
Abstract
Objective:
Shark bites are rare, with intense media exposure. There are no known studies of the psychological impacts of this specific type of traumatic event. This is the first study that describes those directly and indirectly affected, and evaluates the prevalence of post-traumatic stress disorder (PTSD) and related risk factors.
Methods:
In total, 124 members of an Australian shark-bite peer-support group were invited to complete an online survey assessing demographic, event, media and psychological factors. Response rate was 48% (n = 60, 63% male, 44 ± 14 years). Retrospective and current measures of PTSD (PTSD Checklist for DSM-5 [PCL-5]) and suicidality (Suicidal Ideation Attributes Scale [SIDAS-5]) were used.
Results:
Post-event PTSD was prevalent in this sample (n = 16/59, 27.1%, 95% confidence interval [CI] = [15.4, 38.8]), but less so currently (n = 2/55, 3.6%, 95% CI = [0.0, 8.7]). In addition, nine (n = 9/59, 15.3%, 95% CI = [5.8, 24.7]) had subthreshold, but highly symptomatic, syndromes post event. There was no association of PTSD with direct/indirect bite involvement, gender, or prior trauma. Two respondents were at risk of suicidal behaviour. PTSD was commonly reported by those without a partner (odds ratio [OR] = 5.91, 95% CI = [1.52, 22.99], p = 0.01) or with two friends or fewer to rely on (OR = 5.83, 95% CI = [1.62, 21.01], p = 0.01). PTSD was more likely in those with a negative media experience (n = 34/52, 65.4%, OR = 11.90, 95% CI = [1.42, 100.04], p = 0.02) and 61.5% (n = 32/52) of respondents reported media coverage lasting months or years. In multivariate modelling, negative media impact, relationship status and friendships were independently associated with PTSD and explained much of the variance in PTSD (F4,41 = 10.94, p < 0.0001, r2 = 0.52).
Conclusion:
Nearly one-third of members of an Australian shark-bite peer-support group report post-event PTSD, and one-quarter of these were not present at the time of the event. Findings support interventions targeting negative media impact, similar to media reporting guidelines for suicide, and enhancing social support.
Introduction
Shark bites, known colloquially as ‘attacks’, are low-probability high-consequence traumatic events (Crossley et al., 2014). These events are statistically rare with 766 unprovoked events internationally between 2007 and 2016, 61 of which were fatal (Florida Museum of Natural History, 2018). Events are ‘provoked’ if the shark is attracted or human contact is initiated by feeding or fishing, and statistics of unprovoked events are more commonly reported. In Australia, there were 569 unprovoked events recorded in the last 100 years, including 134 fatalities, 47 in the last 50 years, an average of less than one per year (Taronga Conservation Society Australia, 2018) Although rare, survivors, witnesses, first responders and close family/friends are often gravely affected.
There is some evidence to indicate that while absolute and proportional rates of fatality may be decreasing in Australia and internationally, human–shark interaction is growing (West, 2011). This may be, in part, due to increased competition for the ocean for leisure or livelihood and often in economically vulnerable regional areas (Gibbs and Warren, 2015). It may be partly due to changes in measurement methods and instruments. It may also be related to sensitive, political negotiation between ocean-users and marine conservation.
There is high risk of morbidity and mortality with shark-bite events (Rtshiladze et al., 2011). A shark is an ancient, top-order predator that still represents a threat to human life, among globally dwindling mega-fauna. A shark is also native to an environment non-native to humans, contributing their role in myth as monsters. These factors, among others, may impact psychological resilience.
However, there is an added media dimension to this type of trauma, courtesy of a generational Jaws® effect and contemporary cultural artefacts like Discovery Channel® Shark Week (Myrick and Evans, 2014; Neff, 2014). Coverage of a 2017 fatality in Western Australia included headlines, ‘Giant shark stalks beach where girl, 17, killed’, and ‘2,250 great whites menace surfers’ (Lagan, 2017; Pawle, 2017). There is precedent for media impact on mental health in suicide literature, which has led to the development of national Australian media guidelines for Reporting Suicide and Mental Illness (Machlin et al., 2012; Pirkis et al., 2006), and legislation in some countries, such as New Zealand (New Zealand Ministry of Health, 2011).
Nonetheless, this trauma type also involves personal, assaultive violence that may be a risk factor. Literature suggests that gender, trauma type (one-off or multiple/complex), and peri-traumatic dissociation may be more significant than injury severity for PTSD (Breslau, 2009; Sijbrandij et al., 2013). Disfigurement and identity may also be factors, as found in burns trauma (McLean et al., 2015). Moreover, life stressors and poor social supports are risk factors for PTSD relapse (Cloitre et al., 2011).
There have been no previous systematic studies of the psychological impact of shark-bite events. Current literature focuses on emergency medicine, forensic case studies, ocean-user safety, marine management, conservation and public perception (Gouk et al., 2015; Neff and Yang, 2013; Woolgar et al., 2001). Broader human–wildlife conflict literature addresses animal–human interactions but focuses on medico-legal or zoological outcomes, and/or vulnerable targets, such as children (Datko et al., 2015; Gustafsson and Eriksson, 2015; Hejna et al., 2012; Sinton and Byard, 2016). One psychiatric study evaluated the cultural stigma of tiger-attack widows in India, and another ‘suicide by lion’ (Bock et al., 2000; Chowdhury et al., 2016). One author proposed an ‘eco-psychiatric’ specialisation and diagnostic classification of post-traumatic eco-stress disorder (PTESD; Chowdhury et al., 2008). However, this has not been widely adopted.
As the first study of its kind, the primary aim of this survey was to describe this sample from an Australian shark-bite peer-support group and determine the prevalence of PTSD. We then evaluated the following hypotheses:
Negative media experience was an event-specific risk factor for PTSD;
Prior trauma history was a risk factor for PTSD.
Methods
This study was undertaken in partnership with Beyond the Bite Incorporated (BTB), a registered peer-support charity for shark-bite survivors, first responders and their families. BTB is funded by grants and charitable donations, and provides members with mentoring, social connection and shared experience, as well as practical support in hospital, and during rehabilitation, and return to function. The New South Wales Department of Primary Industries awarded BTB funding for the study under the Shark Management Strategy Annual Competitive Grants Program in November 2016. BTB signed a research collaboration agreement with The University of Sydney in May 2017. The university human research ethics committee approved the study in August 2017 (2017/606).
Participants
Members and affiliates of BTB, who all report, direct or indirect exposure to a shark-bite event, were invited to complete an online survey between October 2017 and March 2018. As this survey was the first of its kind, eligibility was limited to BTB members or affiliates residing in Australia.
Invitations containing the Participant Information Statement (PIS) and a survey link were emailed directly to participants by BTB. The online survey was preceded by another copy of the PIS and a Participant Consent Form. Those participants subsequently consenting to follow-up were contacted by researchers regarding qualitative interview.
Measurement
Psychological impact
The primary outcome of PTSD was measured with the validated self-report PTSD Checklist for DSM-5 (PCL-5) with Extended Criterion A (Weathers et al., 2013). No changes were made to the PCL-5, except for the specification of ‘worst shark bite event’ and the time period in the retrospective version, ‘… in the three months immediately following the event’. Extended Criterion A standard questions ‘Did it involve sexual violence?’ and ‘If the event involved the death of a close family member or close friend, was it due to some kind of accident or violence, or was it due to natural causes?’ were omitted to avoid confusion. The Life Events Checklist (LEC-5) was not used in this sample due to the specific nature of the primary stressor.
PTSD symptoms were assessed at two timepoints: retrospectively, to the best of the participant’s recollection, up to 3 months after the event (Cronbach’s α = 0.66); and currently, in the month prior to the survey (α = 0.66). PTSD was determined using a score threshold ⩾ 44, according to previous validation studies (Blanchard et al., 1996; Blevins et al., 2015). A score of 30–43 was used to describe those subthreshold, but highly symptomatic, in line with previous latent class analysis in combat-related PTSD (Korte et al., 2016; McDonald and Calhoun, 2010; Steenkamp et al., 2015).
Mental health variables
Other mental health variables were the well-validated Patient Health Questionnaire (PHQ-9, α = 0.60) used to measure symptoms of current depression with ranges: 1–4 = minimal; 5–9 = mild; 10–14 = moderate; 15–19 = moderately severe; and 20–28 = severe (Kroenke et al., 2001; Spitzer et al., 1999). Moderate or above depression was used in categorical analysis. The World Health Organization Disability Assessment Schedule (WHODAS-12, α = 0.64) was used to assess current disability with ranges: 1–4 = mild; 5–9 = moderate; and ⩾9 = severe (Australian Bureau of Statistics [ABS], 2009). Moderate or above scores were used to indicate disability. The Alcohol Use Disorders Identification Test Consumption (AUDIT-C, α = 0.71) brief screening assessed current alcohol misuse with thresholds of ⩾4 for men and ⩾3 for women (Bradley et al., 2007; Bush et al., 1998). Similarly, a threshold ⩾21 on the Suicidal Ideation Attributes Scale (SIDAS-5, α = 0.68) indicated a current high risk of suicidal behaviour (Spijker et al., 2014).
Demographic, event and media variables
Demographic questions and questions regarding chronic medical conditions were adapted from the National Survey of Mental Health and Wellbeing (ABS, 2007). Event-related risk factors, specific to the shark-bite event, media coverage and prior trauma were developed for this survey. A copy of the full survey is available from the authors. However, relevant custom questions are detailed in Supplementary Table 5. Variables ‘Event Exposure’, ‘Threat to Life’ and ‘Seriously Injured or Killed’ were derived from PCL-5 and Extended Criterion A in survey questions 6, 11 and 12 with minor adaptations to responses as described in Supplementary Table 5.
The variable ‘Prior trauma’ was derived from responses to survey questions 14 and 15 as described in Supplementary Table 5. For this analysis, the variable was derived specifically for post-event, not current, PTSD. Therefore, it includes any traumatic event(s), other than the shark-bite, occurring prior to the shark-bite event. Traumatic events occurring after the shark-bite event are excluded due to the focus on post-event PTSD.
Media variables were derived from questions 20–26 in Supplementary Table 5. The variable ‘Type of media coverage’ reports responses from question 16. ‘Media coverage duration’ is a self-report measure derived from question 21. Variables ‘positive media impact’ and ‘negative media impact’ were derived from separate questions: ‘Did the media coverage positively impact your recovery?’ and ‘Did the media coverage negatively impact your recovery?’. The variable ‘Needed media support’ was derived from question 25: ‘Did you need support in dealing with the media?’. The variable ‘Received media support’ was derived from question 26: ‘Who supported you in dealing with the media?’
Detailed, qualitative interviews were also conducted using the Adult Attachment Interview modified for a specific event (George et al., 1996; McLean et al., 2009; Main et al., 2002). However, these data represent a subset of participants and will be published separately.
Analysis
Quantitative data analysis was performed using SAS®. Baseline univariate analysis was performed on demographic, event, media, and mental health variables in line with initial hypotheses that a negative media experience and/or prior trauma were risk factors for PTSD in this sample. Summary, measurement and categorical variables were derived. In the questions relating to positive and negative media impact to recovery, the ‘no impact’ responses were converted to ‘no’ and some/high/extreme were converted to ‘yes’ separately for each question.
Four sets of analyses were undertaken using: post-event and current PCL-5 score; post-event and current PTSD; post-event and current subthreshold, excluding suprathreshold, PTSD; and post-event and current sub + suprathreshold, PTSD. However, this paper reports predominantly post-event PTSD. Logistic regression was used to calculate odds ratios (OR) in univariate analysis, and multivariate regression models used a backwards elimination approach to determine factors significant to post-event PTSD. Outliers were defined by studentised jackknife residuals greater than two and were removed from final models. Wald/linear proportions generated prevalence confidence limits. All confidence intervals (CIs) are 95% (α = 0.05).
Results
The overall response rate to the survey was 48.4% (60/124) as described in Figure 1. The 122-question survey took 42 minutes on average to complete, excluding outliers. However, participants were permitted to complete it over more than one session if they wished. Six participants (10%) took more than 2 hours to complete the survey. Sixty respondents commenced and 51 (51/60, 85.0%) fully completed the survey. The sample was older than the general Australian population with mean age of 44 ± 14 years.
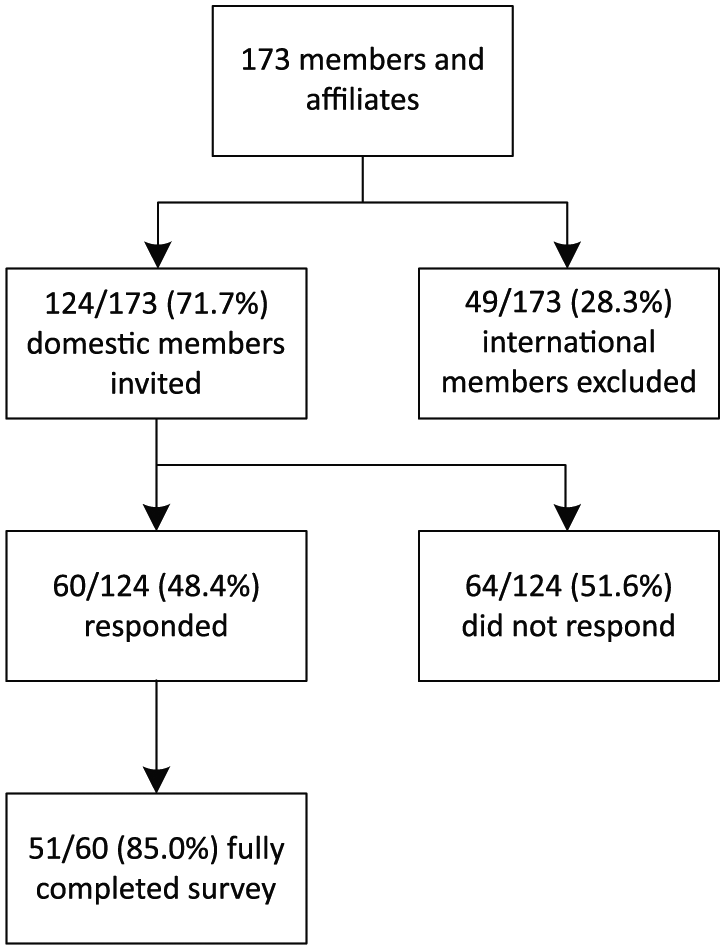
Strobe participant flow diagram.
As described in the following tables, PTSD was prevalent in this sample in the 3 months immediately post event (n = 16/59, 27.1%, 95% CI = [15.4, 38.8]), but less so currently (n = 2/55, 3.6%, 95% CI = [0.0, 8.7]). A further proportion was subthreshold, but highly symptomatic with PCL-5 scores between 30 and 43, both post event (n = 9/59, 15.3%, 95% CI = [5.8, 24.7]) and currently (n = 5/55, 9.1%, 95% CI = [1.3, 16.9]). With so few participants reporting current PTSD, all further analyses focus on post-event PTSD.
Demographic variables and post-event PTSD
As seen in Table 1, post-event PTSD was significantly higher in those without a partner (OR = 5.91, 95% CI = [1.52, 22.99], p = 0.01) or with two or fewer friends to rely on (OR = 5.83, 95% CI = [1.62, 21.01], p = 0.01).
Demographic variables and post-event PTSD.
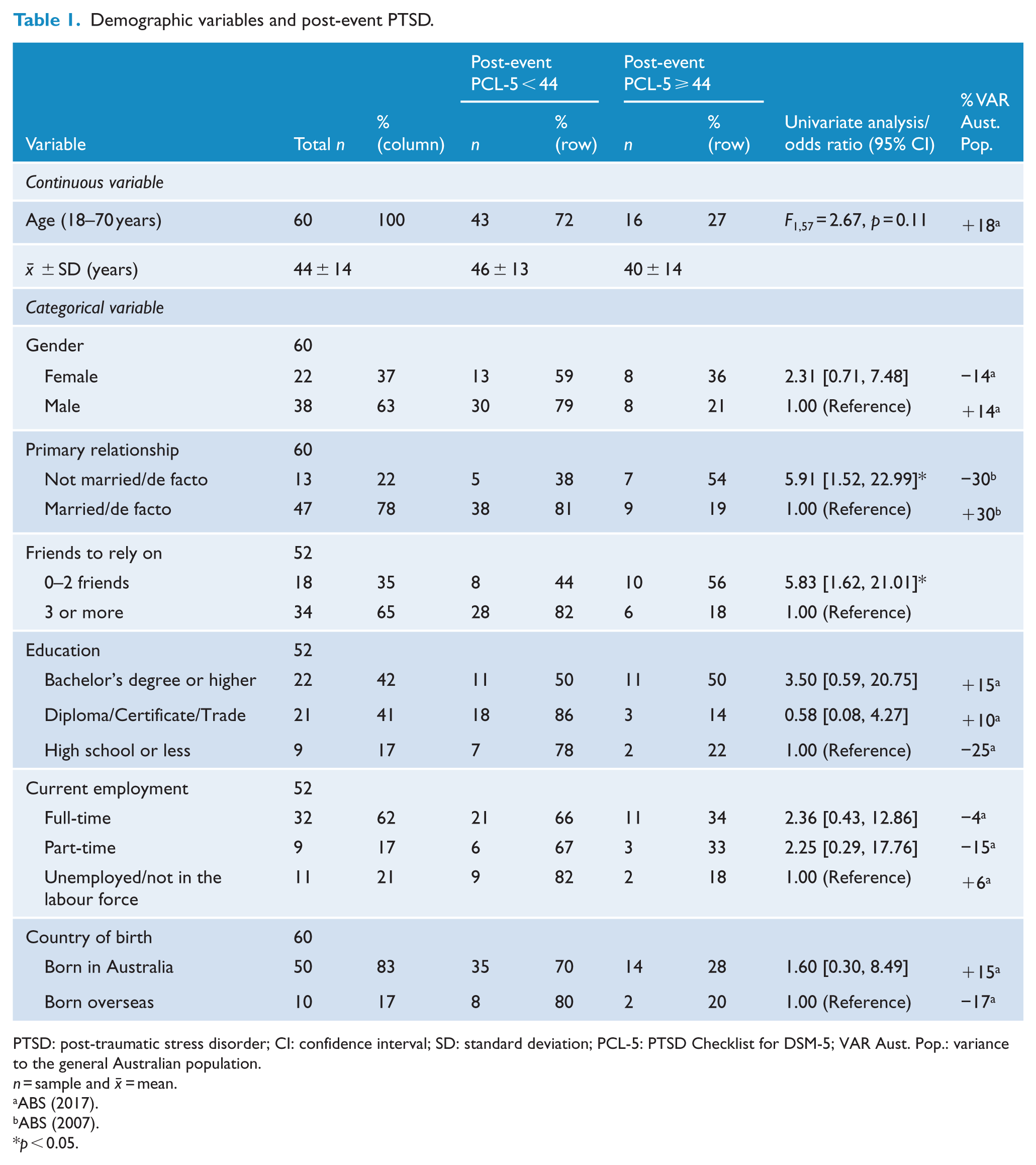
PTSD: post-traumatic stress disorder; CI: confidence interval; SD: standard deviation; PCL-5: PTSD Checklist for DSM-5; VAR Aust. Pop.: variance to the general Australian population.
n = sample and
p < 0.05.
A possible, weak association was found for post-event PTSD and age in this sample in preliminary univariable linear regression (F1,57 = 2.67, p = 0.11). Possible trend was also found in logistic regression of post-event PTSD with categorical variables gender (p = 0.16) and bachelor’s degree or higher education category (p = 0.17). However, there was no univariate association (p ⩾ 0.25) of post-event PTSD with other categories of education, current employment or country of birth.
Event and media variables and post-event PTSD
Event variables
As seen in Table 2, a possible, weak association was found between post-event PTSD and time since event in univariable linear regression (F1,57 = 2.32, p = 0.13). This variable is discussed later in multivariate modelling as a potential confounder.
Event and media variables and post-event PTSD.
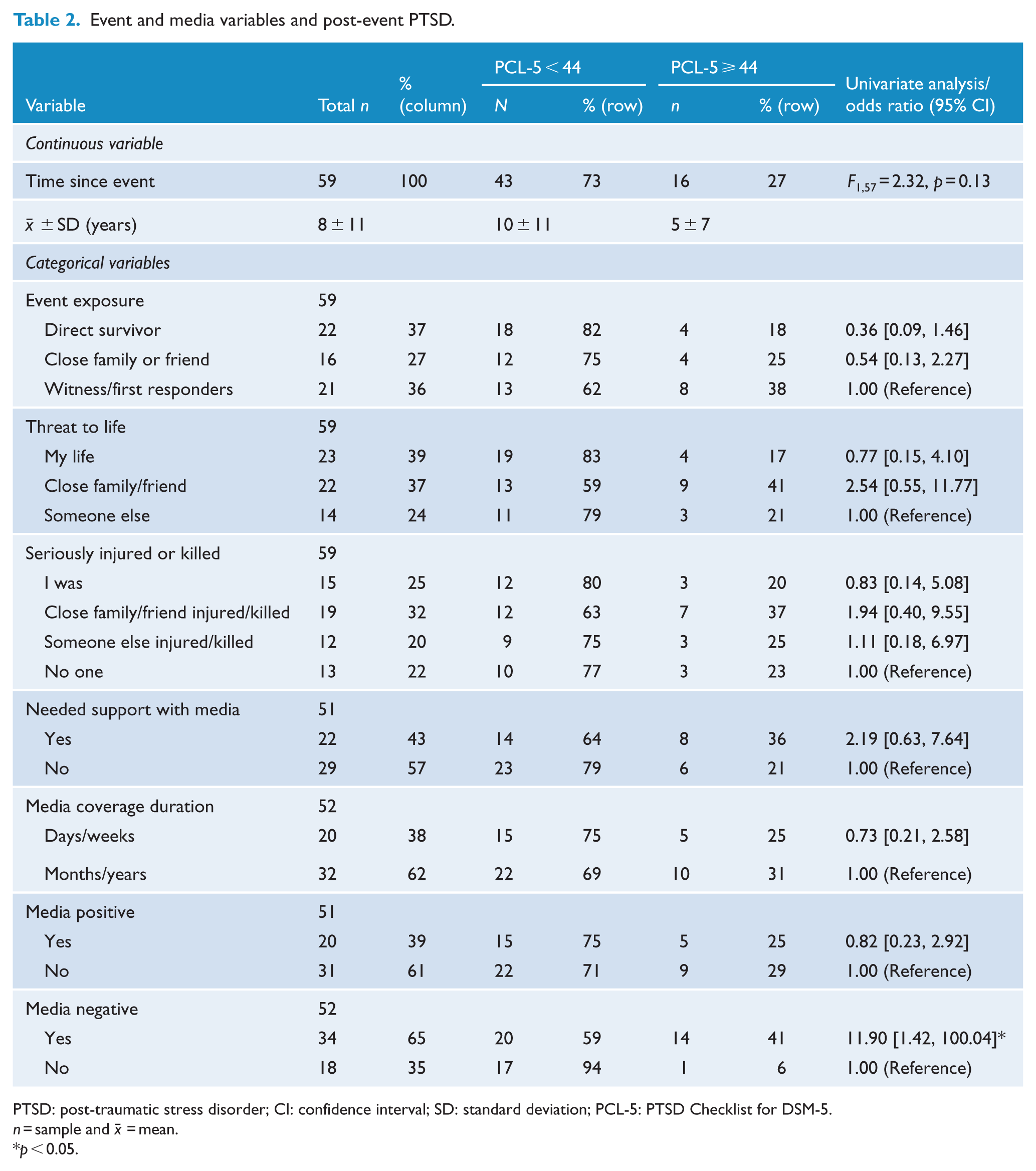
PTSD: post-traumatic stress disorder; CI: confidence interval; SD: standard deviation; PCL-5: PTSD Checklist for DSM-5.
n = sample and
p < 0.05.
A similar weak association was found between post-event PTSD and direct survivor event exposure category (p = 0.15) and close family/friend threat to life category (p = 0.23) in logistic regression. However, no association (p > 0.25) was found between post-event PTSD and whether someone was seriously injured or killed.
Media variables
Most respondents reported media coverage lasting months or years (n = 32/52, 61.5%) as seen in Table 2. Few reported no media coverage (n = 3/55, 5.5%). The media asked respondents: if they wanted the specific shark involved in their event killed (n = 23/51, 45.1%); their opinion on culling (n = 31/51, 60.8%); to relive their event (n = 36/51, 70.6%); and, to re-enact their event (n = 17/51, 33.3%).
Many experienced a negative impact to recovery from media coverage (n = 34/52, 65.4%) and, as seen in Table 2, this was significantly associated with post-event PTSD (OR = 11.90, 95% CI = [1.42, 100.04], p = 0.02). Respondents received support in dealing with the media from family (n = 22/52, 42.3%), friends (n = 15/52, 28.9%), hospital staff (n = 6/52, 11.5%) or professional media management (n = 4/52, 7.7%). In total, 22 respondents (n = 22/52, 42.3%) did not receive any media support, and 7 of these (n = 7/22, 31.8%) indicated that they had needed it.
However, there was little association between PTSD and needing support in dealing with the media (p = 0.22) in this sample, and no association with media coverage duration (p = 0.63) or positive media impact (p = 0.75).
Mental health variables and post-event PTSD
Chronic medical conditions, arising from the event and lasting 6 months or more, included conditions for direct survivors that may be anticipated of a shark-bite event, such as injury to arms/fingers (n = 8/22, 36.4%); legs/feet (n = 10/22, 45.5%); and disfigurement (n = 13/22, 59.1%). However, participants also indicated mental illness as a condition arising from the shark-bite event and lasting six months or more (n = 11/57, 19.3%).
Furthermore as described in Table 3, post-event PTSD was correlated with current PTSD (rs = 0.80, p < 0.001), and current depression (rs = 0.55, p < 0.001). It was also associated in univariate analysis with disability (OR = 5.00, 95% CI = [1.34, 18.62], p = 0.02) and alcohol misuse (OR = 6.02, 95% CI = [1.49, 24.26], p = 0.01).
Mental health variables and post-event PTSD.
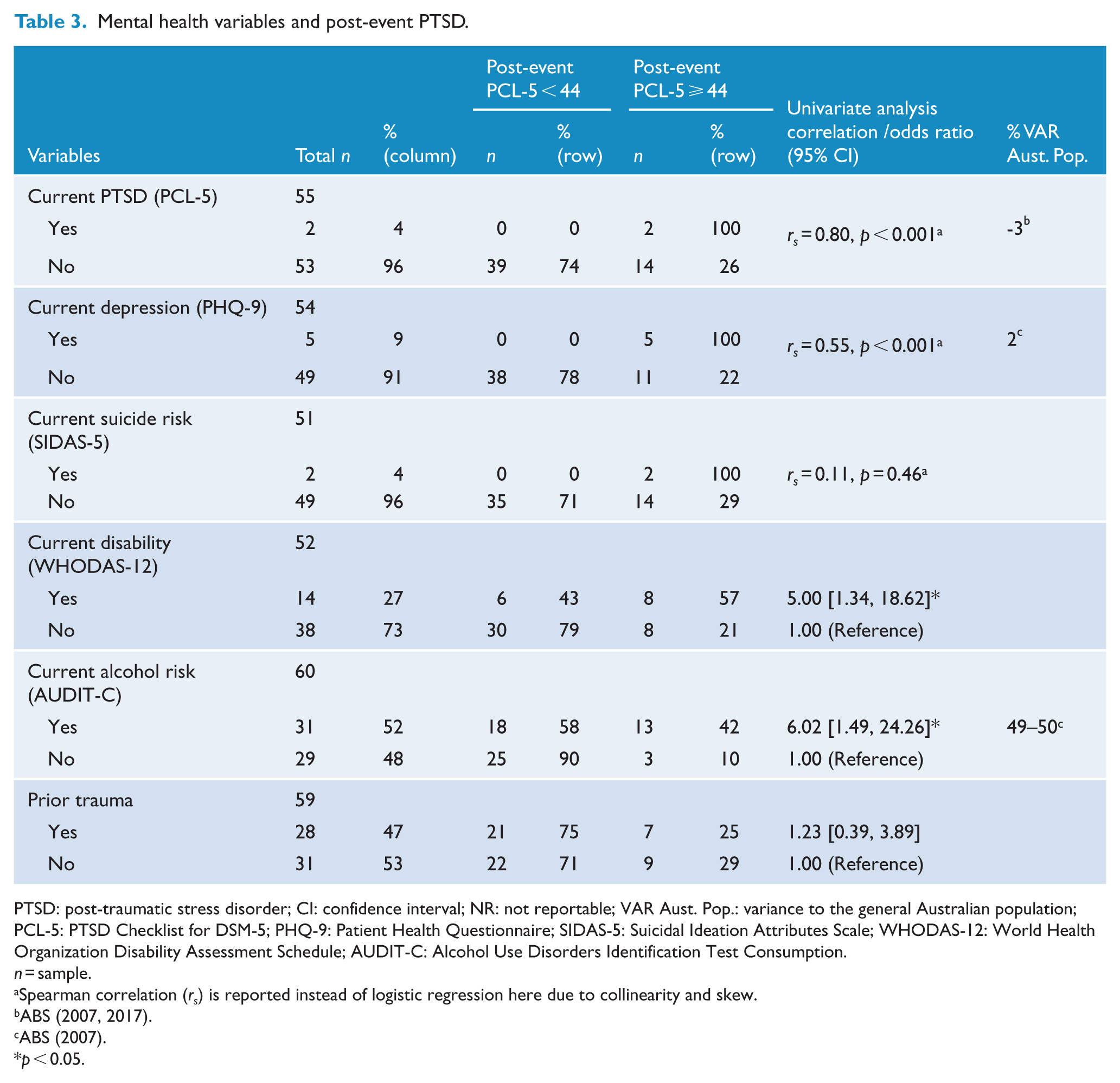
PTSD: post-traumatic stress disorder; CI: confidence interval; NR: not reportable; VAR Aust. Pop.: variance to the general Australian population; PCL-5: PTSD Checklist for DSM-5; PHQ-9: Patient Health Questionnaire; SIDAS-5: Suicidal Ideation Attributes Scale; WHODAS-12: World Health Organization Disability Assessment Schedule; AUDIT-C: Alcohol Use Disorders Identification Test Consumption.
n = sample.
Spearman correlation (rs) is reported instead of logistic regression here due to collinearity and skew.
p < 0.05.
However, as seen in Table 3, PTSD was not associated with prior trauma (OR = 1.23, 95% CI = [0.39, 3.89], p = 0.73).
Multivariate analysis
Multivariate base models were constructed for post-event and subthreshold PTSD. Negative media impact was the only significant event-related factor (F1,50 = 8.13, p = 0.01, r2 = 0.14). Demographic factors significant in univariate testing were: primary relationship (F1,57 = 8.21, p = 0.01, r2 = 0.13); friends to rely on (F1,50 = 9.01, p = 0.004, r2 = 0.15); and education (F2,49 = 3.69, p = 0.03, r2 = 0.13). Other mental health factors were excluded due to commonly known correlations.
Age and time since event were also included in base models as potential confounders of memory, recovery and/or resilience for PTSD. These factors were also correlated with each other (rs = 0.38, n = 59, p = 0.003) and inversely associated with PTSD. Backwards elimination removed time since event and education from the model as non-significant (p > 0.05), and no effect modification was observed for age. Final models were adjusted to remove outliers.
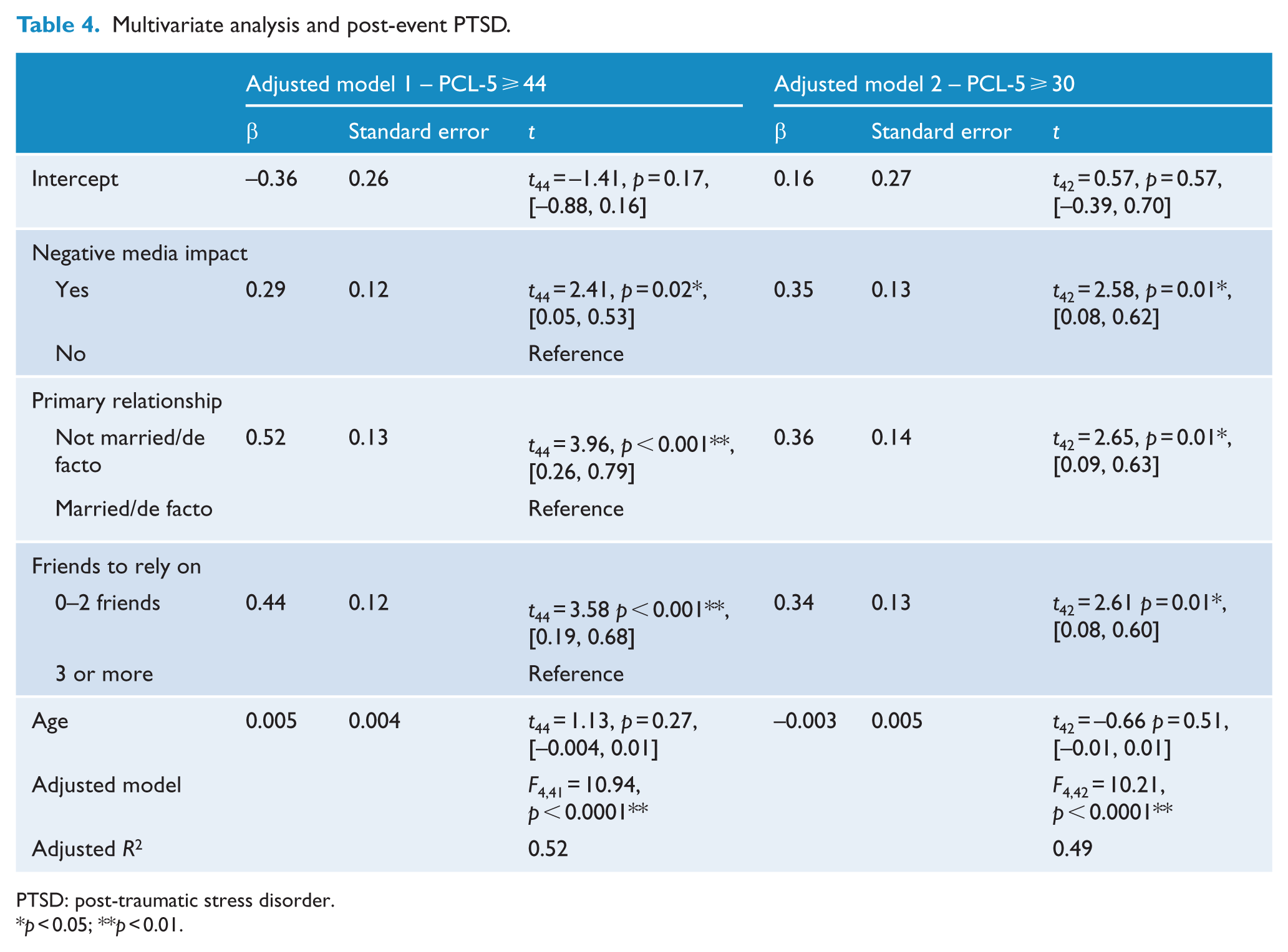
The association between post-event PTSD and negative media impact was significant, controlling for primary relationship, friends and age (F4,44 = 4.28, p = 0.01, r2 = 0.28). After adjustment as seen in Table 4, this association was strengthened, and the final model explained 51.6% of the variance in post-event PTSD (F4,41 = 10.94, p < 0.0001, r2 = 0.52). All factors, except age, were statistically significant (p < 0.05).
Multivariate analysis and post-event PTSD.
PTSD: post-traumatic stress disorder.
p < 0.05; **p < 0.01.
There was also an association between sub + suprathreshold PTSD, with PCL-5 scores over 30, and negative media impact controlling for relationship, friends and age, before (F4,44 = 6.46, p = 0.004, r2 = 0.37) and after adjustment (F4,42 = 10.21, p < 0.0001, r2 = 0.49).
Finally, sensitivity analyses with continuous post-event PCL confirmed a significant association between PTSD symptoms and negative media impact, controlling for age, primary relationship and friends, before (F4,44 = 8.72, p < 0.001, r2 = 0.44) and after adjustment (F4,41 = 12.29, p < 0.001, r2 = 0.55).
Discussion
This is the first study to describe the psychological impacts on people exposed to shark-bite events. There is a high prevalence of retrospectively self-reported PTSD within three months following the event (n = 16/59, 27.1%, 95% CI = [15.4, 38.8]), almost three times the national average (ABS, 2007, 2017). However, respondents also showed possible resilience with a much lower prevalence of current PTSD (n = 2/55, 3.6%, 95% CI = [0.0, 8.7]). Although, there were high levels of subthreshold symptoms post event (n = 9/59, 15.3%, 95% CI = [5.8, 24.7]) and currently (n = 5/55, 9.1%, 95% CI = [1.3, 16.9]), and although depression was equivalent to the general Australian population, there were potentially higher rates of suicidal ideation and disability in this sample (ABS, 2017).
Interestingly, the distinction between direct and indirect event exposure was not significant in the development of post-event PTSD. Direct survivors were not more likely to develop PTSD than witnesses/first responders or family/friends. The non-significance of proximal exposure is a significant finding, particularly for support programmes, and suggests that trauma-specific interventions should target all exposure groups.
This is not necessarily contrary to trauma literature. Bereavement has previously been shown to contribute to the development of PTSD (Liu et al., 2014). PTSD transmission and transgenerational trauma has also been observed in spouses and families, particularly in combat- and conflict-related complex trauma (Burchert et al., 2017; Yehuda et al., 2008). Furthermore, trauma type, such as personally assaultive violence, has been demonstrated as an influential factor in PTSD and complex trauma (Breslau, 2009). Therefore, due to being a top-order predator with cultural status, a shark-bite event may be perceived as violence against an individual in a way that accidents and natural disasters are not. Public perception literature suggests the projection of intentionality onto sharks, and gender studies literature proposes that trauma may be exacerbated by becoming prey (Neff, 2014; Neff and Hueter, 2013; Plumwood and Shannon, 2012).
One finding was contrary to the a priori hypothesis that those with a prior history of trauma are more likely to develop PTSD. Post-event PTSD and prior trauma were not associated in this sample. This may be due to survey design, sample characteristics, trauma type or media exposure. However, it may also be that growth from earlier trauma confers resilience for this type of trauma.
The major finding in this study is the significant association between PTSD and the negative psychological impact of media coverage. In univariate analysis, those reporting a negative media impact to recovery were almost 12 times more likely to develop PTSD (OR = 11.90, 95% CI = [1.42, 100.04], p = 0.02). This factor remained significant in multivariate analysis after controlling for age, primary relationship and friendship (p = 0.01). Moreover, 61.5% (n = 32/52) of respondents experienced media coverage lasting months or years, and 65.4% (n = 34/52) felt that media coverage had a negative impact on their recovery. There was also no evidence that post-event PTSD was associated with needing media support.
While it is possible that those with early symptoms are more likely to have a negative media experience, this finding confirms that the 24-hour news cycle and rapacity of journalists may feel predatory for those affected. As such, individual interventions may not be enough and existing media guidelines for reporting suicide, trauma and mental health, such as those produced by McMahon et al., (2014), may need adaptation for this kind of trauma. Journalists are often first responders and may also be affected.
Respondents also reported a positive impact to their recovery from media coverage. A positive media experience may support development of a personal trauma narrative, a survivor ‘story’, and new identity. Nonetheless, positive media impact was not associated with PTSD.
Therefore, findings support activities targeting negative media impact, such as media reporting and practice guidelines. These might include: acknowledging and defining a shark-bite event as a traumatic event not only for those present, but also their family, and community; minimising the reporting of graphic event detail, such as injuries, shark size and type; and providing accurate information about where to seek help. Peer- and relationship-support is also encouraged. Interventions, such as counselling or psychotherapy, should be trauma-specific and trauma-sensitive. They should support close family/friends, witnesses and first responders, as well as direct survivors.
Limitations
While the response rate is relatively high for community surveys at 48.4%, the small size of this sample is a limitation to data analysis. Effects had to be very strong (OR > 3 or <0.3) to be observed and smaller, potentially important, effects may have been missed when relying upon statistical tests. Recruitment was also limited to Australian residents and members/affiliates of BTB. Future research might include other domestic and international participants to improve representation of shark-bite survivors, and/or the wider community experiencing symptoms or behavioural changes, despite lower levels of exposure.
Similarly, low levels of current PTSD may indicate that, rather than being resilient, some participants experienced Acute Stress Disorder rather than PTSD. Confounding by age and time since event may also mask the healing effect of time, or a memory effect due to the retrospective study design. There was a trend for PTSD in those that were younger and/or chronologically closer to their event. While this might suggest resilience with age or recovery over time, it may also reflect the changes in the digital media landscape over the last 20 years. This may warrant further investigation.
Finally, as this is the first-ever study of the direct and indirect psychological impacts of shark-bite events, retrospective measurement was necessary. However, this may be addressed by timely and consistent baseline and follow-up psychological assessment, such as a case register, for these rare events.
Supplemental Material
Supplementary – Supplemental material for Direct and indirect psychological impacts of shark-bite events
Supplemental material, Supplementary for Direct and indirect psychological impacts of shark-bite events by Jennifer Taylor, Loyola McLean, Anthony Korner and Nicholas Glozier in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
J.T. is the spouse of a board member of Beyond the Bite Incorporated (BTB). This was declared in the Participant Information Statement (PIS).
Funding
The New South Wales Department of Primary Industries awarded the funding for this study under the Shark Management Strategy Annual Competitive Grants Program.