
Abstract
Objective:
We examine the prevalence of quality care (as measured by adherence to recommendations in clinical practice guidelines) for Australian paediatric patients (⩽15 years) with depression and/or anxiety, using data from the CareTrack Kids study; a population-based study of the quality of healthcare practice in inpatient and ambulatory healthcare settings.
Methods:
A multistage stratified sample identified records of 6689 children. Of these, 156 records were identified for depression and 356 for anxiety. These were assessed for adherence to 15 depression and 13 anxiety indicators, respectively, using a review of medical records.
Results:
Adherence to assessment and management guidelines was low for both conditions: assessment bundle (depression = 33%, 95% confidence interval = [20, 48]; anxiety = 54%, 95% confidence interval = [43, 64] and depression management bundle = 35%, 95% confidence interval = [15, 60]). Across both conditions, the highest adherence was recorded for indicators that addressed prescription of medications (e.g. venlafaxine, 100%; benzodiazepines, 100%; selective serotonin reuptake inhibitor, 94% and antidepressants, 91%), while compliance was the lowest for ensuring children with depression had an emergency safety plan (44%), informing parents of the risks and benefits of prescribed anxiety medication (51%) and assessment for other causes (59% for depression; 68% for anxiety).
Conclusion:
These findings suggest that strategies are needed to improve guideline adherence for mental health disorders in children and adolescents, particularly among general practitioners. Learning from these indicators could inform clinical prompts in electronic medical records, as well as links to additional information, to assist in decision-making and streamline work practices.
Introduction
Mental health disorders are the leading cause of global disease burden for children and young people (Gore et al., 2011). Together, depression and anxiety affect around 1 in 5 children and adolescents, with 1 in 10 meeting a clinical mental health disorder meeting international classification standards (Lawrence et al., 2015). These conditions are disabling in terms of academic, social and physical functioning (Jaycox et al., 2009; Lawrence et al., 2015). Their economic impact is immense, both in direct costs to healthcare systems (Medibank Private and Nous Group, 2013) and indirect costs to the community (Lee et al., 2017). Although depression and anxiety are the two most common psychological problems managed in general practice (Britt et al., 2013), these conditions often go unrecognised and untreated (Knapp et al., 2016). Furthermore, depression or anxiety in childhood, if left untreated, is likely to continue into adulthood and over time becomes increasingly difficult to manage (Birmaher et al., 2002). Thus, it is imperative that children and young people with symptoms of depression and anxiety be diagnosed and treated in an appropriate manner (Hoffmann et al., 2012).
Over the last decade or so, clinical practice guidelines (CPGs) for the appropriate management of depression and anxiety in children and adolescents have been developed in several countries (British Columbia Medical Association, 2010; Cheung et al., 2018; Connolly and Bernstein, 2007; National Institute for Health and Care Excellence [NICE], 2005), including Australia (Lyndon et al., 2005). Despite CPG availability, clinical practice is often not aligned with guidelines (Grol, 2001). In previous studies of adults, rates of appropriate care (i.e. care in-line with CPGs) for depression and anxiety vary widely, ranging from 8% to 81% (Fernández et al., 2010; Runciman et al., 2012b). However, despite wide variability in rates of treatment adequacy, primary-care studies generally report that less than 1 in 2 adults receives minimally adequate treatment for depression or anxiety based on CPG recommendations (Roberge et al., 2016). Guideline adherence has been investigated far less in paediatric populations, and the published research has concentrated almost exclusively on treatment indicators, and in particular, antidepressant treatment for children and adolescents with moderate to severe depression (Bhatia et al., 2008; Cheung et al., 2008; de Vries et al., 2016).
Adherence to clinical guidelines is important to optimise the quality of clinical care (Fernández et al., 2010). Indeed, several studies suggest that adherence to depression and anxiety guidelines yield superior treatment outcomes in adult populations (Hepner et al., 2007; Van Dijk et al., 2013, 2015) and is more cost-effective (Pyne et al., 2003). As a result, several initiatives have been undertaken to promote and facilitate the uptake of CPGs (Van Dijk et al., 2013, 2015). For paediatric populations, positive changes in clinical practice have also been inferred following explicit warnings by the US Food and Drug Administration (FDA) and national medicines boards regarding the use of antidepressants in children, which led to reduced prevalence of their prescription (Cheung et al., 2008). Other attempts at improving quality of care for young people with depression have been designed to support client-centred care and collaborative decision-making (Simmons et al., 2017).
Given the serious short-term and long-term consequences of depression and anxiety, monitoring and evaluation of adherence to clinical guidelines is important to track changes and identify where improvements are needed (Runciman et al., 2012a). Currently, there is little available evidence of levels of quality of care for depression and anxiety in paediatric populations; particularly across the entire patient journey and using a range of clinical indicators (e.g. diagnosis, treatment and ongoing management) covering several treatments (e.g. pharmacotherapy and psychotherapy). Such information could provide baseline data for future healthcare system planning. In response to the need to evaluate adherence to clinical guidelines in paediatric populations in Australia, the CareTrack Kids (CTK) study was undertaken (Braithwaite et al., 2018; Hooper et al., 2015). CTK assessed care of Australian children and adults (aged 0–15 years), in 2012 and 2013, to determine the proportion that received care in-line with CPG recommendations for 17 common conditions (Braithwaite et al., 2018). Across the 17 conditions, appropriate care per occasion of care was provided at an average of 59.8% (95% confidence interval [CI] = [57.5, 62.0]) and at 71.5% (95% CI = [56.4, 83.8]) for depression and at 80.8% (95% CI = [75.5, 85.4]) for anxiety. The aim of this paper is to describe and report indicator-level CTK results for depression and anxiety.
Methods
The CTK methods have been described in detail elsewhere (Braithwaite et al., 2018; Hooper et al., 2015; Wiles et al., 2015). We describe some aspects specifically relevant to depression and anxiety, with a focus on indicator development.
Development of indicators
We modified and applied the RAND Corporation/University of California Los Angeles (RAND-UCLA) method to develop indicators (Fitch et al., 2001). For the purposes of this study, a clinical indicator is defined as a measurable component of a standard or guideline, with explicit criteria for inclusion, exclusion, time frame and practice setting (Runciman et al., 2012a; Wiles et al., 2019).
A systematic search for Australian and international CPGs for depression and anxiety care for children and adolescents relevant for the years 2012 and 2013 yielded 14 CPGs (n = 7 for depression, n = 8 for anxiety; includes one for both conditions), from which 235 recommendations (n = 147 for depression and n = 88 for anxiety) were extracted (Wiles et al., 2019). We screened recommendations for eligibility and excluded those that did not meet the following criteria: (1) their strength of wording (‘may’ and ‘could’ statements were excluded), (2) a low likelihood of the information being documented, (3) guiding statements provided without recommended actions; and (4) aspects of care deemed out of the scope of the CTK study such as ‘structure-level’ recommendations; 124 recommendations were excluded, with the remaining 111 recommendations (n = 38 for depression and n = 73 for anxiety) submitted for review. They were then classified according to phases of care (diagnosis, treatment or ongoing management) and assigned the type of quality of care addressed (underuse or overuse).
Proposed indicators were ratified by experts over a two-stage multi-round modified Delphi process, which comprised an email-based three-round internal review and a collaborative, online, wiki-based two-round external review, custom-designed for the study (Wiles et al., 2015, 2019). In total, six experts (comprising two general practitioners and four psychiatrists) were recruited for the internal (n = 4) and external review (n = 2). An expert coordinator was appointed to lead the reviews for each condition. Reviewers completed a Conflict of Interest Declaration (Wiles et al., 2015), and these were managed according to an established protocol (National Health and Medical Research Council [NHMRC], 2012).
In the internal review, experts scored each indicator against three criteria: acceptability, feasibility and impact; recommended indicators for inclusion or exclusion; and provided any additional comments (Wiles et al., 2015, 2019). For the external review, experts registered to the online wiki and self-nominated for CTK conditions based on their clinical experience (Boulkedid et al., 2011). External reviewers applied the same scoring criteria as internal reviewers and, in addition, used a 9-point Likert-type scale to score each indicator as a representative of appropriate care delivered to children during 2012 and 2013 (Fitch et al., 2001; Wiles et al., 2015). The expert coordinator for each condition commented on reviewers’ responses and made final recommendations regarding the inclusion of the indicators. For internal and external reviews, experts completed their assignments independently to minimise group-think bias (Hasson and Keeney, 2011). A total of 15 final indicators (n = 8 for depression and n = 7 for anxiety) were ratified by experts and formatted into 28 medical record audit indicator questions (n = 15 for depression and n = 13 for anxiety). All indicator questions are shown in Tables 2 and 4, with additional details in Supplemental Appendix 1A and 1B.
Sample size, sampling process and data collection
CTK targeted 133 medical records for depression, 267 medical records for anxiety and 6000 medical records for 15 other conditions. If any of the 6400 medical records we targeted and sampled contained an occasion of care for either depression or anxiety, a separate assessment was made for each visit. Detail on the general sampling methods is provided in the paper presenting CTK top-level results (Braithwaite et al., 2018); additional details specific to depression and anxiety can be found in Supplemental Appendix 2. Briefly, we sampled four healthcare settings: hospital inpatients and Emergency Department (ED) presentations, and consultations at general practices (GPs) and paediatricians’ offices in randomly selected Health Districts in Queensland (Hospital Health Services), New South Wales (NSW; Local Health Districts) and South Australia (Local Health Networks), for children aged ⩽15 years receiving care in 2012 and 2013. For the main CTK study, 34 of 37 (92%) eligible hospitals that were approached agreed to participate. For GPs, the estimated recruitment rate was 24%, and for paediatricians 25% (see Supplemental Appendix 2 for additional details). Figure 1 illustrates number of visits by state and care setting.
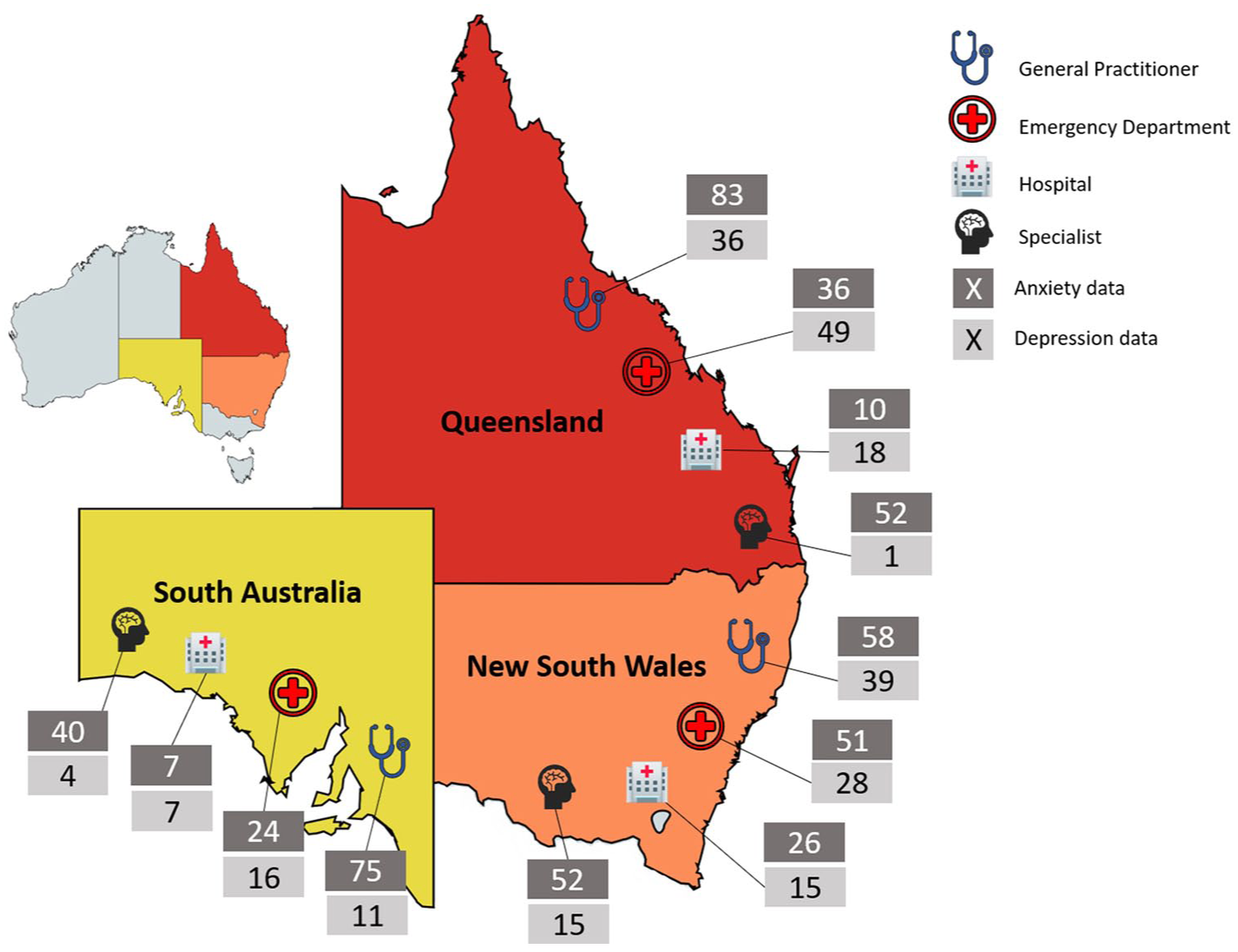
Anxiety and depression assessments by state and healthcare provider type.
Recruited hospitals identified visits for anxiety or depression using the International Classification of Diseases (ICD) or the Systematised Nomenclature of Medicine (SNOMED) codes, while GPs identified consultations using practice software, and these were selected randomly by central project staff until a site-specific quota was achieved; for paediatricians, surveyors were instructed to take random samples on-site, but a single standardised method could not be applied or randomness assured (see Supplemental Appendix 2 for additional details). Of the four healthcare settings sampled in this study, the overwhelming majority of episodes of care are estimated to be in GPs’ (depression: 86%; anxiety: 58%) or paediatrician’s offices (depression: 12%; anxiety: 41%; see Supplemental Appendix 2). ED and inpatient settings only contribute 1–3% of all episodes of care and were oversampled (see below for further detail); these settings likely contain the more severe end of the patient spectrum.
Data were collected via medical record review. Nine experienced paediatric nurses (‘surveyors’), after 5 days of training to assess eligibility for indicator assessment and compliance with CPGs, visited sites during March–August 2016 to undertake the reviews. In their review, a diagnosis of anxiety or depression needed to be confirmed by one of the following methods: identification of a relevant ICD-10 AM code (or an equivalent Systematised Nomenclature of Medicine – Clinical Terms, SNOMED-CT, in NSW only) in the hospital record; or clear identification of the diagnosis in the GP or paediatrician record (see Supplemental Appendix 2 for ICD-10 and SNOMED-CT codes). Surveyors were informed that if they were unsure about the diagnosis, not to make assumptions, to minimise the likelihood of false-positive records.
Analysis
At indicator level, adherence was estimated as the number of indicators scored as ‘Yes’ as a percentage of all indicators answered either ‘Yes’ or ‘No’. Results for some clinically related indicators were aggregated as bundles of care. For example, indicators DEPR01–DEPR05 all relate to children who presented with suspected depression; all five of these indicators would have to be scored ‘Yes’ for the bundle to be scored as being compliant with the CPG. When assessing bundles, a visit was only included if there were ‘Yes’ or ‘No’ responses for all component indicators.
Sampling weights were constructed as specified in Supplemental eAppendix 4 of the paper reporting top-level CTK results, to adjust for oversampling of states and healthcare settings and for sampling within health districts (Braithwaite et al., 2018). The weighted data were analysed in SAS, version 9.4 (SAS Institute Inc., North Carolina, USA), using the SURVEYFREQ procedure. Variance was estimated using Taylor series linearisation, and the primary sampling unit (Health District) was specified as the clustering unit. Stratification and, where appropriate, domain analysis were used (see Supplemental Appendix 2). Exact 95% CIs were generated using the modified Clopper–Pearson method, except when the point estimate was 0% or 100%, where the unmodified Clopper–Pearson method was used (Korn and Graubard, 1998). In both indicator and bundle reports, results were suppressed if there were <25 assessed visits.
Ethical considerations
We received primary ethics approval from relevant bodies including hospital networks and the Royal Australian College of General Practitioners (HREC/14/SCHN/113; HREC/14/QRCH/91; HREC/14/WCHN/68; NREEC 14-008) and site-specific approvals from 34 sites. Australian Human Research Ethics Committees can waive requirements for patient consent for external access to medical records if the study entails minimal risk to providers and patients (Hooper et al., 2015); all relevant bodies provided this approval. Ethics approvals included reporting by healthcare setting type for condition-level papers. Participants were protected from litigation by gaining statutory immunity for CTK as a quality-assurance activity, from the Federal Minister for Health under Part VC of the Health Insurance Act 1973 (Commonwealth of Australia).
Results
Characteristics of surveyed medical records
Details of the 156 children with one or more eligible assessments of CPG compliance for depression and 356 children with eligible assessments for anxiety are provided in Table 1.
Characteristics of the eligible children, 2012–2013.
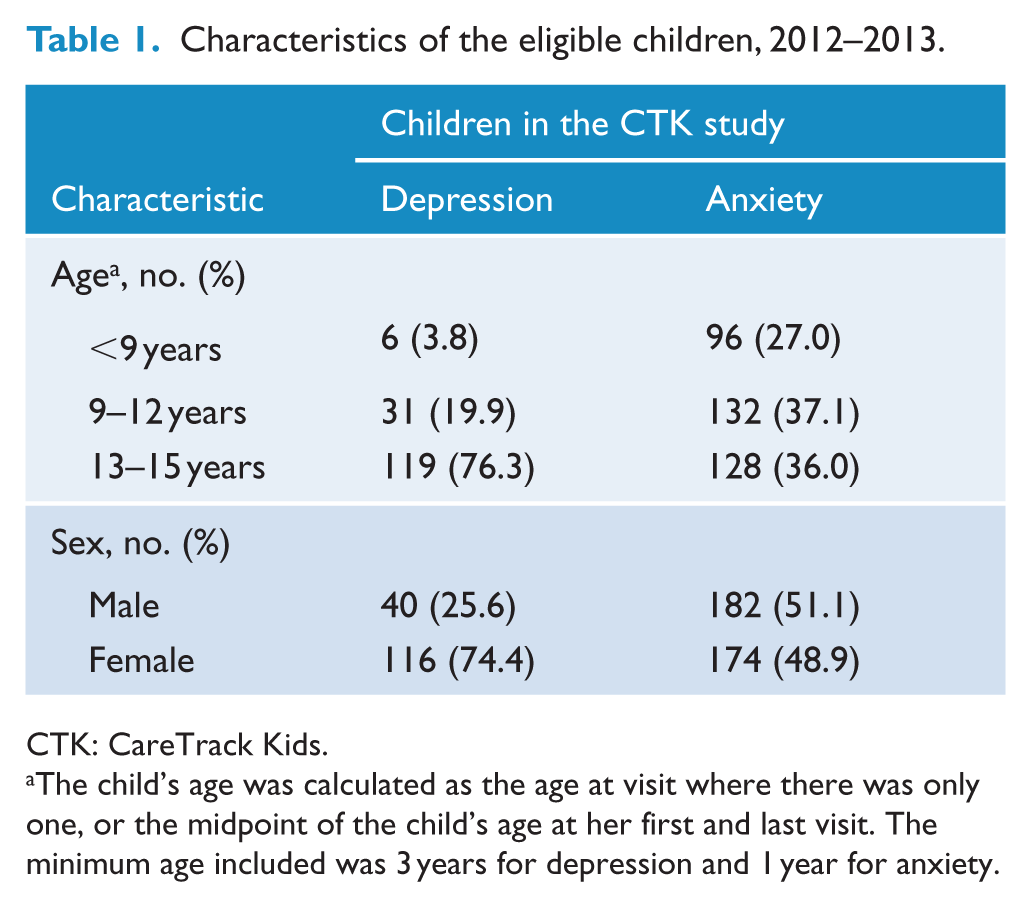
CTK: CareTrack Kids.
The child’s age was calculated as the age at visit where there was only one, or the midpoint of the child’s age at her first and last visit. The minimum age included was 3 years for depression and 1 year for anxiety.
For depression, three-quarters of the children were aged 13–15 years, and about three-quarters were female children. This is in accordance with the findings of the second Australian Child and Adolescent Survey of Mental Health and Wellbeing (Lawrence et al., 2015), which showed that prevalence rates for depression increase during the early adolescent years, and female children are much more at risk of depression than male children. Each child had between one and six eligible visits during 2012–2013 (median = 1). Of 4050 possible indicator assessments, 137 (3.4%) were automatically filtered out by healthcare setting restrictions, and the surveyors designated 1632 (40.3%) as not applicable or otherwise ineligible. The surveyors conducted 2281 indicator assessments grouped into 239 visits, at a median of 11 indicators per visit. Visits for depression were assessed in 30 GPs’ and 10 paediatricians’ offices, 31 hospital EDs and by 19 hospital inpatient service providers. The 239 visits for depression are drawn from an estimated pool of 141,000 episodes of care of depression for children under 15 years of age in Australia in 2012–2013 (see Supplemental Appendix 2; Braithwaite et al., 2018).
For anxiety, about a third of the children in the CTK sample were aged <9 years, 9–12 years or 13–15 years, with almost equal numbers of male and female children. Each child had between one and eight visits (median = 1). Of 7085 possible indicator assessments, 1304 (18.4%) were automatically filtered out by healthcare setting restriction, and the surveyors designated 2622 (37.0%) as not applicable or otherwise ineligible. The surveyors conducted 3159 indicator assessments grouped into 514 visits, at a median of 7 indicators per visit. Visits for anxiety were assessed in 46 GPs’ and 19 paediatricians’ practices, 32 hospital EDs and by 19 hospital inpatient service providers. The 514 visits for anxiety are drawn from an estimated pool of 323,000 episodes of care of anxiety for children under 15 years of age in Australia in 2012–2013 (see Supplemental Appendix 2; Braithwaite et al., 2018).
Adherence to quality care for depression
For each depression indicator, the assessed adherence is shown in Table 2. Adherence is reported for all 15 indicators and separately by healthcare setting. Overall adherence ranged from 43.8% for ‘Children and adolescents with depression had an emergency safety plan’ (DEPR09) to 91.3% for ‘Children and adolescents with mild depression, defined in accordance with the ICD-10 as having four criteria symptoms (NICE, 2013), were not prescribed antidepressant medication as a first-line intervention’ (DEPR10). The interquartile range for adherence in the 15 indicators was 67.3–79.1%. In general, the lowest levels of adherence were reported for GPs, and the highest levels were reported in hospital inpatient and ED settings. There were insufficient data to present levels of compliance separately for paediatricians.
Adherence to quality care for depression, by clinical indicator, 2012–2013.
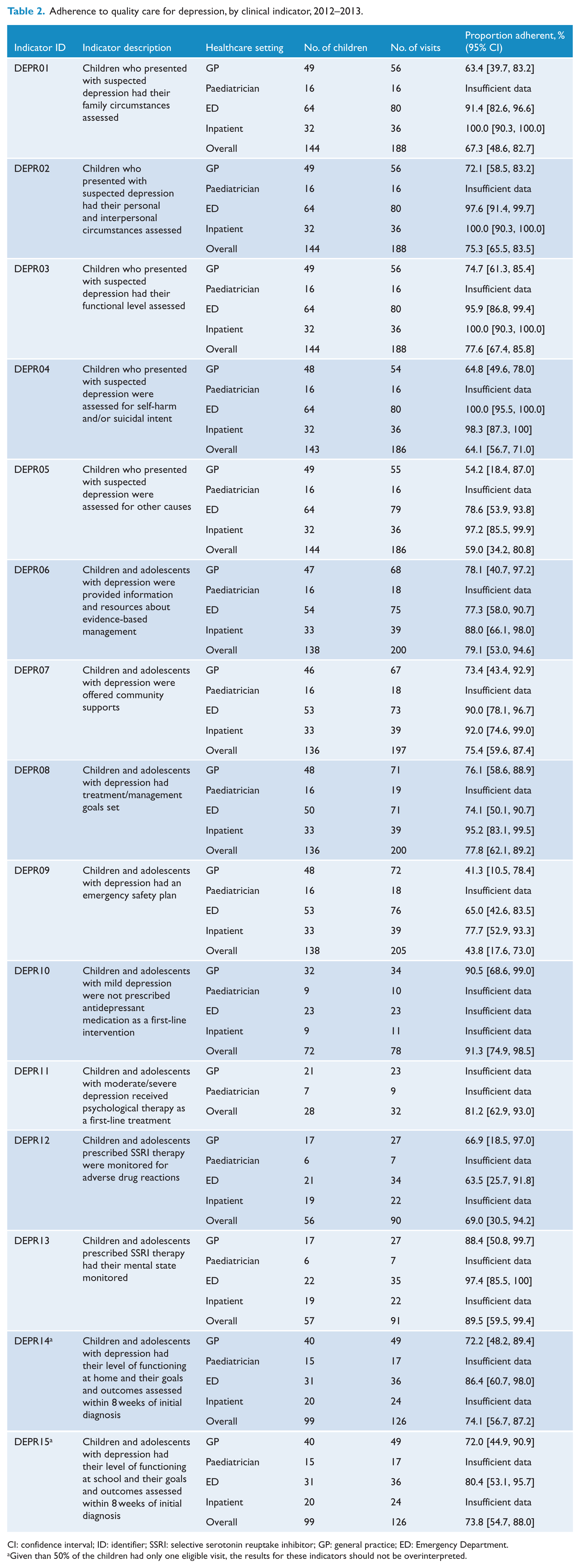
CI: confidence interval; ID: identifier; SSRI: selective serotonin reuptake inhibitor; GP: general practice; ED: Emergency Department.
Given than 50% of the children had only one eligible visit, the results for these indicators should not be overinterpreted.
The assessed adherence of two bundles is shown in Table 3, both assessed separately by healthcare setting. Bundle A consists of five indicators which relate to appropriate assessment of a child presenting with suspected depression and found 33.0% compliance (95% CI = [20.2, 48.0]); the component indicator with the lowest compliance was documentation of other possible causes (59.0%; 95% CI = [34.2, 80.8]; DEPR05). Bundle B appraised four elements relating to facilitation of information, treatment support and management and found 35.3% compliance (95% CI = [15.1, 60.3]); the component indicator with the lowest compliance was documentation of an emergency management plan (43.8%; 95% CI = [17.6, 73.0]; DEPR09). For both Bundle A and Bundle B, compliance for GPs was lowest at 30.3% (95% CI = [11.7, 55.3]) and 31.8% (95% CI = [7.7, 66.5]), respectively.
Adherence to quality care for depression, by bundle of care, 2012–2013.
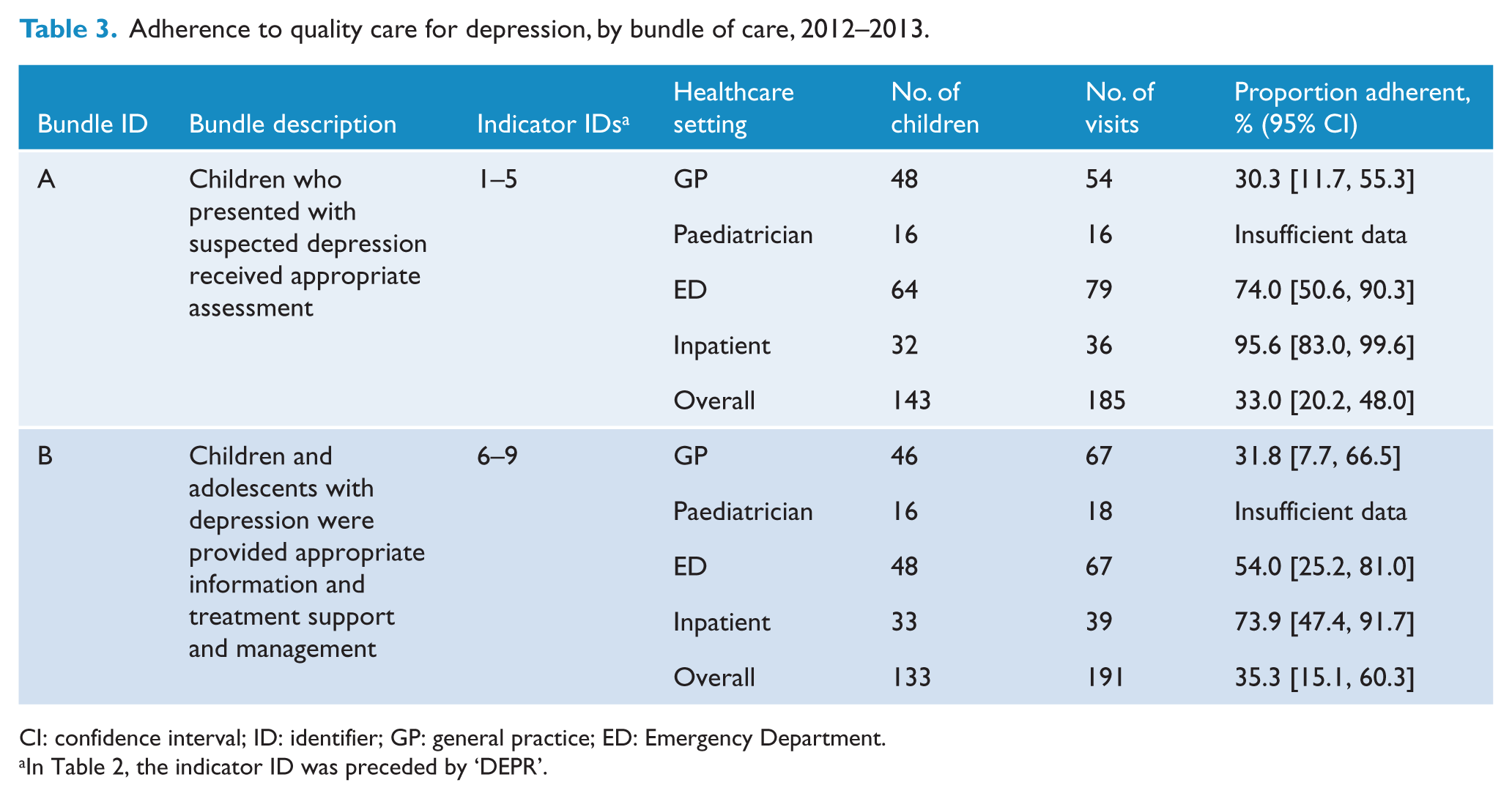
CI: confidence interval; ID: identifier; GP: general practice; ED: Emergency Department.
In Table 2, the indicator ID was preceded by ‘DEPR’.
Adherence to quality care for anxiety
The assessed adherence for each anxiety indicator by healthcare setting is shown in Table 4. Overall adherence is not reported for 1 of the 13 indicators because it had fewer than 25 surveys. For the 12 indicators where adherence was reported, the overall compliance ranged from 51.3% for informing parents of the risks and benefits of prescribed medication (ANXI10) to 100% for appropriate non-prescription of medications, such as venlafaxine and benzodiazepine (ANXI13). The interquartile range for adherence in the 12 indicators reported was 72.8–92.6%. In general, the lowest levels of adherence for anxiety indicators were reported for GPs and EDs, and the highest levels were reported for paediatricians and hospital inpatients.
Adherence to quality care for anxiety, by clinical indicator, 2012–2013.
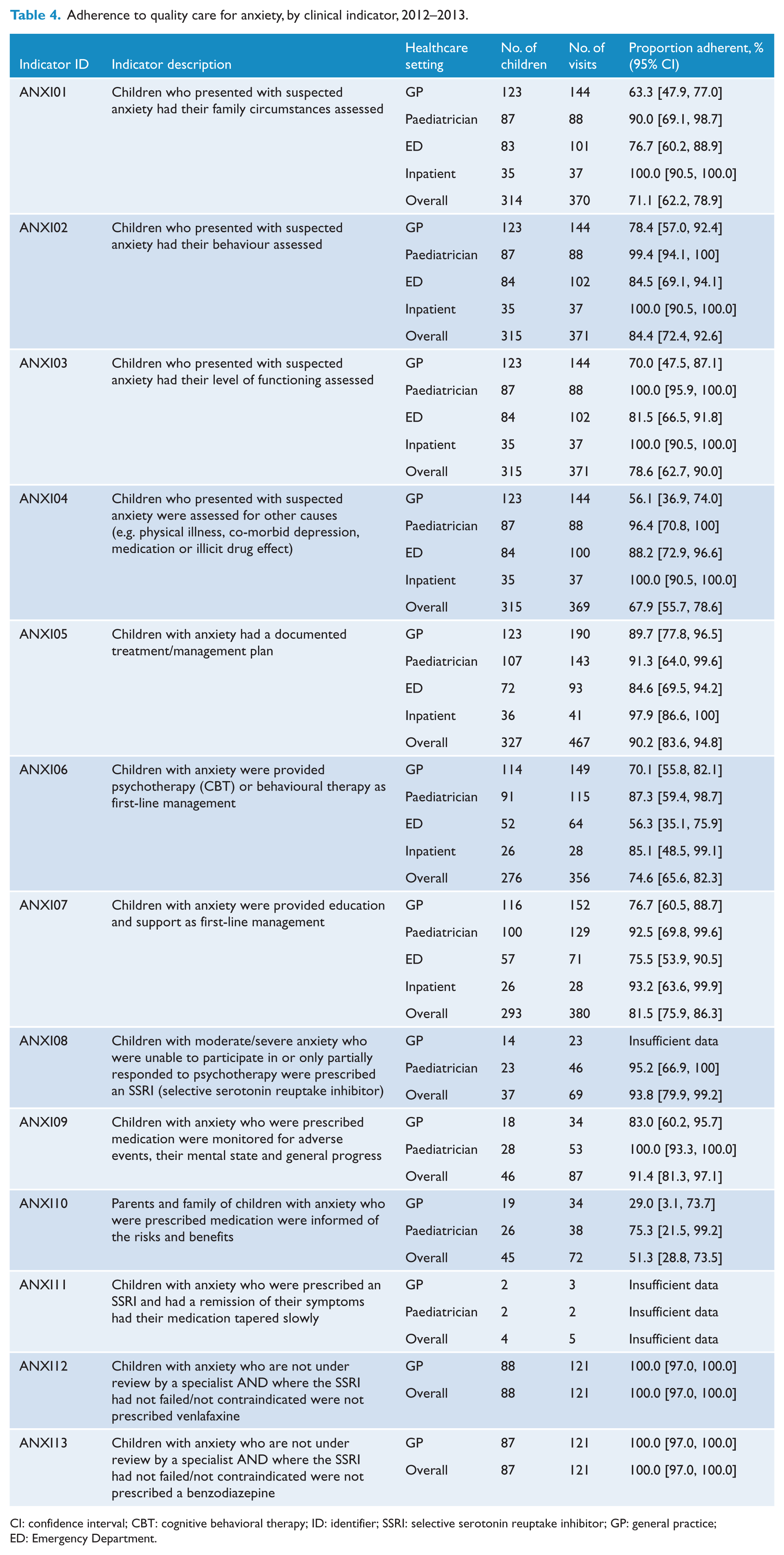
CI: confidence interval; CBT: cognitive behavioral therapy; ID: identifier; SSRI: selective serotonin reuptake inhibitor; GP: general practice; ED: Emergency Department.
For the bundle of care for anxiety, the assessed adherence is shown in Table 5, by healthcare setting. The bundle consisted of four indicators which relate to appropriate assessment of a child presenting with suspected anxiety, across all four healthcare settings, and estimated 53.7% adherence (95% CI = [43.2, 64.0]). The component indicator with the lowest adherence was documentation of the assessment of other possible causes (67.9%; 95% CI = [55.7, 78.6]; ANXI04), with GPs having the lowest bundle estimated adherence at 39.9% (95% CI = [20.6, 61.9]).
Adherence to quality care for anxiety, by bundle of care, 2012–2013.
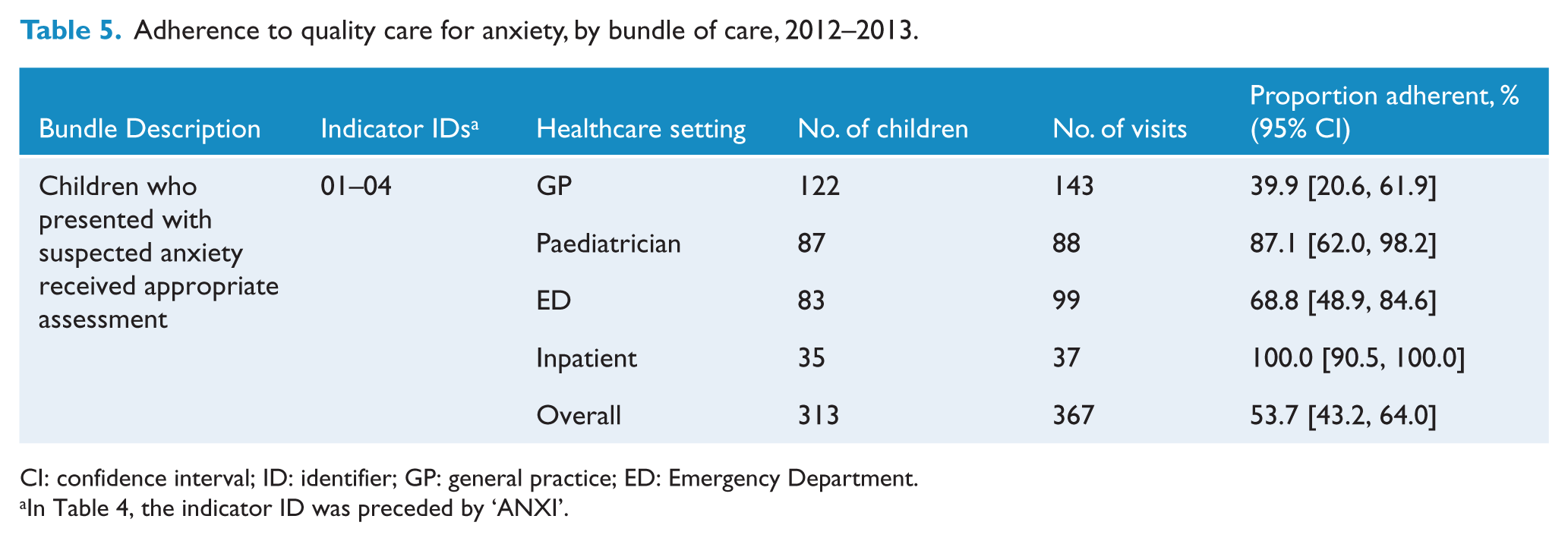
CI: confidence interval; ID: identifier; GP: general practice; ED: Emergency Department.
In Table 4, the indicator ID was preceded by ‘ANXI’.
Discussion
In our study, Australian children with eligible assessments for depression or anxiety received appropriate care at an average of 72% and 81% of the time, respectively. At present, few comparable studies exist that consider a range of clinical indicators in paediatric populations, but results calculated as averages for depression and anxiety in previous studies with adults are reported in Supplemental Appendix 3 for comparison. The results from our study are higher than self-report interviews of appropriate care for adults in the United States (Wang et al., 2002), Europe (Fernandez et al., 2007) and Australia (Andrews et al., 2000), as well as studies of medical records in the Netherlands (Prins et al., 2010) and Australia (Runciman et al., 2012b). A more comparable study (in terms of sample and methods) of US adolescents with depression (Kramer et al., 2008) reported that based on examination of medical records in seven clinics across two states, adolescents received care consistent with consensus guidelines at an average of 68% of the time, a finding that is more consistent with our results for depression (72%). However, the CPGs used in their study were narrowly focused on treatment, applicable to specialist mental healthcare rather than primary healthcare professionals, and the research was conducted almost a decade ago. Therefore, the differences between our results and those from previous studies are, at least in part, likely to reflect differences in the age of participants of interest, as well as the indicators chosen, system performance or performance improvement over time.
In the broader CTK study of 17 common paediatric conditions (Braithwaite et al., 2018), as in other system-level studies (Mangione-Smith et al., 2007), variation in adherence between conditions was considerable. In CTK, higher adherence was found for mental health conditions (>70%), in comparison to other conditions, such as tonsillitis (44%) and upper respiratory tract infection (URTI; 53%). The comparatively higher results for mental health conditions, including depression and anxiety, may in part reflect Australian initiatives over the past two decades, seeking to address mental health services at a national level, such as the National Mental Health Strategy commencing in 1992, five 5-year mental health plans covering the period from 1993 to 2014, a National Action Plan of Mental Health under the Council of Australian Governments (COAG) between 2006 and 2012, the Better Access initiative introduced in 2006 and annual National Report Cards on Mental Health and Suicide Prevention commencing in 2012. Such initiatives may have improved awareness among healthcare professionals regarding appropriate diagnosis and treatment of these conditions (Pirkis et al., 2011).
Approximately one-third of children’s medical records related to depression (33.0%) and one-half for anxiety (53.7%) showed full documented adherence for all elements of assessment. At indicator level across both conditions, the highest adherence was recorded for indicators that addressed inappropriate prescription of medications, such as venlafaxine (100%; ANXI12), benzodiazepines (100%; ANXI13), a selective serotonin reuptake inhibitor (SSRI; 94%; ANXI08) and antidepressants as a first-line intervention (91%; DEPR10). This may also be in accordance with international efforts to improve appropriate prescription of psychotropic medications to young people such as through regulatory warnings for prescribing antidepressants to children and adolescents (Cheung et al., 2008).
For depression, adherence was lowest for ensuring children, and adolescents with depression had an emergency safety plan (DEPR09, 44%). An emergency safety plan is important in ensuring that children and their families have a crisis plan and resources they can access when needed.
For anxiety, documented adherence was the lowest for informing parents of the risks and benefits of prescribed medication (ANXI10, 51%). Although SSRIs are generally well tolerated by children, side effects including headaches and gastrointestinal problems are documented (Birmaher et al., 2002), and thus, this information forms an important part of safe prescribing. For both anxiety and depression, assessment of other causes (ANXI04, 68%; DEPR05, 59%) was also low. The importance of assessing psychosocial risk factors, such as family discord, bullying or abuse, is highlighted in depression and anxiety guidelines (NICE, 2013, 2014), as well as whether they meet the criteria for a depressive or anxiety disorder.
Overall, across both depression and anxiety, lower levels of compliance were reported for GPs than other healthcare settings, a finding that is consistent with previous research (Wang et al., 2002; Young et al., 2001). In Australia, GPs are typically the first point of contact for people seeking help for mental health problems and are the ‘gatekeepers’ to other service providers. Possible reasons for lower levels of compliance for GPs may, therefore, reflect the competing demands experienced by GPs for their attention and resources and a lack of training or knowledge concerning optimal treatments (Wang et al., 2002). However, it is important to recognise that overall, the results of this study were very positive in comparison to other conditions from our CTK study, as well as previous research on adherence to CPGs in paediatric mental health.
Strengths and limitations
The key strength of the broader CTK study is that it was designed to be representative of the Australian population rather than a convenience or purposive sample, with cohorts drawn from three states, representing 60% of the Australian population. An unavoidable consequence of this strategy is that the number of eligible children and surveys can be low for some indicators. Across both depressive and anxiety disorders, this was the case for only one indicator (namely ANXI11; see Table 4). While we had 92% recruitment of selected hospitals, we estimate about 25% recruitment of GPs and paediatricians, creating a possible self-selection bias; if recruited GPs and paediatricians had higher than average adherence to guidelines, our study will have over-estimated adherence. Furthermore, given the scope of the CTK study and resourcing limitations, we developed indicators that were applicable to generalised anxiety disorders (to optimise the practical feasibility of data collection for the condition anxiety). Therefore, our findings may not capture nuances of the care recommended and/or provided for any of the other specific anxiety types (e.g. social phobia, separation anxiety disorder and obsessive–compulsive disorder). For a number of indicators, there were insufficient data for one or more healthcare setting, thus limiting our ability to report differences by healthcare setting across all indicators. In addition, while medical records are often deficient in relevant information required to be confident about the diagnostic status of a child or adolescent, surveyors were instructed that if they were unsure about the diagnosis, not to make assumptions, to minimise the likelihood of false-positive records. Furthermore, medical records are often brief, using abbreviations and technical jargon, thus presenting challenges to surveyors interpreting whether indicators had been completed. This was particularly the case for indicators DEPR14 and DEPR15, where many of the children had only one eligible visit, making it difficult to assess whether the goals and outcomes had been assessed within 8 weeks of diagnosis. In this case, surveyors used documentation on file to make a judgement in relation to these two indicators (e.g. letters from psychologists/psychiatrists), and thus, the results for these indicators should not be overinterpreted. However, surveyors were experienced paediatric nurses who underwent 5 days of training and competency assessment on reviewing medical records and were provided with an in-depth surveyor manual and ongoing support.
This study specifically looked at medically diagnosed depression and anxiety; of all episodes of care for children aged ⩽15 years in the targeted four settings, 1.1% were estimated to be for anxiety and 0.5% for depression (see Supplemental Appendix 2). A population-based survey of anxiety and depression found prevalence of any anxiety disorder to be 6.9% at ages 4–11 years and 7.0% at 12–17 years, and prevalence of depression to be 1.1% at ages 4–11 years and 5.0% at ages 12–17 years (Lawrence et al., 2015). Even after dilution of these estimates for assumed low rates of anxiety and depression for children aged <4 years of age, it is likely that a substantial proportion of prevalent anxiety and disorders do not present for care. Indeed, research shows that most children and adolescents do not access mental health treatment; just over a third (35.0%) of 4–17 year olds with a mental health disorder had seen a GP, and less than a quarter had seen a psychologist (23.9%) or paediatrician (21.0%) in a 12-month period. As such, our study does not attempt to make any inference about population-based care of children with depression or anxiety that do not reach medical attention in the settings studied.
Another limitation of the CTK study has been its reliance on process indicators to audit care as documented within the medical record. Previous research has suggested that medical records may underestimate the quality of care provided by healthcare services, with doctors being more likely to document medication names and less likely to document background history, medication allergies and information provided to patients despite such procedures exist (Owen et al., 2015; Soto et al., 2002). Correlation with or predictive value of compliance with our indicators on clinical and patient-reported outcomes cannot be determined. Future research should employ a variety of population-level and individual patient outcomes and explore the appropriateness of care provided to children with anxiety and depression by relevant allied health professionals (e.g. psychologists). Integrated e-health medical records, with clinical standards embedded and accessible across healthcare facilities and provider types, would enhance the provision of guideline-compliant care, the consistency and completeness of documentation and facilitate large-scale surveillance (audits) of current practice as well as its responsiveness to national initiatives to improve healthcare (Runciman et al., 2012a).
Conclusion
To our knowledge, this is the largest cross-sectional survey of paediatric medical care for anxiety and depression in Australia and internationally. While our methodology did not allow for the tracking of longitudinal trends, it does provide valuable baseline data on the appropriateness of care for children with medically diagnosed depression and anxiety, which is necessary for benchmarking purposes and the targeting and evaluation of national initiatives for specific gaps identified in this care. While our findings may offer a measure of reassurance to clinicians and patients alike, there are a number of areas for improvement. Clinical gains can be made in documenting a thorough assessment, providing information to patients and ensuring children and adolescents with depression have an emergency safety plan. These items could form the content of prompts in electronic medical records, as well as links to additional information to assist in the decision-making process and streamline work practices.
Supplemental Material
ANP_866512_supplementary_material – Supplemental material for Assessing the quality of care for paediatric depression and anxiety in Australia: A population-based sample survey
Supplemental material, ANP_866512_supplementary_material for Assessing the quality of care for paediatric depression and anxiety in Australia: A population-based sample survey by Louise A Ellis, Louise K Wiles, Ruth Selig, Kate Churruca, Raghu Lingam, Janet C Long, Charlotte J Molloy, Gaston Arnolda, Hsuen P Ting, Peter Hibbert, S Bruce Dowton and Jeffrey Braithwaite in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by an Australian National Health and Medical Research Council Partnership Grant (grant no.: APP1065898), with contributions by the National Health and Medical Research Council, Bupa Health Foundation, Sydney Children’s Hospital Network, New South Wales Kids and Families, Children’s Health Queensland and the South Australian Department of Health (SA Health).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.