
Abstract
Background:
Many concerns have been raised regarding the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria for Internet gaming disorder and International Classification of Diseases, 11th Revision (ICD-11) criteria for gaming disorder.
Aims:
In this study, we demonstrated the diagnostic validity of each criterion for Internet gaming disorder in the DSM-5 in terms of their intensity and frequency thresholds and evaluated functional impairments, unhealthy behaviors and complications among adults with Internet gaming disorder and gaming disorder.
Methods:
We recruited 69 subjects with Internet gaming disorder, 69 regular gamers and 69 controls without regular gaming based on diagnostic interviewing conducted by a psychiatrist according to the DSM-5 Internet gaming disorder criteria.
Results:
Except for the ‘deceiving’ and ‘escapism’ criteria, all criteria for Internet gaming disorder had a diagnostic accuracy ranging from 84.7% to 93.5% in differentiating between adults with Internet gaming disorder and regular gamers. A total of 44 participants with Internet gaming disorder (63.8%) fulfilled the gaming disorder criteria. In addition, 89% and 100% of the Internet gaming disorder and gaming disorder groups, respectively, had academic, occupational or social functional impairment. Both the Internet gaming disorder and gaming disorder groups had higher rates of delayed sleep phase syndrome and insomnia. The gaming disorder group also had a higher obesity proportion.
Conclusion:
The ‘deceiving’ and ‘escapism’ criteria had relatively lower diagnostic accuracy. Both the Internet gaming disorder and gaming disorder groups demonstrated functional impairments and unhealthy behaviors. They also exhibited complications, such as obesity and sleep disorders. These results support the utility of the DSM-5 Internet gaming disorder and ICD-11 gaming disorder criteria in identifying individuals who need treatment for both gaming addiction symptoms and complications resulting from the addiction.
Introduction
The Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) proposed the diagnostic criteria for Internet gaming disorder (IGD) to define Internet gaming addiction. Based on these criteria, the global prevalence is estimated to range between 0.5% and 6% (Petry et al., 2015). Several researchers have raised concerns about the threshold, validity and utility of the DSM-5 criteria for IGD (Kuss et al., 2017a; Starcevic, 2017). The International Classification of Diseases, 11th Revision (ICD-11) also recently included its own definition of gaming disorder (GD). More empirical data are required to evaluate the diagnostic validity and utility of both the DSM-5 IGD and ICD-11 GD criteria to resolve scholars’ concerns (Aarseth et al., 2017).
DSM-5 IGD
Starcevic (2017) criticized the polythetic, nonhierarchical DSM-5 diagnostic criteria for IGD and the inadequate support for ‘withdrawal’ and ‘tolerance’ as criteria. Escape and preoccupation were frequently observed not only among individuals with IGD but also among casual gamers (Ko et al., 2014; Przybylski et al., 2017; Rehbein et al., 2015) and provided little information on the severity of IGD (Király et al., 2017). Establishing a reasonable severity threshold for each criterion was suggested to distinguish between casual gamers and those with IGD (Ko and Yen, 2014) to prevent false positives. Furthermore, functional impairment caused by gaming was proposed as a required criterion (Griffiths et al., 2016). Petry et al. (2015) argued that the presentation of criteria should be clinically significant. However, how impairment should be investigated and measured by clinicians has yet to be demonstrated. Therefore, it is crucial to evaluate the differences in functional impairment between healthy gamers and those with IGD to determine the threshold of clinical significance.
ICD-11 GD
The ICD-11 included GD as an addictive disorder in 2018 (World Health Organization, 2018). Some researchers have cautioned against including GD in the ICD-11 because of insufficient scientific evidence (Van Rooij et al., 2018). However, many other clinicians and researchers have supported it based on clinical evidence and in the interest of public health (Higuchi et al., 2017; Rumpf et al., 2018). Numerous critical concerns, such as the possible over-pathologizing of casual gamers and the utility of diagnosis, have been raised (Aarseth et al., 2017; Van Rooij et al., 2018). Thus, evaluating the diagnostic validity (i.e. the ability to distinguish a case of GD from a healthy gamer) and diagnostic utility (i.e. implication of assigning a patient to GD, Jablensky, 2016, such as indication of required intervention) is necessary to resolve such concerns (Higuchi, 2017).
Complications associated with IGD
King and Delfabbro (2018) stated that it is imperative to determine the specific harm to players induced by IGD. However, the link between IGD and social, mental and physical health has not been well evaluated (Przybylski et al., 2017). Physical complications, which can be more objectively evaluated, are a crucial area for determining whether IGD and GD are harmful. Sleep problems, such as limited sleep time, have been correlated with IGD based on self-report questionnaires (Hawi et al., 2018; Macgregor, 2000; Männikkö et al., 2015). However, unhealthy behaviors and physical complications attributed to excessive gaming have yet to be evaluated through objective diagnostic interviews.
Evaluating IGD and GD diagnostic criteria
Most studies have evaluated IGD on the basis of nonstandard approaches, such as questionnaires (Yao et al., 2017), which might limit the definition of functional impairment and exaggerate the severity of IGD. Furthermore, the criteria should be evaluated in terms of their ability to distinguish between individuals with IGD and healthy gamers (Griffiths et al., 2016; Mueller, 2018). On the basis of standard evaluations of reasonable comparison subjects, the sensitivity and specificity of each criterion can be evaluated to develop more effective diagnostic formula (Mueller, 2018).
To address the concerns raised by other scholars (Griffiths, 2018; Kardefelt-Winther et al., 2017; Király et al., 2015; Kuss et al., 2017a; Mueller, 2018), in this study, we evaluated the diagnostic accuracy of IGD criteria, compared the DSM-5 criteria for IGD and the ICD-11 criteria for GD, and demonstrated the functional impairment, risky health behaviors and complications associated with IGD and GD.
Methods
Participants
Individuals with IGD (IGD group), regular gamers (RGs) (RG group) and nongamers (control group) were recruited through advertisements around university campuses and on the online bulletin board systems of universities in Taiwan from April 2017 to February 2018. The following inclusion criteria were adopted for the IGD group: (1) aged 20–38 years with an education of >12 years; (2) online video game activity of ⩾4 hours per day on weekdays and ⩾6 hours per day on weekends and (3) consistent pattern of Internet gaming maintained for >2 years. We listed the aforementioned criteria, study evaluation process, financial incentives for the evaluation (1100 New Taiwan Dollars for diagnostic study) and contact information in the advertisements. Individuals who met the inclusion criteria participated in diagnostic interviews based on the IGD criteria defined in the DSM-5 to confirm the diagnosis.
The participants in the RG and control groups were frequency-matched by gender and age (±3 years) with the participants in the IGD group. The recruitment criteria for the participants in the control group were that their nonessential Internet use was <4 hours per day (Ko et al., 2014) and that this time did not involve regular gaming. The RGs participated in regular online gaming (⩾3 days per week) without fulfilling the diagnostic criteria of IGD. The diagnosis of both groups was confirmed through psychiatric interviewing.
The diagnostic interviews comprised three parts as follows: (1) a diagnostic interview based on the DSM-5 criteria for IGD with intensity and frequency thresholds; (2) the Chinese version of the Mini-International Neuropsychiatric Interview (Sheehan et al., 1998) to exclude participants with psychotic disorders, bipolar I disorder and substance abuse disorders and evaluating comorbidity and (3) a history-taking interview to exclude mental retardation, severe physical disorder and brain injury. All participants were interviewed by an experienced psychiatrist who specialized in IGD, and the interviews lasted between 20 minutes and 1 hour. In total, 207 participants—69 in each group—were included after obtaining informed consent. This study was conducted in accordance with the Declaration of Helsinki. This human study was approved by the Institutional Review Board of Kaohsiung Medical University Hospital. All participants provided written informed consent to participate in this study.
Measures
DSM-5 criteria for IGD
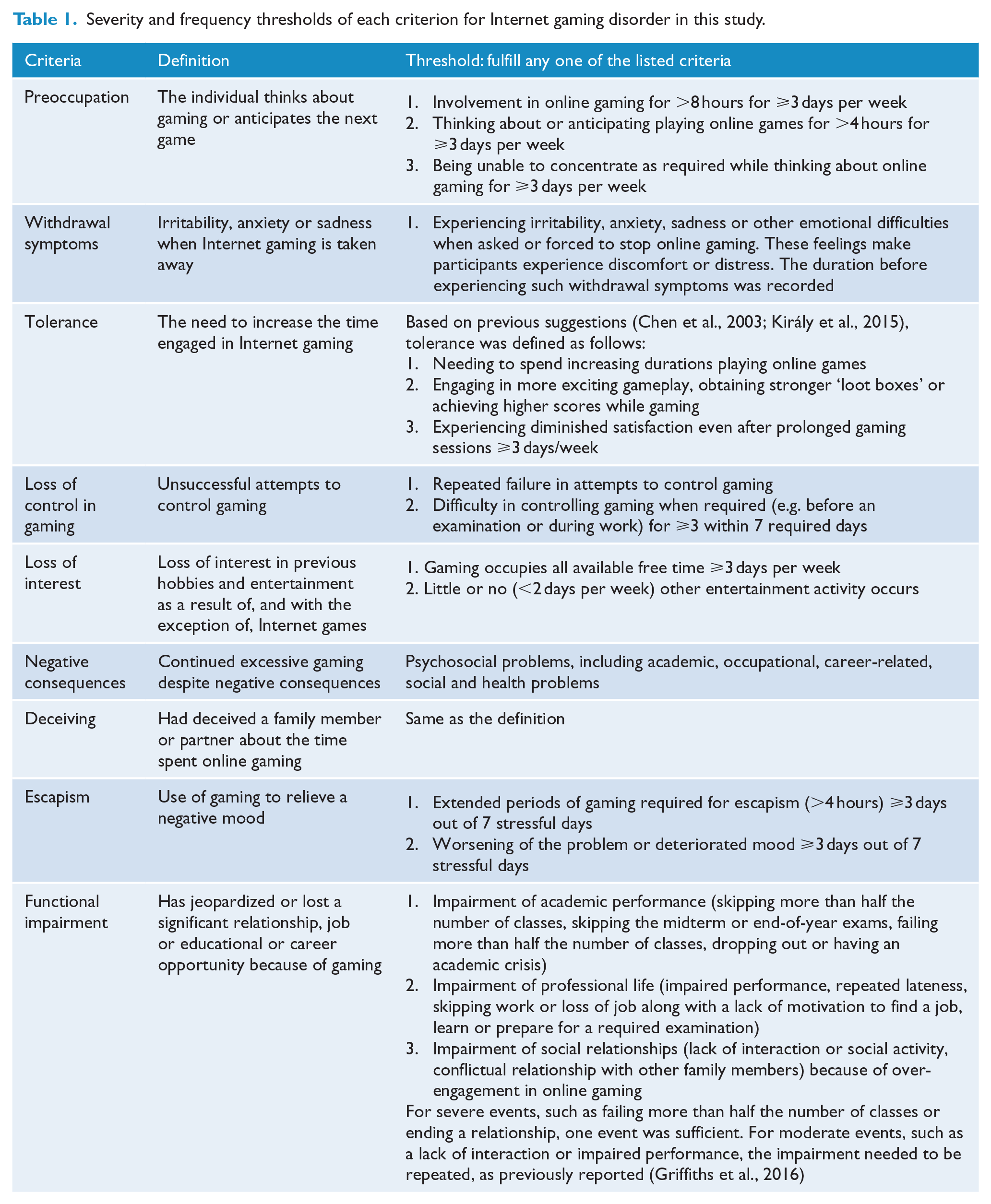
We developed a semi-structured interview schedule to examine the severity and frequency of each DSM-5 criterion for IGD. The thresholds to fulfill the criteria are presented in Table 1. Participants fulfilling five or more criteria were included in the IGD group.
Severity and frequency thresholds of each criterion for Internet gaming disorder in this study.
Unhealthy behaviors or health problems
The problems resulting from engagement in online gaming included inadequate sleep time (<4 hours for ⩾2 days per week), turning night into day, irregular diet (skipping meals), immobilization (>4 hours for ⩾3 days per week), no exercise (for >3 weeks), eye problems since engaging in online gaming, increased body weight, wrist or back pain and others.
Diagnostic criteria of GD in ICD-11
The criteria for GD are as follows: (1) impaired control over gaming habits; (2) increased priority given to gaming to the extent that gaming tasks take precedence over other activities and (3) continued gaming despite negative consequences. These behavioral patterns result in marked functional impairment over a period of >12 months. In this study, participants with GD were required to fulfill the severity thresholds mentioned in the fourth, fifth, sixth and ninth criteria of the DSM-5 IGD.
Diagnostic criteria for hazardous gaming
Hazardous gaming (HG) refers to a gaming pattern that increases the risk of harm to physical or mental health. Participants who played games online for >25 hours per week and experienced at least one of the academic, social and family functional impairments, unhealthy behaviors or health problems were included in the HG group, if they did not fulfill the ICD-11 criteria for GD.
Complications from IGD or GD
Obesity
Participants with a body mass index of >27 kg/m2 were classified as obese according to the definition established by the Taiwan Ministry of Health and Welfare.
Insomnia disorder
Insomnia was diagnosed by a psychiatrist based on (1) the difficulty faced initiating or maintaining sleep or nonrestorative sleep; (2) significant distress or functional impairment and (3) symptoms occurring at least three nights per week for at least 3 months according to the DSM-5 criteria.
Delayed sleep phase syndrome
The psychiatrist interviewed participants on (1) whether their preference in eveningness was fixed; (2) whether they were unable to fall asleep if they had tried to sleep earlier and (3) whether they had trouble sleeping when their sleep pattern was disrupted. The participants who answered positively to these three questions, went to bed later than 1 a.m. and woke up later than 9 a.m. were categorized as having delayed sleep phase syndrome.
Chen Internet Addiction Scale—Gaming Version
The Chen Internet Addiction Scale (CIAS) is a 26-item self-report instrument scored on a four-point Likert-type scale ranging from 1 (does not match my experience at all) to 4 (definitely matches my experience). It assesses the severity of the Internet addiction with scores ranging from 26 to 104 (Chen et al., 2003). The colloquial expressions of the CIAS—Gaming Version were modified to assess the participants’ online gaming experiences, with a Cronbach’s α of 0.96 (Ko et al., 2005). A high score indicated a high severity of IGD.
Statistical analysis
One-way analysis of variance was conducted to evaluate the differences in age, education level and severity of IGD among the IGD, RG and control groups. The chi-square test was used to evaluate the differences in demographics and sleep behavior among the three groups. The performance of the criteria for distinguishing IGD from regular gaming was evaluated by determining their diagnostic accuracy ([true positive + true negative]/all). The chi-square test was also used to evaluate the association between the DSM-5 and ICD-11 diagnostic criteria and their association with unhealthy behaviors, functional impairment and complications. A p < 0.05 was considered significant for all analyses, which were performed using SPSS version 20.0.
Results
A total of 69 participants were included in the IGD group. Female participants comprised 21.7% of each group. The IGD group had a higher CIAS score (82.87 ± 10.49) than did the RG (55.87 ± 14.69) and control (30.86 ± 8.11) groups (Table 2). The CIAS scores of all controls were lower than the cutoff point for Internet addiction proposed in a previous study (Ko et al., 2005). Therefore, we analyzed the diagnostic validity of the criteria only in the IGD and RG groups.
Gender, age, job, gaming time, sleep time and severity of Internet gaming disorder of all participants.
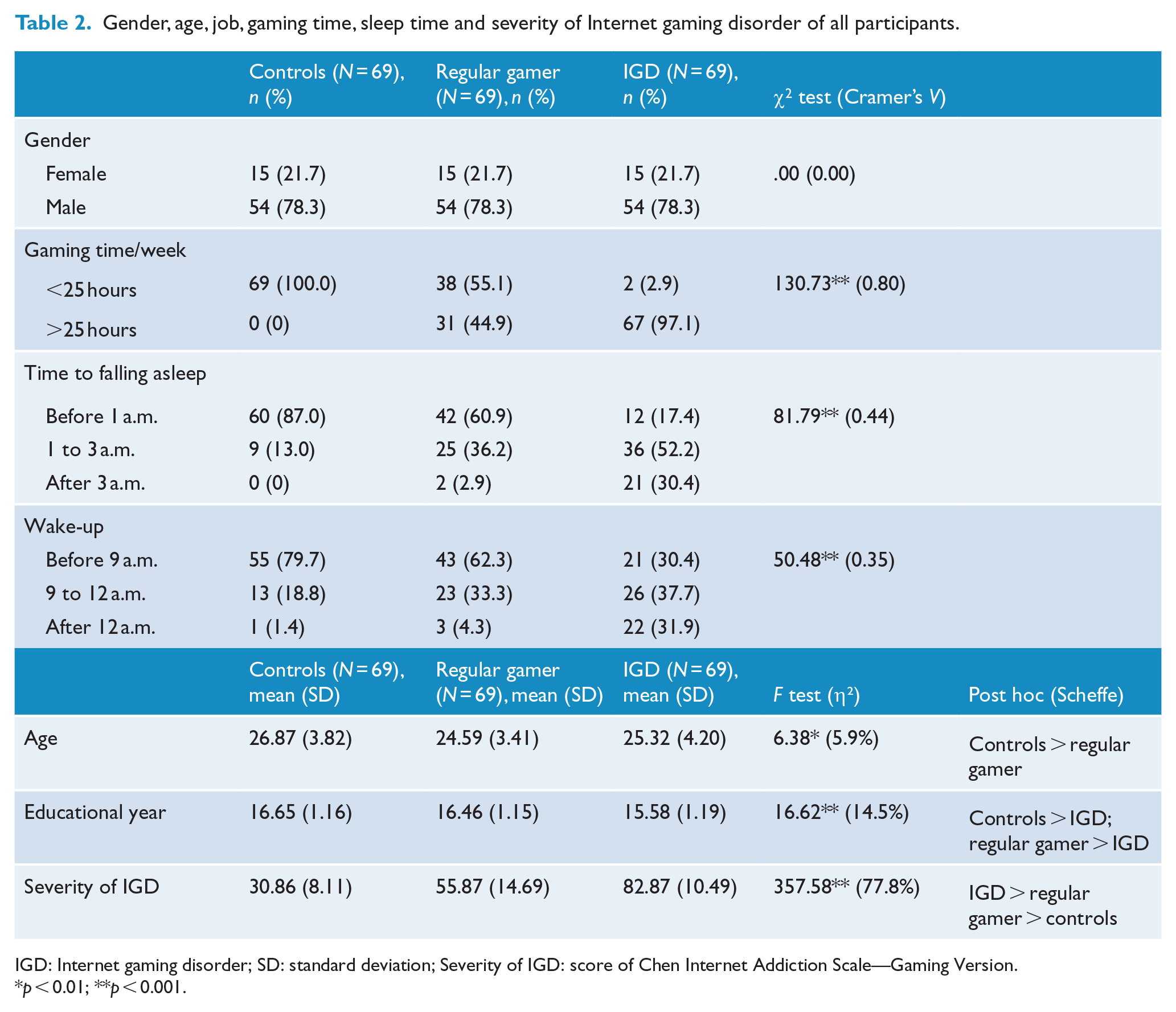
IGD: Internet gaming disorder; SD: standard deviation; Severity of IGD: score of Chen Internet Addiction Scale—Gaming Version.
p < 0.01; **p < 0.001.
Diagnostic validity of the DSM-5 criteria
The diagnostic accuracy for the ‘preoccupation’ criterion was 84.7% (Table 3). A total of 52 (75.4%), 10 (14.5%) and 31 (44.9%) participants played online games for >8 hours a day ⩾3 days a week, thought about online gaming when they were not playing for >4 hours a day ⩾3 days a week, and were preoccupied with online gaming even though they needed to do other things, respectively. Details on the frequency and severity of all criteria are provided in Supplementary Data 1.
Diagnostic validity of each criterion of Internet gaming disorder (IGD) and the association between the diagnostic criteria of IGD and those of ICD-11 gaming disorder.
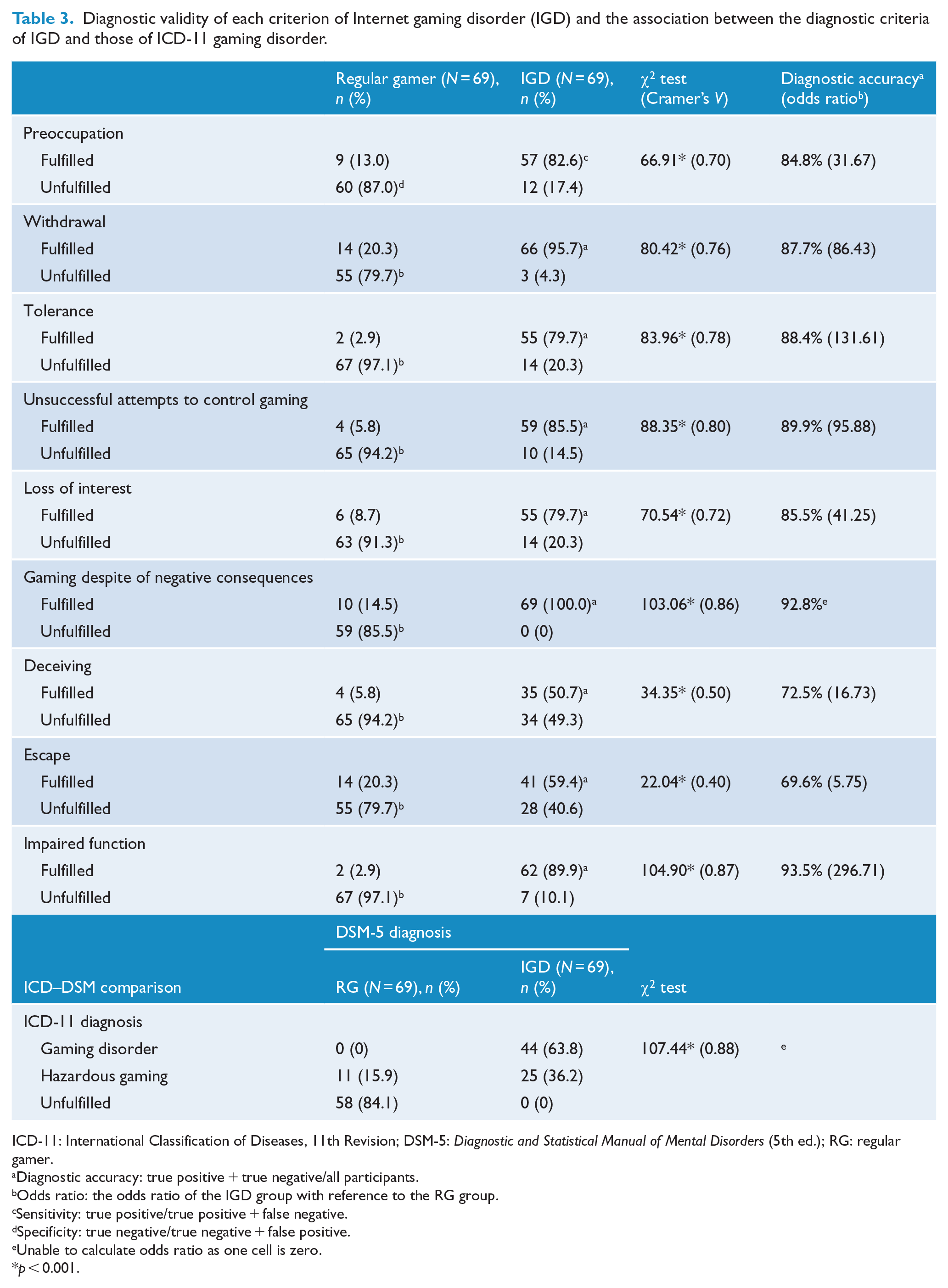
ICD-11: International Classification of Diseases, 11th Revision; DSM-5: Diagnostic and Statistical Manual of Mental Disorders (5th ed.); RG: regular gamer.
Diagnostic accuracy: true positive + true negative/all participants.
Odds ratio: the odds ratio of the IGD group with reference to the RG group.
Sensitivity: true positive/true positive + false negative.
Specificity: true negative/true negative + false positive.
Unable to calculate odds ratio as one cell is zero.
p < 0.001.
The ‘withdrawal’ criterion had a diagnostic accuracy of 87.7%. The interval between the interruption of gaming and the experience of these symptoms was 1, 2–3, 4–5 and 6–7 days in 27 (40.9%), 34 (51.5%), 1 (1.5%) and 4 (6.1%) participants, respectively, in the IGD group (Supplementary Data 1).
The ‘tolerance’ criterion had a diagnostic accuracy of 88.5%. A total of 19 (27.5%), 31 (44.9%) and 41 (59.4%) participants sought to extend the duration of their online gaming sessions, ‘grinded’ gaming content (to access ‘loot boxes’ or more content) and felt unsatisfied even after prolonged gaming time ⩾ 3 days a week, respectively. Grinding is the act of performing repetitive tasks to advance one’s character level and to unlock content such as ‘loot boxes’, which are randomized consumable virtual items. The grinding can be bypassed and the virtual items can be accessed by paying money.
The ‘unsuccessful attempts to control gaming’ criterion had a diagnostic accuracy of 89.9%. A total of 45 (65.2%) participants failed in their attempts to control their online gaming addiction. In addition, 41 (59.4%) participants failed to control their gaming time when required to do so ⩾3 out of 7 days.
The ‘loss of interest’ criterion had a diagnostic accuracy of 85.6%. A total of 54 (78.3%) participants had no other interests or had other interests less than twice a week. Furthermore, 45 (65.2%) participants played games for so long that they had no time for any other interest ⩾3 days a week.
The ‘gaming despite negative consequences’ criterion had a diagnostic accuracy of 92%. All participants in the IGD group reported at least one health, academic, occupational or social negative consequence resulting from online gaming.
The ‘deceiving others about the time spent gaming’ criterion had a diagnostic accuracy of 72.5%.
The ‘escapism’ criterion had an accuracy of 69.6%. A total of 48 (82.8%) participants spent >4 hours gaming to escape, and 33 (56.9%) participants experienced increased stress and emotional difficulty after playing. A total of 41 (59.4%) participants escaped with these problems ⩾3 days out of 7 stressful days (Table 3 and Supplementary Data 1).
A total of 89.9% of the IGD group fulfilled the final criterion of ‘functional impairment’. Of these participants, 21 (30.4%), 30 (43.5%) and 44 (63.8%) reported academic, occupational and social functional impairment, respectively. Among the participants in the IGD group, 42.0% and 2.9% had impairments in two or three dimensions, respectively.
Comparison of diagnosis between DSM-5 and ICD-11
Based on the definition of GD in the ICD-11, 44 participants in the IGD group (63.8%) fulfilled the criteria (Table 3). A t test demonstrated that those who fulfilled the ICD-11 criteria had significantly higher CIAS scores (86.5 ± 10.46) than did those in the IGD group (76.5 ± 7.09; t = 4.70; p < 0.001; Cohen’s d = 1.11). This result suggests that the ICD-11 has a higher threshold for the diagnosis of GD than does the DSM-5.
A total of 25 participants in the IGD group and 11 RGs had at least one functional impairment caused by excessive gaming. They were categorized in the HG group based on ICD-11 criteria.
Unhealthy behaviors or health problems in the IGD and GD groups
The frequency of unhealthy behaviors and health problems was higher among the IGD group than it was among the RG group, except for eye discomfort (p = 0.085; Table 4). Furthermore, significant differences existed in the percentage of unhealthy behaviors among the GD, HG and RG groups. The three most frequent unhealthy behaviors or health problems encountered in the IGD and GD groups were immobilization, inadequate sleep time and turning night into day.
Functional impairments and unhealthy behaviors among the DSM-5 Internet gaming disorder (IGD) and ICD-11 gaming disorder (GD) groups.
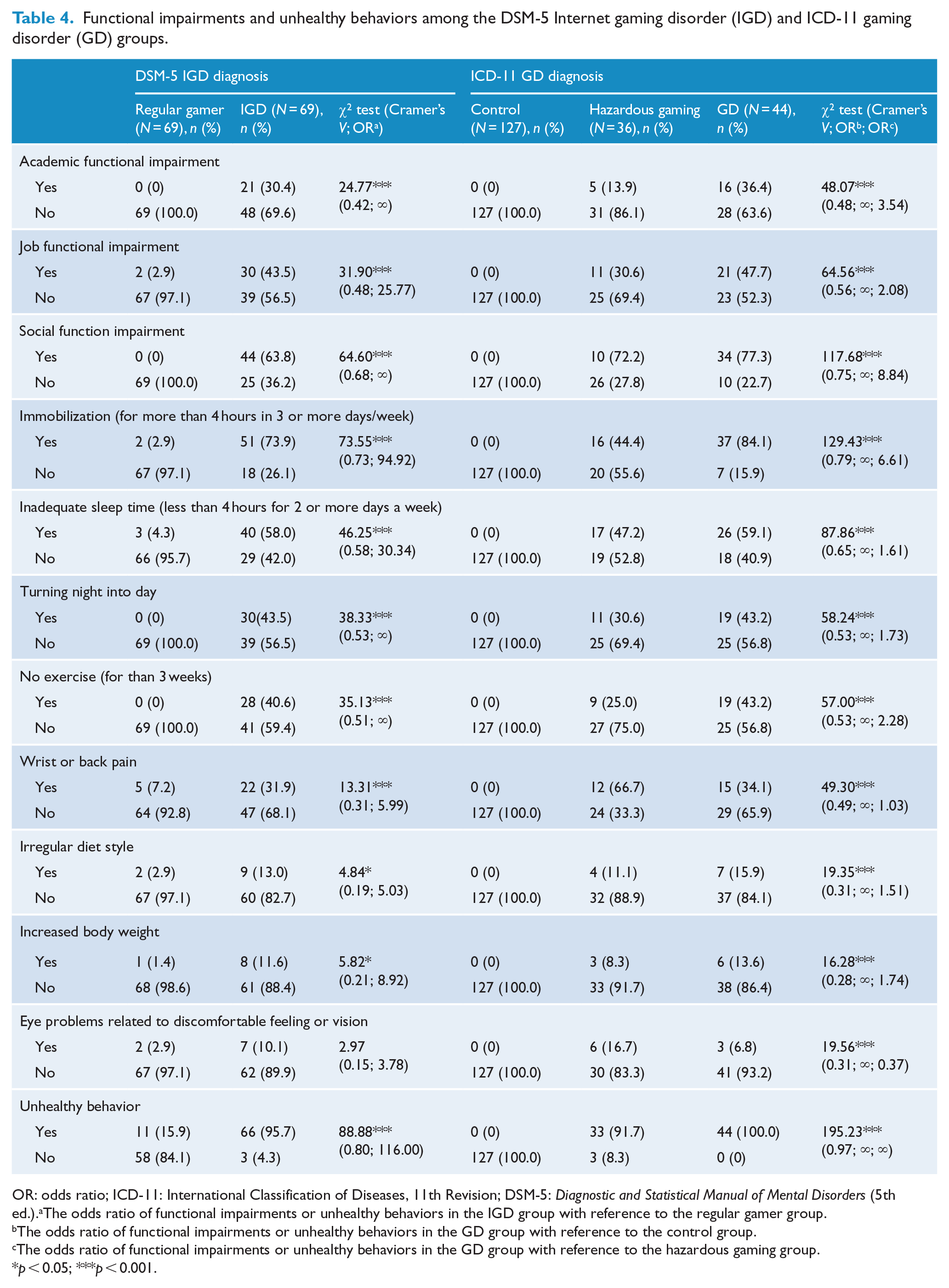
OR: odds ratio; ICD-11: International Classification of Diseases, 11th Revision; DSM-5: Diagnostic and Statistical Manual of Mental Disorders (5th ed.).aThe odds ratio of functional impairments or unhealthy behaviors in the IGD group with reference to the regular gamer group.
The odds ratio of functional impairments or unhealthy behaviors in the GD group with reference to the control group.
The odds ratio of functional impairments or unhealthy behaviors in the GD group with reference to the hazardous gaming group.
p < 0.05; ***p < 0.001.
Complications caused by IGD and GD
The participants in the IGD group had a significantly higher occurrence of delayed sleep phase syndrome and insomnia than did the controls; moreover, their percentage of obesity trended higher (p = 0.06; Cramer’s V = 0.16) than the controls. In addition, the percentage of obesity, delayed sleep phase syndrome and insomnia in the GD group was higher than that in the control group (Table 5).
Complications of DSM-5 Internet gaming disorder (IGD) and ICD-11 gaming disorder (GD).
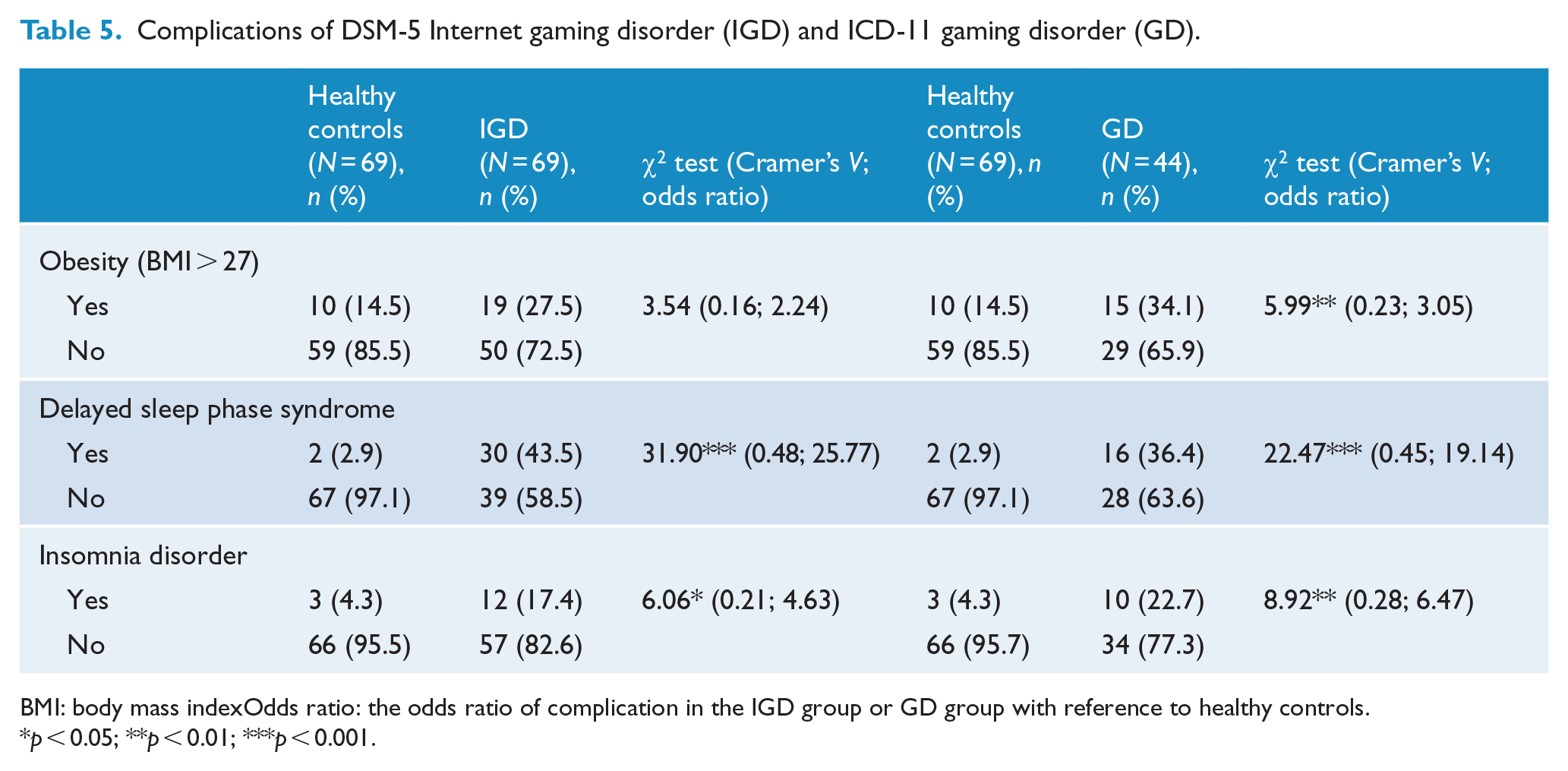
BMI: body mass indexOdds ratio: the odds ratio of complication in the IGD group or GD group with reference to healthy controls.
p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
Diagnostic validity of the criteria of IGD based on frequency and severity
This study is the first to provide clear information regarding the frequency and severity of each IGD criterion by its their validity using diagnostic interviews. All criteria, except for ‘deceiving’ and ‘escapism’, had a diagnostic validity higher than 80%. The following discussion examines each criterion and proposes suggestions for determining their thresholds.
Preoccupation
Based on previous works on preoccupation (Griffiths et al., 2016; King and Delfabbro, 2014; Kuss et al., 2017a), we considered the time spent gaming and the time being distracted by gaming as indicators of preoccupation. Smartphone gamers were often required to return to a game to obtain ‘loot boxes’ available at a limited time. Potenza (2018) reported that a patient died while his or her care provider was gaming. Our study reveals that gaming can distract 75.4% of individuals with IGD from work-related tasks or other activities, which should be addressed to prevent negative consequences.
Withdrawal
A total of 61 (88%) individuals with IGD experienced withdrawal symptoms within 3 days after stopping games (one participant on the 4th–5th day and four participants on the 6th–7th day). Emotional difficulties are not easily distinguishable from a craving response when symptoms emerge on the 6th–7th day. Therefore, we suggest limiting the duration to 3 days for this criterion to measure the experience of withdrawal symptoms. However, most participants with IGD rarely experienced this symptom (Kaptsis et al., 2016) because gaming is highly accessible and alternative activities, such as watching other players stream, can attenuate the withdrawal feeling. Therefore, this claim and the concrete mechanism underlying these emotional presentations must be confirmed in future experimental studies.
Tolerance
Only 28% of the IGD group participants increased their gaming time to maintain their sense of satisfaction. For those gaming >8 hours per day, there was limited room to further extension of gaming time. Even after prolonged gaming, 58% of the IGD group participants experienced dissatisfaction. Therefore, we could promote alternative healthy interests for individuals with IGD by discussing the unsatisfactory state experienced when increasing tolerance.
Unsuccessful attempts to control gaming
Healthy gamers can intermittently lose control while gaming without severe negative consequences. The severity and frequency thresholds of this criterion prevented false positives (6.3%) and resulted in a diagnostic accuracy of 89.9% in this study.
Loss of interest
Kuss et al. (2017a) and Billieux et al. (2013) suggested that a reasonable replacement of other interests by gaming should not be problematic unless it leads to detrimental consequences. Under this threshold, only 8.7% of the RG group participants fulfilled the criterion in our study. This suggested that a reasonable threshold could provide an indicator of true ‘impaired interest’, the loss of interest in activities other than gaming, but not ‘replaced interest’, which is simply a relative preference for gaming among various other interests.
Gaming despite negative consequences
All individuals with IGD fulfilled this criterion. This might suggest that even if one individual reached a reasonable threshold for other criteria, all had significant negative consequences in their daily life. This result could support the ICD-11 GD criteria to recruit it as a required criterion.
Deceiving
In this study, this criterion had the second lowest diagnostic accuracy of 72.5%, which was similar to the results from another diagnostic study (Ko et al., 2014) that reported a diagnostic accuracy of 68%. Its sensitivity (50.7%) was too low to be an effective criterion (Király et al., 2015; Ko et al., 2014).
Escapism
It is normal to relieve negative emotions through leisure activities such as gaming, and many gamers view the use of gaming to escape as a positive feature (Wood and Griffiths, 2007). In the RG group, 38 participants (55%) exhibited escapism; however, only 14 of them (20.2%) reached the threshold. This indicated that escaping behaviors did not necessarily result in negative consequences for healthy gamers. However, this criterion had low specificity (66.3%) and diagnostic accuracy (69.6%).
Functional impairment
In total, 42.0% of the IGD group experienced two or more dimensions of impairment. The results also revealed that academic crisis, impaired job performance and inadequate social interaction were the most frequent academic, professional and social problems encountered, respectively (Supplementary Data 1). Interventions could help individuals with IGD cope with these negative consequences to attenuate the vicious cycle. Furthermore, a standard evaluation, such as the World Health Organization Disability Assessment Schedule 2.0, should be conducted in future studies to determine the measurable level of functional impairment in IGD.
ICD-11 GD and HG
In total, 63.8% of the participants in the IGD group fulfilled the GD criteria of the ICD-11. This suggested that ICD-11 had a higher intensity threshold than the DSM-5. This answers a major concern raised in the literature (Aarseth et al., 2017; Van Rooij et al., 2018), namely, the over-pathologizing of normal gaming. In this study, 56.8% of the participants with GD exhibited impaired function in two or more dimensions, and all of them reported unhealthy gaming behaviors. Several scholars have raised concerns about the lack of scientific evidence of mental or physiological complications from GD (Aarseth et al., 2017; Przybylski et al., 2017). This study demonstrated that the participants with GD had higher rates of obesity, delayed sleep phase syndrome and insomnia. This suggests the clinical utility of identifying people with GD in need of further help, not only for their addictive gaming behaviors but also for other complications resulting from gaming.
In addition, 25 participants with IGD were categorized into the HG group instead of the GD group. HG indicated that gaming behaviors increase the risk of harm to physical or mental health. Therefore, interventions to educate gamers as well as prevent and attenuate these risks are necessary. However, addictive symptoms, such as loss of controls in gaming, also need to be evaluated and addressed.
Unhealthy behaviors and complications from IGD and GD
Previous epidemiological studies have reported no significant difference in mental and physical health between an IGD group and controls (Markey and Ferguson, 2017; Przybylski et al., 2017). In this study based on diagnostic interviews, more than 40% of the participants in the IGD and GD groups experienced immobilization, inadequate sleep, turning night into day and no exercise. Furthermore, the GD group had a higher rate of obesity. Both the IGD and GD groups had higher rates of insomnia disorder and delayed sleep phase syndrome than the control. Because these unhealthy behaviors have to be maintained for a certain period before causing these disorders, these complications might only appear in chronic cases; therefore, the disorders may be less frequently reported in young adolescents. Therefore, more interventions among young people with GD or IGD are required to decrease unhealthy behaviors and the risk of future complications.
Obesity is a risk factor of cardiovascular disorders (Bastien et al., 2014). Insomnia and short sleep duration are associated with mortality from cardiovascular disorders (Bertisch et al., 2018). In addition, immobility contributes to venous thromboembolism (Braithwaite et al., 2016). In this study, 27.5% of the IGD group participants were obese, 30.4% slept after 3 a.m., 58.0% slept for <4 hours for ⩾2 days a week, 43.4% had delayed phase sleep syndrome, 73.9% were immobile and 40.6% did not exercise. These unhealthy behaviors may accumulate and make them predisposed to cardiovascular events. Braithwaite et al. reported a case of pulmonary thrombosis where the patient had been online continuously for a 36-hour period, sitting for up to 12 hours at a desk without getting up before the incident (Braithwaite et al., 2018). Our study revealed clear risk factors for cardiovascular accidents in the IGD group, which raises the question of a possible link between excessive gaming and cardiovascular accidents.
A review suggested that mental health professionals, game developers and the media should work together to build healthy approaches to online games (Kuss et al., 2017b). A new set of features for Facebook and Instagram mobile apps help users manage their time online. Based on our results, we suggest that game developers help gamers manage their time spent gaming, particularly for excessive prolonged gaming and gaming after midnight. Governments must also pay attention to this mental and physical health concern and promote preventive interventions and the necessary regulations, particularly for gaming after midnight and immobilization among adolescents.
Limitations
First, the diagnosis of IGD was reached relying solely on the participants’ responses to a psychiatric interview. Further information gathered from other sources, such as parents or partners, may provide additional details. Second, recall bias could not be excluded without the direct observation of the unhealthy behaviors. Third, this study was conducted before the publication of the ICD-11. Therefore, the diagnosis of ICD-11 for GD was based on similar criteria present in the DSM-5 IGD. Nonetheless, the core concepts were the same, and a severity threshold was required for both the IGD and GD criteria. Additional studies are warranted to determine the reasonable threshold for each GD criterion to correctly identify individuals that need treatment. Finally, to prevent overt heterogeneity and enable matching in a limited sample, we set some inclusion criteria, namely, an education level of >12 years, and excluded participants with severe physical disorders. However, this could have limited the generalization of the present results, such as for children or individuals with physical impairment.
Conclusion
Based on the intensity and frequency thresholds of each criterion, all criteria reached adequate diagnostic accuracy, except for the ‘deceiving’ and ‘escapism’ criteria. The participants in the GD group exhibited at least one functional impairment dimension, and a higher percentage of participants had comorbidity of obesity, delayed phase sleep syndrome and insomnia. They also had a higher frequency of unhealthy behaviors, such as short sleep duration or immobilization. These results support the IGD and GD criteria and indicate that individuals fulfilling those criteria need interventions for the symptoms of addiction, comorbid psychiatric disorders and physiological complications. Furthermore, the ICD-11 GD criteria have a higher threshold than do the DSM-5 IGD criteria; this finding partially addressed the concern regarding over-pathologizing normal gaming behaviors.
Supplemental Material
Supplemnet_revised – Supplemental material for Validity, functional impairment and complications related to Internet gaming disorder in the DSM-5 and gaming disorder in the ICD-11
Supplemental material, Supplemnet_revised for Validity, functional impairment and complications related to Internet gaming disorder in the DSM-5 and gaming disorder in the ICD-11 by Chih-Hung Ko, Huang-Chi Lin, Pai-Cheng Lin and Ju-Yu Yen in Australian & New Zealand Journal of Psychiatry
Footnotes
Author Contributions
C.-H.K. designed the study, acquired the data and drafted the article; H.-C.L. and P.-C.L. contributed to the acquisition and analysis of the data; J.-Y.Y. acquired, analyzed and interpreted the data and gave the final approval for the version to be submitted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the Ministry of Science and Technology (Taiwan) (Nos MOST105-2314-B-037-027-MY2 and MOST107-2314-B-037-101-MY2), Kaohsiung Municipal Hsiao-Kang Hospital (No. KMHK-104-006), Medical University Hospital (No. KMUH105-5R54) and the Research Center for Environmental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan from the Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education in Taiwan (No. NHIRD-1060407). These institutions had no role in the design, process, analysis and production of this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.