
Abstract
Objectives:
The aims of this study were to assess evidence for a novel, universal mental health literacy programme in the school setting (teen Mental Health First Aid) as an intervention to improve peer support towards adolescents at risk of suicide and to examine whether participation in a school-based programme dealing with suicide was distressing to participants.
Method:
In a cluster randomised crossover trial, Australian high school students aged 15–17 years (N = 1605, 44.74% female, Mage = 15.87) received either teen Mental Health First Aid or a matched control physical first aid course. Data were collected before, immediately after and 12 months after training through online surveys assessing correct recognition of suicidality and intentions to help a fictional peer (John) who was depicted as experiencing depressive symptoms and suicidal thoughts in a vignette. Students were also asked whether any information in the training or surveys was found distressing and completed a validated measure of psychological distress (the Kessler Psychological Distress Scale).
Results:
Students receiving teen Mental Health First Aid training were much more likely to report an increase from pre- to post-training in recognition of suicidality (OR = 1.97, 95% CI = [1.14, 3.39], p = 0.02) and appropriate first aid intentions towards a peer at risk of suicide than students receiving physical first aid (OR = 35.40, 95% CI = [19.86, 63.14], p < 0.001). Twelve months after training, most effects were still significant. Although a greater proportion of teen Mental Health First Aid participants self-reported feeling briefly distressed after the training, there was no evidence of greater distress at 12 months on the Kessler Psychological Distress Scale.
Conclusion:
teen Mental Health First Aid is effective in increasing recognition of and intentions to assist a suicidal peer. Although the open discussion of mental health first aid for a suicidal peer was distressing for some students, results suggest this was transient and not associated with harm. Future studies are required to ascertain whether these increases are indeed associated with better provision of support and prevention of youth suicide.
Background
Young people account for nearly one-third of the 800,000 people globally who die by suicide each year, with suicide a leading cause of death among 15- to 29-year-olds (Lee et al., 2019). Clearly, there is a critical need to address suicidality among youth, particularly as young people often do not seek or receive help for suicidal thoughts or behaviour (Calear et al., 2016). There have been many recent and evidence-based suggestions for population-level and health-system interventions to better prevent suicide in Australia (Atkinson et al., 2018; Horgan and Malhi, 2018; Jorm, 2019). However, schools offer an obvious opportunity for implementing suicide-prevention programmes, as they have huge potential for reach, for increasing capacity outside of the health setting, and for reducing some of the socio-cultural factors that are also known to influence suicide rates (Pridmore, 2018). Indeed, one recent review found a higher proportion of school-based suicide-prevention programmes were effective at reducing suicidal ideation and attempts than both community-based interventions and those delivered in healthcare settings (Calear et al., 2016).
Within the school setting, suicide-prevention programmes can be categorised into three forms, defined by the groups they target (Silverman and Maris, 1995). Universal programmes are designed to reach an entire school population and aim to enhance protective factors or reduce risk factors without needing to discern which individuals are at elevated risk. Selective interventions are targeted to those identified as being at risk of suicide. Finally, indicated programmes are designed for people who are already displaying suicidal behaviour, such as experiencing suicidal ideation or planning a suicide attempt. Within the school setting, universal interventions can be implemented more easily and more cost- and time-effectively than selective or indicated prevention programmes, which require screening (Jacobs et al., 1999). The opposite is true for prevention programmes based in the community or adult settings, where often cost effectiveness comes from selective or indicated interventions, and this risk-focused approach has recently been criticised as of ‘little impact’ (Jorm, 2019; Mulder, 2019). Furthermore, providing a whole school with an effective suicide-prevention programme is consistent with Rose’s Theorem and the idea that ‘a population-oriented approach is beneficial because it reduces the likelihood that more people will develop a large number of significant risk factors’ (Sher, 2019).
There is also evidence for the effectiveness of universal programmes over indicated and selective approaches in schools specifically. Researchers speculate that this may be due to higher levels of personal engagement with population programmes, as adolescents appear reluctant to accept screening and gatekeeper interventions (Wasserman et al., 2015) but are more amenable to universal programmes received by every student.
Indeed, universal interventions have consistently been found to be effective at improving knowledge of, attitudes towards and help-seeking for suicidal behaviour in young people (Cusimano and Sameem, 2011; Zalsman et al., 2016). While the best indicator of the efficacy of suicide programmes is a reduction in suicide-related outcomes (i.e. attempts and deaths), it is difficult to measure these relatively rare events, making the feasibility of well-powered randomised controlled trials (RCTs) particularly low (Isaac et al., 2009). A meta-analysis of gatekeeper training (Isaac et al., 2009) found that in two instances where population-level data on incident rates of suicide attempts and deaths could be linked with programme implementation, gatekeeper training was successful in increasing knowledge and improving attitudes while also leading to decreases in suicide-related outcomes. A more recent meta-analysis also found gatekeeper training to be associated with significantly reduced suicidal ideation among youth (Pistone et al., 2019).
By targeting mental health knowledge and attitudes, universal programmes (unlike targeted or selective interventions) are able to offer another avenue for suicide prevention: peer support. Teaching young people to recognise the warning signs for suicide, and empowering them to help their peers, capitalises on young people’s preference for seeking help from their friends (Jorm and Wright, 2007; Wright et al., 2005). Young people may be reluctant to seek help from a professional, and three in four young people report they would first turn to a friend for help if they were considering suicide (Michelmore and Hindley, 2012). If peers can be equipped with the skills and knowledge to recognise warning signs and get appropriate help for their friends, they can provide an opportunity for early detection and intervention when an adolescent is at risk of suicide.
Despite increasing evidence for the potential positive impact of universal interventions, concerns exist that such programmes could have potential iatrogenic effects. A 2013 systematic review noted the lack of robust evidence that suicide intervention programmes cause no harm, especially to already vulnerable students, such as those with existing mental health problems (Robinson et al., 2013). To date, there is a lack of research including measures of psychological distress before and after the implementation of suicide-prevention programmes, and until it is established that standalone universal suicide-prevention programmes do no harm, they should be grounded within broader mental health promotion activities (Robinson et al., 2013).
Currently, although effective suicide-prevention interventions do exist (Aseltine and DeMartino, 2004; Aseltine et al., 2007; Wasserman et al., 2015), there has not been a universal intervention to improve adolescents’ knowledge about and attitudes to suicide, which meets these criteria (i.e. embedded in a broader mental health literacy programme, with evidence of doing no harm), and which can be delivered feasibly and efficiently within a school setting.
This study examined the evidence for a novel, universal mental health literacy programme for adolescents in the school setting – teen Mental Health First Aid (tMHFA) – as an effective intervention to improve peer support towards adolescents at risk of suicide. Mental health first aid is defined as the help provided to someone who is developing or experiencing a worsening of a mental health problem or is experiencing a mental health crisis, such as suicidal ideation or behaviours. The first aid is provided until appropriate professional help is received or the crisis resolves (Kitchener et al., 2017). Mental health first aid training has been provided by Mental Health First Aid Australia (MHFA) since 2000 (Jorm and Kitchener, 2011) with courses for adults, including the Standard course (for adults assisting other adults; Kitchener et al., 2017), the Youth course (for adults assisting adolescents with mental health problems; Kelly et al., 2017) and adaptations for specific culturally and linguistically diverse groups (e.g. Hart et al., 2010). The core tenet of MHFA training is the teaching of a five-step action plan, in the same way that physical first aid (PFA) teaches the DRSABCD (Danger, Response, Send for help, open Airway, check for Breathing, start CPR, attach Defibrillator) emergency response action plan. A recent meta-analysis of 18 trials of MHFA training with adults found it effective in making attendees’ attitudes and behavioural intentions more helpful and supportive towards those with mental illness (Morgan et al., 2018).
tMHFA was developed in 2012 to meet the specific needs of adolescents in the upper high school years (Hart et al., 2016). It was created from a Delphi expert consensus study (Ross et al., 2012), designed to reduce known barriers to help-seeking among young people (Yap et al., 2011, 2013) and actively involved young people with lived experience in content design (Hart et al., 2016). The programme aims to increase mental health literacy, supportive behaviours towards peers with mental health problems or in mental health crises, and help-seeking from reliable and trusted adults, as well as reduce stigmatising attitudes. A cluster randomised crossover (CRXO) trial, which compared tMHFA to a PFA course of equivalent duration, found tMHFA to be effective in increasing supportive first aid intentions and mental health literacy in adolescents (Hart et al., 2018). tMHFA, therefore, offers a framework of proven benefits in the context of a broader mental health programme, which other universal, suicide-specific programmes may lack.
The current study analyses data gathered in the previously reported CRXO trial (Hart et al., 2018), but specifically examines the effects of the tMHFA programme on adolescents’ knowledge and intentions towards a peer at risk of suicide and any associated participant distress or evidence of iatrogenic harm. It was hypothesised that, compared to recipients of PFA training, recipients of tMHFA training would be (1) more likely to correctly recognise suicidality in a fictional vignette; (2) more likely to endorse adequate suicide first aid responses; (3) less likely to endorse negative or ‘harmful’ strategies such as ignoring the person because they are seeking attention; and (4) may report higher levels of transient distress associated with discussing how to support someone at risk of suicide in their course (as compared to discussing PFA; Jorm et al., 2007) but would not report ongoing psychological distress associated with the course.
Methods
The descriptions below follow the CONSORT 2010 statement and extension for cluster randomised control trials (Campbell et al., 2012). They refer to the aspects of the trial design and methodology relevant to the aims of this study, but full details can be found in Hart et al. (2018).
Trial design
A CRXO trial was undertaken, with schools defining clusters. CRXO is a refinement of the matched-pair cluster design; in CRXO trials, all clusters receive all interventions with the sequence of administration being randomly assigned. With two interventions, two distinct waves of participants (i.e. student grade level cohorts) undertake the separate trial conditions (Giraudeau et al., 2008; Turner et al., 2007)
This research was registered with the Australian New Zealand Clinical Trials Registry (ANZCTRN12614000061639) and had ethics approval from the University of Melbourne Human Research Ethics Committee (HREC1341238) and the State Government Education Department for Victoria (No. 2014_002268).
Participants
Eligible students were recruited from four participating government-funded secondary schools in the greater metropolitan area of Melbourne, Australia. To recruit schools, the research team emailed a request to all accredited Youth MHFA instructors in the Melbourne area asking for an introduction to any secondary schools with an expressed interest in receiving training for staff and students. Two schools agreed to participate through this mechanism, with a further two schools selected for matched demographic variables: Index of Community Socio-Educational Advantage (ICSEA; M = 1000, SD = 100) and Year 10 cohort size in the first year. Schools were required to be within 1 SD on ICSEA and within 100 students in size. Schools were blinded to condition until enrolment and randomisation to intervention order had taken place. Randomisation was completed by our statistician blinded to school identity.
Details of the sociodemographic characteristics of the four schools are given in Table 1. Of the 1942 10th grade students who were eligible to participate, 1605 returned analysable data before the training, 1116 returned data immediately after and 894 returned data 12 months after training. Hence, attrition from baseline to post-training was 30% and from baseline to 12-month follow-up was 44%.
Participant characteristics by school and intervention.
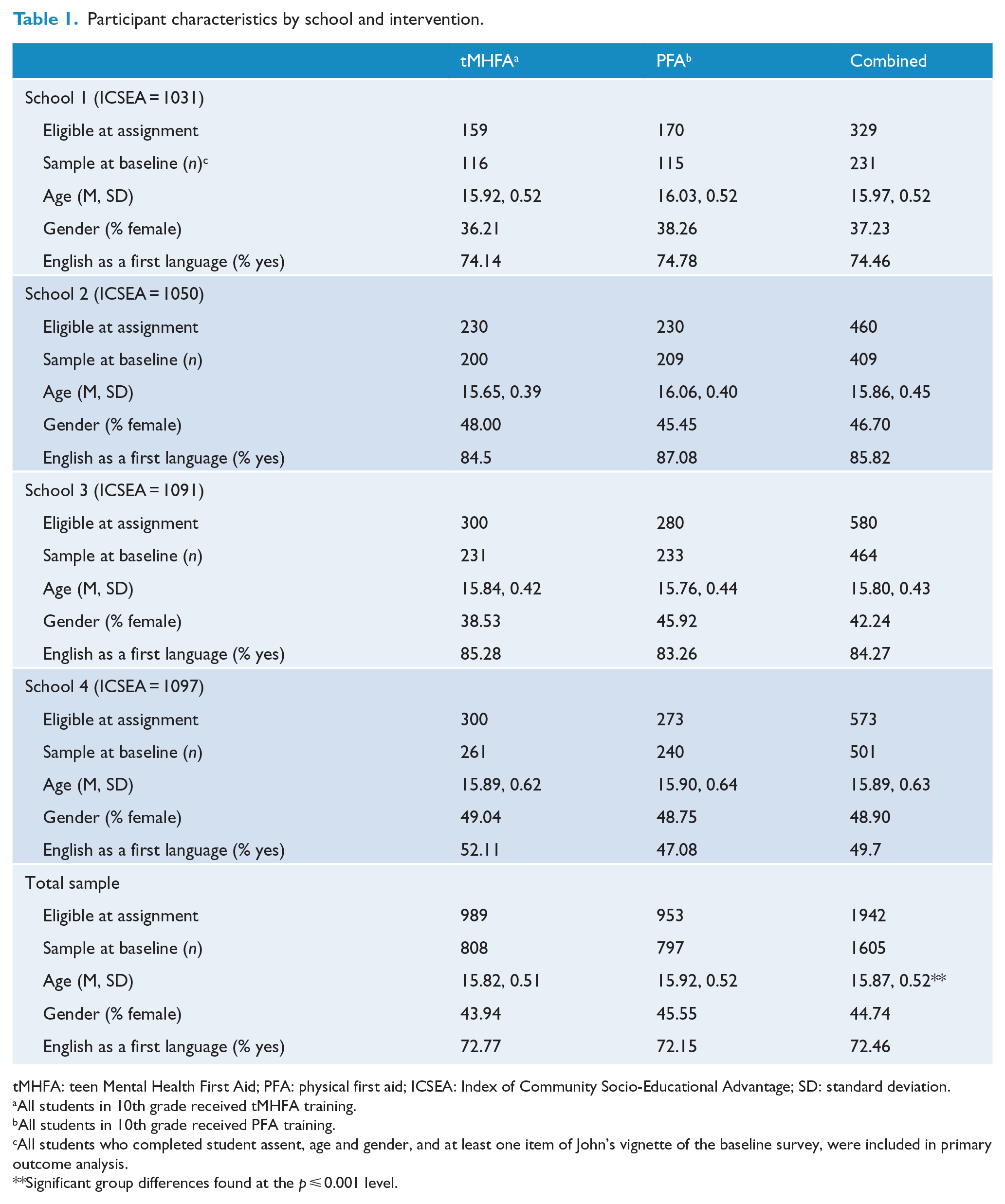
tMHFA: teen Mental Health First Aid; PFA: physical first aid; ICSEA: Index of Community Socio-Educational Advantage; SD: standard deviation.
All students in 10th grade received tMHFA training.
All students in 10th grade received PFA training.
All students who completed student assent, age and gender, and at least one item of John’s vignette of the baseline survey, were included in primary outcome analysis.
Significant group differences found at the p ⩽ 0.001 level.
To be eligible, schools needed to be willing to withhold any overlapping mental health classroom programmes until the completion of the research and agree to two consecutive cohorts of 10th grade students undertaking survey sessions and three training sessions in regular class time. The only exclusion criterion was having provided a mental health intervention designed to increase mental health literacy or help-seeking to the current 9th or 10th grade cohorts over the previous 2 years. Students were eligible to participate if they had parental consent and provided assent at the beginning of each survey. Passive parental consent was used. The research team provided parent, teacher and student information sessions, as well as electronic and hardcopy information statements, 3 weeks prior to baseline measures. Parents could opt their child out of the training or evaluation by returning a signed form to the participating school. No data were gathered on non-consenters. Assent was also sought from students at the time of data collection.
Interventions
Both interventions consisted of three 75-minute classroom sessions presented by trained external instructors according to a manualised curriculum. In each intervention, students were provided with a specific programme booklet and completion certificate. Session content is provided in Table 1. Training was normally completed within 3 weeks (one session per week).
tMHFA
A detailed explanation of the tMHFA programme can be obtained elsewhere (Hart et al., 2016), but relevant details are noted in Table 2. Training involved a PowerPoint presentation, videos, role-plays, group discussion, small group and workbook activities (Hart et al., 2012). In particular, Session 2 focused on teaching the skills to help a friend in a mental health crisis and included a video depicting a teenager experiencing thoughts of suicide and group discussions about helping someone who is suicidal, and about confidentiality versus safety.
Structure and content of first aid interventions.
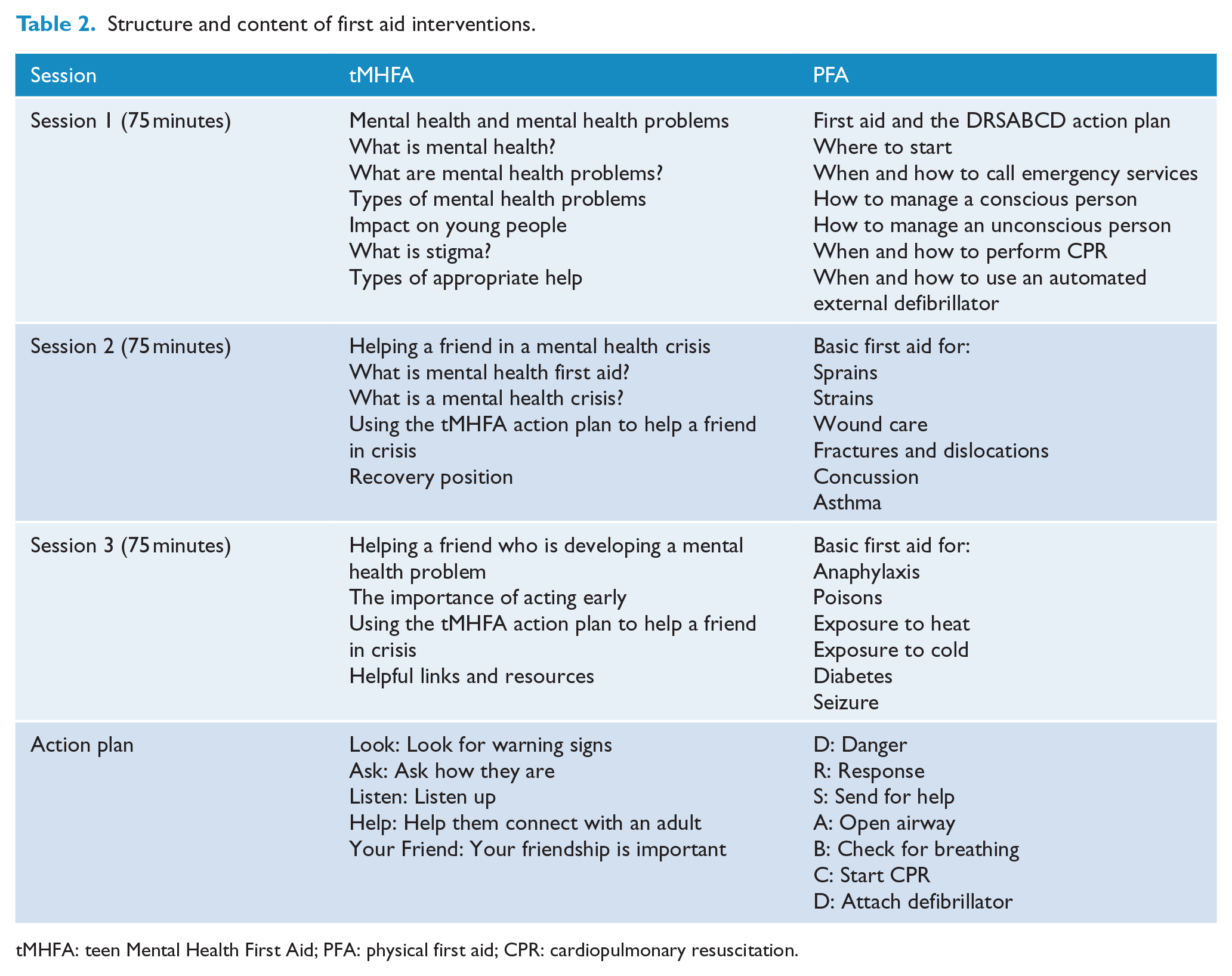
tMHFA: teen Mental Health First Aid; PFA: physical first aid; CPR: cardiopulmonary resuscitation.
PFA
PFA training involved introductions of topic content, role-plays using mannequins, bandages and splints, and group discussions (see Table 2).
Measures
The student questionnaire included items adapted from the Australian National Survey of Youth Mental Health Literacy (Yap and Jorm, 2012), which related to a vignette of an adolescent depicted as experiencing depression with suicidal ideation (John). The vignette is provided in Table 3.
Vignette used to assess recognition of suicidality, quality of suicide first aid intentions, and unhelpful peer intentions.
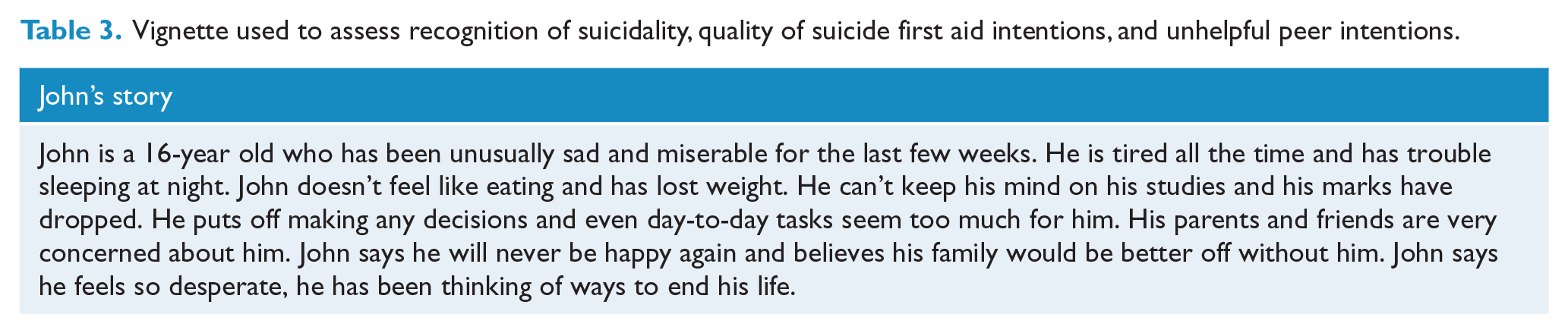
Recognition of suicidality was assessed with the single item: ‘What, if anything, do you think is wrong with John?’. Responses were open-ended, and resulting data were coded by a researcher blind to cluster and period and in accordance with a structured protocol whereby students scored 1 point for any reference to suicide (including ‘wants to die’, ‘wants to end his life’, ‘is thinking of killing himself’ and ‘doesn’t want to live’; Mason et al., 2015).
Adequate suicide first aid responses were measured through four items, in accordance with Delphi expert consensus studies on mental health first aid for the suicidal person and the teachings of the tMHFA course (Hart et al., 2012; Kelly et al., 2008). After reading the vignette, students were also asked the following question: ‘If John was a friend, I would …’. Students were then presented with 12 forced-choice options, of which they could select multiple responses. Six of these responses were designed to be concordant with the teachings of the tMHFA action plan; the remaining six were discordant (Hart et al., 2016; Mason et al., 2015). The following options were considered the minimum required responses for providing adequate first aid to someone at risk of suicide: (1) Ask John if he is thinking of suicide; (2) Tell John I have noticed something is wrong, and I want to make sure he is okay; (3) Suggest John tell a health professional about his problems (e.g. a counsellor, general practitioner [GP] or psychologist); and (4) Suggest John tell an adult (other than a health professional) about his problems (e.g. a parent or teacher). Students needed to endorse both Items 1 and 2, but either of Items 3 or 4, as these represented equally satisfactory responses as taught by the tMHFA programme. The proportion of students reporting adequate suicide first aid responses was then compared before and after receiving training, for students in both the intervention and the control groups.
The following two response options were considered negative or ‘harmful’ first aid strategies: (1) Ignore John because he is attention-seeking and (2) Avoid talking about suicide, because it might put the idea in John’s head. The proportion of students reporting either of these responses was compared over time and across groups.
Students’ psychological distress was measured in two ways. First, psychological distress over the past 4 weeks was measured using The Kessler Six-Item Psychological Distress Scale (K6; Kessler et al., 2002) administered at baseline and at 12-month follow-up. To examine any deterioration in psychological distress, a reliable change index was calculated based on statistics at baseline (SD = 5.35 and Cronbach’s α = 0.88). The reliable change criterion was calculated to be 5.17, indicating that any increase or decrease greater than 5.17 could be regarded as reliable. The proportion who reported a reliable deterioration between baseline and 12-month follow-up was then examined across intervention groups.
Second, transient distress arising from having completed either the tMHFA or the PFA course was measured through the following item in the post-training survey: ‘Did any of the information provided in the program make you feel distressed (e.g. sad, stressed, overwhelmed, nervous or depressed)?’. Response options were ‘no’, ‘not sure’ and ‘yes’. Those who answered ‘no’ were skipped to the next section. Those responding ‘yes’ or ‘not sure’ were then asked a series of subsequent questions about their distress. To determine whether the suicide-related content of the tMHFA course led to their distress, students were asked the open-ended item ‘please describe what in particular made you feel distressed’. Resulting data were coded in accordance with a structured protocol whereby responses were coded by reference to suicide-related content; mental health problem–related content (non-suicide); course content or materials generally; lack of confidence in applying learnings; instruction; no distress; and non-specific. All data were coded by one researcher, but the second researcher also coded a random sample of 30 items representing each of the seven possible codes. Both were blind to condition, and Cohen’s kappa ranged from 1 (perfect agreement; for all but three codes) to 0.63, indicating substantial agreement.
Participants were then asked, ‘if you felt distressed, would you say that it was still worthwhile attending the First Aid program?’ (with responses on a five-point Likert-type scale from ‘yes definitely’ to ‘definitely not’) and ‘how long did the distressed feeling last for?’ (choice of ‘a few moments’, ‘a few hours’, ‘a few days’ and ‘a week or more’).
Statistical analysis
Mixed-effects models were used for analysing binary outcome variables, including group-by-measurement-occasion interactions, taking into account the hierarchical structure (Rabe-Hesketh and Skrondal, 2012). All models included a random effect for student cohort (period-clusters) and fixed effect for school (cluster), year (period), and student age and gender to accommodate possible non-independence of student responses in cohorts. Gender and age were found to be associated with missingness, with older boys being less likely to provide data at follow-up, and were thus included as fixed effects in order to help meet the missing at random assumption. Analyses were performed in Stata 14 (StataCorp, 2015).
Statistical power
It was conservatively estimated that there would be 100 10th grade students per school, with a 50% consent and assent rate. Across four schools and eight clusters, this would give 400 adolescents (200 per intervention). The estimated intra-class correlation for students (ICC = 0.003) at the school cluster level was based on findings from previous research (Hart et al., 2016) and not included in the power calculations due to the likely small design effect and the counterbalancing of schools. With an assumed 0.70 correlation between pre- and post-measurements, the study would have a 0.80 power to detect small (d = 0.17) group-by-measurement-occasion differences at α = 0.05.
Results
The proportion of students who correctly identified suicidality in John’s vignette, across baseline, post-training and 12-month follow-up measurement occasions, is shown in Table 4. Recognition of suicidality was low at baseline (10% PFA, 11% tMHFA) with few students labelling John’s problem as related to suicide. At post-training, this increased to over 16% among students receiving tMHFA, but among those receiving PFA training, it dropped to 9%. Among the tMHFA students 12 months later, the proportion recognising suicidality dropped (to 13%), but still remained significantly higher than the proportion in the PFA group (8.6%). When comparing the change in recognition of suicidality from baseline to post-training, the tMHFA students were significantly more likely to report an increase than the PFA students (OR = 1.97). When comparing the change in recognition of suicidality from baseline to 12-month follow-up, the difference between the two groups was no longer statistically significant (OR = 1.50).
Proportion of students in each training intervention group reporting correct recognition of suicidality, adequate suicide first aid and avoidance of talking about suicide, over three survey measurements.
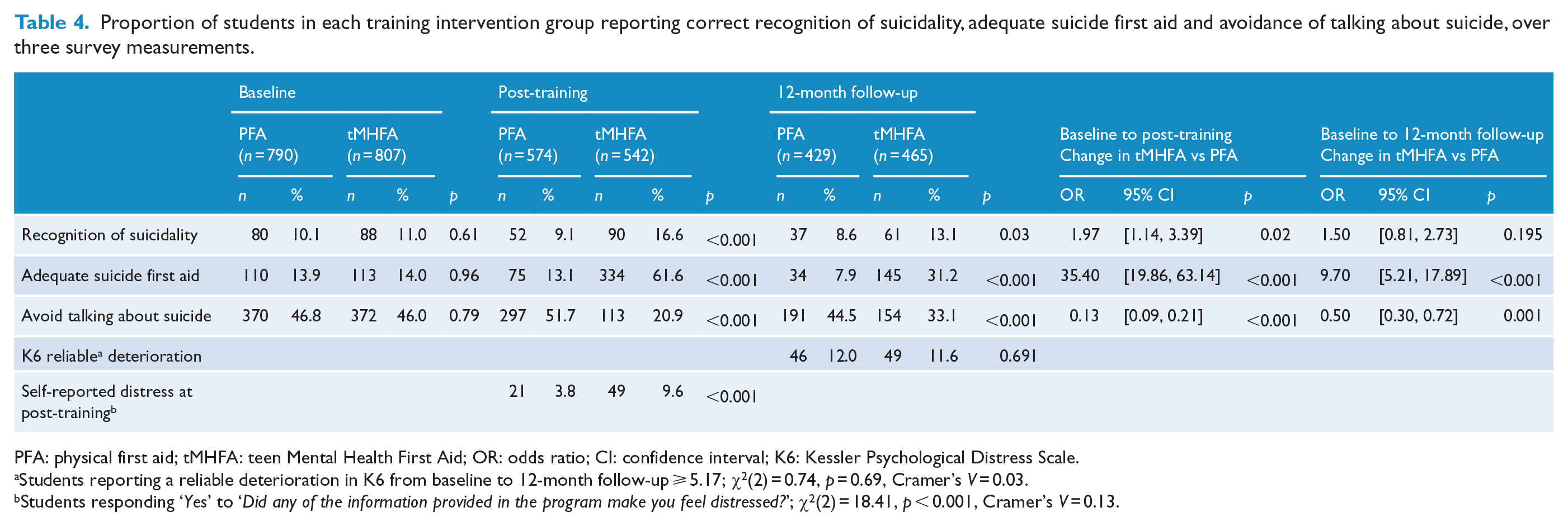
PFA: physical first aid; tMHFA: teen Mental Health First Aid; OR: odds ratio; CI: confidence interval; K6: Kessler Psychological Distress Scale.
Students reporting a reliable deterioration in K6 from baseline to 12-month follow-up ⩾ 5.17; χ2(2) = 0.74, p = 0.69, Cramer’s V = 0.03.
Students responding ‘Yes’ to ‘Did any of the information provided in the program make you feel distressed?’; χ2(2) = 18.41, p < 0.001, Cramer’s V = 0.13.
The proportion of students reporting adequate suicide first aid responses is also shown in Table 4. At baseline, just 14% of students (in both groups) reported the three required first aid responses of ‘ask about suicide’, ‘tell John you noticed something is wrong and want to make sure he is okay’ and ‘suggest John tell an adult’. At post-training, 62% of students receiving tMHFA reported adequate suicide first aid, while just 13% of students receiving PFA did so. The odds of a student in the tMHFA group reporting adequate first aid at post-training, compared to baseline, was 35 times higher than the odds of a student in the PFA group reporting adequate first aid at post-training. Although weakened, these results were still significant 1 year later. The percentage of tMHFA students who responded with the three appropriate first aid intentions reduced to 31% at 12-month follow-up, while the percentage of PFA students also dropped to 9%. The odds of tMHFA students increasing their adequate first aid responses from baseline to 12-month follow-up were nine times higher than for students receiving PFA.
The negative or harmful response ‘ignore John because he is attention seeking’ was only endorsed by a very small minority of the total sample: just 33 students (2%) at baseline endorsed this option. Because the numbers for this variable were so low and participant attrition at subsequent measurement occasions reduced the sample further, this item was removed from further analyses. The negative or ‘harmful’ first aid strategy of ‘avoid talking about suicide, because it might put the idea in John’s head’ was much more broadly endorsed at baseline, with 46% of students selecting this response (see Table 4). At post-training, this proportion had significantly decreased among the students receiving tMHFA (21%) and significantly increased among students receiving PFA (52%). At 12-month follow-up, the change in these student proportions was smaller than at post-training, but still apparent in comparison with baseline (tMHFA 33%, PFA 44%). The odds of tMHFA students showing a reduction in ‘avoid talking about suicide’ from baseline to post-training were significantly higher than the odds of PFA students showing a reduction (OR = 0.13), and this was also true when examining the change from baseline to 12-month follow-up (OR = 0.50).
When asked in the post-training survey whether any of the information in the training had made them feel distressed, a significantly higher proportion of students receiving tMHFA said ‘yes’ (10%) than those receiving PFA (4%). Responses to the subsequent questions about the nature and duration of the distress are provided in Table 5. The majority of those students who reported feeling distress, in both the tMHFA and the PFA intervention groups, also reported that they felt attending the training was still worthwhile (51% tMHFA, 71% PFA). In addition, the majority of students across both interventions reported that the distress was short-lived – from a few moments to hours (tMHFA 80% of those reporting distress, PFA 85% of those reporting distress). There were no significant differences between the tMHFA and the PFA groups on these measures. The main reasons for distress, given in the open-ended responses among the tMHFA group, were the course content or materials generally (n = 15/45, 33%, e.g. ‘The videos’ and ‘it just made me sad thinking about all the people who need help’) and suicide-related content (n = 13/45, 29%, e.g. ‘The videos were very depressing, the teenage boy thought about suicide which made the story very sad’ and ‘the part about suicide’). Another key response was content relating to other mental health problems, whether students referenced these problems in themselves, others or did not specify (n = 10/45, 22%, e.g. ‘I think I might have something similar’ and ‘I am struggling with mental illnesses at the moment so the realness of it’). In the PFA group, the most common reason given for distress was the course content or materials generally (n = 8/17, 47%, e.g. ‘How many people die each year because of accidents and diseases made me feel distressed’ and ‘the information about the broken and dislocated bones’), followed by students who reported personal experience of first aid scenarios (n = 3/17, 18%, e.g. ‘Needles cause I don’t like them and talking about seizures reminded me of my sister’ and ‘putting an epi-pen put into me because I have one’).
Answers to subsequent questions among students reporting feeling distressed as a result of receiving their first aid training (post-training survey).
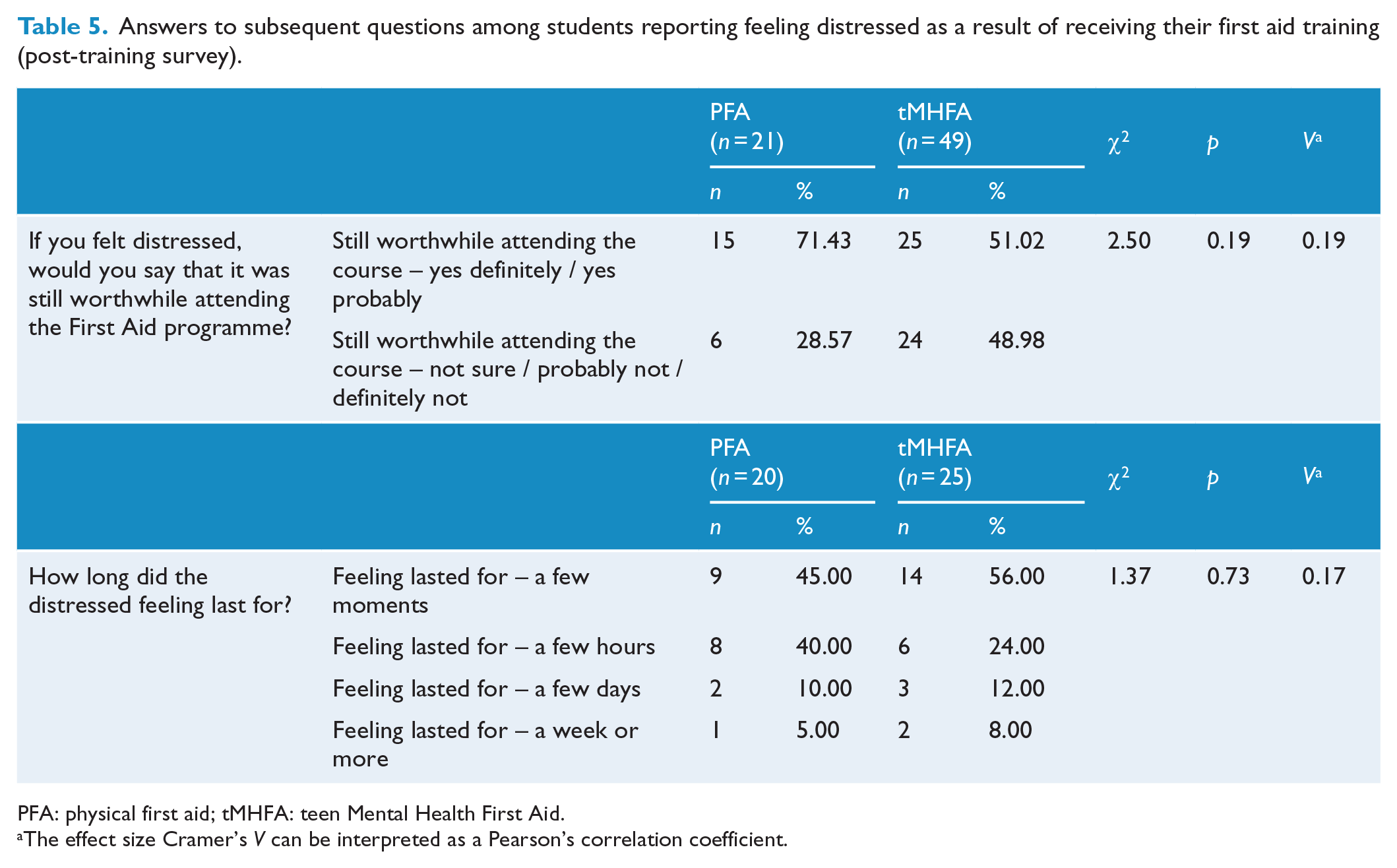
PFA: physical first aid; tMHFA: teen Mental Health First Aid.
The effect size Cramer’s V can be interpreted as a Pearson’s correlation coefficient.
At the two timepoints where the K6 was administered (baseline and 12 months), 421 tMHFA students and 382 PFA students provided data. The median change in scores was 0, though the mean change for tMHFA students was 0.23 (SD = 4.93) and for PFA students was 0.26 (SD = 4.76), indicating that both groups showed slight mean increases in psychological distress over the year. Results comparing the proportion of students reporting a reliable deterioration are shown in Table 4. Twelve percent of students in both groups reported a reliable deterioration in K6 scores, and hence there were no statistically significant differences across the training conditions.
Discussion
This study examined the outcomes from a CRXO trial to assess evidence for tMHFA as an effective intervention to improve peer support towards adolescents at risk of suicide and the impact of providing this universal mental health literacy intervention on students’ psychological distress. Results suggest that students receiving tMHFA were indeed more likely to recognise, and much more likely to appropriately respond to, a peer at risk of suicide. tMHFA students were 35 times more likely to report adequate suicide first aid after receiving their training, than students receiving PFA, and this significant effect was sustained 1 year later. Furthermore, although the tMHFA programme was associated with more participant-reported distress immediately after the training, it was not associated with greater levels of distress as measured by the K6 at 12-month follow-up, indicating that the distress reported by students was transient and not associated with long-term harm. This was also corroborated by student responses indicating distress most often lasted from a few moments to a few hours.
The results at post-training indicated that the proportion of tMHFA students reporting adequate first aid (62%) was much higher than the proportion who correctly recognised and labelled suicidality in the vignette (17%). This suggests that accurate problem recognition is not as important as the willingness to just ask someone if they are thinking about suicide, as twice as many students reported this intention to help John, without having labelled John’s problem as related to being suicidal. Given the tMHFA programme encourages adolescents to look for general warning signs of mental health problems in peers, rather than specific symptom profiles, and then to ask the peer directly if they are thinking about suicide, these results are perhaps not surprising. In addition, as previously noted in the report on broad trial outcomes from baseline to post-training (Hart et al., 2018), when correct recognition of John’s problem was coded as any reference to depression or suicidality, recognition was indeed very high among both groups (baseline: PFA = 79%, tMHFA = 74%; post-training: PFA = 80%, tMHFA = 77%; OR = 1.18, 95% CI = [0.71, 1.96], p = 0.528). Together, these findings suggest that recognition is high for depressive symptoms, appears more wanting for suicidality, yet adequate first aid intentions do not appear dependent on recognition of suicidality. Given that asking a person directly if they are thinking about suicide is the most accurate way to discern suicide risk, we think the findings of the current study add weight to arguments for embedding suicide-prevention information within universal mental health literacy programmes, as increasing peer support for and openness to discussing mental health problems generally is likely more effective than specific knowledge relating to suicidality in particular. Future research could examine whether tMHFA proves more efficacious in suicide prevention than specific interventions focused on increasing suicide literacy alone.
This study adds important evidence to the very limited number of RCTs evaluating suicide-prevention programmes while examining potential harms (Robinson and Pirkis, 2013). These results provided no evidence of lasting psychological distress associated with the programme, and no adverse outcomes were reported by any schools, students or parents associated with the trial. Indeed, the CRXO design provides high-quality evidence that the tMHFA programme has a positive impact on intentions to provide supportive first aid actions towards a peer at risk of suicide, without unintended harms. This suggests that the tMHFA programme promotes action to prevent suicide while also equipping students to better understand mental health problems in adolescents, decrease barriers to care and increase supportive behaviours towards peers. However, it remains a limitation of this study that we were unable to monitor suicide attempts and completions in our participating schools, though this is planned for future research.
Although successful in increasing suicide literacy in the current trial, the tMHFA training only managed to raise the proportion of students reporting adequate first aid for suicide to 61% at post-training, and 31% a year later. This suggests that the dose may not yet be adequate and perhaps simple booster sessions, such as online modules or opportunities in class to practice first aid scenarios and enact the action plan, could assist with ongoing re-learning and retention of behavioural intentions. There is also growing evidence for the efficacy and acceptability of online interventions among young people (Robinson et al., 2018; Witt et al., 2017). Clearly, further research is required to understand how programme effects might be improved.
Limitations of this study include the significant student attrition from baseline to 12-month follow-up and the lack of fidelity measures. Despite an almost halving of the sample at follow-up, the results reported here are unlikely to be strongly biased by sample attrition; the conservative mixed-effects modelling including intention-to-treat principles produces unbiased estimates under the missing-at-random assumption, and despite attrition, the remaining sample was of a sufficient size to provide ample statistical power. No fidelity measures were implemented in this study due to constraints on research staffing levels and budget allowances for instructor time. However, the main teaching points in Session 2, which focussed on suicide first aid in particular, were the film portraying a first aid scenario and the five-step action plan outlined in the PowerPoint slides. Both of these programme components are highly likely to have been presented, as they form the basis for further activities and discussion points. Future research should, however, assess the impact of instructor fidelity on student outcomes. Strengths of this study include the large sample, robust cluster crossover design and multiple measures of student distress. Outcomes from this study would be augmented by future qualitative follow-up, gaining data on actual first aid provided or received, and whether these interventions reduced suicide risk among peers. Pending these outcomes, the tMHFA programme could be integrated into a comprehensive population-level initiative (Schaffer and Sinyor, 2019) to reduce death by suicide through the implementation of multiple upstream levers, such as better prompting to help-seeking and social support from peers.
Conclusion
tMHFA is a novel programme to train senior secondary students in how to recognise and support a peer who is at risk of suicide. This high-quality CRXO trial showed that tMHFA is effective in increasing knowledge and skills in assisting a suicidal peer. Although the tMHFA programme was associated with a higher level of participant-reported distress immediately after the training, as compared to the matched PFA control condition, tMHFA was not associated with any ongoing or long-term harm, suggesting its feasibility as a population-level suicide-prevention programme for schools. Although this research provides very promising results, future studies are required to ascertain whether these increases in suicide literacy indeed lead to improvements in the provision of first aid and the prevention of suicide among young people.
Footnotes
Acknowledgements
This research was registered with the Australian New Zealand Clinical Trials Registry (ANZCTRN12614000061639).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: A.F.J. is on the Board of Directors of Mental Health First Aid International (trading as MHFA Australia). C.M.K. is an employee of Mental Health First Aid International. The authors will not benefit financially or otherwise from the publication of this research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was funded by a Mental Health Research Grant awarded to the authors by Australian Rotary Health, a National Health and Medical Research Council Fellowship awarded to A.F.J. and an Australian Rotary Health Post-doctoral Fellowship awarded to L.M.H. These sponsors had no role in the study design; the collection, analysis and interpretation of data; the writing of the report; or the decision to submit the manuscript for publication.