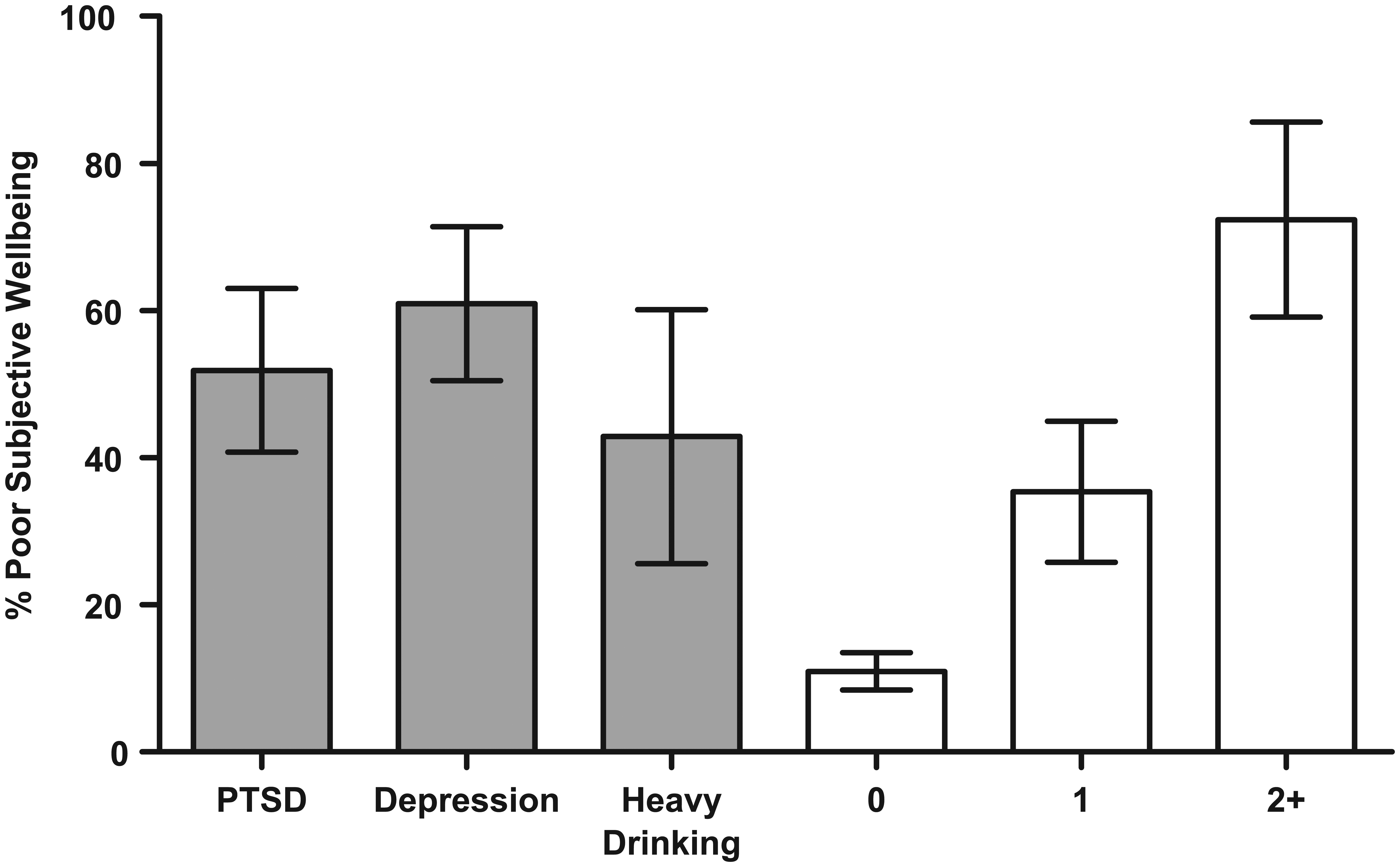
The impact of type and number of mental and/or alcohol use disorders on subjective wellbeing.
Figure 2 displays the negative impact of cumulative trauma exposure on mental health and alcohol use. Controlling for potentially confounding demographic variables (sex, age, rank and employment status), a higher number of fatal incidents attended across all years of service were associated with significantly greater chance of being afflicted by each of the mental and alcohol use disorders. Specifically, fire-fighters who had attended more than 21 fatal incidents across all years of service had significantly greater odds of suffering from probable PTSD (OR = 3.82; 95% CI = [1.81, 8.05]; p < 0.01) and depression (OR = 2.62; 95% CI = [1.26, 5.46]; p = 0.01) compared to those who had attended 1–5 fatal incidents. In addition, there was a non-significant trend towards attendance at more than 21 fatal incidents across all years of service resulting in greater odds of fire-fighters engaging in heavy drinking (OR = 2.71; 95% CI = 0.99, 7.37; p = 0.05) relative to 1–5 fatal incidents. There was strong evidence of a positive linear relationship between the number of fatal incidents attended across all years of service and the odds of being afflicted by any of the mental and alcohol use disorders (p < 0.02 for all). Quadratic models were constructed but were found to be no more predictive than linear models (p > 0.10 using Likelihood Ratio tests).
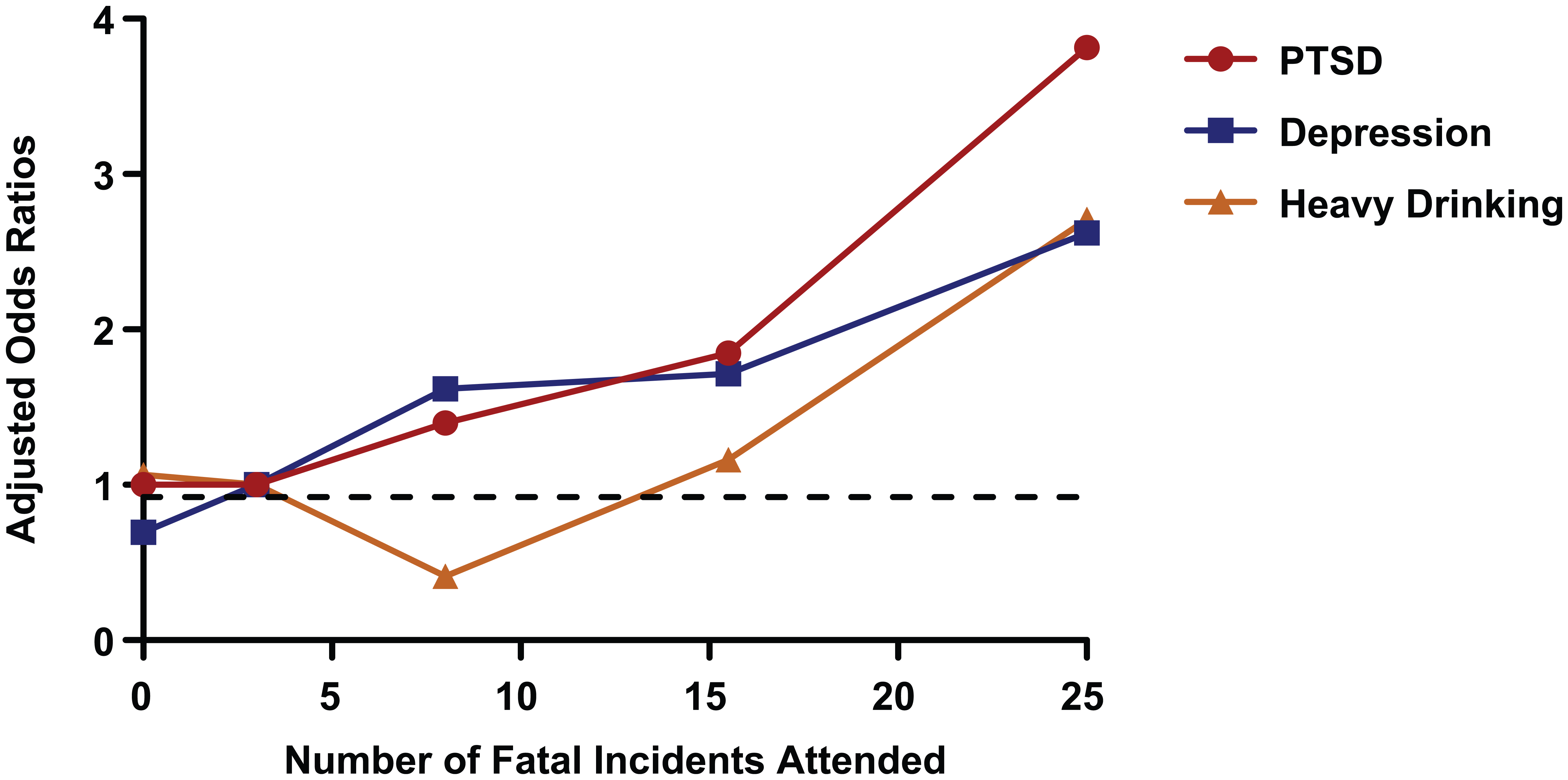
The impact of cumulative trauma exposure on mental disorders.
In contrast, there was no association between the frequency of fatal incidents attended per year of service and the odds of being afflicted by any of the mental or alcohol use disorders (p > 0.05 for all).
A sensitivity analysis was completed, where all analyses conducted using the larger enriched sample were repeated in the smaller, less biased prevalence estimate sample. The associations between each of the mental disorders and poor subjective wellbeing remained unchanged. Similarly, the significant linear association between the number of fatal incidents attended and an increasing prevalence of PTSD (p = 0.004) remained. The trends towards greater depression and heavy drinking as cumulative trauma exposure increased also remained, but were reduced to non-significant levels due to the reduced sample size. The lack of any association between the frequency of fatal incidents and all mental disorders remained.
Discussion
We have demonstrated substantial levels of psychiatric morbidity among both current and retired fire-fighters. Beyond demonstrating high levels of symptomatology among this important occupational group, this study makes three important contributions to the literature on the mental health of emergency workers. First, it extends research findings beyond the traditional focus on the prevalence of PTSD to also consider other mental health outcomes, particularly depression and heavy drinking. The importance of this extension is highlighted by the observation that disorders other than PTSD became more prevalent as the exposure to trauma accumulated. Second, it reports on the rates of mental disorders and alcohol use in retired fire-fighters, a subgroup that has been largely neglected in previous studies. In our study, retired fire-fighters were found to be substantially more mentally unwell than current fire-fighters, with higher rates of PTSD and depression. Finally, our study has clarified the important role of cumulative trauma exposure in emergency workers, by clearly demonstrating a positive linear relationship between the total accumulated occupational trauma exposure and the risk of PTSD, depression and heavy drinking.
This study has a number of strengths. Most significantly, it was designed with a two-step sampling technique that allowed for both an accurate relatively unbiased estimate of the prevalence of a variety of mental disorders and a sufficiently sized enriched sample to examine important associations. The use of well-validated measures also adds to the strengths of our findings. Despite this, this study also had some important limitations. First, there were differing sampling techniques and response rates among current and retired fire-fighters. The lower response rate among retired fire-fighters may have introduced sampling bias, which could limit the generalisability of the findings. As there was no information available on the characteristics of the non-participants, it is difficult to determine how this may have affected this study’s results. Individuals with a history of mental disorders may be more interested in participating in research that has personal relevance and so may have been over-represented in the sample of retired fire-fighters. Conversely, studies utilising population linkage data have found that individuals with mental disorders tend to be under-represented in community health studies (Knudsen et al., 2010), which would push our findings in the other direction. Reassuringly, other studies examining the links between trauma exposure and health outcomes have concluded that overall response rates had little effect on important associations (Tate et al., 2007). Second, related to the issue of sampling bias among the retired fire-fighters, the survey did not include a question on the reason for retirement. As such, we cannot discount the possibility that the higher levels of psychiatric symptomatology among the retired fire-fighters are the result of a significant proportion having retired due to mental health problems. Third, this study utilised self-report questionnaires, which while selected on the basis of their strong validity do not have comparable diagnostic precision to structured clinical interviews. Notably, the number of alcoholic drinks consumed per week is not an exact indicator of alcohol abuse and/or dependence. Nonetheless, excessive alcohol consumption, as distinct from alcohol use disorder, is associated with poorer physical and psychological functioning as well as health service utilisation (Tuithof et al., 2014). Moreover, the study was undertaken from 2009 to 2010, before the updated DSM-5 criteria for PTSD had been publicly released. As such, the self-report questionnaire used to assess PTSD symptoms was based on DSM-IV criteria, although recent studies suggest the changes to DSM criteria will not significantly alter estimated PTSD prevalence in trauma-exposed samples (O’Donnell et al., 2014). An additional issue created by the timing of this survey is the possibility that new initiatives will be undertaken by FRNSW since this survey may have altered some of the prevalence findings. Fourth, there is a risk of type 1 errors in any study, particularly when multiple comparisons are reported. We were careful to only undertake a small number of statistical tests related to our a priori hypotheses, meaning corrections for multiple comparisons were not required (Perneger, 1998). However, even if such corrections were made, the majority of our reported findings remained statistically significant. Finally, the cross-sectional design of is study limits the inferences that can be made with regard to the direction of causation in any associations reported.
Previous studies on the prevalence of PTSD in emergency service workers have reported mixed findings. However, the results of this study (8%) are strikingly similar to those of a recent international meta-analysis which revealed a PTSD prevalence of 7% among fire-fighters (Berger et al., 2012). The reason for the discrepant findings in other studies is uncertain, but is most likely due to differences in the methods of diagnosis employed and inadequate sample sizes. Using self-report questionnaires that assess only a subset of post-traumatic stress symptoms, estimates of PTSD prevalence among fire-fighters have been as high as 37% (Bryant and Harvey, 1995). In contrast, self-report surveys that examine Criterion A in addition to the full spectrum of PTSD symptoms, like that used in this study, have resulted in PTSD prevalence estimates that are more comparable to that achieved with structured clinical interviews (Del Ben et al., 2006; Meyer et al., 2012).
While PTSD has traditionally been the focus of the research on the mental health of emergency service workers, this study has demonstrated that other mental disorders are also widespread and need more attention. Studies of military personnel exposed to repeated traumas have found high rates of both depression and alcohol misuse (Fear et al., 2010; Iversen et al., 2009); however, we found a relatively low prevalence of depression and heavy drinking among current fire-fighters (5% and 4%, respectively). This is not dissimilar to the results of another study of current fire-fighters, which estimated the prevalence of depression to be 3.5% (Meyer et al., 2012). When examining alcohol consumption in this study, 24% of current and retired fire-fighters were exceeding the recommended limit of 21 alcoholic drinks per week. However, the use of a more stringent cut-off point (more than 42 alcoholic drinks per week) showed that 6% of the total sample were engaging in heavy drinking. The drinking of alcohol has been associated with high levels of comradeship in some occupational settings (Browne et al., 2008) and could be considered part of a culturally relevant method of coping with stressful situations. However, the levels of alcohol use reported by some fire-fighters in this study could have a negative impact on their physical and mental health, and occupational functioning (Skogen et al., 2009; Vahtera et al., 2002)
The relative prevalence of different mental disorders has implications for the ongoing policy debate regarding the possible role of mental health screening in emergency services. While some have suggested that screening for depression and PTSD symptoms may be justified in high-risk groups such as military personnel and emergency workers (Grieger et al., 2006; McFarlane and Bryant, 2007), others have raised concern about the potential risks (Demaria et al., 2006). Any screening test can produce false-positive results, increase distress, heighten stigma and make individuals more focused on their symptoms (Rona et al., 2005). These potential risks need to be weighed against the possible benefits, most notably the facilitation of early intervention. Our results suggest that the discussion regarding the possible role for screening needs to broaden beyond consideration of only depression and PTSD symptoms. There is a solid evidence base to support the effectiveness of screening for alcohol misuse and brief interventions in primary care situations (US Preventive Services Task Force, 2004). Our findings related to the impact of cumulative trauma exposure also have important policy implications. While our finding of increasing rates of mental disorder among those with greater cumulative trauma exposure may not be surprising, previous studies had failed to find such an association (Meyer et al., 2012). The absence of such an association could have been interpreted to suggest that post-traumatic mental health problems only affected a group of vulnerable individuals and that once someone had experienced a certain number of traumatic events without developing mental health symptoms, they could be assumed to be resilient. Our results suggest this is not true; the risk of PTSD, depression and heavy drinking continued to increase at the same linear rate with each additional trauma exposure. Fire-fighters who had experienced more than 20 traumatic incidents involving fatalities had more than four times the rates of PTSD as less exposed fire-fighters and significantly increased levels of depression and heavy drinking. Any intervention, such as screening, aimed at high-risk groups must therefore consider the level of cumulative trauma exposure. Our results also raise questions as to whether emergency services should consider policies aimed at reducing the total cumulative trauma exposure, such as monitoring the number of incidents attended and moving individuals who reach a certain threshold into less intense situations. Such rotational policies are not without difficulty or risk, as there is good evidence for the importance of team cohesion and consistency in enhancing individual resilience (Iversen et al., 2008).
The causes of the markedly increased prevalence of mental disorders among retired fire-fighters are unclear. It may be that there are elements of emergency worker culture regarding mental health problems and alcohol use that allow unhelpful coping strategies to be carried into retirement. However, it is also possible that, as with retired military personnel, the loss of role, regular activity and reduction in support from their previous workplace play an important part (Harvey et al., 2011). The results of our post hoc analysis comparing the recently retired to those who have been retired for more than 5 years suggest that the increase in mental health symptoms is not a temporary response to the adjustment of retirement, but an ongoing state. As noted earlier, it may be speculated that retired personnel who responded to the survey were a self-selective group who had left the fire service because of mental health problems. Further investigation of the mental health of retired emergency workers, such as following a cohort from active service into the first few years of retirement, is clearly required. It may be that initiatives aimed at supporting the mental health needs of active-duty fire-fighters need to extend into retirement.
In summary, we have identified high levels of psychiatric morbidity among currently serving fire-fighters and particularly high rates of PTSD and depression among retired fire-fighters. Cumulative trauma exposure appears to be a key risk factor for mental disorder among this group, with increasing rates of PTSD, depression and heavy drinking with each additional traumatic exposure. Our findings have important implications for the ongoing debates surrounding screening of mental disorders in emergency workers and for policy considerations around the welfare of retired emergency workers.
Footnotes
Acknowledgements
We would like to thank Mark Howard and Fiona Kerin for their contributions to the study. R.A.B., R.K., H.M.P. and M.D. devised the study; H.M.P., E.L.H. and A.M.M. collected and organised the data; S.B.H. conducted the analysis of the data; and S.B.H. and J.S.M.-S. wrote the first draft of the manuscript. All authors contributed to the interpretation of the results, read and contributed to subsequent versions of this manuscript and approved the final version of this manuscript.
Declaration of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that they have no conflict of interest relevant to this paper, although one author (M.D.) is employed by Fire and Rescue New South Wales.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Australian Research Council Linkage Grant (LP0989719), which included financial and non-financial contributions from Fire and Rescue New South Wales. S.B.H. and J.S.M.-S. were supported by funding from New South Wales Health.