
Abstract
Objective
Our study focussed on the obstetric and psychosocial outcomes of pregnant women with Borderline Personality Disorder (BPD) who received care via a specialist antenatal clinic in Western Australia.
Method
This study is a retrospective examination of outcomes for 80 women with a confirmed diagnosis of BPD, with findings compared with published population outcome data for the state.
Results
Pregnant women with BPD appeared to be at a risk of complications including pre-eclampsia and special care nursery admission for their newborns when compared to population data. Furthermore, the studied women had elevated rates of psychiatric admissions during pregnancy, child protection involvement, and domestic violence. Polypharmacy exposure was frequent, with the likely impact on obstetric and neonatal outcomes requiring further study.
Conclusion
The findings reinforced the notion that pregnant women with BPD experience complex multifaceted vulnerabilities and require enhanced multidisciplinary care. Our study further calls for the development of clinical practice guidelines for managing BPD in the perinatal period.
The mental disorder known as Borderline Personality Disorder (BPD) or Emotionally Unstable Personality Disorder (EUPD) has evolved from its initial description of being a border between the psychotic and neurotic disorders to an understanding that its pathogenesis likely lies in interactions between developmental disruptions such as trauma and biological predispositions, although the precise mechanism remains unclear. 1 While the disorder is seen to affect up to 6% of the population 2 and 23% of psychiatric outpatient presentations, 3 there appears to be a discrepancy in terms clinical, service provision, and research priority compared to disorders such schizophrenia and bipolar. Patients with BPD may encounter stigma from having the validity of their presentation and diagnosis questioned, a situation that partly stemmed from the former grouping of personality disorders as Axis II on the Diagnostic and Statistical Manual IV edition 4 distinguishing it from other mental disorders such as schizophrenia on Axis I. Such a position diminishes the multifaceted dysfunction and disability experienced by sufferers and creates barriers in access to care.
BPD is also a disorder that commonly affects women of reproductive age, with presentations often occurring in the perinatal setting with potential downstream consequences on the development of their offspring. Prasad et al. 5 found the pooled prevalence of BPD in perinatal women to be 14% while Nagel et al. 6 in their study at a tertiary maternity hospital found 10.1% met BPD criteria while 19.5% had BPD traits. To the best of our knowledge there have been only four studies examining the obstetric, neonatal, and social outcomes for pregnant women with BPD. De Genna et al. 7 studied 379 pregnant women with BPD and found symptom severity to be associated with teenage pregnancy, unintended pregnancies as well as abortions and still births. Over two-thirds of these women met criteria for at least one substance abuse or dependence in their lifetime. Pare-Miron et al. 8 in their study of 989 pregnant women with BPD found that having this diagnosis was associated with elevated risks of gestational diabetes mellitus (GDM), premature rupture of membranes, chorioamnionitis, venous thromboembolism, caesarean delivery, and preterm birth, when compared with a non-mentally ill control group. Two studies of pregnant women with BPD in Australia showed further difficulties encountered by these patients. Blankley et al. 9 compared outcomes for 42 pregnant women with BPD with their non-mentally ill counterparts and found that babies of mothers with BPD had lowered Apgar scores, prematurity, and special care nursery referrals. The studied population also displayed high rates of substance abuse and child protection involvement. Another study by Nagel et al. 6 found that when compared to unmatched controls, pregnant women who met the clinical criteria for BPD and those with subthreshold BPD traits had high rates of unplanned pregnancy, being unpartnered, having substance use, and child protection involvement during pregnancy. This study also highlighted the diagnostic challenge of BPD in the perinatal period with psychiatric comorbidity being common.
With these findings in mind, our study aimed to examine obstetric, neonatal, and psychosocial outcomes for pregnant women with BPD who gave birth at the state’s tertiary maternity hospital with further comparison of these outcomes with existing population data for non-mentally ill pregnant women.
Methods
The study was an extension of the gestational diabetes in women with SMI with the methodology previously discussed. 10 An amendment to the study focused on pregnant women with BPD was carried out with approval from the hospital Human Research Ethics Committee (RGS 2016128EW).
Pregnant women who gave birth through the specialist Childbirth and Mental Illness Clinic (CAMI) between 2007 and 2019 and had a recorded diagnosis of BPD or EUPD on presentation, either as a primary diagnosis or secondary diagnosis, or had documented BPD traits were included in this study. All women received comprehensive perinatal psychiatrist assessments during pregnancy with their diagnoses coded. Further confirmation of the diagnosis of BPD as a predominant condition in cases of comorbidity was undertaken by cross-checking the patient unique medical record identifier with the state-wide Psychiatric Services On-line Information System (PSOLIS), which allows for a longitudinal picture of the patient’s diagnostic journey.
Obstetric, neonatal, and social outcomes for the studied women were extracted from clinical notes and the purpose designed perinatal database. Available data regarding domestic violence (DV) were obtained using linked patients medical record numbers with existing data from the study by Suparare et al. 11
Statistical analysis
Data were managed and analysed using SPSS version 24 and MedCalc for Windows, version 18.11. Descriptive statistics for the CAMI BPD sample and the state population data - WA Mothers and Babies 2015 report 12 are presented and compared using χ2 tests of association for categorical variables (Fisher’s exact results present where expected cell frequency was below 5) and ANOVA tests for continuous variables. The prevalence of delivery outcomes and neonatal outcomes and the unadjusted risk associated with BPD relative to the state population data are presented. Psychosocial outcomes in the BPD sample are presented separately due to no available comparison data. For all analyses, statistical significance is determined using p-value of less than .05.
Results
Of 573 pregnant women who gave birth at the CAMI clinic between 2007 and 2019, 80 women with BPD were identified.
Sociodemographic characteristics, with inferential comparisons between CAMI BPD and WA mothers and babies 2015
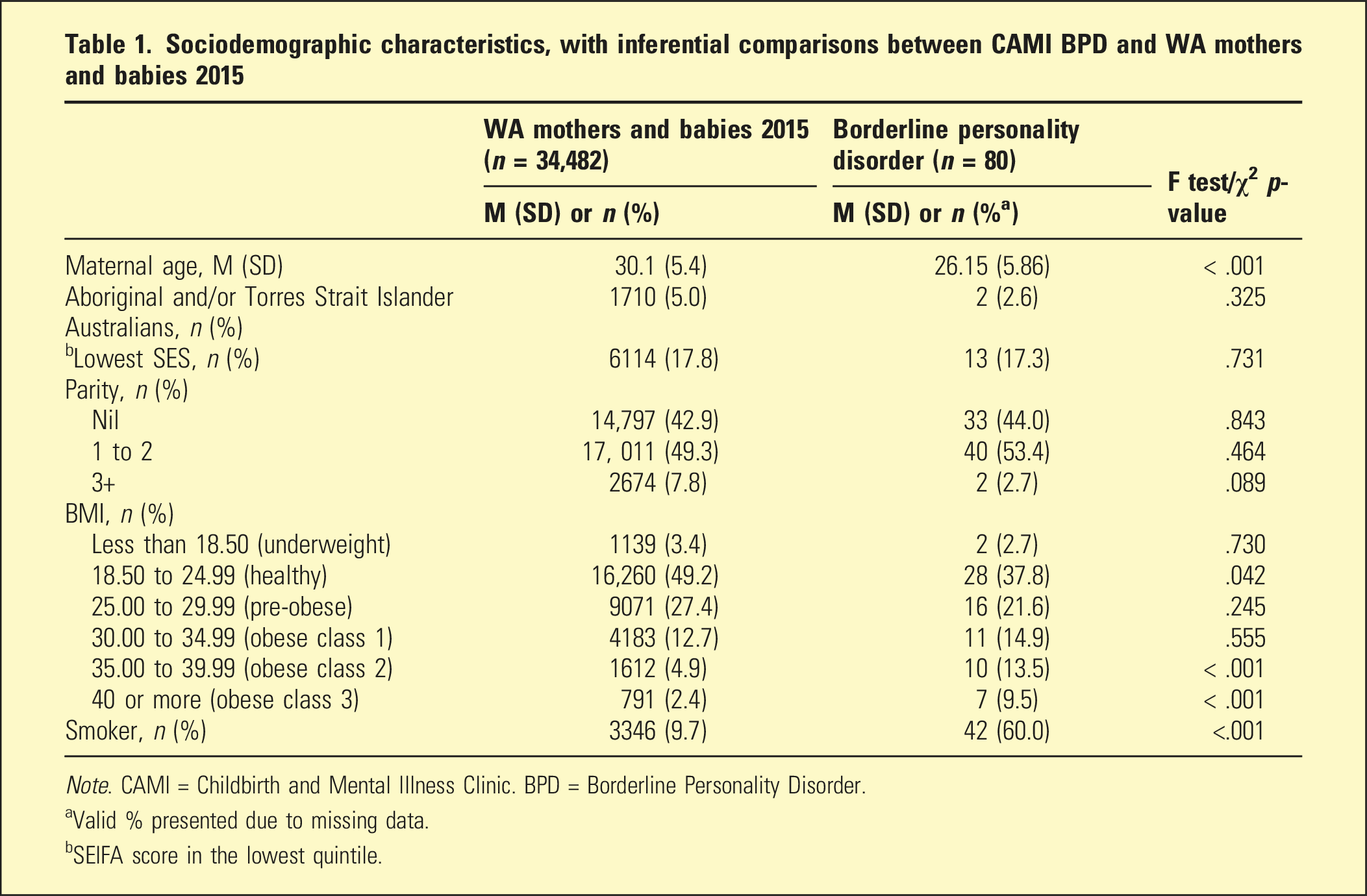
Note. CAMI = Childbirth and Mental Illness Clinic. BPD = Borderline Personality Disorder.
aValid % presented due to missing data.
bSEIFA score in the lowest quintile.
Antenatal, delivery, and neonatal outcomes for women with BPD
Prevalence of antenatal, delivery, and neonatal outcomes and the unadjusted risk associated with CAMI BPD relative to the WA mothers and babies 2015
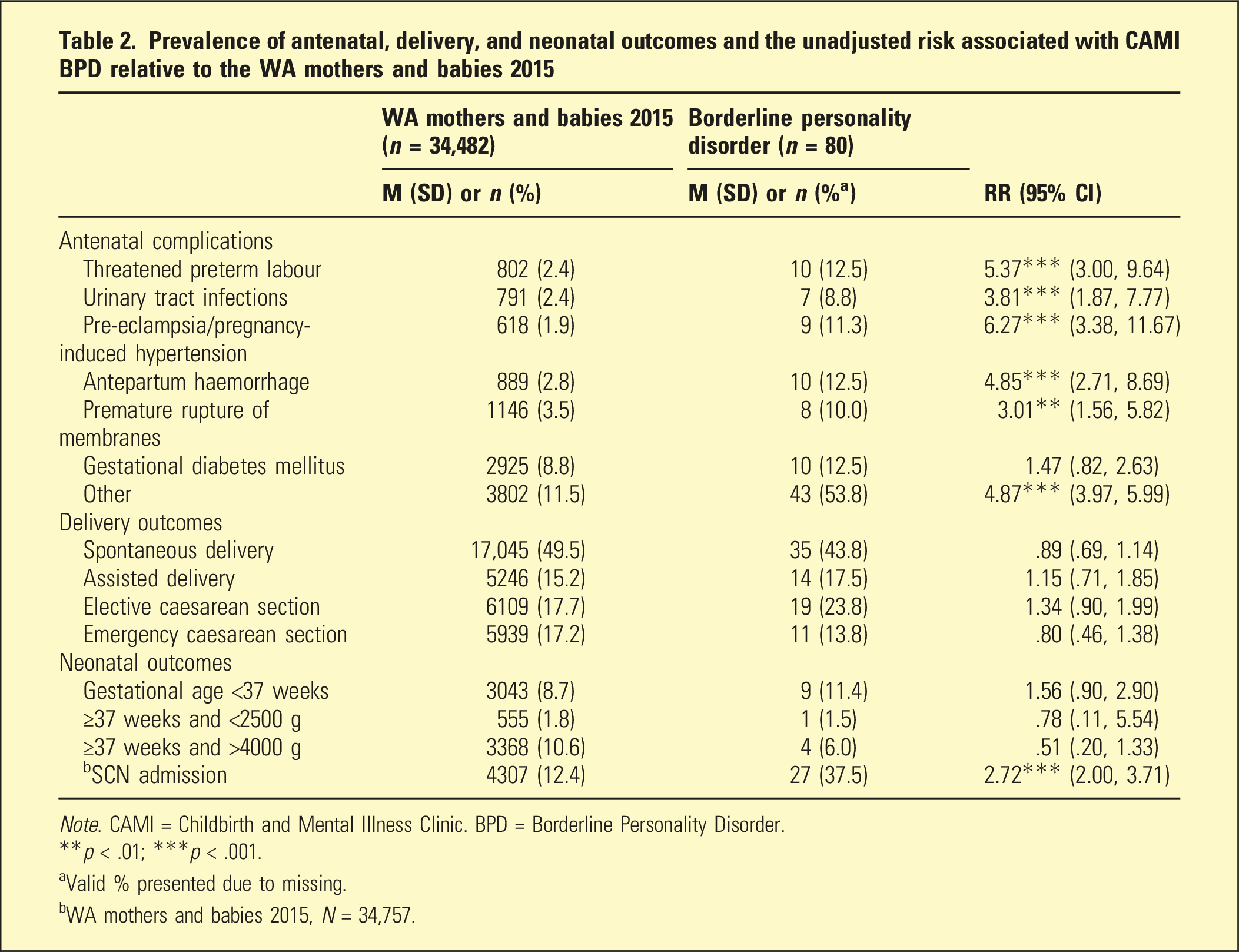
Note. CAMI = Childbirth and Mental Illness Clinic. BPD = Borderline Personality Disorder.
**p < .01; ***p < .001.
aValid % presented due to missing.
bWA mothers and babies 2015, N = 34,757.
Psychosocial outcomes for women with BPD
Prevalence of psychosocial outcomes for CAMI BPD only
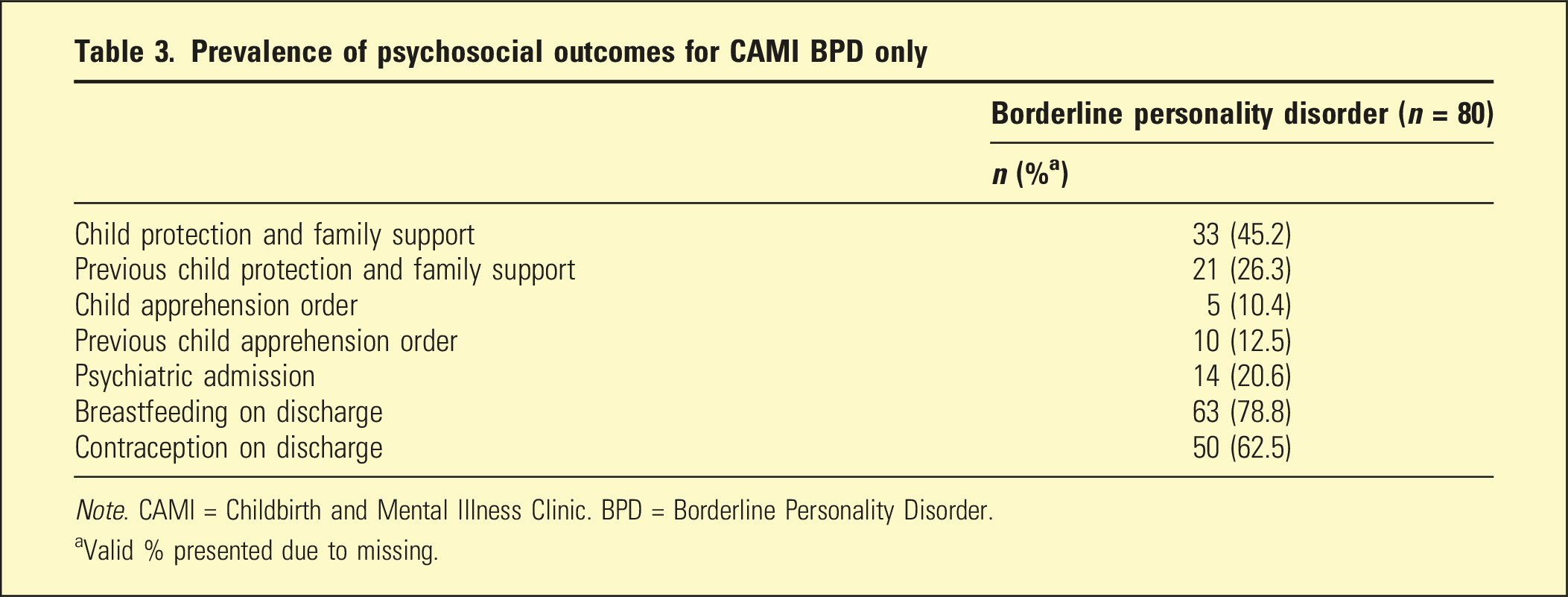
Note. CAMI = Childbirth and Mental Illness Clinic. BPD = Borderline Personality Disorder.
aValid % presented due to missing.
Polypharmacy
In our study, 10 (12.5%) women had no psychotropic medication exposure while 21 (26.2%) were taking one, 26 (32.5%) took two, 15 (18.7%) took three, 7 (8.8%) took four, and 1 woman (1.2%) took five psychotropic medications, respectively. When grouped into those who were prescribed 0–2 psychotropic medications and those with >2 psychotropics, the rates of GDM were 10.5% versus 17.4%, pre-eclampsia 8.8% versus 17.4%, and SCN admissions (n = 72) 32.5% versus 50.0%, respectively. All p-values are non-significant. Upon initial referral to the antenatal clinic, 22 women had comorbid diagnoses of bipolar affective disorders. The rates of polypharmacy of those who presented with bipolar were 7/23 (30.4%) in the 0–2 medication group, while 15/57 (26.3%) were in the three or more psychotropic group, with no significant difference.
Discussion
Our study contributes to the existing data on pregnant women with BPD and further highlights the complex needs of this vulnerable group of women. In keeping with previous studies, the findings suggest that women with BPD struggle during pregnancy with obesity as well as higher rates of obstetric complications including pre-eclampsia and admission of their neonate to a special care nursery, than pregnant women in the general population. On a positive note, a majority of women were breastfeeding and had contraception plans on discharge from hospital. While further large-scale research is needed, the data available supports the notion that pregnant women with BPD should be given health priority, much like the call for pregnant women with schizophrenia 13 and renews the call for the development of clinical practice guidelines specifically for this population. 9
Beyond physical health complications, the management of pregnant women with BPD appears complex and challenging as evident by the polypharmacy exposure and comorbid psychosocial adversities. Despite guidelines suggesting that psychotropics do not have a primary role in managing patients with BPD, 14 our study found that 87.5% were on one or more psychotropic agent during pregnancy and 29% were on three or more psychotropic agents. The findings reflect real-world experience of managing patients with BPD, as evident by an Australian study in non-perinatal patients with BPD where 89% were taking at least one psychotropic and 35% were prescribed three or more psychotropics. 15
We reported also on some obstetric complications related to polypharmacy, and while the findings were not statistically significant likely due to low sample size, the trend for higher rates of GDM, pre-eclampsia, and SCN admission with exposure to more than two psychotropics require further studies with larger samples. In our sample, 27% of women had diagnoses of bipolar affective disorder on referral, which appeared consistent with the 20% comorbidity between BPD and bipolar reported by Zimmerman and Morgan. 16 The presence of bipolar in the studied women did not significantly impact on the rate of polypharmacy exposure.
Among the women studied, we found one-fifth had at least one psychiatric admission during pregnancy, suggesting this is a potential time of destabilisation for women with BPD. However this relationship may be bidirectional, in that BPD destabilisation may lead to unplanned pregnancies. 7 It is also likely that BPD destabilisation may be associated with relational stressors, such as domestic violence. In our sample, nearly half of the women, of whom data were available, reported exposure to DV. Beyond the health impact of DV on a pregnant woman and her offspring, 17 its presence together with psychiatric destabilisation and substance use can further lead to the adverse outcome of statutory child protection involvement. Nearly half (45.2%) of the women studied had child protection involvement with one in ten subjected to a child removal order. This high rate of child protection involvement is in line with the Australian study by Blankley et al. 9 and comparable to previous findings for women with schizophrenia,11,18 which further emphasises the need for an enhanced multidisciplinary model of antenatal care.
Limitations of our study include the retrospective methodology and the relatively low sample size, including some missing data. However, we were able to examine in detail the complex psychiatric, obstetric, and social vulnerabilities and needs of pregnant women with BPD. Our findings serve to advocate for further research and the development of a tailored continuum of care for women with BPD of childbearing age, ranging from preconception review of polypharmacy, physical health, and relationships, to enhanced multidisciplinary antenatal care and postnatal follow-up.
Footnotes
Acknowledgements
The authors thank those who have both supported and given advice in the development of the Childbirth and Mental Illness Clinic at KEMH. We are also grateful to all the staff who have worked at the clinic and the women and their families who attended it.
Author contributions
TN, JF, SW, and MG conceived the idea of the study. TN and JF collected the data. SW provided the main statistical analysis. All authors drafted the manuscript and approved the final submission.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
The study received ethics approval from the local Human Research Ethics Committee (RGS 2016128EW).