
Abstract
On 26 December 2004 an Indian Ocean tsunami destroyed large parts of the southwestern coastal regions of Southeast Asia, as well as parts of the western Australian and the southeastern Indian and African coasts. This massive natural disaster, which followed a strong earthquake in the Indian Ocean, caused the death of approximately 230 000 individuals. At the beginning of 2005 tens of thousands were missing and more than 1.7 million people were displaced [1].
Apart from being the permanent place of residence to approximately 600 million people, the affected area of southeastern Asia is a holiday region for tourists from all over the world. During the annual Christmas break in 2004, an unknown number of tourists from dozens of nations spent their holidays there. Around 130 Swiss tourists never returned home: they were either killed directly by the wave or remained missing in the aftermath of the tsunami [2]. The Swiss Federal Department of Foreign Affairs (EDA) in Bern set up a helpline immediately after the tsunami occurred. From 26 December 2004, 11:19 CET, a total of 4118 Swiss tourists were reported missing; an unknown percentage being possible tsunami victims.
Individuals affected by a natural disaster such as this tsunami are exposed to extreme stressors. These stressors represent risks for mental health problems, in particular post-traumatic stress disorder (PTSD) [3]. Studies conducted in adults after natural disasters report an incidence of acute PTSD of up to 89% within the first 3 months, and a prevalence of chronic PTSD of 6–50% [4–10].
Studies currently available on the psychological outcome of the 2004 tsunami were mostly conducted on inhabitants of the affected areas and show PTSD prevalence rates of 13–56% [11–17]. In addition to the primary impact of the traumatic event, inhabitants of affected areas run the risk of secondary, ongoing difficulties such as lack of water, food and shelter and so on, which might play an important role in determining the amount of psychiatric morbidity [18]. Therefore, hitherto reported PTSD prevalence rates following natural disasters, specifically the 2004 tsunami, represent the consequences of multiple, sequential traumatization and are considered to be high when compared to findings in tourists who returned home after the disaster. The availability and sufficiency of mental health treatment for homecoming tourists affected by distant, large-scale disasters remain important but underresearched subjects.
Apart from the possible development of psychopathology in the aftermath of natural disasters, for some trauma survivors, the more time passes the more chance there is of positive personal change. Previous research on trauma survivors has shown that in some people coping with significant trauma can lead to psychological growth. Post-traumatic personal growth has been shown to be related to reduced distress and improved quality of life [19]. Against this backdrop, post-traumatic personal growth is an important and indispensable factor to be included in long-term trauma research [20].
Aims
The purpose of the present study was to extend the current knowledge about tourists involved in the hazardous events of the 2004 tsunami with respect to psychiatric morbidity, mental health treatment and potential positive outcomes after their return to Switzerland. Given Switzerland's highly effective health-care system and stable socioeconomic situation, we anticipated low levels of psychopathological symptomatology in the present sample of Swiss tourists returning from the area affected by the 2004 tsunami. With regard to post-traumatic personal growth, the study was of an exploratory nature and, therefore, no hypotheses were formulated.
Methods
Subjects and procedure
For the period of 1 month, 26 December 2004–25 January 2005, a tsunami helpline was operating day and night at the Swiss Federal Department of Foreign Affairs (EDA), Bern, Switzerland. A total of 3855 addresses of missing persons, couples and families were reported to the EDA by relatives, friends or anyone worried about a person possibly located in the region affected by the tsunami. We obtained the approval of both the Ethics Committee of the canton of Zurich and the EDA to analyse the addresses of couples and families and we continued to identify a total of 4118 individuals who had been reported to the EDA. From this group of people potentially affected by the tsunami, we excluded the following: 100 deceased persons; 108 persons under 18 years of age at the time of the tsunami; 1060 persons living in the non-German-speaking part or outside of Switzerland; 1153 persons with incomplete and/or untraceable addresses and 73 persons who were not in the affected region when the tsunami occurred.
Thus, 1624 individuals were eligible for the postal survey on German-speaking adult Swiss tourists affected by the tsunami. The questionnaires were sent out in mid-May 2007. A total of 209 questionnaires were sent back by the Post Office as undeliverable. By 1 September 2007, 342 questionnaires (24.2%) had been returned and were completed sufficiently for inclusion in the analysis.
Measures
The actual tsunami exposure was assessed by a question offering six response categories related to the tsunami experience: ‘I was caught up in the wave’; ‘I could seek shelter, i.e. run away’; ‘I saw the wave and the destruction, i.e. from a safe spot’; ‘I came into the destroyed area after the wave, but did not see the wave itself’; ‘I heard about the tsunami while staying in an affected country’; ‘I heard about the tsunami while staying in an unaffected country’. For part of the analysis we grouped categories 1–2 as direct and categories 3–6 as indirect/no exposure.
Symptoms of PTSD were assessed by the German version [21] of the self-report Post-traumatic Diagnostic Scale (PDS) [22] by which participants are asked to rate the presence of each of the 17 symptoms of PTSD. The PDS uses 4 point (0–3) Likert scales, ranging from 0 = not at all, 1 = a little bit, 2 = somewhat, to 3 = very much, to measure symptom severity. This scale produces a symptom severity score with 1–10 representing mild; 11–20 moderate; 21–35 moderate–severe; and 36–51 severe symptomatology. In addition, based on the PDS it can be established whether or not a subject fulfils the diagnostic criteria for PTSD. In the present study the PDS demonstrated high internal consistency (Cronbach's α = 0.92).
Anxiety and depression were assessed on the Hospital Anxiety and Depression Scale (HADS), a 14-item self-rating questionnaire for the dimensional assessment of anxiety and depression [23]. The range for both scales is 0–21; scores 8–10 indicate possible, scores >10 indicate a probable depression or anxiety disorder. In the present study the HADS demonstrated good internal consistency on the anxiety (α = 0.83) and depression scale (α = 0.85).
Post-traumatic personal growth was assessed using the German version of the Post-traumatic Growth Inventory (PTGI) [24, 25]. The PTGI consists of a global score with 21 items that are rated on a Likert scale from 0 (not true) to 5 (completely true), the total score range is 0–105. In the present study the PTGI demonstrated excellent internal consistency (α = 0.97).
Mental health treatment was assessed using two questions about psychiatric and/or psychological treatment (yes/no) before and after the tsunami occurred.
Data analysis
All statistical analyses were performed using SPSS version 15.0 for Windows (SPSS, Chicago, IL, USA).
Sequential regression analysis was applied in order to identify the statistical influence of trauma exposure (entered in step 2 in the regression model; six categories ranging from ‘I was caught up in the wave’ to ‘I heard about the tsunami while staying in an unaffected country’) over four risk factors (age, gender, psychiatric history, current partnership; entered in step 1 of the model) on the dependent variable PTSD symptom score.
General linear models (GLMs) were applied to test the influence of tsunami exposure (direct vs indirect/no tsunami exposure) on the sum scores of PDS, HADS–Anxiety (HADS-A), HADS–Depression (HADS-D), and PTGI. Each of these models was controlled for those variables that proved to be of statistical significance in step 1 of the regression analysis described here. Because PDS, HADS-A, HADS-D, and PTGI might be interrelated, the dependent variables of the three remaining models were entered as covariates in each model also.
Because some participants had obtained mental health treatment after the tsunami, regression analysis and GLMs were repeated with the exclusion of the respective subjects. This precaution, however, had virtually no influence on the analyses, therefore the results of multivariate analyses are reported for the complete sample only.
Results
Sociodemographic characteristics are presented in Table 1. The mean age at the time of the tsunami for the total sample was 46.9 years (SD = 13.8). Mean age of male respondents was 49.1 years (SD = 13.5), that of female respondents was 44.3 years (SD = 13.7). Respondents were older than non-respondents (Pearson's χ2=15.618, df = 3, p = 0.001) and a greater proportion of women who were contacted participated in the survey compared with the proportion of men (Pearson's χ2=5.368, df = 1, p = 0.021).
Subject characteristics
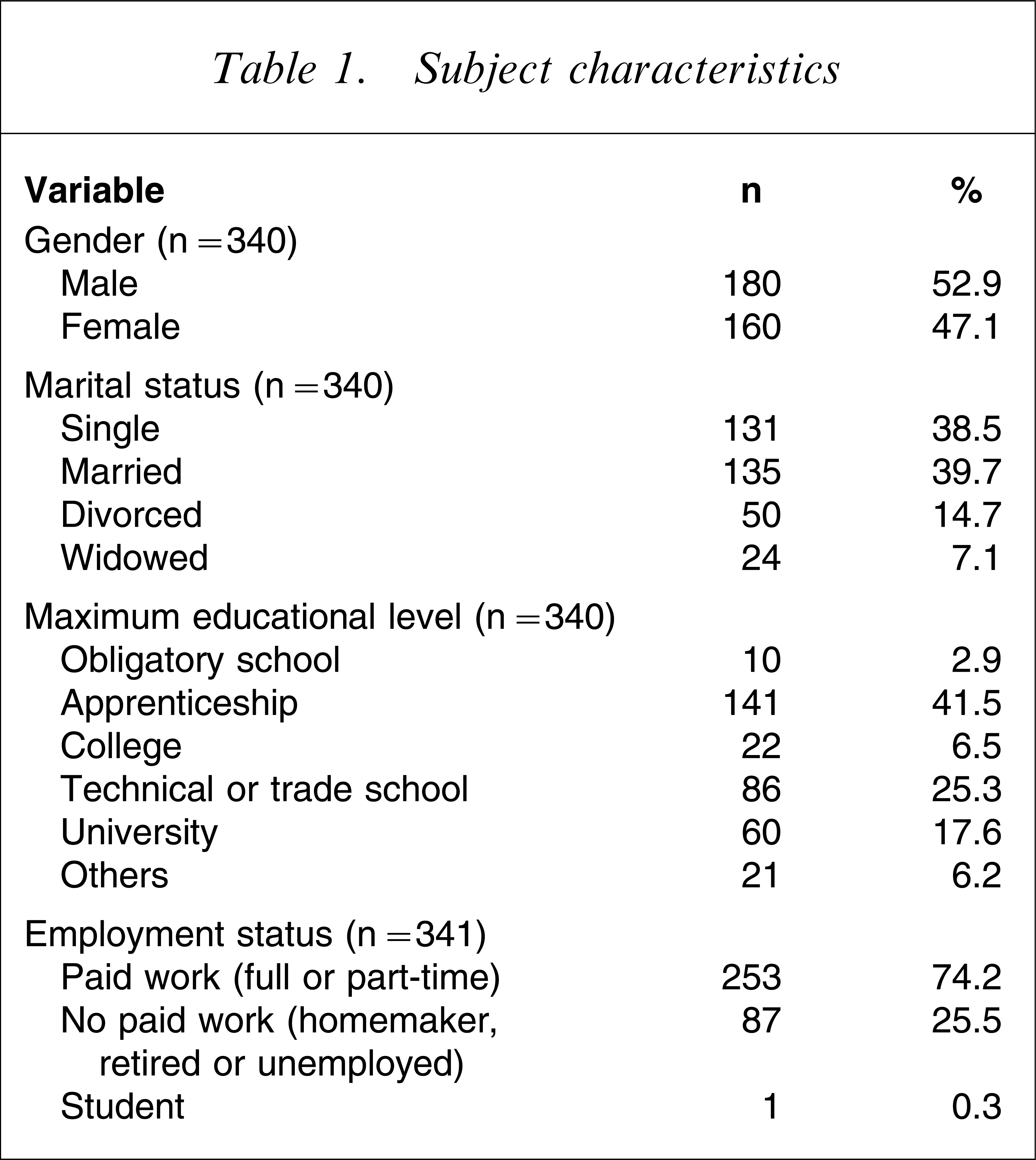
A total of 178 individuals reported direct exposure to the tsunami, while 159 individuals had indirect or no exposure (missing, n = 5). A total of 55 respondents (16.8%) fulfilled diagnostic criteria for the DSM-IV diagnosis of PTSD. We found a mild PTSD symptomatology in seven (12.8%), a moderate form in 24 (43.6%), moderate–severe symptoms in 19 (34.5%) and severe PTSD symptoms in five (9.1%). Among those who fulfilled diagnostic criteria for PTSD, 44 (80%) had been directly affected, and 10 (18.2%) had been indirectly/not affected by the tsunami (missing, n = 1; χ2=21.6; df = 1; p < 0.001). Analysis of the anxiety data indicated a possible anxiety disorder in 37 (11.0%) and a probable anxiety disorder in 23 (6.8%). We found a possible depressive disorder in 20 respondents (5.9%) and a probable depressive disorder in seven (2.1%).
A total of 2.6% of variance (adjusted R2) of PTSD symptom severity was explained by step 1 of the sequential regression analysis, with gender (β = 0.12) and age (β = 0.11) reaching statistical significance. Step 2 (tsunami exposure, β = 0.38) added 14.1% variance explanation, totalling a 16.7% overall variance explanation for PTSD symptom severity (all βs taken from step 2 of the regression model).
Detailed results of GLMs for PDS, HADS-A, HADS-D and PTGI scores are presented in Table 2. Controlling for the influence of several covariates, the dichotomized measure of direct versus indirect/no tsunami exposure resulted in significant group differences for PDS and PTGI scores, but not with respect to HADS-A/D scores.
Psychological outcome of tsunami survivors using GLM
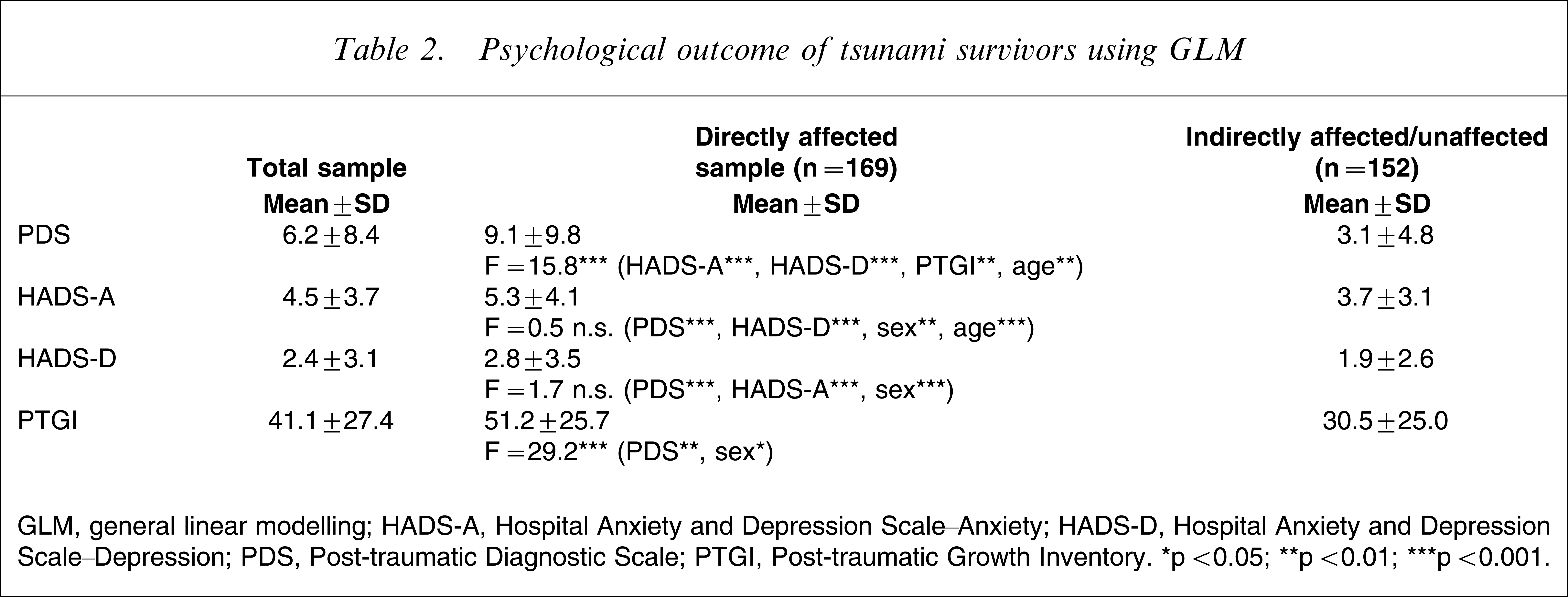
GLM, general linear modelling; HADS-A, Hospital Anxiety and Depression Scale–Anxiety; HADS-D, Hospital Anxiety and Depression Scale–Depression; PDS, Post-traumatic Diagnostic Scale; PTGI, Post-traumatic Growth Inventory. ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
A total of 77 (22.8%) respondents reported having had psychological or psychiatric treatment at some point before the tsunami occurred. After the tsunami, 25 of them were currently (i.e. still or again) undergoing psychiatric/psychological treatment. During the 2½ years following the tsunami, a total of 58 respondents (17.2%) received psychological or psychiatric treatment. Participants receiving mental health treatment after the tsunami reported significantly higher scores in all four main outcome measures (PDS, t = 4.9; HADS-A, t = 4.8; HADS-D, t = 3.2; PTGI, t = 5.7; all p < 0.01) than untreated respondents.
A total of 14 (18.9%) of the tsunami survivors who had undergone some sort of mental health treatment prior to the disaster, and 41 (16.2%) of the formerly untreated participants fulfilled the criteria for PTSD at the time of the present survey. Sixty per cent of all PTSD subjects did not receive treatment for PTSD during the period we observed.
Discussion
To the best of our knowledge, we are presenting the first study of tsunami-affected tourists that uses validated measures and addresses both negative and positive long-term psychological outcomes. A considerable proportion of Swiss tsunami survivors (16.8%) showed clinically relevant levels of PTSD symptomatology as long as 2½ years after the disaster. Despite Switzerland's highly developed mental health-care system, however, the majority of these survivors did not receive appropriate treatment.
The present study has a number of limitations that should be borne in mind when interpreting the results. First, although the cross-sectional design provides an initial insight into associations of disaster factors and psychological outcome, a longitudinal design would have allowed for more in-depth analyses of the natural course and of potential protective and risk factors, such as intervening events. A truly prospective follow-up study including pre-trauma baseline assessments is almost impossible to carry out because, by definition, disaster strikes unexpectedly. Second, concerning gender and age, the present respondents were older and more frequently female than the non-respondents. Because an increased risk for post-traumatic stress symptoms is reported for female gender and older age [26, 27], this sampling bias might have influenced the results towards a higher PTSD prevalence. Regression analysis, however, demonstrated that only a little over 2% of the variance in PTSD symptoms were ascribable to gender, age, pre-traumatic psychiatric morbidity and current partnership. Third, we have no information about additional traumatic events that might have occurred after the participants returned to Switzerland. Potentially traumatic events during the 2½ year period between the tsunami and the survey may have again influenced the results towards an increase in PTSD symptom levels.
We found the PTSD prevalence in the present sample to be in the lower range of the existing data reported on psychological outcome following natural disasters. We suggest that a limited impact of secondary stressors and a restored sense of safety after returning home, can be seen as some protective factors that paved the way to this relatively low level of post-traumatic morbidity in the present sample of Swiss tourists compared to earlier studies of victims of natural disasters [16, 28]. Despite this comparatively low PTSD prevalence, however, we found that 16.8% of the home-coming Swiss tourists met the diagnostic criteria for PTSD 2½ years after the tsunami. This prevalence rate is substantially higher than rates previously reported from the follow up of severely injured accident victims in Switzerland [29, 30]. In the present study PTSD symptom severity was explained by gender, age and tsunami exposure, but none of the other investigated predictor variables. Thus, we imply that natural disasters possess a major destructive potential on psychiatric morbidity exceeding the psychologically destructive potential of accidents.
Only in the directly affected tsunami survivors were anxiety levels seen to exceed the values of the general population. All other findings for anxiety or depression were comparable to, or even below, corresponding results for the general population [31–34]. Direct tsunami exposure was strongly associated with elevated PDS and PTGI scores, but not with HADS-A/D scores. Therefore the present data support the so-called complication model, which considers comorbidity a consequence of PTSD [35]. According to this model, comorbidity occurs ‘in reaction to, or as complications of, PTSD’ [10]. This is in accordance with data from many studies reporting that comorbid disorders develop secondarily to PTSD or that further mental disorders are common in traumatized subjects with PTSD, but not in subjects exposed to traumatic events who do not develop PTSD [35].
In addition to the potentially devastating effects on mental health, traumatic events can provoke processes of personal growth and development. Post-traumatic personal growth might result from dealing with an unexpected and overwhelming traumatic event and the resulting adversities. We identified several studies conducted in German-speaking countries, reporting PTGI scores ranging from approximately 20 to 50 [25, 36]. The present subgroup of directly affected tourists had PTGI scores >50, pointing to the possibility of post-traumatic personal growth as a possible outcome following a natural disaster. This finding lends support to the idea of relational closeness of adversity and growth and is in keeping with the generally received wisdom that ‘struggle often precedes growth’. Therefore, processes of post-traumatic personal growth may play an important role in processing the adverse effects of natural disasters.
During the observation period, only 40% of all participants who fulfilled diagnostic criteria for PTSD in the present study received psychiatric treatment. Switzerland does suffer natural disasters such as massive rock falls, land slides, avalanches and storms but it is rarely affected by large-scale natural disasters. Therefore, Swiss health professionals may not be sufficiently aware of the resulting psychological problems and might perhaps miss the challenge of linking a distant disaster to ‘imported’ psychopathology in patients who had once been disaster-affected tourists. A second reason for this probable under-supply of treatment may be found in the severity of the PTSD symptoms. Fifty per cent of moderate severe/severe PTSD subjects had mental health support, whereas only 14.7% of people with mild cases received treatment.
To summarize: we assume that the relatively high PTSD prevalence in the present study reflects the major destructive potential of natural disasters and may also be explained by undetected PTSD symptoms, consecutively missed treatment, and possibly insufficient psychotherapeutic interventions when tourists return home after experiencing hazardous events. We recommend that home-coming tourists returning from regions affected by natural disasters be informed about PTSD and that careful screening be given to those found to be at risk of PTSD.
Footnotes
Acknowledgements
The authors wish to thank the Swiss Federal Department of Foreign Affairs (EDA) for cooperation. The study was supported by the Anna Feddersen-Wagner-Fonds.