
Abstract
Objective:
Despite considerable morbidity and functional losses associated with adolescent borderline personality disorder, little is known about psychopathological outcomes. This study examined associations between adolescent borderline personality disorder symptoms and subsequent depressive, psychotic and hypomanic symptoms.
Methods:
We used data from the Avon Longitudinal Study of Parents and Children. Participants were adolescents living in the community who had data for all longitudinal outcomes (N = 1758). We used logistic regression and path analysis to investigate associations between borderline personality disorder (five or more probable/definite symptoms) reported at age 11–12 years and depressive and psychotic symptoms reported at age 12 and 18, and lifetime hypomanic symptoms reported at age 22–23 years.
Results:
Adolescent borderline personality disorder symptoms were associated with psychotic symptoms (odds ratio: 2.36, confidence interval: [1.82, 3.06]), diagnosis of depression at age 18 years (odds ratio: 1.30, confidence interval: [1.03, 1.64]) and hypomanic symptoms (odds ratio: 2.89, confidence interval: [2.40, 3.48]) at 22–23 years. Path analysis controlling for associations between all outcomes indicated that borderline personality disorder symptoms were independently associated with depressive symptoms (β = 0.97, p < 0.001) at 12 years and hypomanic (β = 0.58, p < 0.01) symptoms at 22–23 years. Borderline personality disorder symptoms were also associated with psychotic symptoms at age 12 years (β = 0.58, p < 0.01), which were linked (β = 0.34, p < 0.01) to psychotic symptoms at age 18 years.
Conclusion:
Adolescents with borderline personality disorder symptoms are at future risk of psychotic and hypomanic symptoms, and a diagnosis of depression. Future risk is independent of associations between psychopathological outcomes, indicating that adolescent borderline personality disorder symptoms have multifinal outcomes. Increasing awareness of borderline personality disorder in early adolescence could facilitate timely secondary prevention of these symptoms subsequently, helping to prevent future psychopathology.
Keywords
Introduction
Borderline personality disorder (BPD) is a common and serious mental disorder with community prevalence ranging from 0.7% to 1.8% (Lieb et al., 2004; Winsper et al., 2019). The validity and clinical importance of adolescent BPD is increasingly recognized (Sharp and Fonagy, 2015; Winsper et al., 2016a). Indeed, BPD may be better conceptualized as a youth disorder, arising in early adolescence and then slowly declining from young adulthood onwards (Chanen et al., 2014). Adolescents with BPD are common among help-seeking populations. Adolescent BPD is reported in up to 11% of psychiatric outpatients (Chanen et al., 2004) and 33–49% of psychiatric inpatients (Chanen et al., 2014; Grilo et al., 1998). These individuals often experience long-term social, educational, work and financial impairment and have a substantial need for healthcare (Winsper et al., 2015). Nevertheless, our understanding of the outcomes of adolescent BPD remains rudimentary.
Our previous systematic review indicated a limited number of prospective studies investigating links between adolescent BPD and subsequent psychopathology (Winsper et al., 2015). Existing studies are limited by methodological problems. Clinical studies are confounded by treatment effects and the sampling of individuals with severe psychopathology. Community studies are restricted by the lack of validated, structured assessment tools specifically designed to screen for adolescent BPD, and moderate sample sizes limiting power for detecting specific diagnostic or subsyndromal-level associations (Cohen et al., 2007). Some community studies tend to focus on high-risk populations, e.g. oversampling for conduct disorder (Stepp et al., 2012), or are focused on twin populations (Belsky et al., 2012). Furthermore, few studies have controlled for earlier life experiences (e.g. abuse), which have been found to link to later psychopathology (Jaffee, 2017). Another major issue is that the extant literature primarily focuses on associations between adolescent BPD and future personality disorders (Chanen et al., 2004; Lofgren et al., 1991), anxiety and depression symptoms (Johnson et al., 1999; Wenning, 1990), substance misuse (Cohen et al., 2007) and self-harming behaviours (Johnson et al., 1999). There is very limited evidence examining associations with subthreshold or threshold psychotic (Thompson et al., 2012) or bipolar spectrum disorders. These omissions need to be addressed as psychotic symptoms are relatively common in adult BPD (Kaess et al., 2014) and concurrent comorbidity between BPD and bipolar disorder is approximately 25–30% (George et al., 2003). Finally, previous studies have not simultaneously modelled pathways between BPD and multiple psychopathological outcomes, despite the known high levels of comorbidity between psychopathologies (Winsper et al., 2016a). Such an approach is now needed to determine whether associations represent independent links between adolescent BPD symptoms and subsequent psychopathologies, or whether such associations are an artefact of symptom overlap.
Aims
We bridge these gaps in the literature by addressing the following questions:
Are BPD (five or more probable/definite) symptoms in early adolescence associated with subsequent depressive (reported at 12 and 18 years), psychotic (reported at 12 and 18 years) and lifetime hypomanic (reported at 22–23 years) psychopathology following adjustment for early environmental risks?
Are the associations between BPD symptoms and psychopathology reported in late adolescence/early adulthood (i.e. 18 and 22–23 years) significantly mediated by psychopathological symptoms in early adolescence (i.e. 12 years)?
Methods
Sample
The Avon Longitudinal Study of Parents and Children (ALSPAC) is a UK birth cohort study examining the determinants of development, health and disease during childhood and beyond. The study is described in detail elsewhere (Boyd et al., 2013). ALSPAC recruited pregnant women in Avon with expected dates of delivery between the 1 April 1991 and 31 December 1992. A total of 14,541 pregnant women were initially enrolled in the study and had returned at least one questionnaire or attended a ‘Children in Focus’ clinic by 19 July 1999. Out of the initial 14,541 pregnancies, all but 69 had known birth outcome. These 14,472 pregnancies yielded 14,676 foetuses in the initial sample. Of these, 14,477 were singleton, 195 were twin, 3 were triplet and 1 was quadruplet. There were 14,062 live births, of which 13,988 children were alive at 1 year of age (see Figure 1 for the flowchart of sample numbers at each stage of the study). When the oldest children were approximately 7 years old, the sample was bolstered with eligible cases who had failed to join the study originally. Consequently, when considering variables collected from the age of 7 onwards, there are data available on 14,701 children (an additional 713 children). The study website contains details of the data available through a fully searchable data dictionary (www.bris.ac.uk/alspac/researchers/data-access/data-dictionary/). From the first trimester of pregnancy, parents completed postal questionnaires about the study child’s health and development. The child attended annual assessment clinics, including face-to face interviews and psychological and physical tests. Ethical approval for the study was obtained from the ALSPAC Law and Ethics Committee and the local research ethics committees.
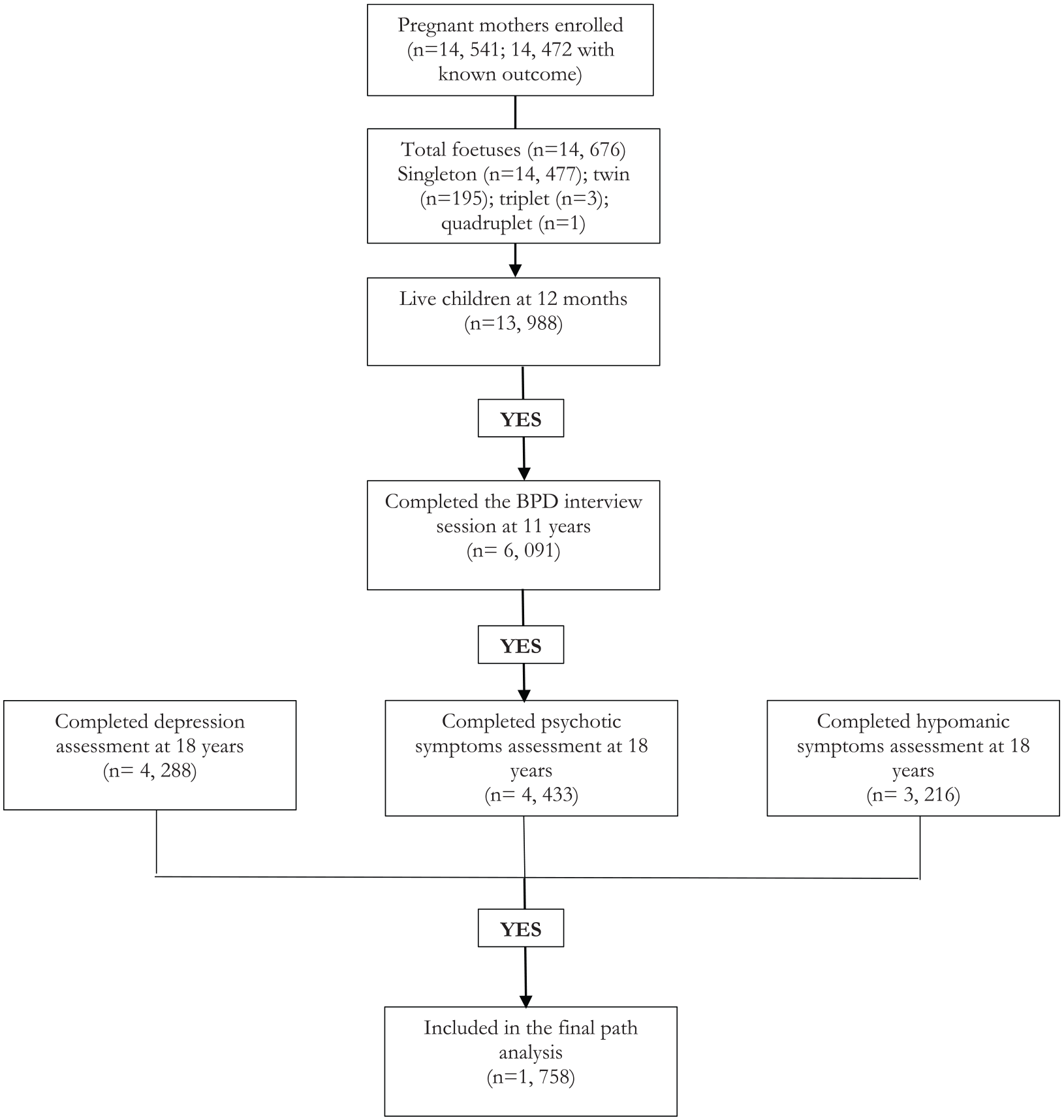
Flow diagram detailing numbers of participants who completed key follow-up assessments during the Avon Longitudinal Study of Parents and Children (ALSPAC).
Assessments
BPD symptoms at 11–12 years
Adolescents were interviewed to assess BPD symptoms over the past 2 years. Trained psychologists used a face-to-face semi-structured interview: the UK Childhood Interview for DSM-IV Borderline Personality Disorder [UK-CI-BPD] (Zanarini et al., 2004). The UK-CI-BPD was adapted from the US version of the CI-BPD and both are based on the module for BPD in the Diagnostic Interview for DSM-IV Personality Disorders. The inter-rater and test–retest reliability of the Diagnostic and Statistical Manual of Mental Disorders (3rd ed.; DSM-III), Diagnostic and Statistical Manual of Mental Disorders (3rd ed.; rev., DSM-III-R) and Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) versions of this measure are good to excellent (Zanarini and Frankenberg, 2001). In a test of convergent validity, the CI-BPD diagnosis was significantly associated with clinician diagnosis (kappa = 0.34, p < 0.001), and other measures of BPD (i.e. Borderline Personality Features Scale, Personality Assessment Inventory – Borderline subscale) reported by patients and parents (Sharp et al., 2012). The inter-rater reliability of the UK-CI-BPD within the current sample ranged from 0.36 to 1.0 (median: 0.88); 86% of the kappa values were within the excellent range of >0.75 (Zanarini et al., 2011).
Consistent with the DSM-IV and Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) Section II conceptualizations of BPD, the UK-CI-BPD covers nine symptoms: intense inappropriate anger; affective instability; emptiness; identity disturbance; paranoid ideation; abandonment; suicidal or self-mutilating behaviours; impulsivity and intense unstable relationships. Each symptom was rated as absent (score = 0), probably present (score = 1) or definitely present (score = 2). Definitely present refers to very frequent occurrence (daily or at least 25% of the time), and probably present refers to repeated but not very frequent occurrence. As in previous studies (Winsper et al., 2015), we constructed a dichotomous BPD symptom variable. Participants were assigned a positive status if they scored 1 or 2 on five or more of the DSM-IV diagnostic criteria. This symptom threshold (i.e. five or more symptoms) is consistent with the current DSM-5 diagnosis of BPD (American Psychiatric Association, 2013). However, we lowered the frequency threshold to include the repeated (score of 1) and very frequent (score of 2) occurrence of each symptom to ensure that sufficient positive cases were identified in our community sample. Therefore, our BPD assessment is more sensitive than current clinical diagnosis.
Depressive symptoms at 12 years
Child-reported depressive symptoms over the past 2 weeks were assessed using the Short Mood and Feelings Questionnaire (SMFQ). The SMFQ is a 13-item scale (items on a three-point scale) with high validity and reliability (Zwierzynska et al., 2013). Responses to items (no = 0; sometimes = 1; true = 2) were summed yielding a maximum score of 26 points. The total score for each participant was collapsed into a dichotomous variable (threshold score ⩾ 11), with higher scores consistent with clinically relevant levels of depressive symptoms (Zwierzynska et al., 2013).
Psychotic symptoms at 12 years
Psychotic symptoms were assessed with the semi-structured Psychosis-Like Symptom Interview, which contains 12 core questions, which are hallucinations (visual and auditory), delusions (spied on, persecution, thoughts read, reference, control and grandiosity) and experiences of thought interference (broadcasting, insertion and withdrawal). Unspecified delusions were also rated. Items are derived from the Diagnostic Interview Schedule for Children, Version IV (DISC-IV) and the Schedules for Clinical Assessment in Neuropsychiatry, Version 2.0 (SCAN). Trained interviewers rated each item as absent, suspected or definitely present. The average kappa was 0.72 indicating good inter-rater reliability. Consistent with previous research, we used at least one definite psychotic symptom (Singh et al., 2014), to demarcate the presence of relevant experiences.
International Classification of Diseases, 10th Revision, depression at 18 years
Depression was assessed with the Revised Clinical Interview Schedule (CIS-R; Lewis et al., 1992). The CIS-R has been validated in community populations (Lewis et al., 1992) and is widely used in the Adult Psychiatric Morbidity Surveys of Great Britain. The CIS-R was self-administered via computerised interview during a research clinic. This scale establishes the severity of symptoms of depressive disorders in the past month and uses diagnostic cut-off points based on International Classification of Diseases, 10th Revision (ICD-10) criteria. We used a categorical depression variable representing an ICD-10 diagnosis of mild, moderate or severe depression at the age of 18 years.
Psychotic symptoms at 18 years
Psychotic symptoms since age 12 were assessed with the semi-structured Psychosis-Like Symptom Interview when participants were age 18 (Winsper et al., 2016b) (described above). The average kappa value was 0.83. Test–retest reliability was assessed with 162 adolescents re-interviewed after approximately 47 days (kappa = 0.76, standard error [SE] = 0.078), 46 of whom were re-interviewed by the same interviewer (kappa = 0.86, SE = 0.136) (Zammit et al., 2013). Consistent with previous research, the psychotic symptom outcome represented at least one definite psychotic symptom (Winsper et al., 2016b).
Hypomanic symptoms at 22 years
Participants completed the ‘Your Life Now (at age 21+)’ postal questionnaire at age 22–23 years, including the Hypomania Checklist Questionnaire (HCL-32). Hypomanic symptoms were not assessed before this point. The HCL-32 is a self-report questionnaire pertaining to the lifetime experience of manic symptoms (Angst et al., 2005). Respondents are asked to consider a time when they were in a ‘high or hyper’ condition and endorse various statements about their emotions, thoughts and behaviours during this time. There are 32 symptom statements, e.g. ‘I think faster’ and ‘I need less sleep’. The HCL-32 was developed to screen for possible subthreshold hypomanic syndromes in people with depressive disorders and has been used previously in non-clinical populations of youth.
Consistent with this previous work (Marwaha et al., 2017), we constructed a lifetime history of hypomania variable, with a threshold of 14+ out of 32 hypomanic features. In addition, participants had to report the following: at least one occurrence of either ‘negative consequences’ or ‘negative plus positive consequences’, due to hypomanic symptoms; and that mood changes caused a response (neutral, negative or negative and positive) in close others; and that hypomanic symptoms lasted for a duration of at least ‘2–3 days’. A duration of 2–3 days or more was originally chosen because it was deemed important that the screening tool was sensitive to experiences of brief hypomania (i.e. syndromes lasting 2–3 days rather than the usual diagnostic threshold of 4 days). This duration increases the detection of individuals at risk of bipolar disorder that meets diagnostic criteria and previous research had demonstrated that individuals who experience brief hypomania have similar clinical and family histories to individuals with bipolar I disorder (BD-I) and bipolar II disorder (BD-II). We choose this conservative threshold (i.e. severity, duration and impairment) to identify clinically relevant symptoms.
Psychosocial confounders
We controlled for gender, family adversity and physical and sexual abuse, given that they are associated with depression, psychotic symptoms and hypomania (Marwaha and Bebbington, 2015; Marwaha et al., 2016). Multiple family risk factors were assessed using the Family Adversity Index (FAI) during pregnancy (‘long index’), 2 years (‘long index’) and 4 years (‘short index’). The FAI ‘long index’ comprises 18 items (Wolke et al., 2012). The short index has 15 of the same items (e.g. financial status, housing). Each item was given one point (if yes). Points were summed at each time-point for a total FAI score.
Physical and sexual abuse were mother reported (postal questionnaire) when children were 1.5, 3.5, 4.8, 5.8 and 6.8 years old. We constructed two variables representing physical and sexual abuse, respectively, at any time-point.
Statistical analysis
Missing data
While 6091 completed the BPD interview at age 11 years, inclusion in the final sample depended on the child also having completed the depression computerised interview at 18 years, the psychotic symptoms interview at 18 years and the hypomania questionnaire at 22–23 years. This meant that the sample for the final path model was 1758 (see Figure 1). We conducted logistic regressions to determine the predictors of missing data. These were male sex, low birthweight and family adversity (Supplemental Table S1). We therefore constructed weights based on these predictors, to account for missing data within our analysis.
Logistic regression analysis
We chose to take an approach that used dichotomous variables so that measures of effect were odds ratios (ORs), which are generally more easily understood among clinicians than coefficients. Where possible, the dichotomous variables are also linked with relevant clinical diagnoses, aiding the extent to which results are clinically interpretable. We conducted logistic regressions with SPSS version 25. BPD was the independent variable and depressive, psychotic and hypomania symptoms were the dependent variables.
We developed our model in four stages, iteratively adjusting for confounders: (1) unadjusted associations; (2) adjusted for gender, family adversity and physical/sexual abuse; (3) plus depressive and psychotic symptoms at 12 years and (4) plus depressive and psychotic symptoms at age 18 for the hypomanic outcome, depression at 18 years for the psychotic outcome and psychotic symptoms at age 18 years for the depression outcome.
Path analysis
We conducted path analysis modelling using Mplus version 7.11. We controlled for multiple pathways (concurrent and prospective) between psychopathological measures (e.g. depressive symptoms at 12 and 18 years; depressive and psychotic symptoms at 18 years) to determine the independent associations between BPD and subsequent psychopathologies. We included our weighting variable in the path model.
Results
Descriptive and unadjusted statistics
At age 11–12 years, 6.7% of adolescents reported five or more probable/definite symptoms over the past 2 years. At 18 years, 7.9% had any ICD-10 diagnosis of depression (experienced during the past month), while 4.1% reported experiencing one or more psychotic symptoms since age 12 years. At 22–23 years, 8% reported lifetime clinically relevant hypomanic symptoms. Psychotic and depressive symptoms were strongly associated (OR: 5.50; 95% confidence Interval [CI]: [3.20, 9.45]). Associations between psychotic experiences and hypomania symptoms (OR: 1.69; 95% CI: [0.82, 3.47]) and depression and hypomania symptoms were not significant (OR: 1.44; 95% CI: [0.82, 2.54]).
Logistic regression models
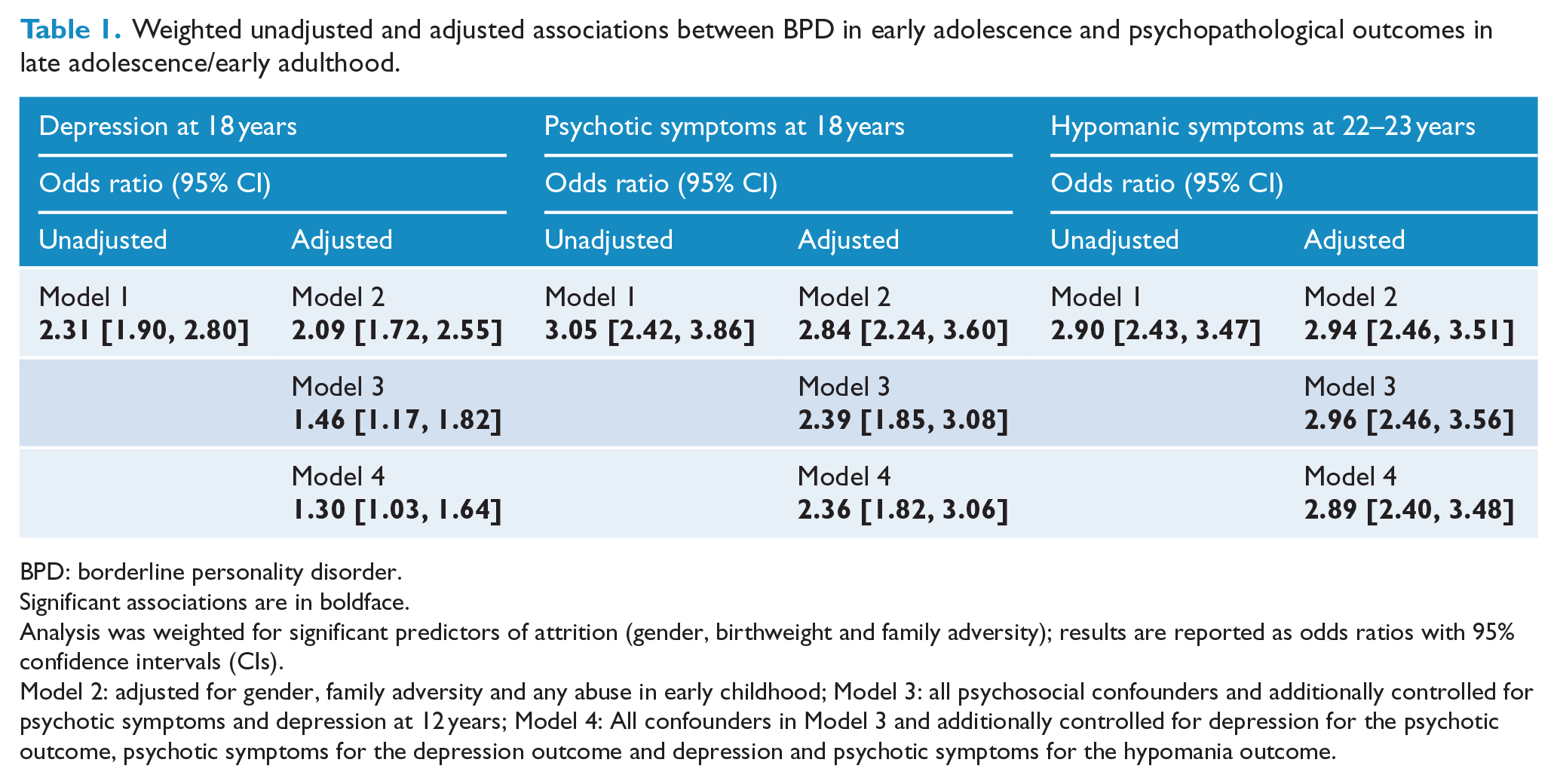
Results of the weighted analysis are reported in Table 1. BPD symptoms significantly predicted each of the psychopathological outcomes in both unadjusted and adjusted analyses. Associations remained largely unchanged following control for psychosocial confounders (Model 2). Overall, the biggest attenuation effect followed the incorporation of depressive and psychotic symptoms at 12 years (Model 3).
Weighted unadjusted and adjusted associations between BPD in early adolescence and psychopathological outcomes in late adolescence/early adulthood.
BPD: borderline personality disorder.
Significant associations are in boldface.
Analysis was weighted for significant predictors of attrition (gender, birthweight and family adversity); results are reported as odds ratios with 95% confidence intervals (CIs).
Model 2: adjusted for gender, family adversity and any abuse in early childhood; Model 3: all psychosocial confounders and additionally controlled for psychotic symptoms and depression at 12 years; Model 4: All confounders in Model 3 and additionally controlled for depression for the psychotic outcome, psychotic symptoms for the depression outcome and depression and psychotic symptoms for the hypomania outcome.
Path analysis
The path model is shown in Figure 2. The model had adequate (confirmatory fit index [CFI] = 0.94) to good (χ2 = 23.84, p = 0.07; root mean square error of approximation [RMSEA] = 0.02) fit. Four independent trajectories from BPD were evident in the path analysis. First, BPD symptoms were independently associated with clinically relevant depressive symptoms, one or more psychotic symptoms at 12 years and clinically relevant hypomanic symptoms at 22–23 years. Second, BPD symptoms were indirectly associated with ICD-10 depression (mild, moderate or severe) at 18 years via depressive symptoms at 12 years. BPD symptoms were not significantly indirectly associated with psychotic symptoms at 18 years via psychotic symptoms at 12 years. However, BPD symptoms were significantly linked to psychotic symptoms at age 12 years, which in turn were significantly associated with psychotic symptoms at age 18 years (Table 2 and Figure 2).
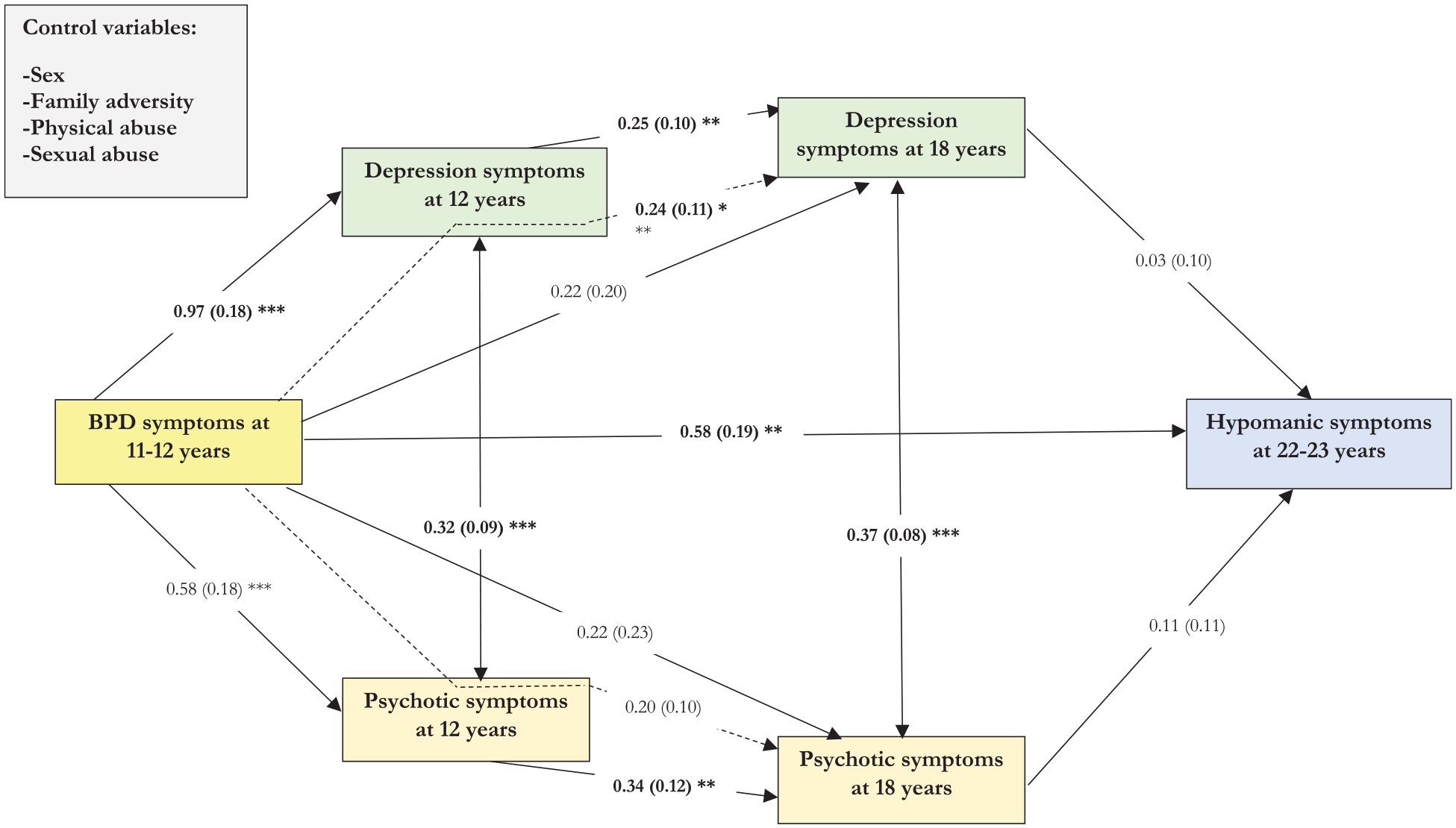
The final path model including associations between adolescent BPD and subsequent psychopathologies.
Direct and indirect associations between BPD, depression, psychotic and hypomanic symptoms within the final path model.
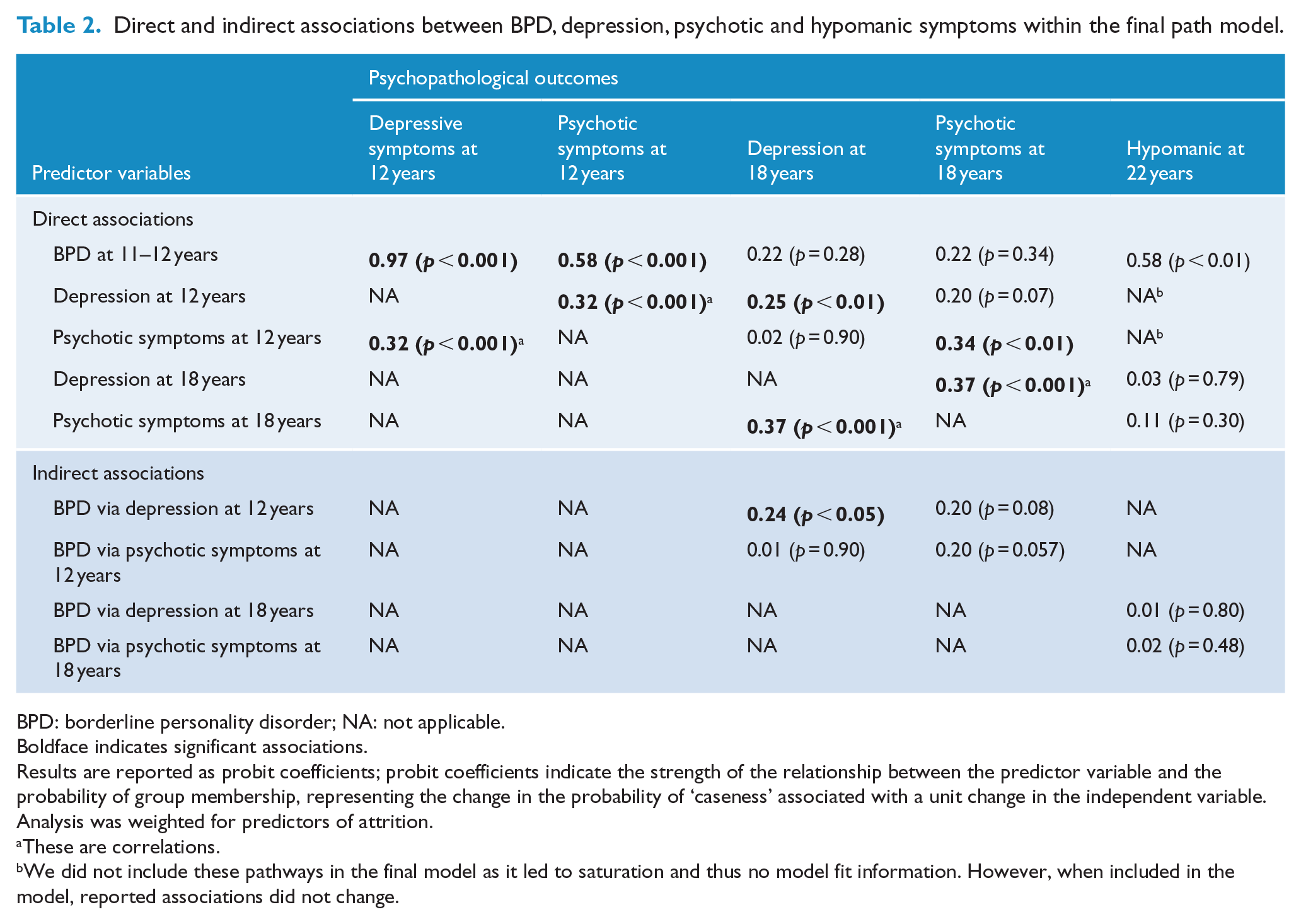
BPD: borderline personality disorder; NA: not applicable.
Boldface indicates significant associations.
Results are reported as probit coefficients; probit coefficients indicate the strength of the relationship between the predictor variable and the probability of group membership, representing the change in the probability of ‘caseness’ associated with a unit change in the independent variable. Analysis was weighted for predictors of attrition.
These are correlations.
We did not include these pathways in the final model as it led to saturation and thus no model fit information. However, when included in the model, reported associations did not change.
Discussion
Our study represents a first step towards explicating the psychopathological sequelae of BPD symptoms (five or more repeated or very frequent) in a community population. Adolescent BPD symptoms increased the risk of subsequent psychotic symptoms, a diagnosis of depression reported at 18 years and clinically relevant lifetime hypomanic symptoms reported at 22–23 years. The prospective direct association with depression diagnosis at 18 was not significant following control for all confounders (including inter-relationships between all psychopathological symptoms) in the path analysis. However, BPD was significantly indirectly associated with depression diagnosis via depressive symptoms at 12 years.
The associations between adolescent BPD symptoms and subsequent psychotic and hypomanic symptoms are notable given that they have received limited prospective investigation. It is suggested that many psychiatric disorders are sequentially comorbid, recurrent or chronic (Caspi et al., 2014). Our findings suggest that young adolescents with substantial BPD symptomatology are at increased risk of experiencing a range of clinically relevant psychiatric symptoms across several developmental stages (early/late adolescence, early adulthood). Independent developmental pathways linked to hypomania and psychotic symptoms were not likely attributable to symptom overlap between outcomes, as we simultaneously controlled for all associations between each of the psychopathological outcome assessments. These findings are consistent with notions of multifinality (i.e. BPD has divergent outcomes).
Our results are in line with the hypothesis that early BPD symptoms can be seen as an adolescent manifestation of the confluence of internalizing and externalizing (IE) psychopathology on the severity pathway that leads to subsequent major mental disorders (Sharp and Wall, 2018). These outcomes may be determined by the severity level of IE, mediating and moderating contexts and transactional feedback loops with the manifest syndrome (Beauchaine and Cicchetti, 2016). Indeed, Hayes et al. (2017) hypothesize that the genetic architecture of maladaptive personality traits and serious mental illness may be shared, with emotional instability (a key feature of BPD), in particular predicting serious mental illness. Maladaptive interpersonal functioning (e.g. self–other relatedness, including maladaptive self-perception and social function), which is another key feature of BPD, may be particularly important as a precursor to other personality pathology (Sharp et al., 2018; Sharp and Wall, 2018). Thus, personality pathology can be considered an important severity indicator in adolescence that should not be ignored.
Previous research suggests three trajectories for individuals with adolescent BPD symptoms: (1) continuation of BPD symptoms over time, (2) remission of psychiatric symptoms and (3) the development of other disorders (Winsper et al., 2015). Our analyses highlight that there is a risk that individuals develop other types of clinically relevant psychopathology and supports the idea of heterotypic continuity as a developmental pathway. It also supports the notion that adolescents with BPD symptoms are a clinically vulnerable group by virtue of their current symptomatology, but also due to risks of future psychopathology. This helps explain the long-term morbidity associated with the condition and why the outcomes can be for so devastating into adulthood.
Our study has strengths and limitations. Strengths include the use of data from a large, well-defined birth cohort, with repeated assessments of important psychopathologies covering a developmental period largely neglected in BPD research. Using a validated interview for BPD, we could identify adolescents with five or more BPD symptoms, thus creating a variable comparable in composition to the DSM-5 diagnosis for BPD (American Psychiatric Association, 2013). In our community sample, 6.7% of adolescents met our criteria for substantial BPD symptoms. This rate is somewhat higher than the 1.8% (95% CI: [1.2%, 2.5%]) reported in adult community populations (Winsper et al., 2019) and is likely attributable to our lower symptom frequency threshold (i.e. inclusion of repeated and very frequent symptom counts). Other small-scale community studies with younger populations have suggested a higher prevalence of BPD (e.g. 11% using algorithms for DSM-III-R diagnosis), with a peak in prevalence at 12–13 years of age (Bernstein et al., 1993). This suggests that our data handling strategy is likely to have some clinical utility (i.e. in identifying subclinical youth at heightened risk of BPD). While our BPD symptom variable does not equate to a clinician-derived BPD diagnosis, it does represent a good balance between clinical and scientific needs. We were able to study a relatively large group of youths demonstrating five or more BPD symptoms, while avoiding the inevitable resource issues associated with providing clinical assessments in epidemiological research. At age 18 years, 7.9% of the sample had any ICD-10 diagnosis of depression consistent with previous epidemiological data (Costello et al., 2005), again supporting the validity of our approach to data handling and analysis. Another strength was our use of advanced analytical methods, e.g. path analysis, which allowed us to understand the prospective connections between psychopathological clusters. Future analyses should consider the use of network analysis to further understand the interconnections between multiple psychopathological and other parameters in studies of adolescent BPD.
There were also limitations. First, while the prospective design enabled us to model predictive pathways based on temporal ordering, some assessments lacked temporal precision, e.g. psychotic symptoms at 18 referred to events occurring since the previous assessment (12 years), and the hypomanic scale referred to lifetime occurrence. However, it should be highlighted that pre-pubertal hypomania is very rare (Kroon et al., 2013), and it is unlikely that respondents would remember symptoms occurring several years ago. Second, there was considerable selective attrition in the cohort reducing statistical power and potentially biasing our results. We weighted both our logistic and path analyses to account for this attrition (Kinner et al., 2007). Third, while we included clinically relevant levels of psychiatric symptoms where possible (e.g. ICD depression diagnosis, hypomanic symptoms according to severity, duration and impairment), we could not include psychotic disorder as the frequency was too low. Nevertheless, psychotic symptoms are a marker for, and significantly increase risk of, psychotic disorder in adults (Fisher et al., 2013). Fourth, childhood risk factors, including family adversity and physical and sexual abuse, were reported by the child’s mother. This could have led to issues such as under-reporting as mothers may have been unaware of abuse experiences or were reluctant to report these factors as they could imply neglected care. Thus, there is a small chance that we could have underestimated the impact of confounders on associations between psychopathologies. Furthermore, some of our psychopathological outcomes were assessed via interview, either face to face or computerized (i.e. psychotic symptoms reported at 12 and 18 years and depression symptoms reported at 18 years), and others via self-report postal questionnaire (i.e. depression symptoms reported at 12 years and hypomania symptoms reported at 22–23 years). Thus, there were variations in mode of administration, which could have potentially influenced responses in reference to the different psychopathological outcomes (Bowling, 2005). These differences could have led to an under-estimation of the strength of associations between psychopathologies. Ideally, we would use interview data for all psychopathologies as the gold standard approach to assessing mental disorders. However, this was not possible due to the considerable resource demands, e.g. young adults assessed at 22–23 years of age likely moved to locations across the country. Fifth, BPD symptoms were only assessed once in this cohort. This is unfortunate and likely reflects the substantial costs involved in administering clinical interviews to very large samples, and the current underfunding of BPD in comparison to other psychiatric disorders (Zimmerman and Gazarian, 2014). Subsequently, we could not examine whether adolescents with BPD symptoms continued to manifest chronic BPD symptoms in early adulthood or whether associations with other psychopathological outcomes (e.g. psychotic and hypomania symptoms) remained significant following control for concurrent BPD symptoms. Therefore, it is possible that associations between adolescent psychopathology and subsequent psychotic, depression and hypomania symptomatology were explained by a continuation of BPD symptoms into late adolescence and early adulthood. Clinical studies indicate that most episodes of psychotic and dissociative symptoms in patients with BPD are transient, and of a different structural, functional and physiologic nature to those observed in psychotic disorder (e.g. amygdala over-reactivity vs decreased amygdala activity). This suggests that associations were not solely attributable to concurrent BPD in late adolescence. However, studies do indicate that a subset of BPD patients may experience permanent and more severe psychotic symptoms over time (Barnow et al., 2010). Similarly, clinical studies suggest that BPD and bipolar disorders are independent, though there may be a subgroup of individuals with characterological bipolar disorder, i.e. they demonstrate both BPD and BD-II symptoms that are less tied to BD-I (Gunderson et al., 2014). Relatedly, given the overlap between diagnostic clusters of mental disorders and the fact that those who did not meet criteria for BPD symptoms in early adolescence may have done so subsequently (e.g. at 18 or 22–23 years), it is possible that we measured the same transdiagnostic symptom pool over several time-points. We cannot completely discount this possibility, but it is likely that the reliable and valid measures such as the UK-CI-BPD, CIS-R and HCL are at least to some extent able to accurately differentiate different symptom clusters. Finally, we did not examine the influence of treatment within our analyses. However, in the UK context, services and specialist programmes for adolescents with BPD are very limited and it is unlikely that specific treatment for BPD in adolescence will have had a major influence on our findings, especially given that few UK psychiatrists will diagnose BPD before age 18 years.
In conclusion, in a large birth cohort study, we found that adolescent syndromal BPD was associated with a range of psychopathological sequelae up to 10 years later. Our findings add to the growing literature on the adverse outcomes of adolescent BPD (Winsper et al., 2015) and should raise clinical awareness that if BPD symptoms are measured in early adolescence, a significant subpopulation already appears to have a BPD-like syndrome and these individuals are at risk of a range of future psychopathologies. This study raises the possibility that early secondary intervention (Chanen et al., 2014) may help reduce the risk of poor psychopathological outcomes potentially offering an avenue for primary prevention of other major mental disorders. The next step in our investigation is to identify the determinants (e.g. environmental risks) of different developmental trajectories to increase our understanding of the varied outcomes of adolescent BPD (Forbes et al., 2016).
Supplemental Material
Supplementary_Tables – Supplemental material for Psychopathological outcomes of adolescent borderline personality disorder symptoms
Supplemental material, Supplementary_Tables for Psychopathological outcomes of adolescent borderline personality disorder symptoms by Catherine Winsper, Dieter Wolke, Jan Scott, Carla Sharp, Andrew Thompson and Steven Marwaha in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors are extremely grateful to all the families who took part in this study, the midwives for their help in recruiting them and the whole ALSPAC team, which included interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses. The authors give special thanks to Dr Andrea Waylen, PhD, and Dr Jeremy Horwood, PhD, who helped in the conduct of the study. The UK Medical Research Council and Wellcome (Grant ref. 102215/2/13/2) and the University of Bristol provide core support for ALSPAC. This publication is the work of the authors and C.W. and S.M. will serve as guarantors for the contents of this paper.
Declaration of Conflicting Interests
S.M. attended a World Psychiatric Association consensus meeting on early intervention sponsored by an unrestricted educational grant from Sonuvion. All the other authors declare no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.