
Abstract
Objective:
The five personality disorder trait domains in the proposed International Classification of Diseases, 11th edition and the Diagnostic and Statistical Manual of Mental Disorders, 5th edition are comparable in terms of Negative Affectivity, Detachment, Antagonism/Dissociality and Disinhibition. However, the International Classification of Diseases, 11th edition model includes a separate domain of Anankastia, whereas the Diagnostic and Statistical Manual of Mental Disorders, 5th edition model includes an additional domain of Psychoticism. This study examined associations of International Classification of Diseases, 11th edition and Diagnostic and Statistical Manual of Mental Disorders, 5th edition trait domains, simultaneously, with categorical personality disorders.
Method:
Psychiatric outpatients (N = 226) were administered the Structured Clinical Interview for DSM-IV Axis II Personality Disorders Interview and the Personality Inventory for DSM-5. International Classification of Diseases, 11th edition and Diagnostic and Statistical Manual of Mental Disorders, 5th edition trait domain scores were obtained using pertinent scoring algorithms for the Personality Inventory for DSM-5. Associations between categorical personality disorders and trait domains were examined using correlation and multiple regression analyses.
Results:
Both the International Classification of Diseases, 11th edition and the Diagnostic and Statistical Manual of Mental Disorders, 5th edition domain models showed relevant continuity with categorical personality disorders and captured a substantial amount of their information. As expected, the International Classification of Diseases, 11th edition model was superior in capturing obsessive–compulsive personality disorder, whereas the Diagnostic and Statistical Manual of Mental Disorders, 5th edition model was superior in capturing schizotypal personality disorder.
Conclusion:
These preliminary findings suggest that little information is ‘lost’ in a transition to trait domain models and potentially adds to narrowing the gap between Diagnostic and Statistical Manual of Mental Disorders, 5th edition and the proposed International Classification of Diseases, 11th edition model. Accordingly, the International Classification of Diseases, 11th edition and Diagnostic and Statistical Manual of Mental Disorders, 5th edition domain models may be used to delineate one another as well as features of familiar categorical personality disorder types. A preliminary category-to-domain ‘cross walk’ is provided in the article.
Introduction
It is well established that the categorical personality disorder (PD) diagnoses in International Classification of Diseases, 10th edition (ICD-10) and Diagnostic and Statistical Manual of Mental Disorders (4th and 5th edition; DSM-IV/5) are compromised by serious limitations, including high heterogeneity, arbitrary thresholds and diagnostic overlap, which unfortunately complicates treatment and research (e.g. Widiger and Samuel, 2005). Additionally, there is insufficient evidence supporting that PDs are truly categorical (Trull and Durrett, 2005) or that there are 8–12 discrete PD types (Eaton et al., 2011). In contrast, a dimensional PD model that delineates level of impairment (severity) along with personality traits (style) to dictate its manifestation has significant connection to both scientific evidence and universal utility (Bender, 2013; Bernstein et al., 2007; Tyrer et al., 2015). Consequently, the World Health Organization (WHO) committee for the forthcoming International Classification of Diseases, 11th edition (ICD-11) and the American Psychiatric Association (APA) committee for the DSM-5 have both moved toward dimensional models of PD.
The proposed ICD-11 PD model involves evaluation of severity (mild, moderate or severe PD) and a separate description of five stylistic trait domains comprising Negative Affectivity, Detachment, Disinhibition, Dissociality and Anankastia (WHO, 2017). The ICD-11 trait domain descriptors may be used to characterize the personality features of individuals diagnosed with PD (in the chapter on Mental and behavioral disorders) or Personality difficulty (in the chapter on Factors influencing health status and contact with health services). However, a trait domain should be coded only if its features are prominent in the personality makeup of the individual diagnosed with personality difficulty or disorder, and there is evidence that the characteristics described by the trait domain are associated with impairment in psychosocial functioning. Multiple trait domains may be specified to capture the individual’s characteristics that are relevant to the personality problems (WHO, 2017).
Similarly, the alternative model of personality disorders (AMPD) 1 published in DSM-5 Section III includes evaluation of functioning/impairment (criterion A) and a separate description of 25 stylistic traits (criterion B) that are organized into five domains of negative affectivity, detachment, antagonism, disinhibition, and psychoticism (Krueger et al., 2012). Unlike the ICD-11 proposal, these two criteria are combined to represent six individual PD types retained from Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) as well as a PD diagnosis that is trait specific for those cases where an individual does not map onto any particular type.
This study is only focusing on the trait component of these classification systems and not the severity/functioning component. The domains of Negative Affectivity, Detachment, Antagonism/Dissociality and Disinhibition are concordant across the two systems, whereas the DSM-5 domain of Psychoticism and the ICD-11 domain of Anankastia are not. In the ICD-11 model, trait dimensions of Psychoticism are not included because WHO considers such features (i.e. schizophrenia spectrum disorders) as segregated from PD phenomena (Parnas et al., 2005). Likewise, in the DSM-5 model, the domain of Anankastia is embodied by the facets of rigid perfectionism and perseveration from the (low) Disinhibition and Negative Affectivity domains, respectively (Bach et al., 2017c).
To date, the five proposed ICD-11 PD trait domains have been partially supported by initial empirical evaluations that subsequently have resulted in further revisions and adaptations of the model (Kim et al., 2015; Tyrer et al., 2014). In a preliminary field trial, Kim et al. (2015) reported that the domains of Anankastia, Detachment and Dissociality emerged as sound domains, whereas two separate domains of anxious-dependent and emotionally unstable overlapped too much resulting in a combined domain of Negative Affectivity as evident from the current ICD-11 proposal. The currently proposed ICD-11 five-domain model has been tested in a total sample of 606 psychiatric patients, where Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II)-rated PD symptoms were assigned into one of the five proposed ICD-11 domains (Mulder et al., 2016). Findings from this study failed to confirm the presence of a distinct Disinhibition domain, whereas the remaining four proposed ICD-11 domains were empirically supported (Mulder et al., 2016). However, Disinhibition (or low conscientiousness) has consistently emerged in other factor analytic trait studies and has reliably appeared in research on the DSM-5 AMPD trait system as well as other trait models. Accordingly, there may be an insufficient representation of disinhibition within the DSM-IV criterion sets for its emergence in a discrete factor (Widiger and Oltmanns, 2016). Moreover, Oltmanns and Widiger (2017) have recently developed a self-report inventory for the ICD-11 trait domains, which shows conceptually meaningful convergence with other established measures of personality and personality pathology, including and Eysenck Personality Questionnaire - Revised (EPQ-R) MMPI-2 Personality Psychopathology Five (PSY-5) (Oltmanns and Widiger, 2017). Finally, Bach et al. (2017c) have developed an algorithm for generating ICD-11 domain scores from the Personality Inventory for DSM-5 (PID-5), which was employed in this study (see Table 1). The empirical foundation for the proposed ICD-11 model and the alternative DSM-5 model is reviewed in detail elsewhere (see overviews in Morey et al., 2015; Tyrer et al., 2015). Notably, in contrast to the DSM system, the ICD system is the official world classification system for all diseases, including PD.
Designated PID-5 facets for generating DSM-5 and ICD-11 trait domains.
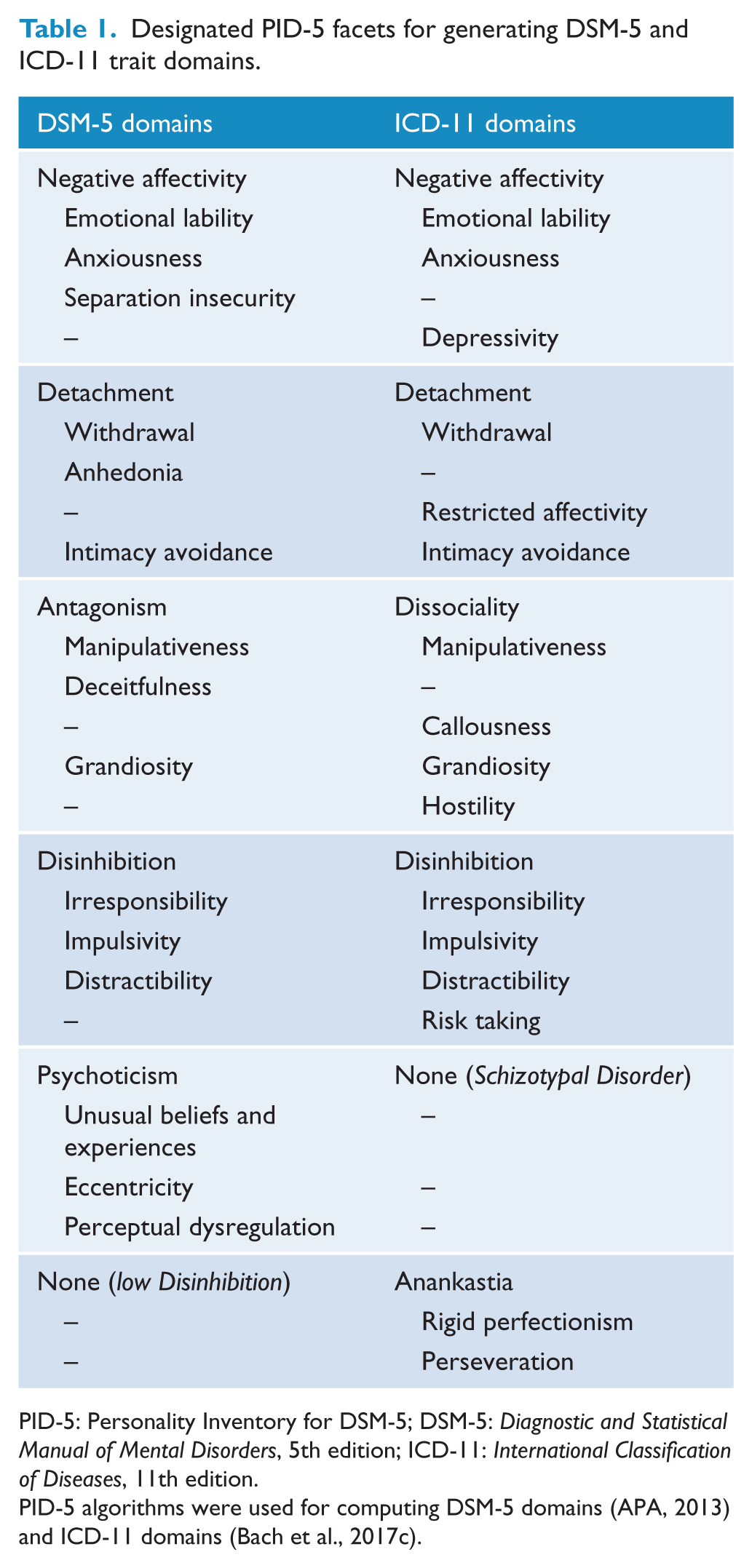
PID-5: Personality Inventory for DSM-5; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th edition; ICD-11: International Classification of Diseases, 11th edition.
PID-5 algorithms were used for computing DSM-5 domains (APA, 2013) and ICD-11 domains (Bach et al., 2017c).
Although both the ICD-11 and the DSM-5 trait models have the potential to provide a much-needed refurbishment of the problematic categorical classification system, it is also vital that valuable clinical information from the categorical PDs is not lost in the transition. In this study, we acknowledged that the somewhat challenging shift from categorical models to new dimensional models will be smoother to the extent that connections across the models are understood and articulated empirically. Accordingly, it is imperative to investigate the continuity between established categorical PDs and the proposed WHO ICD-11 domains, as well as correspondence with the APA DSM-5 AMPD trait domains.
The goal of this study was to explore the association (i.e. continuity) of the five ICD-11 domains versus five DSM-5 domains with the 10 categorical PD types. 2 This served as the first examination of the ICD-11 personality domains’ ability to capture categorical PD types using a new scoring algorithm that has already been established (see Bach et al., 2017c) that seeks to harmonize between the DSM-5 trait systems and the proposed ICD-11 PD domains. The boldfaced associations in Table 4 indicate hypothesized domain–disorder relationships according to previous conceptualizations and empirical findings (e.g. Anderson et al., 2014; Hopwood et al., 2012; Skodol et al., 2011).
Method
Participants and procedure
This study was based on consecutively recruited outpatients (N = 226), of which 142 patients were from a psychiatric hospital unit specialized in the assessment and treatment of PDs and emotional disorders (setting 1), and 84 patients were from a liaison psychiatry clinic specialized in the treatment of functional disorders (setting 2). Ages for the total sample ranged from 18 to 58 years (M = 32.54; SD = 10.02). Approximately 58% were women; 57% were in a relationship; 35% had regular employment or were students, whereas 65% were unemployed or on long-term sick leave; 64% had finished high school and/or college, whereas 36% had only completed elementary school.
All patients (setting 1 and 2) were included in the study in terms of a naturalistic design and were examined with structured diagnostic interviews performed by a clinical psychologist (first author) and a psychiatrist (third author), as a part of their clinical assessment program for research and clinical purposes. Patients in setting 1 were examined with Mini International Neuropsychiatric Interview (MINI; Sheehan et al., 1998), whereas patients in setting 2 were examined with Schedules for Clinical Assessment in Neuropsychiatry (SCAN; Wing et al., 1990). Both interviews were used to operationalize and characterize the DSM-IV/5 criteria for common mental disorders as presented in Table 2.
Characteristics of DSM-5 Section II personality disorders and common mental disorders.
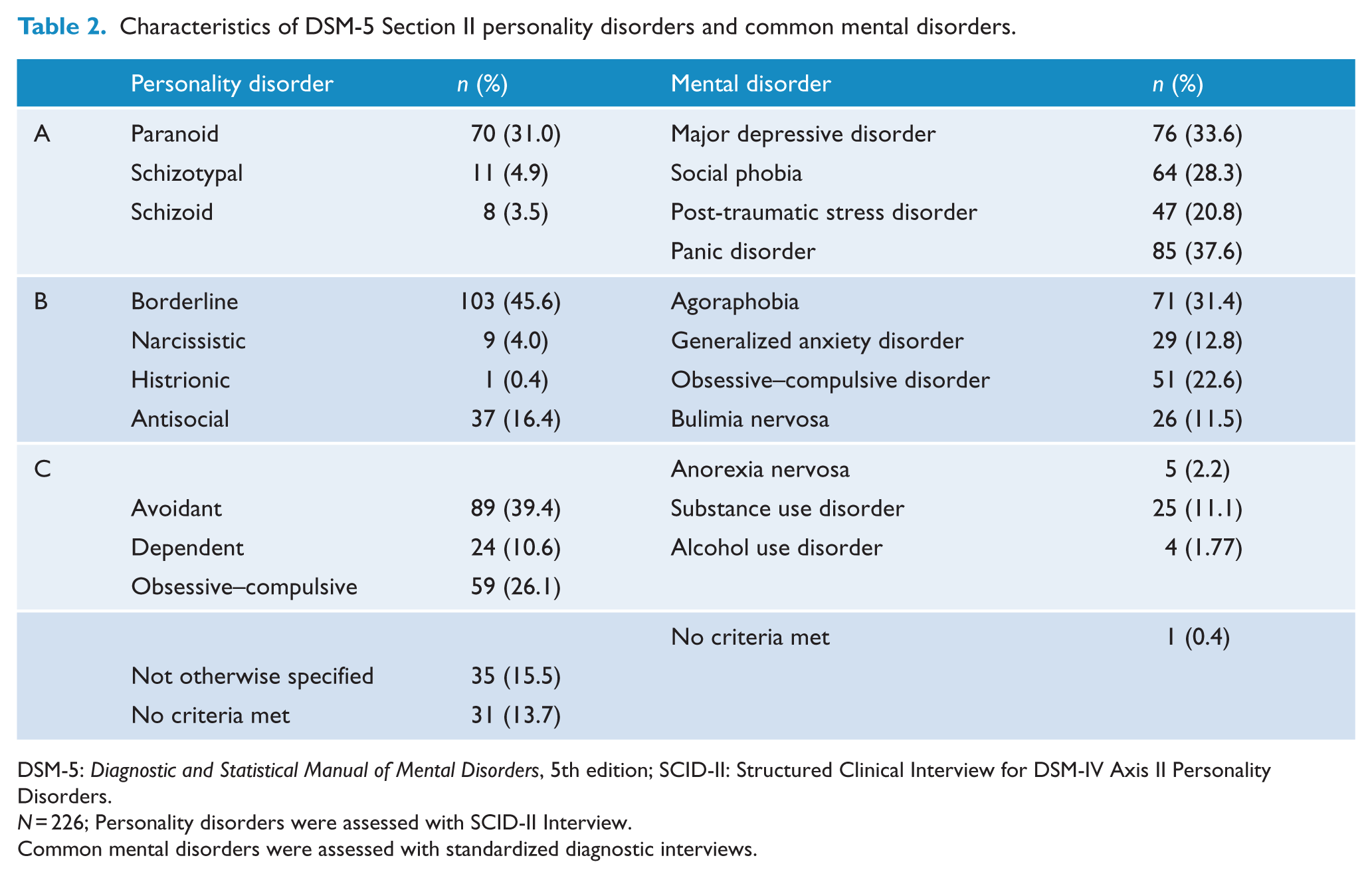
DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th edition; SCID-II: Structured Clinical Interview for DSM-IV Axis II Personality Disorders.
N = 226; Personality disorders were assessed with SCID-II Interview.
Common mental disorders were assessed with standardized diagnostic interviews.
Personality trait data and sociodemographic information were obtained using secure online questionnaire software. As presented in Table 2, all patients met the criteria for at least one DSM-IV/5 nonpsychotic disorder, and two-thirds of the patients met the diagnostic criteria for a PD. Patients suspected of having a current organic brain disorder, substance-induced condition, psychotic disorder, severe depression, autism or manic episode would not have been included; however, no such patients were excluded in this study as they were all correctly referred to our clinics. All patients gave informed consent, and the study was approved by the Regional Ethics Committee of Zealand. The data used in this study are not freely accessible due to regulations by the Danish Data Agency, but they are available upon individual request.
Instruments
SCID-II
The SCID-II was used to measure PDs, categorically and dimensionally. Dimensional scores were computed by adding the number of fulfilled polythetic criteria for each category (i.e. criterion count; First et al., 1994). All SCID-II interviews were performed and recorded independently of the administration and scoring of the self-reported pathological trait dimensions (PID-5). In setting 1, 13 randomly selected SCID-II interviews were concurrently inter-rated by a blinded psychologist. In setting 2, 10 randomly selected interviews were video-recorded and subsequently inter-rated by a blinded psychologist. The two raters and inter-raters were thoroughly trained and supervised in the SCID-II assessment procedure. Acceptable inter-rater reliability was identified for both inter-raters on the basis of criterion counts, with two-way random intra-class correlation coefficients of 0.977 and 0.823, respectively. Descriptive statistics for SCID-II criterion counts are presented in supplemental Table S1 and Table S2.
PID-5
The PID-5 is a 220-item self-report inventory measuring the pathological traits (i.e. 25 trait facets and five high-order trait domains) of the alternative DSM-5 model for PDs, as well as corresponding traits in the proposed ICD-11 model (Bach et al., 2017c; Krueger et al., 2012). Patients were required to rate each PID-5 item on a 4-point Likert scale from 0 (Very False or Often False) to 3 (Very True or Often True). We used the Danish version of the PID-5, which has demonstrated acceptable psychometric properties (Bach et al., 2016, 2017b; Bo et al., 2016) and facet-level continuity with categorical PDs (Bach et al., 2016, 2017a; Bach and Fjeldsted, 2017; Bach and Sellbom, 2016). In this study, we used the official scoring algorithm for computing the DSM-5 trait domains (APA, 2013) and a newly developed scoring algorithm for computing the proposed ICD-11 domains (Bach et al., 2017c). 3 As shown in Table 1, the two algorithms included 15 and 16 PID-5 facets, respectively. In this study, alpha coefficients for all PID-5 facets used in the two algorithms ranged from 0.74 (Irresponsibility) to 0.95 (Eccentricity) with a median alpha of 0.87. Descriptive statistics for PID-5 scales are presented in supplemental Table S1, and inter-correlations among DSM-5 and ICD-11 domains are presented in Table 3.
Inter-correlations among DSM-5 and ICD-11 domain scores.
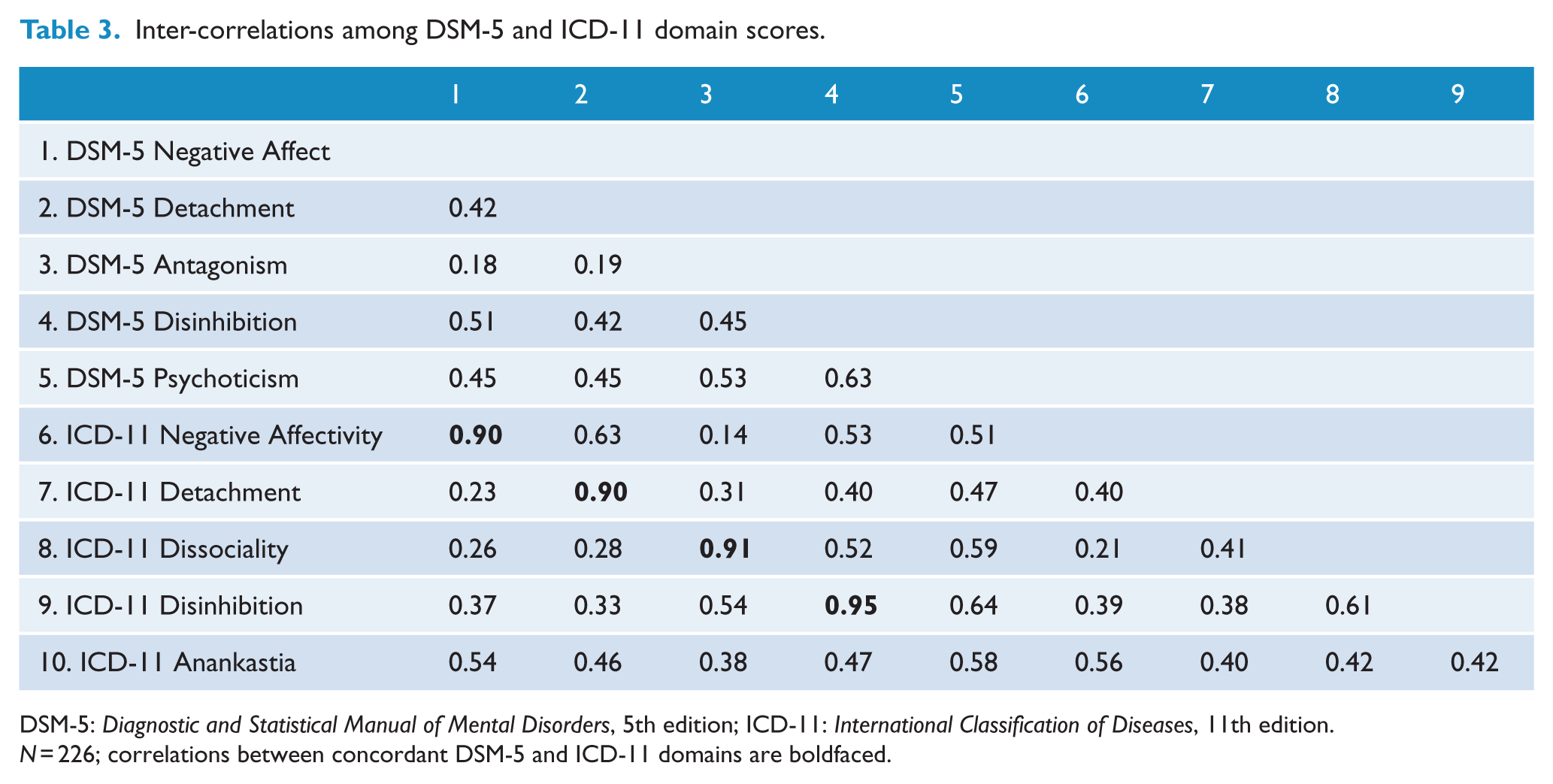
DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th edition; ICD-11: International Classification of Diseases, 11th edition.
N = 226; correlations between concordant DSM-5 and ICD-11 domains are boldfaced.
Results
Bivariate associations
Table 4 presents bivariate correlations between PD trait domains (ICD-11 and DSM-5 Section III) and categorical PDs. 4 Although correlations above 0.23 were statistically significant at the 0.001 level, we focus primarily on coefficients with at least medium effect size (above 0.30) given the number of comparisons. In general, the trait domains show strong convergence with PDs they were hypothesized to indicate (according to boldfaced coefficients). For ICD-11 domains, the median boldfaced correlation (i.e. hypothesized domain) was 0.46, whereas the median nonboldfaced correlation (i.e. nonhypothesized domain) was 0.26. For DSM-5 domains, the median boldfaced correlation (i.e. hypothesized domain) was 0.43, whereas the median nonboldfaced correlation (i.e. nonhypothesized domain) was 0.24. However, some coefficients were lower than expected, such as the correlation between Negative Affectivity and obsessive–compulsive PD (0.23), and some correlations that were not hypothesized to indicate certain PDs were quite high, such as Disinhibition and Paranoid PD (0.48/0.49). Overall, patterns were consistent with the trait disorder ‘cross-walk’ provided by Skodol et al. (2011).
Bivariate associations of ICD-11 and DSM-5 personality trait domains with personality disorder criterion count.
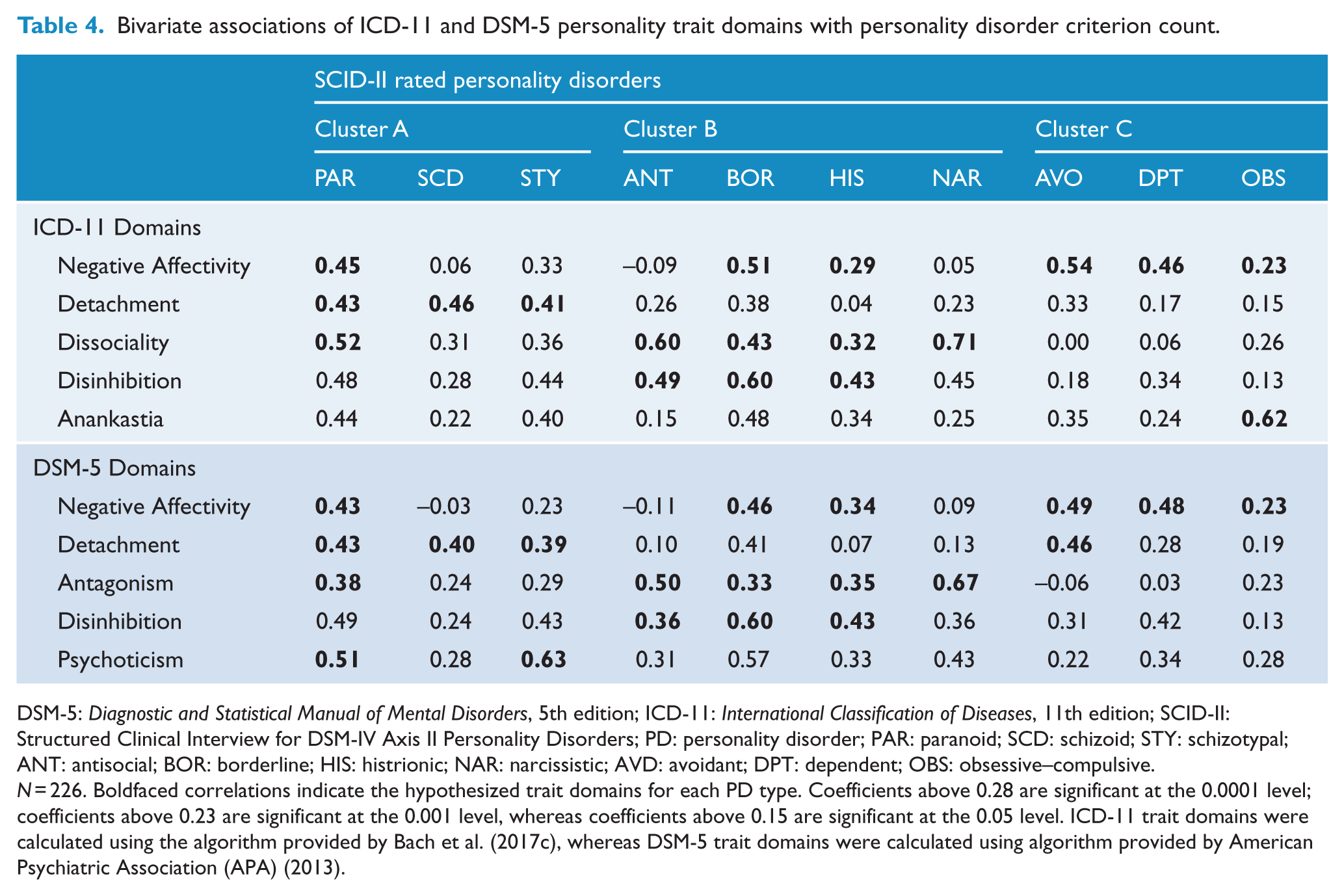
DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th edition; ICD-11: International Classification of Diseases, 11th edition; SCID-II: Structured Clinical Interview for DSM-IV Axis II Personality Disorders; PD: personality disorder; PAR: paranoid; SCD: schizoid; STY: schizotypal; ANT: antisocial; BOR: borderline; HIS: histrionic; NAR: narcissistic; AVD: avoidant; DPT: dependent; OBS: obsessive–compulsive.
N = 226. Boldfaced correlations indicate the hypothesized trait domains for each PD type. Coefficients above 0.28 are significant at the 0.0001 level; coefficients above 0.23 are significant at the 0.001 level, whereas coefficients above 0.15 are significant at the 0.05 level. ICD-11 trait domains were calculated using the algorithm provided by Bach et al. (2017c), whereas DSM-5 trait domains were calculated using algorithm provided by American Psychiatric Association (APA) (2013).
Unique associations
To further explore the adequacy of the trait domains to capture information of the 10 PD types, we regressed each of the 10 PD constructs onto the five trait domains for the ICD-11 and DSM-5 model, separately, by means of both criterion count and binary PD diagnoses. As shown in the two left columns of Table 5, we first investigated the ability of ICD-11 and DSM-5 domains to predict PD dimensions (i.e. SCID-II criterion counts). For this purpose, we employed a multiple negative binomial regression model (count regression) to account for the non-normal count distribution of SCID-II data. The reported regression weights reflect change in dependent variable (PD count score) for a standard deviation increase in independent variables (trait domains). As presented in the two right columns of Table 5, we next investigated the ability of ICD-11 and DSM-5 domains to predict binary PD diagnoses (i.e. SCID-II categories as yielded by established thresholds). For this purpose, we employed a multiple logistic regression model with each PD category as dependent variable and trait domains as independent variables. Odds ratios (ORs) were used to characterize magnitude of individual domain predictors. An OR > 1 indicates that the risk of the outcome falling in the PD category relative to the risk of the outcome not falling in the PD category increases as the trait domain variable increases. Likewise, an OR < 1 indicates that the risk of the outcome falling in the PD category relative to the risk of the outcome not falling in the PD category decreases as the domain variable increases.
Unique associations of ICD-11 and DSM-5 personality trait domains with categorical personality disorders.
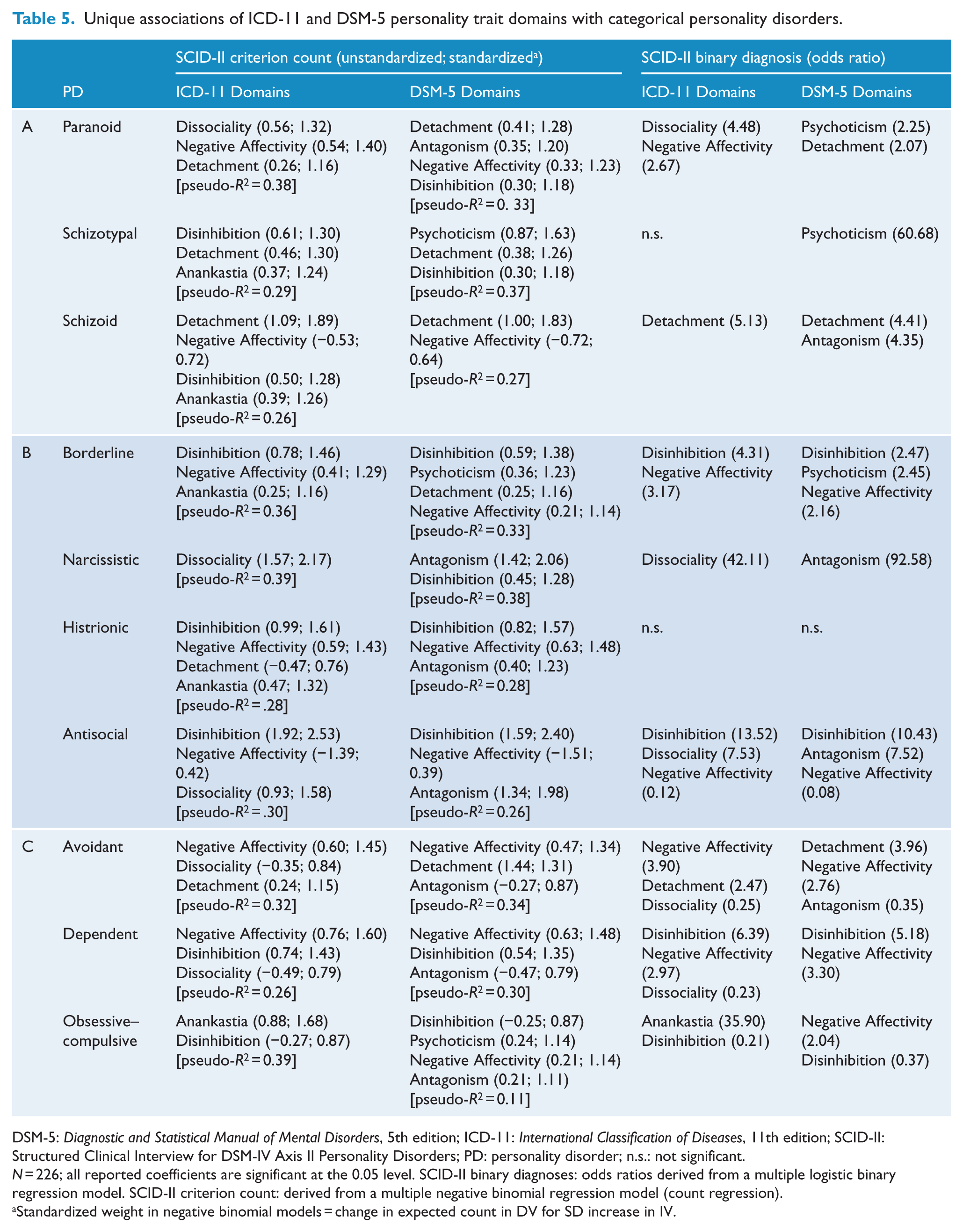
DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th edition; ICD-11: International Classification of Diseases, 11th edition; SCID-II: Structured Clinical Interview for DSM-IV Axis II Personality Disorders; PD: personality disorder; n.s.: not significant.
N = 226; all reported coefficients are significant at the 0.05 level. SCID-II binary diagnoses: odds ratios derived from a multiple logistic binary regression model. SCID-II criterion count: derived from a multiple negative binomial regression model (count regression).
Standardized weight in negative binomial models = change in expected count in DV for SD increase in IV.
As presented in Table 5, each PD (criterion count and binary diagnoses) was generally predicted by hypothesized ICD-11 and DSM-5 trait domains. The ICD-11 domain of Anankastia showed the strongest prediction of obsessive–compulsive PD, whereas the DSM-5 domain of Psychoticism showed the strongest prediction of schizotypal PD. Additionally, when using the binary PD diagnoses as dependent variables, the unique associations became more succinct and exclusively involved the most predominant domains for each PD category, which will be further elucidated in the discussion.
Discussion
This study provides preliminary evidence that the PD domains of the forthcoming ICD-11 model (operationalized with an algorithm for PID-5) capture essential information of the established categorical PDs and furthermore involve substantial overlap with the trait domains in DSM-5 Section III (as expected). Accordingly, the ICD-11 domains and the DSM-5 domains showed continuity with categorical PDs on equal terms. This finding suggests that the new trait domain models capture a substantial amount of reliable information in categorical PDs; thus, little information is lost in the transition. As hypothesized, the ICD-11 domains were superior in capturing obsessive–compulsive PD, while the DSM-5 domains were superior in capturing schizotypal PD, which is not surprising in light of Anankastia and Psychoticism, respectively, being relatively specific to these PDs. Table 6 provides a preliminary category-to-domain cross-walk for ICD-11 and DSM-5 traits, which is derived from findings in this study while also being consistent with previous findings on DSM-5 trait domains (e.g. Anderson et al., 2014; Hopwood et al., 2012; Skodol et al., 2011), and the originally proposed DSM-5 trait-to-disorder associations (Skodol et al., 2011). Thus, these findings may potentially add to narrowing the gap between the current ICD-10/DSM-5 Section II categorical models and the forthcoming ICD-11, while also demonstrating the potential harmonization between the dimensional domains in ICD-11 and DSM-5 Section III.
Preliminary category to domain cross-walk for DSM-5 and ICD-11 personality disorder models.
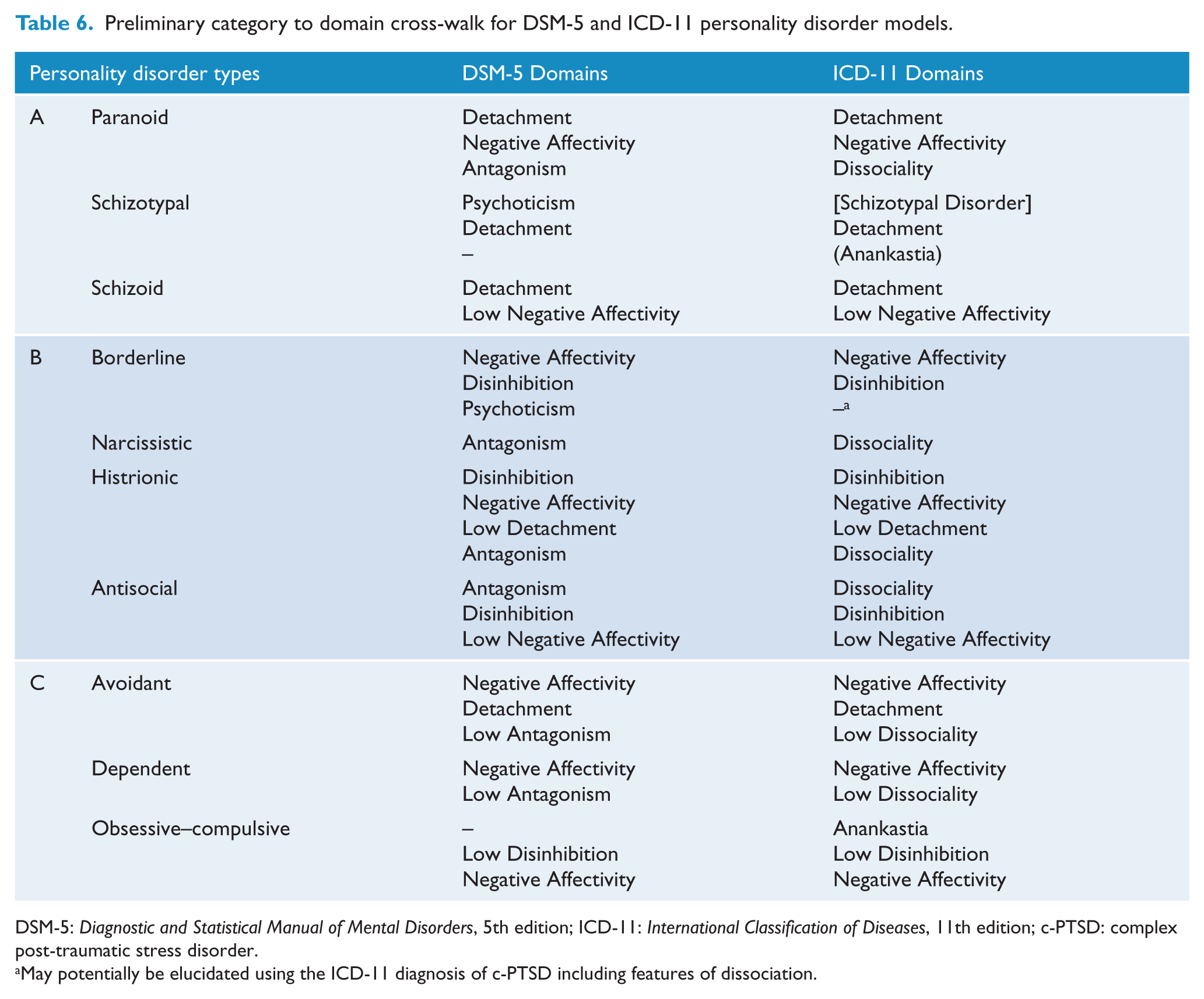
DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th edition; ICD-11: International Classification of Diseases, 11th edition; c-PTSD: complex post-traumatic stress disorder.
May potentially be elucidated using the ICD-11 diagnosis of c-PTSD including features of dissociation.
Apart from the various expected findings, we also observed some unexpected patterns of association: Paranoid, Schizotypal, and Schizoid PDs were predicted by Disinhibition, which is not conceptually coherent but somewhat consistent with previous findings indicating that Distractibility (facet of Disinhibition) is structurally related to the domain of Psychoticism in clinical samples (e.g. Bach et al., 2017b; Bastiaens et al., 2016; Krueger et al., 2012). In addition, the separation of Disinhibition and Psychoticism has been debated, with Eysenck (1990) arguing that psychoticism would be a reflection of an extreme manifestation of Disinhibition. Indeed, research on Psychoticism and Disinhibition evidence moderate to large correlations across studies and measures (e.g. Wright et al., 2012). Likewise, Borderline, Schizotypal and Schizoid PDs were predicted by ICD-11 Anankastia, which is nevertheless partially meaningful in terms of previous findings indicating that perseveration (facet of Anankastia) is structurally related to DSM-5 Psychoticism (Wright et al., 2012). Additionally, a large number of studies indicate substantial associations between Schizotypal PD and obsessive–compulsive PD features (e.g. Chmielewski and Watson, 2008). Moreover, we found that Dependent PD was predicted by Disinhibition, which was unexpected but nevertheless consistent with previous findings showing that irresponsibility (facet of Disinhibition) is associated with Dependent PD (Bach et al., 2017a), most likely related to the diagnostic criterion 2 for DSM-5 Section II Dependent PD: ‘Needs others to assume responsibility for most major areas’ (APA, 2013). Finally, in this study, Borderline PD was not predicted by Dissociality or Antagonism, which we had expected because Hostility (feature of Dissociality) is defined as a Borderline PD trait specifier (APA, 2013). However, Hostility is also a potential facet of Negative Affectivity in both the ICD-11 and DSM-5 models.
As an essential issue of this paper, it seems important to elucidate the differences between the two models in terms of the ICD-11 domain of Anankastia and the DSM-5 domain of Psychoticism. First, some scholars have emphasized that obsessive–compulsivity is an important dimension of maladaptive personality in its own right, which must have its own set of more specific lower order facets (Ayearst et al., 2012). In this study, the ICD-11 domain of Anankastia was superior in predicting obsessive–compulsive PD. However, the DSM-5 domain of low Disinhibition also showed significant prediction of obsessive–compulsive PD and could furthermore be specified using the facets of rigid perfectionism (low Disinhibition) and perseveration (Negative Affectivity).
Second, research has highlighted the importance of DSM-5 Psychoticism in order to characterize Schizotypal PD in terms of eccentricity, derealization and depersonalization (Chmielewski et al., 2014; Crego and Widiger, 2016). However, a more fundamental question is whether Schizotypal PD is itself a personality disorder? To address this question, we need to consider that the DSM and ICD systems have risen from different backgrounds and diagnostic assumptions about symptoms (e.g. psychoticism). More specifically, schizotypal features have never been classified as such in the ICD where it is placed within its schizophrenia spectrum section. Accordingly, none of the five ICD-11 domains concern schizotypal cognitive-perceptual aberrations. One may also argue that DSM-5 Psychoticism as measured with the PID-5 goes beyond schizotypal peculiar and magical thinking to include overt Schneiderian schizophrenic delusions. This may apply to thought withdrawal (item 192): ‘Sometimes I think someone else is removing thoughts from my head’; thought insertion (item 154): ‘Sometimes I feel “controlled” by thoughts that belong to someone else’; and thought-broadcasting (item 150): ‘Sometimes I can influence other people just by sending my thoughts to them’. Such DSM-5 features of Psychoticism are perhaps best understood as schizophrenic psychotic phenomena (Schneider, 1959), rather than reflecting the magical thinking and perceptual confusions that apply to patients who are merely odd, peculiar and/or eccentric in a schizotypic manner (Parnas et al., 2005; Torgersen et al., 2002)? Nevertheless, in the ICD-11 beta draft it says that ‘Schizotypal disorder is characterized by an enduring pattern (i.e. characteristic of a person’s functioning over a period of at least several years) of eccentricities in behavior, appearance and speech, accompanied by cognitive and perceptual distortions, and unusual beliefs [...]’ (WHO, 2017). Accordingly, these ICD-11 characteristics of schizotypal disorder seem rather PD-like in their nature.
Finally, DSM-5 Psychoticism may also characterize important features of DSM-5 Section II Borderline PD in terms of stress-related dissociative symptoms (Bach and Fjeldsted, 2017; Bach and Sellbom, 2016; Evans and Simms, 2017; Sellbom et al., 2014). These findings are consistent with the initial construction of the DSM-5 trait model, where one facet of Psychoticism was first labeled Dissociation-proneness but subsequently relabeled Cognitive & Perceptual Dysregulation (Krueger et al., 2012). However, the ICD-10 operationalization of F60.31 Emotionally unstable, borderline type does not include any psychotic-like or dissociative features (WHO, 1992). However, in a recent proposal, the forthcoming ICD-11 category of ‘complex post-traumatic stress disorder’ (c-PTSD) has been highlighted as better, less stigmatizing and more clinically useful than the traditional Borderline PD diagnosis (Kulkarni, 2017), as it explicitly includes dissociation, severe and pervasive problems in affect regulation, persistent beliefs about oneself as diminished, defeated or worthless, accompanied by deep and pervasive feelings of shame, guilt or failure related to the traumatic event, and persistent difficulties in sustaining relationships and in feeling close to others (WHO, 2017). Consequently, beyond high severity rating and prominent domain features of Negative Affectivity and Disinhibition, Borderline PD may potentially be elucidated using the ICD-11 diagnosis of c-PTSD including features of dissociation.
Taken together, the five trait domains in DSM-5 and ICD-11, respectively, generally show meaningful continuity with established categorical PDs, whereas somewhat unforeseen but reasonable cross-associations also apply to this continuity. For example, Psychoticism applies to both Schizotypal PD (e.g. eccentricity) and Borderline PD (e.g. perceptual dysregulation). Anankastia applies to obsessive–compulsive PD (e.g. rigid perfectionism) but may also apply to obsessions in Schizotypal PD (e.g. perseveration). Disinhibition applies to Antisocial PD (e.g. risk taking) and Borderline PD (e.g. impulsivity) but also Schizotypal PD (e.g. distractibility) and Dependent PD (e.g. irresponsibility). Detachment primarily applies to Schizoid PD (e.g. restricted affectivity) but also Avoidant PD (e.g. withdrawal) and Histrionic PD (e.g. low withdrawal, low intimacy avoidance and low restricted affectivity). Antagonism/Dissociality primarily applies to Antisocial PD (e.g. callousness) and Narcissistic PD (e.g. grandiosity) but also Avoidant PD (e.g. low grandiosity). Finally, Negative Affectivity applies to Borderline PD (e.g. emotional lability) and Avoidant PD (e.g. anxiousness) but also Antisocial PD (e.g. low anxiousness) and Schizoid PD (e.g. low emotional lability). Knowledge of these associations may be useful for clinicians that are familiar with the established categories in order to communicate in terms of the new PD domains. This manifold pattern of associations demonstrates that the relatively homogeneous DSM-5 and ICD-11 trait domains share essential features with the relatively heterogeneous PD categories, which supports the continuity from categories to dimensional domains. This may indeed ease the transition for clinicians when exchanging the polythetic categorical PD types with dimensional trait domains while also highlighting their common ground.
This study is not without limitations. The personality trait portion was limited to self-report measurement, which has been well-validated, but future research should be focused on other ratings as well including informants and clinicians. The overall sample composition may have biased the findings (including very low prevalence of Histrionic and Narcissistic PD), and the sampling from two different settings may somewhat have caused systematic bias; but for power, heterogeneity and range reasons, we found it most reasonable to combine the two samples. Finally, there are also high rates of comorbidity and while this is a natural reflection of these patients, it does introduce some ambiguity into the explicit PD-to-trait links. Consequently, future research should replicate these findings in other settings with more externalizing psychopathology, such as forensic or correctional settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Grants have been received from the Health Scientific Research Fund of Region Zealand.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.