
Abstract
Objective:
Grief reactions change over time. However, only a limited number of studies, and none in Australia, have analysed changes in individual grief reactions longitudinally. The aim is to examine changes in grief reactions, mental health and suicidality of close family members bereaved by suicide, 6, 12 and 24 months after their loss compared with those bereaved by other forms of sudden death, adjusting for confounding factors.
Method:
Participants were 142 adult family members bereaved by suicide and 63 by other sudden death, followed up at 6, 12 and 24 months in Queensland, Australia. The Grief Experience Questionnaire, Depression Anxiety Stress Scale and Beck Scale for Suicide Ideation were used as main outcomes. Mixed-effects linear and logistic regressions were utilized for statistical analyses.
Results:
There were significant differences in rejection, stigmatization, shame and responsibility between the suicide and sudden death bereaved over the 2-year period, after adjusting for potential confounding factors. Rejection, stigmatization, search for explanation, somatic reactions and symptoms of depression and anxiety (Depression Anxiety Stress Scale) declined significantly over time in both groups. Rejection and somatic reactions showed group-by-time interaction effects, with a decrease in the suicide bereaved and no change in the sudden death bereaved. Loss of social support and suicidal ideation did not show a group or time effect.
Conclusion:
Although our findings confirm that there are several common dimensions to experiencing a sudden death of a family member, several differences were found between the suicide and non-suicide sudden death bereaved including significantly higher levels of rejection, stigmatization, shame and responsibility remaining in the suicide compared to sudden death bereaved 2 years after their loss. These findings should be considered in clinical practice and when designing postvention services in Australia.
Introduction
A recent meta-analysis estimated that the prevalence of exposure to suicide in the family was 1.1% in the last year and 3.9% lifetime (Andriessen et al., 2017). Close family members including parents, children, siblings and partners report higher levels of perceived impact and adverse reactions compared to exposed non-family members (Cerel et al., 2016, 2017). Although there are a number of similarities in grief reactions across different types of bereavement, some reactions are anticipated for unexpected deaths, and others are proposed to be specific to violent deaths or more specifically to suicide (Jordan and McIntosh, 2011). Thus, some grief reactions are more common among people bereaved by suicide rather than by other types of deaths. It has been reported that suicide bereaved experience higher levels of stigma, shame, responsibility and rejection, while there are inconsistent results for some other reactions (e.g. guilt and poor mental health) (Jordan and McIntosh, 2011; Pitman et al., 2014; Sveen and Walby, 2008).
Much less is known about grief trajectories over time. While there is growing body of research using linkage data (Bolton et al., 2013; Erlangsen et al., 2017), there is only a limited number of studies analysing individual-level changes in grief reactions after suicide longitudinally and none in Australia (Pitman et al., 2014), with a number of them focusing on specific groups such as children (Cerel et al., 1999; Melhem et al., 2011) or older spouses (Farberow et al., 1992). Therefore, the aim of this study is to analyse changes in grief reactions, mental health and suicidality of close family members bereaved by suicide, 6, 12 and 24 months after their loss compared with those bereaved by other sudden deaths, and adjusting for confounding factors.
Method
Study design
A longitudinal prospective study was designed to compare suicide bereavement to bereavement following other types of sudden deaths in Queensland, Australia, with three assessment points at 6 (T0), 12 (T1) and 24 (T2) months, after the death (Kolves and de Leo, 2018; Kolves et al., 2019). The other sudden deaths, used as a control/comparison group, included accidents and sudden natural deaths when death occurred within a few hours, mainly caused by cardiovascular condition (Murai et al., 2001). The methodology had been tested in a pilot study (Kolves and de Leo, 2018).
Recruitment and participants
The study included close relatives, immediate family members bereaved by a suicide or sudden death, who were at least 18 years old, English speaking, where the death occurred in Queensland, Australia, and the person was contactable 6 ± 1 month after death. Immediate family member was defined as a spouse, de facto partner, child, parent, grandparent, grandchild, sibling, aunt, uncle, niece and nephew, and immediate in-laws.
The study was approved by Griffith University’s Human Research Ethics Committee (CSR/04/11/HREC). All participants provided written consent to participate in the study. Participants for the pilot study were recruited in 2012 (Kolves and de Leo, 2018) and for the main study in 2014-2015 (Kolves et al., 2019). The follow-up interviews lasted until the end of 2017.
Suicide bereaved
People bereaved by suicide were identified through the Queensland Suicide Register, a state-wide suicide register which includes contact details of family members (can be multiple) from police forms. The police form indicated their permission to be contacted by the Australian Institute for Suicide Research and Prevention for research purposes. A letter introducing the study, along with the study information sheet and consent form, was sent to 276 potential participants, followed by a phone call 2 weeks later. Interviews were scheduled upon receiving consent. In this group, 47.1% agreed to participate. The main reasons for non-participation were inability to reach the person, not willing to talk or being too busy. An additional 7.2% who consented did not respond or show up at the interview time, or changed their mind (n = 20), leaving the final response rate of 39.9%. Approximately 40% of police forms did not have information regarding permission to contact the next-of-kin (the question is unanswered). Additional ethics committee approval was given to seek active consent from those next-of-kin. A letter introducing the study and invitation to participate was sent to 261 next-of-kin, along with the study information sheet and consent form. Next-of-kin were asked to provide active consent (by signing and sending back the consent forms; no phone calls). Consent was provided by 21.5% of next-of-kin, though of these in 5.0% of cases the criteria 6 ± 1 month since loss of loved one lapsed (n = 3) or they were no longer contactable or withdrew (n = 10), with a final response rate of 16.1%. Clinical interviewers contacted participants via phone after the receipt of a consent form, to schedule interviews. The majority of the interviews (78.9%) were conducted over the phone, the rest face to face (mainly at home).
The follow-up retention rate was 90.1% with 14 suicide-bereaved individuals dropping out at 12 months (11 were not contactable and 3 withdrew) and 77.5% at 24 months with a further 18 dropping out (10 were not contactable, 5 withdrew and 2 did not respond at the time of the scheduled interview; Figure 1).
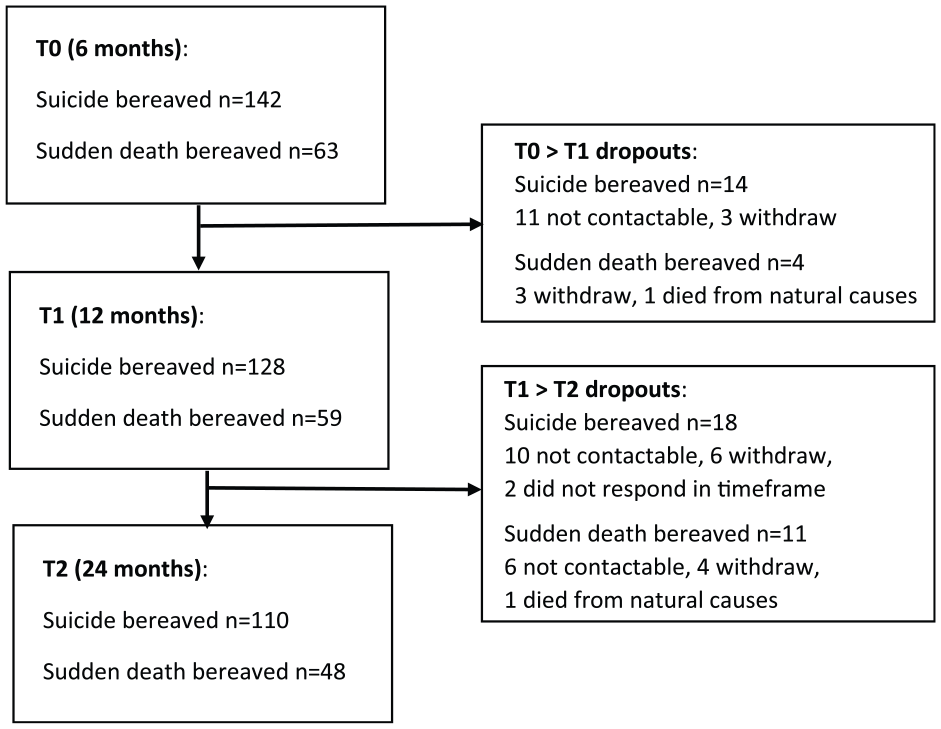
Dropouts from the study.
Other sudden death bereaved
Participants for the sudden death group were identified and recruited by the Queensland Office of State Coroners using the police forms. The ‘reportable deaths’ by the Queensland Coroners Act 2003 need to be sudden in their nature (Queensland Government, 2003). Only next-of-kin of closed cases (i.e. coroner has made their final verdict and closed the case) were approached 5 months after death. A letter introducing the study, along with the study information sheet and consent form, was sent and next-of-kin were asked to provide active consent. After the receipt of a consent form, clinical interviewer(s) contacted participants via phone to schedule interviews. The consent form was received from 32.3% of contacted next-of-kin (n = 233), of which 5.2% included cases where the time period had lapsed (n = 2) or they changed their mind (withdraw or no show to interview, n = 10), with the final response rate of 27.0%. The majority of the interviews (88.9%) were conducted over the phone.
In the sudden death group, more than half of the participants had lost their loved one suddenly to diseases of the circulatory system (52.4%), followed by other external causes of death (25.4%), injury, poisoning and certain other consequences of external causes (6.3%) and ill-defined and unknown cause of mortality (6.3%).
The retention rate was 93.7% with four sudden-death-bereaved individuals dropping out at 12 months (three withdrew and one died from natural causes) and 76.2% at 24 months with a further 11 dropping out (six were not contactable, four withdrew and one died from natural causes; Figure 1).
Although our inclusion criteria comprised immediate family members more widely, in the sudden-death-bereaved group we received responses only from close family members including partners, parents, children and siblings. Therefore, for comparability 10 family members were removed from the suicide-bereaved group in the analysis. Considering that the police form could include multiple family members, in the suicide-bereaved group 10 families had two bereaved family members each and 2 families had three. In the sudden-death-bereaved group, one family had two bereaved and the other had three.
Interview and measures
The interview followed a semi-structured format including mainly validated psychological scales/questionnaires. The primary instrument to measure grief reactions was the Grief Experience Questionnaire (GEQ; Barrett and Scott, 1989). The wording of the questionnaire was changed from ‘spouse’ in the original to the name of the person who died. The GEQ is designed to measure two general types of grief reactions: those expected in any bereavement and those suggested to be specific to suicide, including 11 different grief reactions in total (Barrett and Scott, 1989). We tested the validity of the GEQ in our earlier paper (Kolves et al., 2019), and a good fit was found for a shortened version with eight grief reactions: somatic reactions (Cronbach’s α = 0.81), search for explanation (α = 0.75), loss of social support (α = 0.85), stigmatization (α = 0.82), guilt (α = 0.82), responsibility (α = 0.79), shame (α = 0.79) and rejection (α = 0.83), which is used in the current analysis.
Additional outcome measures included the Depression Anxiety Stress Scale (DASS-21; Lovibond and Lovibond, 1995) and the Beck Scale for Suicide Ideation (BSS; Beck and Steer, 1991). The DASS-21 includes three subscales to measure depression, anxiety and stress in the previous week (Lovibond and Lovibond, 1995). All subscales showed good internal consistency (α values of 0.91, 0.81 and 0.88, respectively). The BSS is a 21-item self-reporting instrument developed to measure the presence and intensity of suicidal intent in the previous week (Beck and Steer, 1991). The BSS also showed good internal consistency (α = 0.84). Background information about the bereaved and the deceased was collected, including sociodemographic information, history of psychiatric problems and suicidality. The follow-up interview included the GEQ, DASS-21, BSS and additional items regarding the participants’ recovery from distress.
Statistical analysis
Descriptive statistics including means, standard deviations and t tests were used to compare continuous variables, and the chi-square or Fisher’s exact test to compare categorical variables.
For the main analyses, linear mixed-effects modelling for repeated measures (MMRM) with restricted maximum likelihood estimation was applied to predict the outcome variables. The MMRM deals with within- and between-subject variance and accounts for the correlation between the repeated measures (Detry and Ma, 2016). It also accommodates unbalanced data with the assumption that missing data are missing at random. The outcome measures including grief reactions (GEQ-8), depression, anxiety, stress (DASS-21 subscales) and suicide risk (BSS) were used as dependent variables. All scales except the score of the BSS had normal distribution (the range for skewness or kurtosis between ‒1.5 and +1.5) (Tabachnick and Fidell, 2013). Time was included as a repeated effect. Fixed effects of group (suicide vs sudden death), time and interaction of group by time were the main estimates (all measured as categorical variables) to identify differences between the two bereavement groups, changes over time and group and time interaction. Models were adjusted for confounding factors including kinship type, gender, age, diagnosis of mental illness, self-harm behaviours of both the deceased and the bereaved (chosen based on previous literature; Pitman et al., 2016) and included as fixed effects. All models were applied to the levels of family × person (as some bereaved were from the same families, participants were nested within groups). To reduce multicollinearity, all variables included as fixed effects were centred (Kraemer and Blasey, 2004). Random intercepts for participants were included in the model for the correlation of within-person factors at the baseline. First-order autoregressive (AR1) and unstructured (UN) covariance structures were used in the analyses. The AR1 structure was identified as the model with the best fit with all dependent variables according to Akaike’s information criterion (AIC). To test the effect of missingness, we conducted sensitivity analyses. First, we compared the effect of missingness on the background characteristics and the outcome measures at T0 using chi-square and t tests. Second multiple imputation, considered as a superior method to replace missing data, was performed. We conducted 20 imputations considering the proportion of dropouts at T2 (Graham et al., 2007).
As noted above, the BSS did not have a normal distribution and was zero-inflated. Two-stage imputation as recommended by MacNeil-Vroomen et al. (2016) was conducted. After the imputation, as suggested by Beck et al. (1999), the BSS score was split into ‘lower risk’ (score 0–1) and ‘higher risk’ (2+), and mixed-effects logistic regression suitable for a dichotomous variable was used. Unlike the mixed-effects linear model, the mixed-effects logistic regression does exclude individuals with missing outcome measures from the analysis. Therefore, only imputed results are presented for this analysis. A probability level of 0.05 was employed. SPSS version 25.0 was used.
Results
In total, 142 suicide-bereaved (73.2% females, average age = 52.7) and 63 sudden-death-bereaved (69.8% females, average age = 53.2 years) persons participating at T0 were included in the analysis. The suicide-bereaved group included significantly more parents, 51.4% vs 27%; χ2(1) = 10.57, p = 0.001, and less partners, 28.2% vs 49.2%; χ2(1) = 8.53, p = 0.003, compared to the sudden death bereaved. Dropouts from the suicide-bereaved group were significantly younger (t140 = 2.91, p = 0.004), more likely to be siblings, χ2(1) = 4.57, p = 0.032, and their deceased relatives were more likely to have had a diagnosis of mental illness compared to those who remained in the study, χ2(1) = 6.15, p = 0.013 (Table 1). There were no significant differences between those who remained in the study and those who dropped out in the sudden-death-bereaved group. In addition, comparison of the outcome measures at T0 between dropouts and those who remained in the study did not show any significant differences (Supplementary Table 1).
Background information in suicide and sudden death bereaved at T0 and T2 and differences between non-dropouts and dropouts at T0.
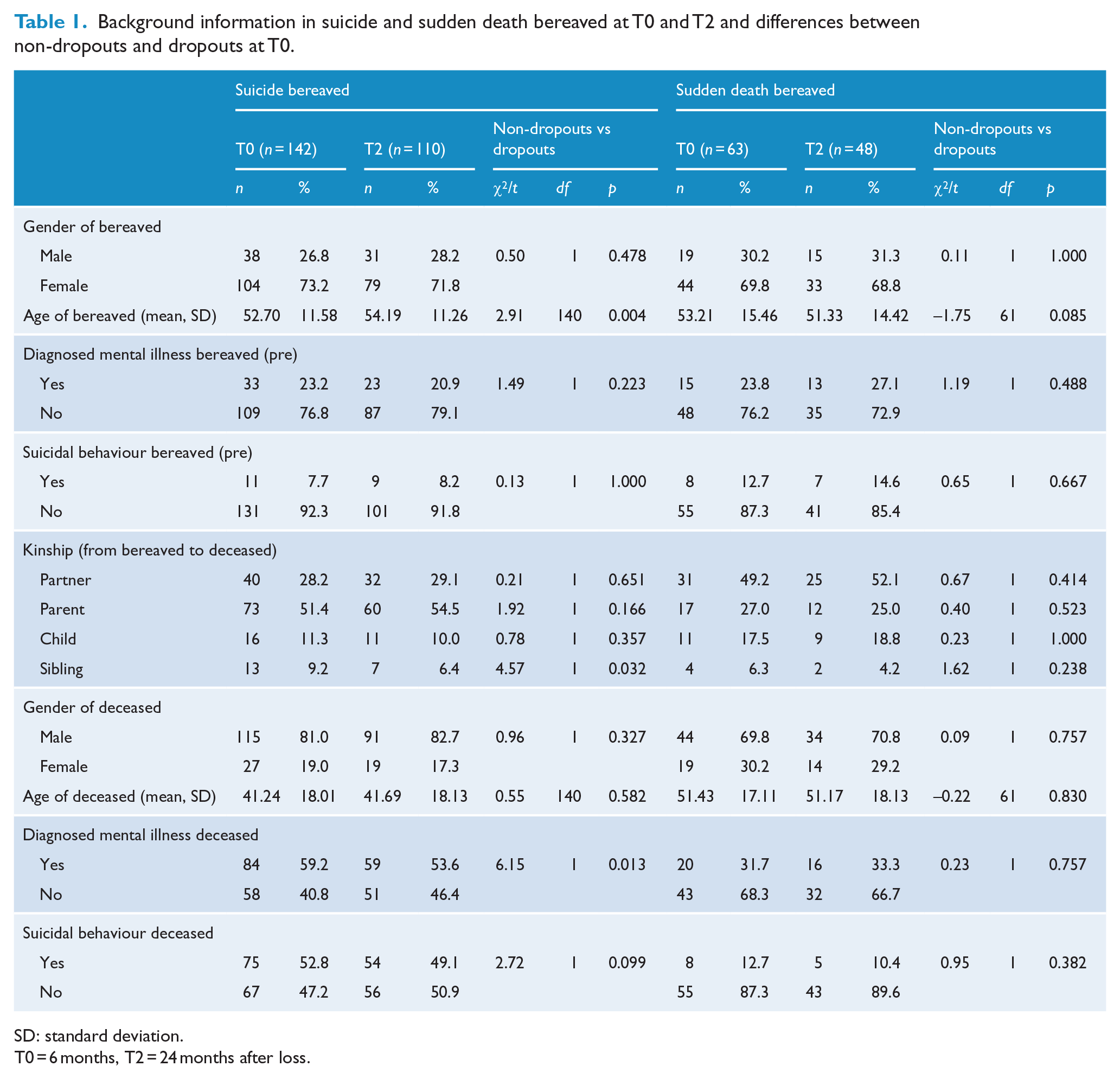
SD: standard deviation.
T0 = 6 months, T2 = 24 months after loss.
Linear mixed models for repeated measures were first adjusted for kinship, gender and age of the bereaved and deceased and then further adjusted for prior mental illness and suicidal behaviour of the bereaved and the deceased (Table 2). Results showed similar results to the initial adjustments, except for guilt. A significant group effect (higher scores in general in the suicide compared to sudden death bereaved) was found for rejection (F = 35.47, p < 0.001), responsibility (F = 9.53, p = 0.002), stigmatization (F = 7.48, p = 0.007) and shame (F = 7.05, p = 0.009). A significant time effect (reduction) was found for search for explanation (F = 44.60, p < 0.001), somatic reactions (F = 21.07, p < 0.001), rejection (F = 10.46, p < 0.001) and stigmatization (F = 4.97, p = 0.008) for bereaved individuals in general. Significant time and group interactions were found for rejection (F = 4.60, p = 0.011) and somatic reactions (F = 3.78, p = 0.024), which showed a decline in the suicide bereaved but almost no change in the sudden death group. There were no significant differences for depression, anxiety and stress levels at the group level and for group and time interaction; however, all had a significant time effect indicating a decline in scores (Table 2). Our sensitivity analyses showed that results based on the multiple imputations were consistent. However, for stigmatization and DASS-21 subscales, the time effects based on the multiple imputations were no longer significant. Therefore, any interpretation regarding the time effects for those constructs should be treated with caution. For suicide risk (measured by the BSS) mixed-effects logistic regression after multiple imputation was utilized, and no significant results were found.
Models of mixed linear regression for repeated measures (fixed estimates).
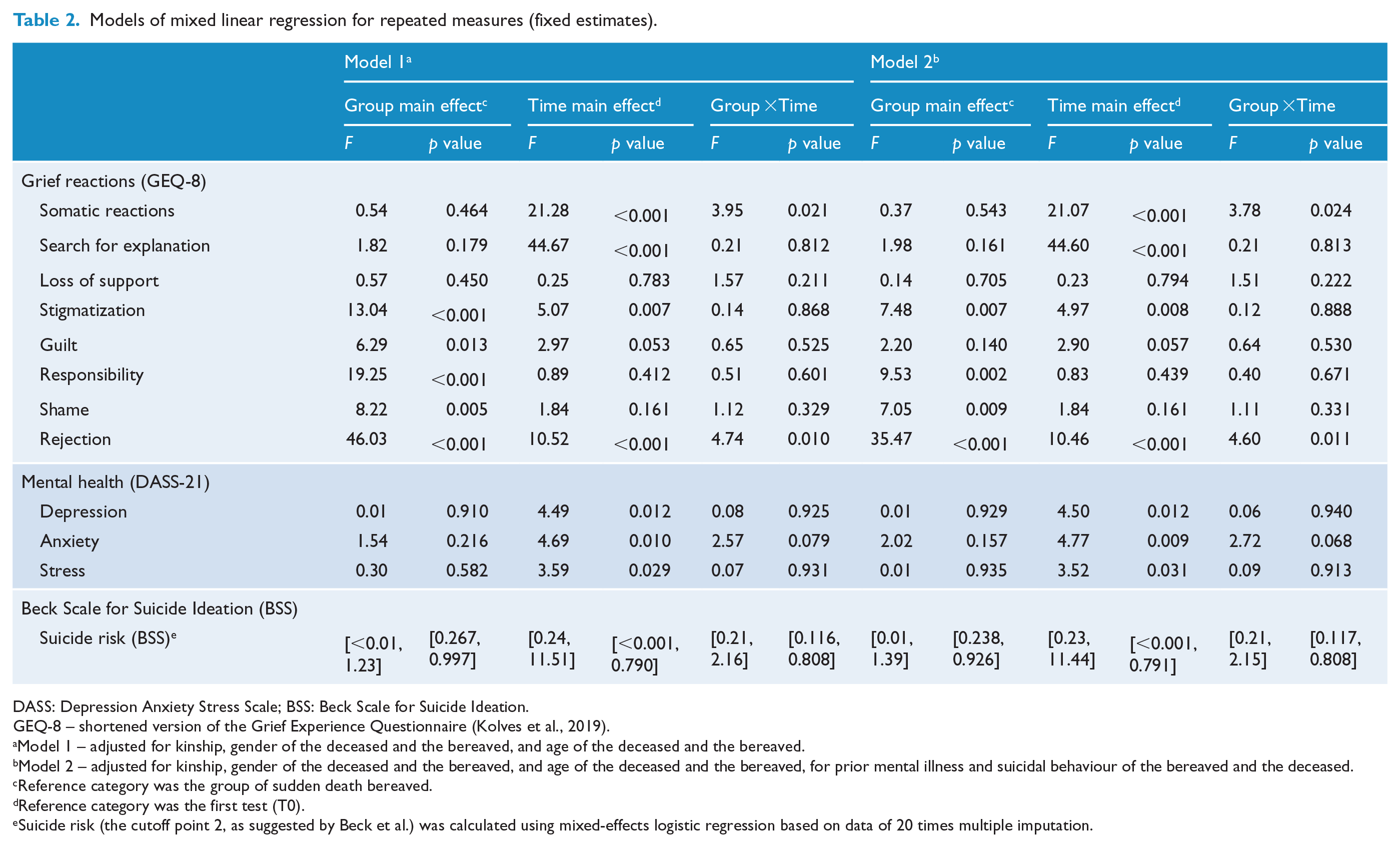
DASS: Depression Anxiety Stress Scale; BSS: Beck Scale for Suicide Ideation.
GEQ-8 – shortened version of the Grief Experience Questionnaire (Kolves et al., 2019).
Model 1 – adjusted for kinship, gender of the deceased and the bereaved, and age of the deceased and the bereaved.
Model 2 – adjusted for kinship, gender of the deceased and the bereaved, and age of the deceased and the bereaved, for prior mental illness and suicidal behaviour of the bereaved and the deceased.
Reference category was the group of sudden death bereaved.
Reference category was the first test (T0).
Suicide risk (the cutoff point 2, as suggested by Beck et al.) was calculated using mixed-effects logistic regression based on data of 20 times multiple imputation.
Figures 2 and 3 present significant differences between suicides and sudden death reactions at specific time points using t tests. The suicide bereaved had significantly higher levels of rejection (T0: t = 8.62, p < 0.001; T1: t = 5.44, p < 0.001; T2: t = 5.58, p < 0.001), responsibility (T0: t = 5.77, p < 0.001; T1: t = 4.83, p < 0.001; T2: t = 4.63, p < 0.001), stigmatization (T0: t = 3.95, p < 0.001; T1: t = 3.54, p = 0.001; T2: t = 3.43, p = 0.001) and guilt (T0: t = 3.22, p = 0.001; T1: t = 2.39, p = 0.018; T2: t = 2.48, p = 0.014) for all time points. Search for explanation was significantly higher in the suicide-bereaved group at T0 (t = 2.53, p = 0.012) and T1 (t = 2.03, p = 0.044), shame at T0 (t = 2.63, p = 0.009) and T2 (t = 2.30, p = 0.023), and somatic reactions at T0 (t = 2.53, p = 0.012). There were no significant group differences for DASS-21 subscales and prevalence of suicide risk.
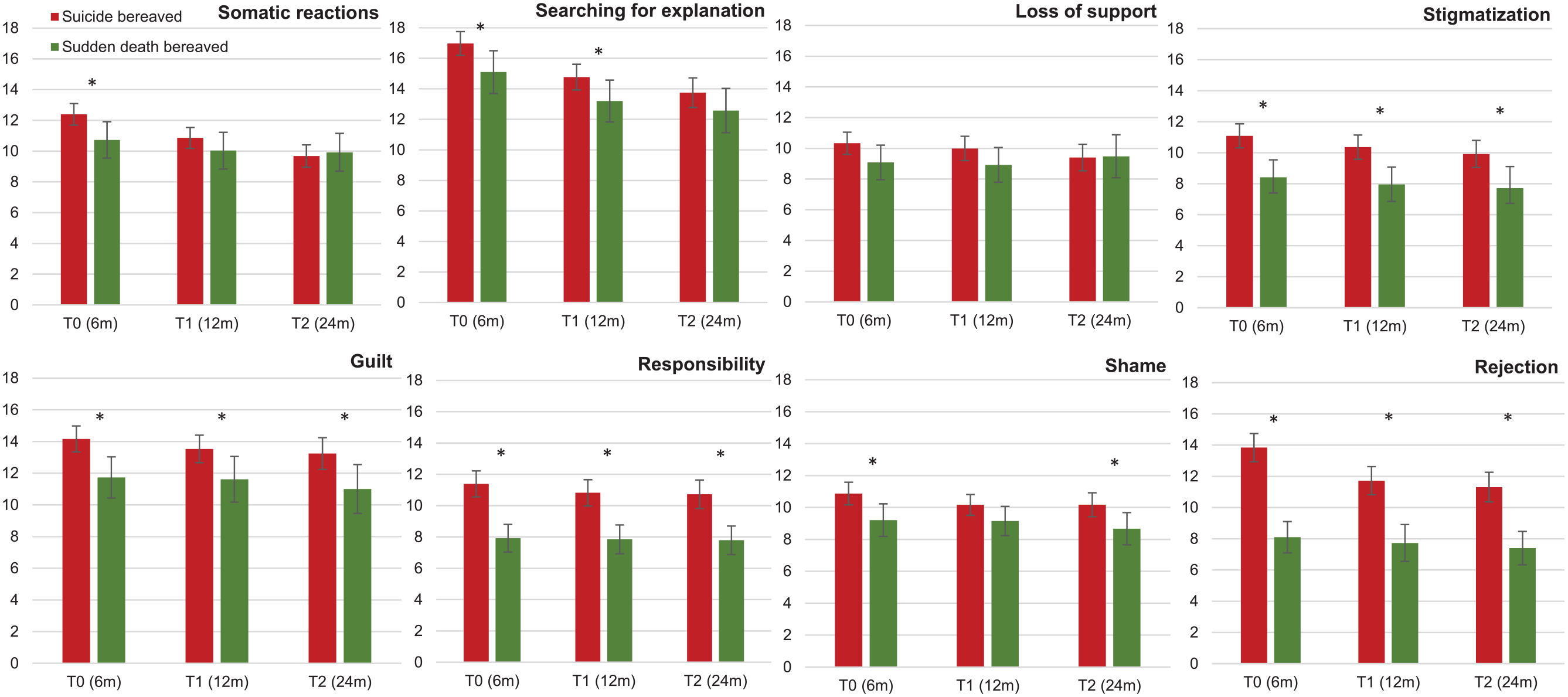
Grief reactions (GEQ-8 – mean scores with 95% CIs) in suicide and sudden death bereaved at different time points.
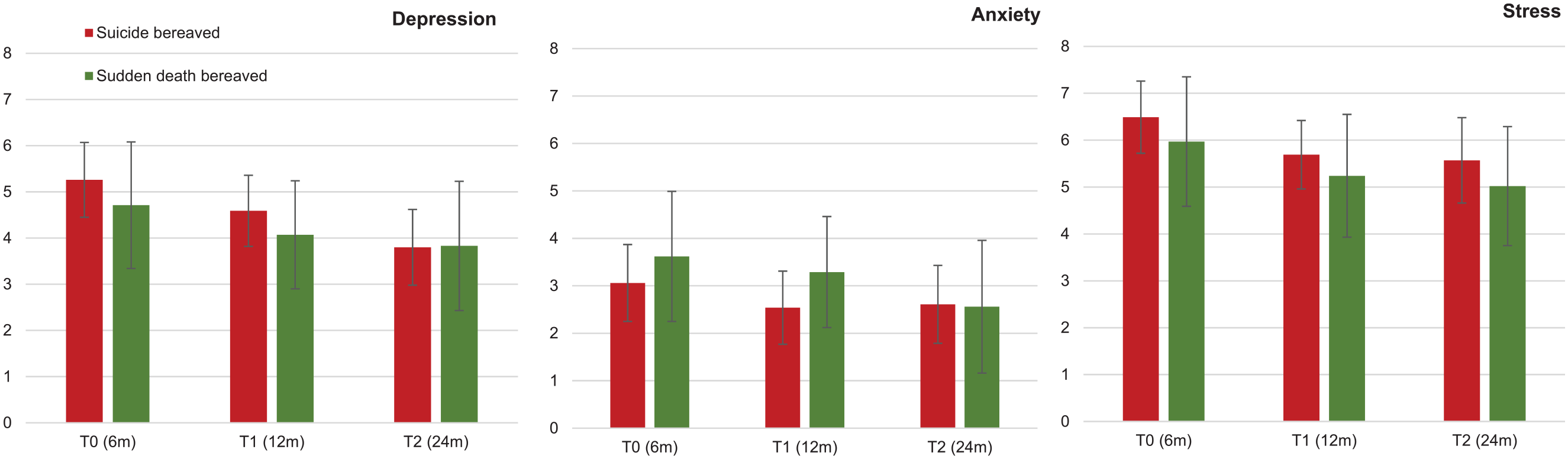
Depression, anxiety and stress (DASS 21 – mean scores with 95% CIs) in suicide and sudden death bereaved at different time points.
Discussion
There are only a limited number of longitudinal studies analysing changes in suicide bereavement that include a comparison group, with the majority from Northern America. Our study is the first Australian study comparing suicide bereavement to sudden death bereavement longitudinally over 2 years since the loss of a loved one. The main outcomes of the current analysis are specific grief reactions using the GEQ-8, which was validated in our earlier paper (Kolves et al., 2019), as well as mental health (DASS-21) and suicidality (BSS). To our knowledge, this is the first study internationally to use a non-convenience sample to measure time, group and time by group effects relating to suicide and sudden death bereavement outcomes.
Significant differences in specific grief reactions between the suicide and sudden death bereaved were found over the 2-year period, after adjusting for potential confounding factors. Overall, bereavement reactions were consistently higher over time for stigmatization, guilt, responsibility and rejection in those bereaved by suicide than by sudden death, and were higher for those bereaved by suicide at one or more time point for somatic reactions, search for an explanation and shame. Irrespective of the cause of the bereavement, family members tended to show significant reductions over time in somatic reactions, searching for an explanation, feelings of stigmatization and rejection, and symptoms of depression, anxiety and stress. Reductions were greater for the suicide bereaved in terms of somatic reactions and feelings of rejection but, at 24 months, the suicide bereaved continued to show greater feelings of stigmatization, guilt, responsibility, shame and rejection than those bereaved by sudden death. Although some earlier studies have also found significantly higher levels of shame and rejection in suicide bereaved compared to the sudden death and natural death bereaved, those studies were not longitudinal and the majority of comparisons were unadjusted for confounding factors (Pitman et al., 2014; Sveen and Walby, 2008).
The finding of significantly higher levels of stigmatization in the suicide bereaved compared to the sudden death group over the 2-year study period is consistent with the recent results of Pitman et al. (2016), who were the first to demonstrate a significant difference between suicide and sudden death bereaved, rather than compared only to the natural death bereaved. However, their study was cross-sectional and therefore did not consider changes over time. Although stigmatization declined over time for both groups, the level continued to be higher in the suicide bereaved. Of particular concern was that a reduction over time was not evident for shame. Both are important grief reactions that impact on help seeking and should be considered in postvention activities. Levels of responsibility and guilt did not change over the 2 years in either group. Some researchers believe that responsibility is an antecedent as well as a consequence of guilt (Berndsen and Manstead, 2007). Nevertheless, responsibility, similarly to earlier studies, was found to be significantly higher in the suicide bereaved than in the sudden death bereaved (Pitman et al., 2014). In contrast, guilt did not differ significantly between groups after adjusting for the diagnosis of mental illness and suicidal behaviour for the bereaved and for the deceased. Although there is still no clear answer whether the suicide bereaved experience higher levels of guilt compared to sudden death bereaved, Pitman et al. (2016) reported higher levels of guilt in blood relatives of suicide bereaved.
Interestingly, we did not find any effects for loss of social support. Earlier literature reviews have noted conflicting results for social support (Pitman et al., 2014; Sveen and Walby, 2008). Furthermore, Sveen and Walby (2008) suggested that results were dependent on the data collection method, and differences according to type of bereavement have been found in studies using the interview method. Although our study also used the interview method, we did not find differences between the suicide and sudden death groups, nor changes over time. Nevertheless, other studies may have operationalized social support differently.
We did not identify differences on the mental health variables of the bereaved – depression, anxiety and stress over time, nor at specific time points. Overall, the average scores were relatively low: only the depression score was above five, indicating mild depression at 6 months (Lovibond and Lovibond, 1995). There was a significant decline in mental health problems over time for participants in general in the main analysis, but this was not confirmed by our sensitivity analyses. Nevertheless, a significant decline in depression has been presented previously in Slovenian and US studies of suicide-bereaved spouses using the Beck Depression Inventory (Farberow et al., 1992; Grad and Zavasnik, 1999). A Dutch study of a mixed sample of close suicide-bereaved relatives showed a longer-term decline in depression scores up to 8–10 years after suicide loss (de Groot and Kollen, 2013). Similarly to earlier individual-level studies (Farberow et al., 1992), suicidal ideation did not differ between the suicide and sudden death bereaved and did not change over time.
In the wider context of our results, it is important to note that the understanding of bereavement has undergone a transformational change in recent decades, and stage theories and other beliefs about grief occurring in a certain predictable way have become outdated (Andriessen et al., 2017; Hall, 2014). In contrast, more recent perspectives such as the dual-process model (Stroebe and Schut, 2010) regard grieving as a dynamic and fluctuating process of coming to terms with the loss of a loved one. Indeed, our earlier qualitative analysis of parents bereaved at 6 and 12 months provided support for the dual-process model as a useful framework for understanding the individual and fluctuating pathways of bereavement reactions in adapting to bereavement over time (Ross et al., 2018). Searching for answers and sense-making was identified as a key theme, and although some parents indicated finding acceptance of their loss at both the 6- and 12-month time points, it is likely that they were oscillating between the loss and restoration-oriented processes as described by the dual-process model. Our current analysis indicated that search for answers declined significantly over the 2-year time period. This is consistent with the dual-process model which purports that, over time, oscillation between opposing grief processes results in a weakening of bereavement reactions such as searching for answers, eventually leading to adaptive coping.
Methodological considerations
The strengths of the study include systematic recruitment using the information obtained from police forms, prospective longitudinal design, use of validated scales, rigorous statistical analysis of repeated measures and adjustment for confounding factors. Nevertheless, our study has some limitations, including different recruitment methods. Response rates in the different groups varied but were comparable to earlier studies (de Leo et al., 2013; Farberow et al., 1992). However, including all bereaved family members into one study would not be feasible considering that police reports only include the closest family members. Although numbers for rare outcomes such as suicide risk are limited by small numbers, retention rates for our study were comparable to earlier studies (Farberow et al., 1992; Grad and Zavasnik, 1999).
Implications
Although our findings confirm that there are several common dimensions to experiencing a ‘sudden’ type of death in a family, a number of differences were found over 2 years depending on the type of death. This suggests that different postvention strategies may be required over extended time periods, dependent upon the nature of the bereavement. Considering that most attention to postvention in national strategies and policies focuses on immediate reactions, the issue of longer-term emotional support for the bereaved needs to be highlighted. Clinicians should consider that some grief reactions such as shame, responsibility, quilt and loss of social support, with two first being higher in the suicide group, did not change over time. While rejection and somatic reactions declined over time for the suicide bereaved, the same did not occur for the sudden-death-bereaved group. Therefore, there is a need for clinicians to pay closer attention to the grief experience peculiar to the suicide or sudden death, such as in counselling or grief support services as well as via evaluation of somatic conditions in persons presenting to general practitioners (GPs) up to 24 months after the experienced loss. Professional development and education for counselling and clinical disciplines providing support services should incorporate awareness of the common impacts of suicide and sudden types of loss which may require prolonged attention. This could be embedded into relevant tertiary education and professional development training programmes.
Further focus on testing different postvention services and grief interventions is required. A recent systematic review suggested that simple interventions (e.g. writing interventions) can reduce the intensity of suicide-specific aspects of grief and may reduce longer-term impacts (Linde et al., 2017). Nevertheless, another review highlighted weakness of the current intervention studies and continued lack of evidence (Andriessen et al., 2019).
In sum, higher levels of rejection, stigmatization, shame and responsibility remaining in the suicide bereaved 2 years after their loss suggest that the suicide bereaved remain stigmatized. This has important implications for the clinical services associated with individual/family counselling as well as community postvention or grief responses.
Supplemental Material
Supplementary_file – Supplemental material for Suicide and sudden death bereavement in Australia: A longitudinal study of family members over 2 years after death
Supplemental material, Supplementary_file for Suicide and sudden death bereavement in Australia: A longitudinal study of family members over 2 years after death by Kairi Kõlves, Qing Zhao, Victoria Ross, Jacinta Hawgood, Susan H Spence and Diego de Leo in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to acknowledge the clinical interviewers, and study participants. They would also like to recognize Queensland Department of Justice, Office of State Coroner (OSC) for assistance with recruitment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the Griffith University Encouragement Grant and the Australian Research Council Discovery Grant ‘Bereavement of suicide and sudden death’ (No. ARC DP140102567).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.