
Abstract
Background:
It is well established that depression and non-communicable diseases are highly co-morbid and bi-directional in nature. ‘Lifestyle medicine’ has recently gained traction in the field of psychiatry, aimed at improvement of both physical and mental health. Online interventions can be an effective and inexpensive alternative or supplement to therapy that is delivered using more traditional modes, overcoming barriers that may prohibit people from accessing treatment by promoting flexibility and accessibility.
Methods:
This systematic review evaluates the existing evidence for the efficacy or effectiveness of lifestyle interventions for (1) individuals with depressive symptoms, (2) clinically depressed populations or discussing the outcomes of depression within a subset of a larger cohort that are delivered online or via smart phone. Included studies were randomised controlled trials, with active comparator conditions, in adult populations and with reported lifestyle and depression-related outcomes. The analysis examined attrition, engagement, adherence and behaviour change techniques employed to achieve the target behaviours.
Results:
Seven studies were included in the review and targeted behaviour change in five domains: alcohol reduction, improved sleep quality/insomnia reduction, increased physical activity, reduced/cessation of substance abuse and smoking cessation. Four of the studies achieved significant improvements in the targeted behaviour; of these three also reported significant improvements in depressive symptoms. No studies reported significant improvements in depressive symptoms without a change in the target lifestyle behaviour.
Conclusion:
The results of this review highlight the potential of online lifestyle interventions as adjunctive treatments for depression, and the possibility of achieving significant improvements in depressive symptoms when targeting lifestyle behaviour change.
Introduction
Depression is now the leading cause of disability worldwide, affecting 322 million people or 4.4% of the world’s population (World Health Organisation, 2017). Depression places a huge burden on the individual, their family and society more generally (Lépine and Briley, 2011). The wide-reaching impacts of this disorder (Hidaka, 2012) highlight the necessity for treatment and prevention strategies that are widely accessible.
Poor lifestyle behaviours, such as poor diet, physical inactivity, insufficient sleep, smoking and substance abuse, are increasingly recognised as contributing to both poorer physical and mental health. For example, poor lifestyle is associated with increased depression risk, while in turn, the symptoms of depression may influence poor lifestyle choices (Sarris et al., 2014). ‘Lifestyle medicine’ has thus gained traction in the field of psychiatry, encompassing treatments targeting nutrition, physical activity, sleep and addictions. In their 2014 review, Sarris et al. highlighted the emerging evidence of these types of interventions in the context of depression, demonstrating the potential for treatments addressing diet, physical activity, smoking cessation, substance abuse and meditation alongside pharmacotherapies and related psychological techniques, in depression management.
It is estimated that in some countries, fewer than 10% of those with major depression currently seek help through mental health services (Hadjistavropoulos et al., 2014). Online interventions (e.g. web-based, mobile, smartphone-delivered) for depression may help to overcome some of the real and perceived barriers to help seeking among this population, providing scalable and cost-effective alternatives. In recent years, an increasing number of studies report successful online delivery of psychological interventions and education programmes for treating or preventing depression (Richards and Richardson, 2012), particularly cognitive behavioural therapy (CBT) based models (Huguet et al., 2016; Mohr et al., 2010; Spek et al., 2007).
Despite their potential advantages, online and smartphone-based interventions can be limited in their ability to engage and retain participants, with high attrition a well-recognised issue in the field (Christensen and Mackinnon, 2006; Eysenbach, 2005; Geraghty et al., 2013). Thus, the ‘success’ of online interventions should also consider uptake, accessibility and robust estimates of ‘effective engagement’ in line with the recent recommendations of Michie et al. (2017). Previous online interventions should be evaluated to determine their efficacy among the target demographic and synthesise teachings about what strategies work best for enhancing user engagement. Research is needed to determine what works, and how, so that future interventions aiming to target behaviour in depressed populations can be evidence-based by design to achieve their behaviour change outcomes.
Online psychological interventions for depression (Griffits et al., 2010; Richards and Richardson, 2012) and health behavioural change (Evers et al., 2003; Webb et al., 2010) have demonstrated success in both achieving desired outcomes, and reaching those with limited access to traditional treatments. However, no current study or review exists that examines the use of lifestyle behaviour change interventions in the context of depression; this is important to address as the fatigue and related symptoms in those with depression may affect the uptake of lifestyle behavioural interventions.
This primary aim of this review was to identify and evaluate the existing evidence for the efficacy or effectiveness of online lifestyle interventions in altering alcohol, physical activity sleep, substance abuse, smoking and/or dietary behaviours for (1) individuals with depressive symptoms, (2) clinically depressed populations or (3) studies discussing the outcomes of depression within a subset of a larger cohort. The analysis examined the key features of interventions that have effectively engaged users, minimised attrition and encouraged users to adhere to the intervention in order to achieve the targeted behavioural change. A secondary aim was to identify the impact of these interventions on depression symptoms.
Methods
This systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO, www.crd.york.ac.uk/PROSPERO, registration number: CRD42017062733) prior to commencement and was conducted in accordance with the PRISMA guidelines. A pre-defined search strategy was applied to identify literature from CINAHL, Cochrane Library, MEDLINE and PsychINFO electronic bibliography databases, and specialist e-Health Journals (Electronic Journal of Health Informatics, Journal of the International Society for Telemedicine and eHealth and Journal of Technology in Human Services). Population search terms included ‘Depression’, ‘Depressive Disorder’ OR ‘Depressive Disorder, Major’ and were combined with intervention terms describing lifestyle interventions ‘Lifestyle Intervention’ OR ‘Risk Reduction Behaviour’ OR ‘Healthy Lifestyle’ OR ‘Sedentary’ or specific lifestyle behaviours ‘Sleep’, ‘Alcohol’, and delivery mode search terms ‘online’ OR ‘web-based’ OR ‘Internet’ OR ‘e-Health’. Search strings used a combination of text and medical subject headings (MESH) and variations on UK and US spellings. Supplementary Appendix 1 contains a full list of the search terms and combinations used for the MEDLINE searches. Searches were limited to studies published in peer reviewed journals with at least an abstract published in English up to June 2017. Potentially eligible abstracts were retrieved and independently assessed against the inclusion criteria by two authors (C.Y. and K.T.), using the online systematic review tool Rayyan (Ouzzani et al., 2016). Conflicts in inclusion or exclusion were resolved by a third author (S.D.).
Criteria for study inclusion
To be eligible for inclusion, articles were required to describe a behavioural or psychosocial lifestyle intervention targeted specifically at a depressed population, a cohort with depressive symptoms or reporting on a subset of a larger cohort where the subset exhibited depression or depressive symptoms. Eligible studies were randomised controlled trials (RCTs) with active control conditions, comprising participants aged 18 years and over, and where the intervention target was a lifestyle behaviour change and did not involve depression treatment. Articles were excluded if there was no reported measure of lifestyle change and/or depression symptoms or if they examined highly specific populations (e.g. pregnant women with postnatal depression) limiting generalizability. Follow-up periods were not part of the inclusion criteria but were assessed in the quality scoring of articles in the subsequent stage of the review.
Full article screening included methodological quality assessment of all included articles using a quality rating checklist developed from the Consolidated Standards of Reporting Trials guidelines for reporting e-Health interventions (e-CONSORT) (Eysenbach, 2011), as well as recommendations from Michie et al. (2017) and Kiluck et al. (2011). A summary of the key components of the quality criteria are shown in Table 1 and the full criteria are in Supplementary Appendix 2. A score was assigned to each included article based on the criteria and aligned to the research questions, with several items rating engagement and adherence measures and reporting. The overall score includes elements of study reporting quality and quality of study design as well as considerations of risk of bias.
Key components of quality criteria.
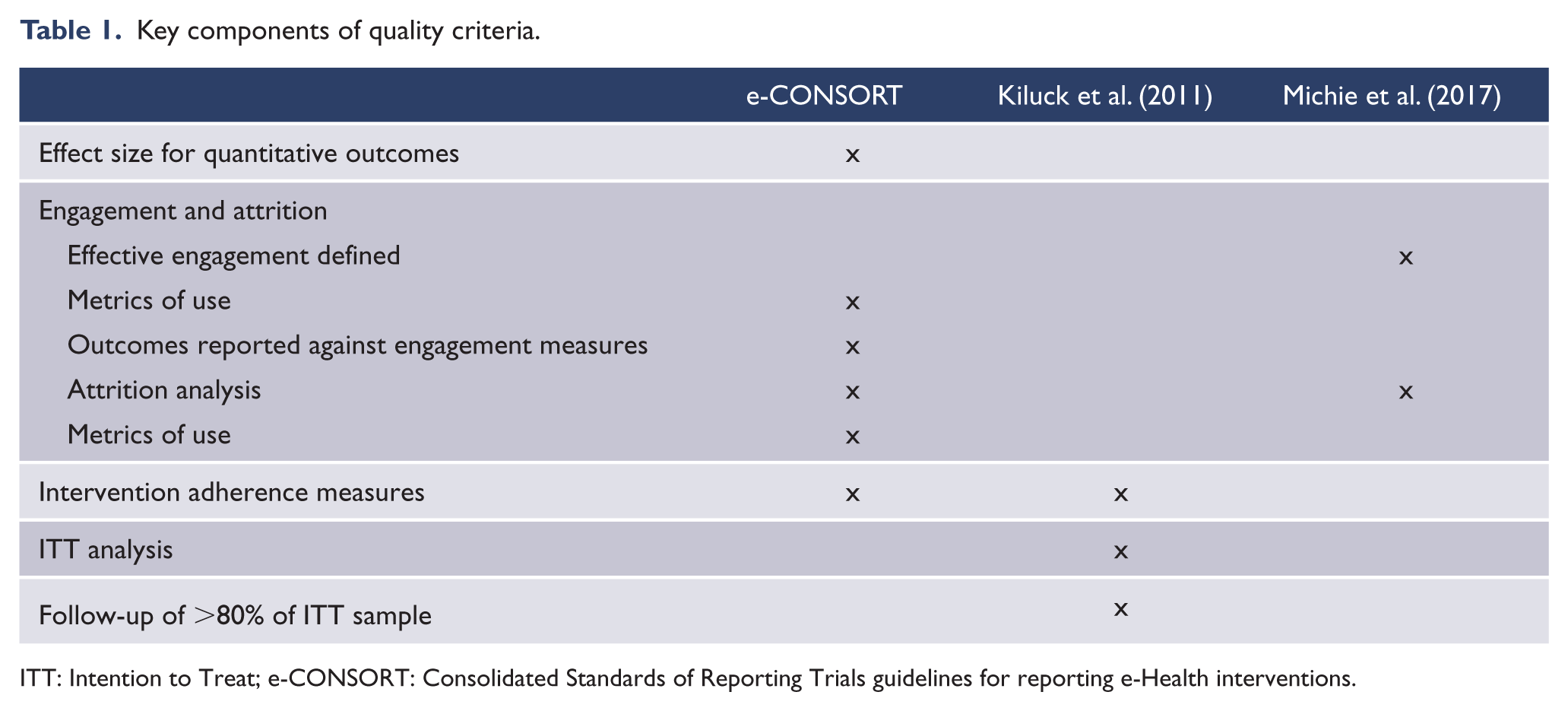
ITT: Intention to Treat; e-CONSORT: Consolidated Standards of Reporting Trials guidelines for reporting e-Health interventions.
Engagement and attrition data were extracted for each study and categorised on a common scale (low <30%, moderate 30–70% and high >70%) summarising features promoting engagement, participation requirements and the metrics employed to measure engagement. Features promoting engagement were derived from intervention design and included content design considerations or any reminders, notifications or interactions with study staff intended to prompt the participant to access the intervention. Participation requirements included any minimum level of activity required of the participant or any specified minimum participation required to progress through the intervention. Behaviour change techniques were examined for each study against The Behaviour Change Technique Taxonomy v1.3 (Michie et al., 2013) and mapped to the intervention features used to implement the technique.
Results
The PRISMA diagram is shown in Figure 1. From 661 initial records, 31 studies were selected for full article screening and 7 studies included in the review.
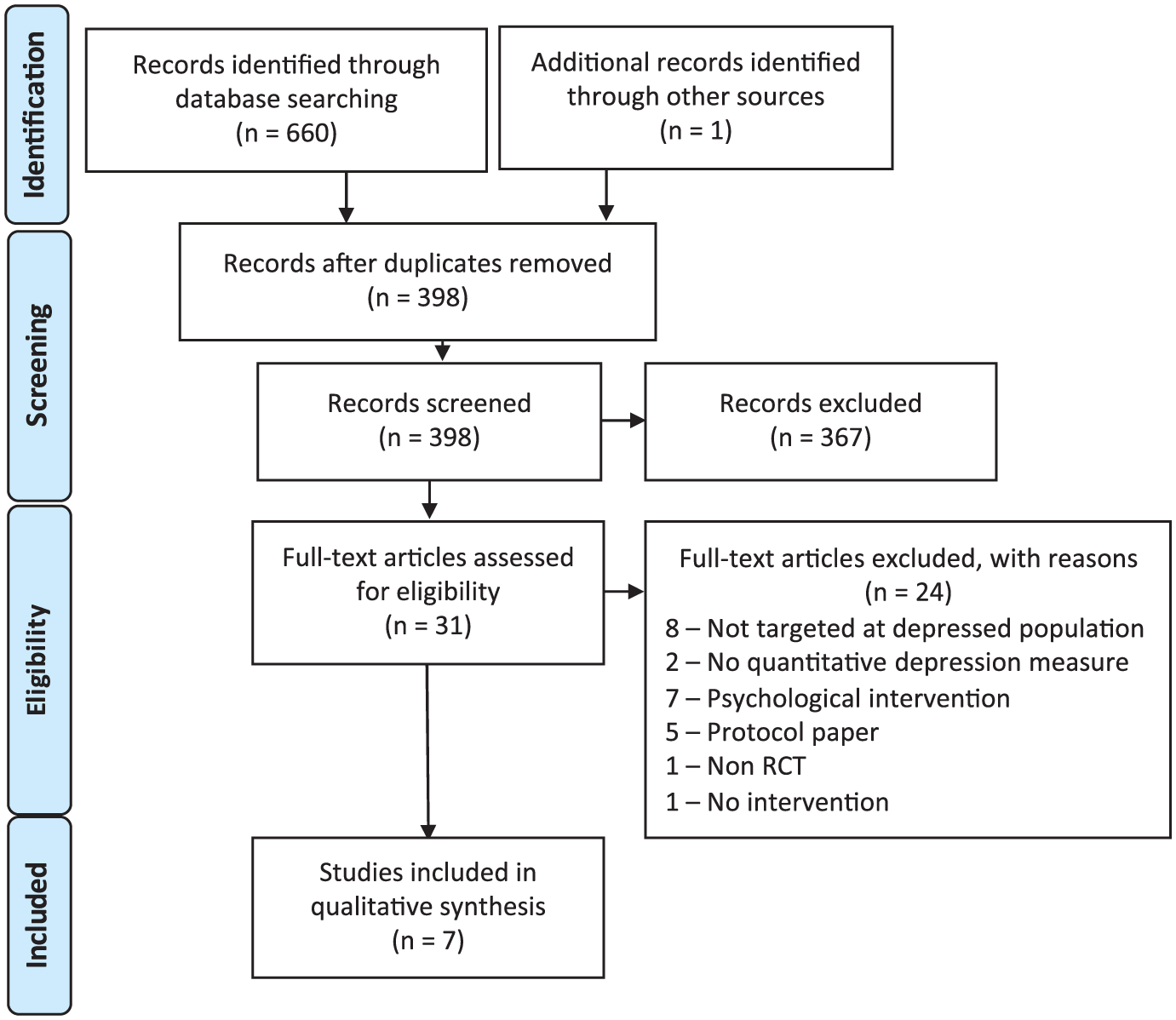
PRISMA flowchart.
Study characteristics
Seven studies were included in the review, encompassing a total of 1964 participants. All of the studies were in adult populations, with three targeting young adults (aged 18–25 years). The interventions were conducted in Australia, Switzerland and the United States, with most employing national recruitment strategies. The behaviour being targeted differed across the seven interventions, spanning five domains: alcohol reduction (Deady et al., 2016; Geisner et al., 2015), improved sleep quality/insomnia reduction (Blom et al., 2015; Christensen et al., 2017), increased physical activity (Mailey et al., 2010), reduced/cessation of substance abuse (Schaub et al., 2012) and smoking cessation (Jones et al., 2015). Five of the studies had been published in the last 2 years (Blom et al., 2015; Christensen et al., 2017; Deady et al., 2016; Geisner et al., 2015; Jones et al., 2015) and all had been published within the last 7 years (Blom et al., 2015; Christensen et al., 2017; Deady et al., 2016; Geisner et al., 2015; Jones et al., 2015; Mailey et al., 2010; Schaub et al., 2012), with the oldest study published in 2010 (Mailey et al., 2010). All of the included studies were Internet-based interventions of differing session lengths, with the majority comprising several modules. The characteristics of each study are summarised in Table 2, including the quality score calculated from the quality criteria.
Summary of study characteristics.
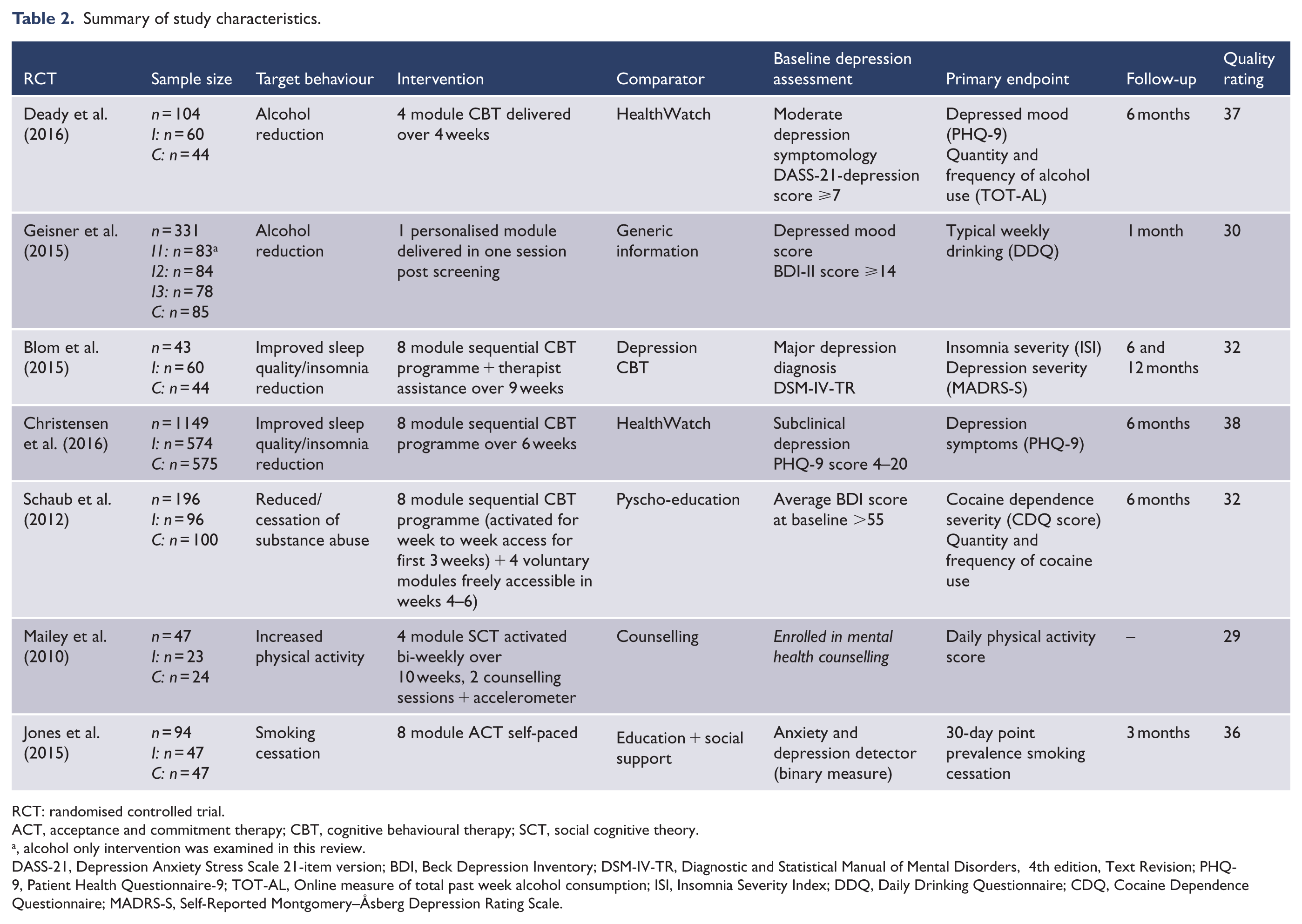
RCT: randomised controlled trial.
ACT, acceptance and commitment therapy; CBT, cognitive behavioural therapy; SCT, social cognitive theory.
, alcohol only intervention was examined in this review.
DASS-21, Depression Anxiety Stress Scale 21-item version; BDI, Beck Depression Inventory; DSM-IV-TR, Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision; PHQ-9, Patient Health Questionnaire-9; TOT-AL, Online measure of total past week alcohol consumption; ISI, Insomnia Severity Index; DDQ, Daily Drinking Questionnaire; CDQ, Cocaine Dependence Questionnaire; MADRS-S, Self-Reported Montgomery–Åsberg Depression Rating Scale.
Changes in target behaviour and depression outcomes
Four studies reported a significant change in the target lifestyle behaviour: lowering alcohol use, improving sleep and increasing physical activity (Table 3). In addition, three studies reported a significant improvement in depression symptom severity, post-intervention. Depression was measured using common, validated psychological measures (Patient Health Questionnaire-9 [PHQ-9], Self-Reported Montgomery–Åsberg Depression Rating Scale [MADRS-S] and Beck Depression Inventory [BDI]) in all included studies except for the smoking cessation study, which employed a binary anxiety and depression detector that had previously been validated by the study authors.
Summary of depression and lifestyle behaviour change outcomes for each study at post-intervention.
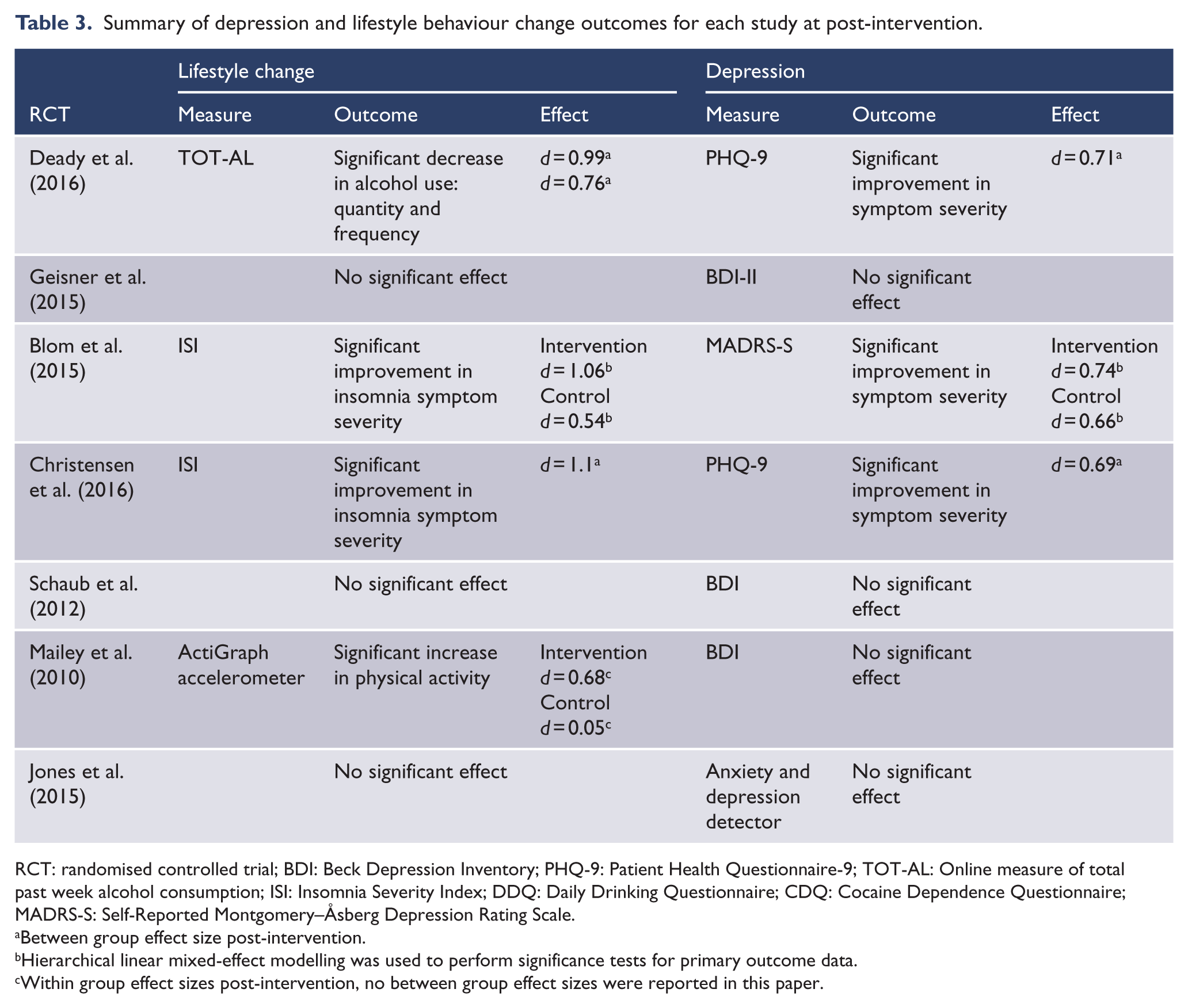
RCT: randomised controlled trial; BDI: Beck Depression Inventory; PHQ-9: Patient Health Questionnaire-9; TOT-AL: Online measure of total past week alcohol consumption; ISI: Insomnia Severity Index; DDQ: Daily Drinking Questionnaire; CDQ: Cocaine Dependence Questionnaire; MADRS-S: Self-Reported Montgomery–Åsberg Depression Rating Scale.
Between group effect size post-intervention.
Hierarchical linear mixed-effect modelling was used to perform significance tests for primary outcome data.
Within group effect sizes post-intervention, no between group effect sizes were reported in this paper.
For the studies reporting significant results in both depression symptoms and lifestyle behaviour change, post-intervention, maintenance of effects results are summarised in Table 4.
Analysis of maintenance of effects for studies reporting significant results in both depression and lifestyle outcomes.
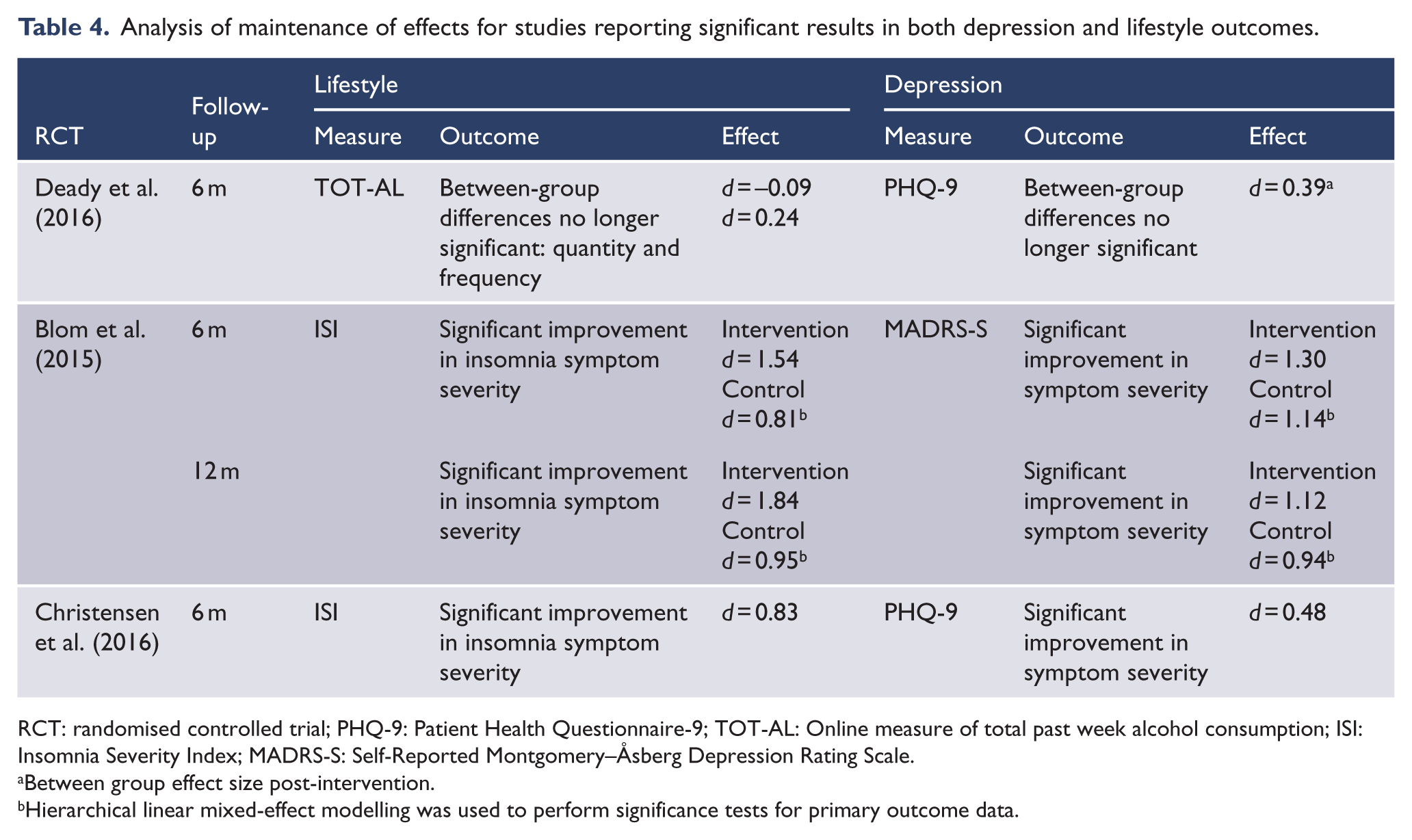
RCT: randomised controlled trial; PHQ-9: Patient Health Questionnaire-9; TOT-AL: Online measure of total past week alcohol consumption; ISI: Insomnia Severity Index; MADRS-S: Self-Reported Montgomery–Åsberg Depression Rating Scale.
Between group effect size post-intervention.
Hierarchical linear mixed-effect modelling was used to perform significance tests for primary outcome data.
Engagement
Effective engagement, as recommended by Michie et al. (2017), was not explicitly defined in any of the studies; however, minimum participation requirements were discussed in most publications; three studies reported low rates of attrition, three moderate and one high. There was no standardised approach to usage measurement with a mix of quantitative and qualitative methods employed. Reporting on ‘Intensity of Use’, as defined by e-CONSORT (Eysenbach, 2011), was limited across the publications with only two out of seven studies reporting quantitative data. Table 5 summarises attrition and engagement measurement in each study, in order of attrition rates and indicates few commonalities between engagement reporting methods and analysis. Only one study reported usage measures against outcomes and concluded that completion of four or more modules was associated with changes target behaviour symptoms and depression (Christensen et al., 2017).
Summary of attrition and engagement analysis for each study.
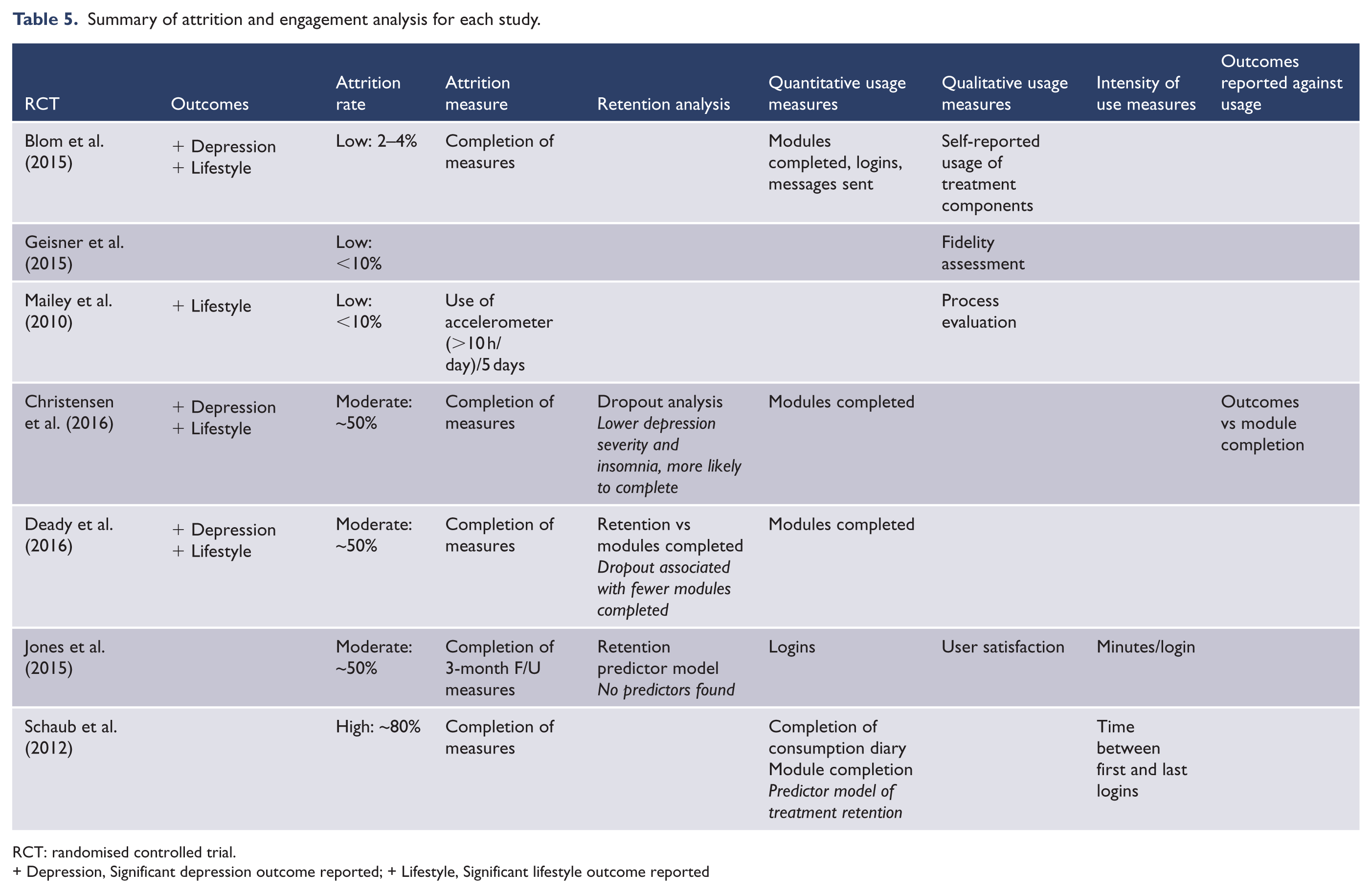
RCT: randomised controlled trial.+ Depression, Significant depression outcome reported; + Lifestyle, Significant lifestyle outcome reported
Intervention features
Table 6 summarises the intervention features, in order of attrition rates, and the requirements of completion for participants. The interventions that were successful in achieving behaviour change and associated improvements in depression symptoms required regular participation, completion of modules and exercises on a weekly basis and were of moderate content length, between four and eight modules. Low attrition rates were seen in interventions that also included therapist assistance or counselling or had lower participation requirements. Interventions employing email and text notifications and follow-up phone calls achieved low to moderate attrition rates. The interventions that employed a greater number of behaviour change techniques and required consistent interactive exercises achieved significant outcomes in both the target lifestyle behaviour change and depression symptoms.
Summary of intervention features promoting engagement and adherence against attrition data.
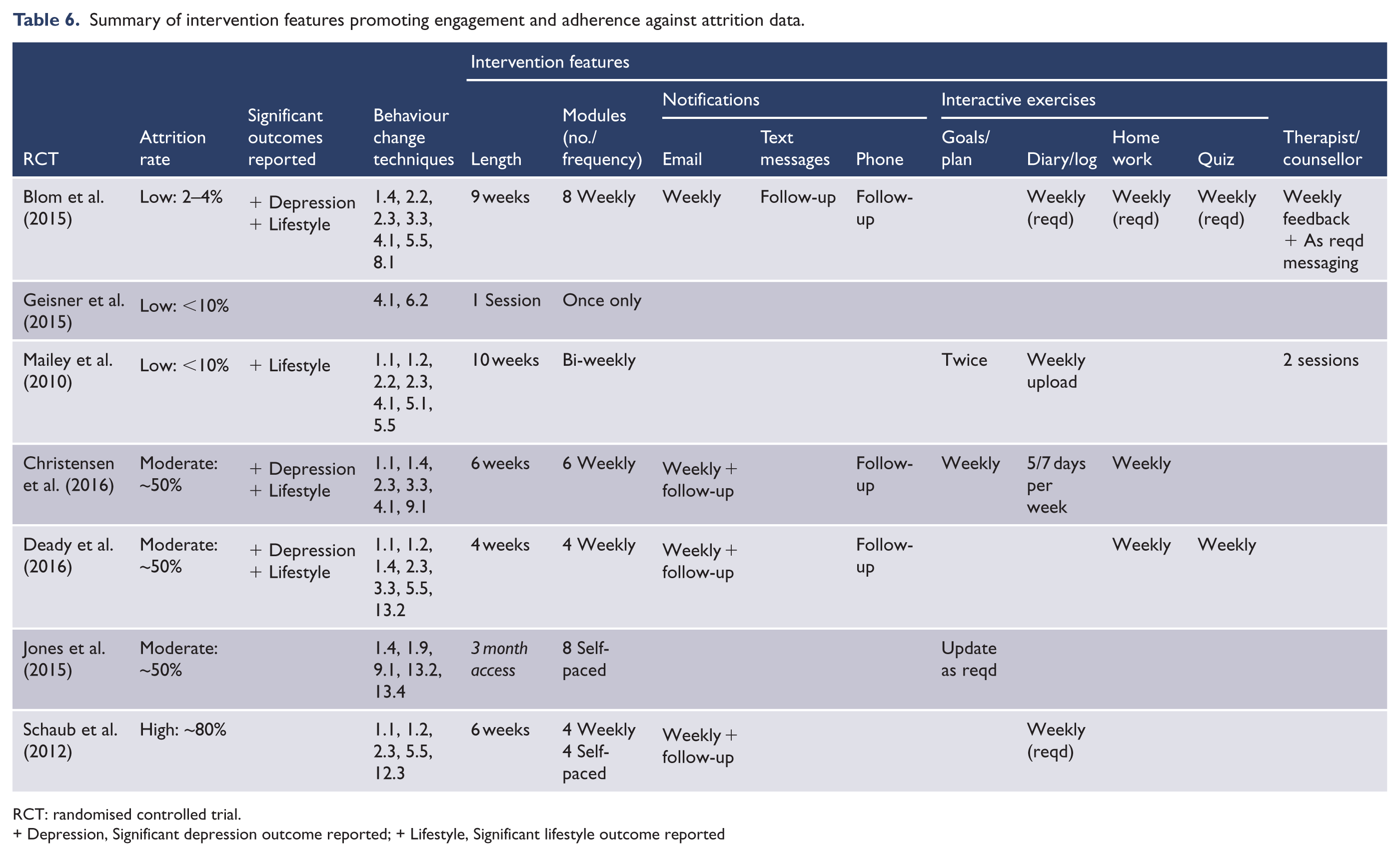
RCT: randomised controlled trial.+ Depression, Significant depression outcome reported; + Lifestyle, Significant lifestyle outcome reported
Behaviour change techniques implementation
Table 7 summarises the implementation of behaviour change technique (BCT) across all studies mapped to the intervention features employed and ranked by the number of studies utilising the BCT. Self-monitoring and providing information on the behaviour were the two most commonly used techniques. Self-monitoring was commonly implemented through interactive exercises such as diaries and logs completed online. Information on health consequences was delivered through module content and a key component in most of the interventions.
Summary of intervention features by behaviour change techniques.
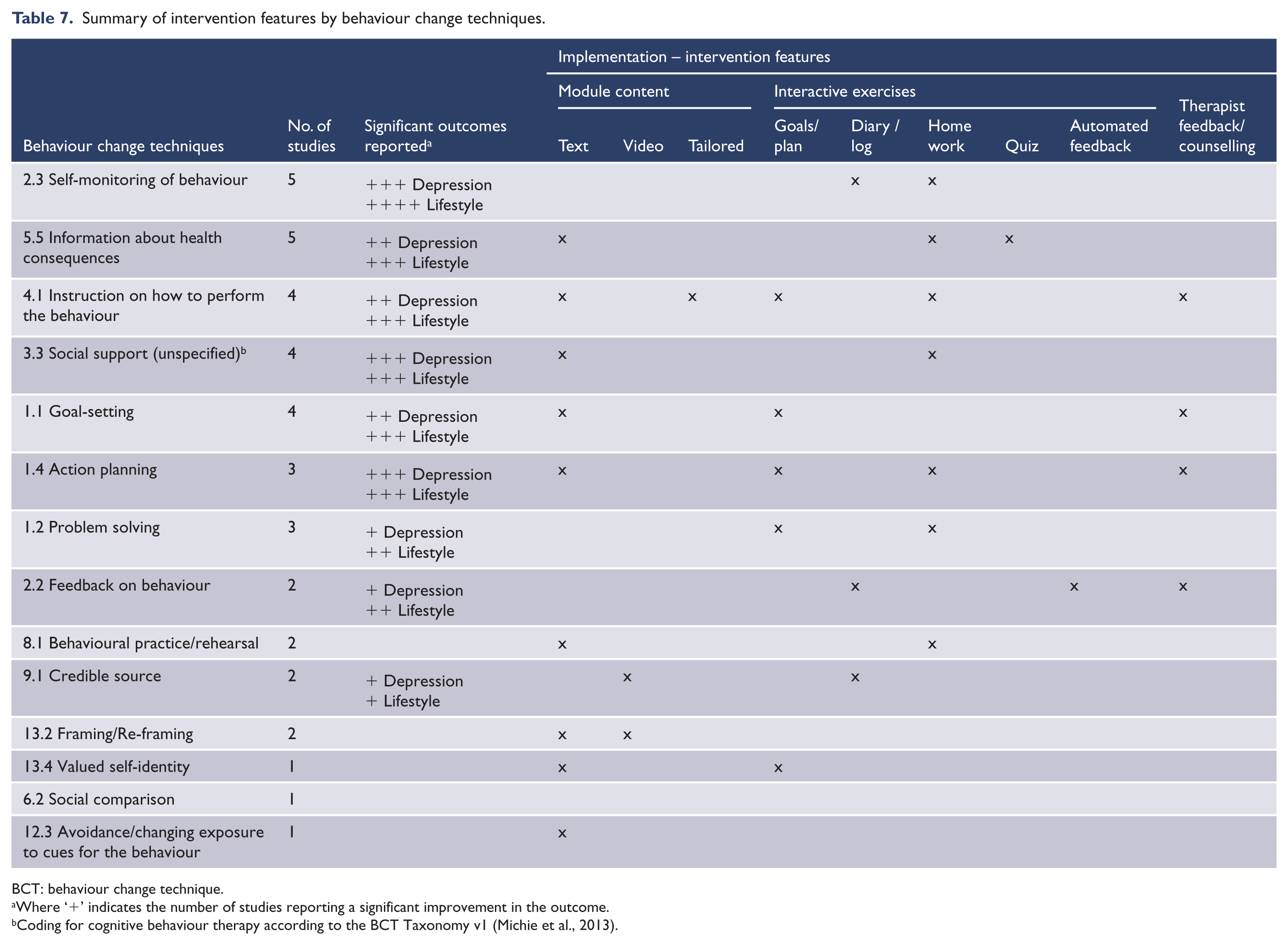
BCT: behaviour change technique.
Where ‘+’ indicates the number of studies reporting a significant improvement in the outcome.
Coding for cognitive behaviour therapy according to the BCT Taxonomy v1 (Michie et al., 2013).
Discussion
The aim of this study was to investigate what evidence exists for online lifestyle interventions in depressed populations and which interventions were successful in achieving lifestyle behaviour change. Of particular interest were the techniques employed to engage participants, the behaviour change techniques utilised and how these were implemented in the interventions to achieve the targeted lifestyle change. Although the seven studies were of varying designs, durations, sample sizes and study qualities, some provide promise that online interventions can be successful in achieving the targeted behavioural change and associated reduction in depressive symptoms (Blom et al., 2015; Christensen et al., 2017; Deady et al., 2016). No studies altered depressive symptoms without changing the target behaviour, suggesting that targeting lifestyle behaviours is a valid approach for achieving changes in depression symptoms.
Lifestyle medicine as a treatment option for depression is an emerging area of interest (Sarris et al., 2014). Whilst other reviews have discussed online lifestyle interventions, and examined which features or designs are effective in achieving behavioural change (Brouwer et al., 2011; Evers et al., 2003; Maher et al., 2014; Norman et al., 2007; Van den Berg et al., 2007), none have explicitly examined these kinds of interventions in depressed populations. This review indicates that there are published data on a small number of lifestyle interventions for depressed populations, and that those requiring consistent but moderate levels of participation and employing a variety of behaviour change techniques, implemented through interactive exercises, achieved results in both the target lifestyle behaviour and associated depression outcomes.
The studies targeted a range of lifestyle behaviours that were deemed important behavioural targets for treating depression. Significant improvement in the target behaviour and significant improvement in depressive symptoms was achieved in one intervention targeting alcohol reduction (Deady et al., 2016) and both interventions targeting insomnia (Blom et al., 2015; Christensen et al., 2017). Each of these interventions required the participants to consistently perform tasks, aligned to several behaviour change techniques and prompted engagement through email notifications (Blom et al., 2015; Christensen et al., 2017; Deady et al., 2016) and some phone follow-up (Blom et al., 2015; Christensen et al., 2017). Self-monitoring, action planning and social support were behaviour change techniques common to each of these interventions, which were all CBT-based. Interestingly, the Mailey et al. (2010) intervention increased the targeted physical activity behaviour but did not report a significant improvement in depressive scores. However, differential patterns of association were seen in the intervention group between changes in physical activity and depression that were significant and in the hypothesised theoretical direction (Mailey et al., 2010). The lack of a baseline depression requirement and small sample size may have impacted the overall intervention outcome in this case.
The studies where the target behaviours were not changed were also unsuccessful in altering depressive symptoms (Geisner et al., 2015; Jones et al., 2015; Schaub et al., 2012). This may be because substance abuse and smoking cessation are more resistant to change in a depressed population (Jones et al., 2015; Schaub et al., 2012), or perhaps, more likely, the lack of change was due to deficits in elements of the intervention design and small sample sizes. In support of this, while no significant results were achieved, Jones et al. (2015) reported positive trends in both depressive symptoms and smoking cessation in their analysis.
The post-intervention effect sizes reported by those studies achieving significant improvement in depression symptoms were substantial. Christensen et al. (2017) note their effect size of 0.69 is much larger than those reported in the literature for online psychological interventions for depression or major depressive disorder and approached the effect size achieved in face-to-face transdiagnostic interventions specifically targeting depression (Christensen et al., 2017). The effect sizes reported by Deady et al. (2016) and Blom et al. (2015) post-intervention were also approaching this magnitude.
Engagement and adherence
Analysis of engagement and adherence may help to evaluate any exposure or dose–response relationships; however, the limited reporting of usage vs outcomes analysis in the included publications made this difficult in the current review. The study by Christensen et al. (2017) was the only study that reported usage vs outcomes. Their analysis was on number of completed modules and showed significant effects relative to control for users who completed four or more of the prescribed modules. Since low motivation is a characteristic symptom of depression, knowing if users dropped out due to low motivation or simply because the intervention measures were onerous would help guide future designs of interventions targeting depressed populations.
All of the studies analysed were replications of treatments that had been tested in a clinical setting, and many required the users to participate in the intervention in the same manner they would if they were attended appointments in a clinical setting. The two sleep interventions, and the substance abuse intervention, were all sequentially delivered modules of CBT that required participants to consume the content in a prescribed manner dependent on either a set schedule or prior completion of a task. While there were no obvious patterns of this structured approach contributing to attrition rates, restricted access limits the amount of content a user can progress through when they have time and willingness to use the intervention. Given that flexibility of access of online interventions is one of the advantages of this mode of delivery, increasing the flexibility of intervention design might be worth considering in future interventions, as long as it does not compromise the staged introduction of techniques and strategies inherent in CBT packages. Deady et al. (2016) highlight the ability to sample from all modules in their intervention may have contributed to the positive results achieved by their intervention, despite the lower number of participants reported as completing all modules. They note that it is difficult to distinguish whether attrition in their study was due to dissatisfaction vs sufficient satisfaction, or having sampled enough information to meet the user’s needs. Analysis of sampling behaviour as users interact with an online intervention would provide data to help define effective engagement.
Attrition was measured in each study by the completion of required measures in the form of questionnaires. As Schaub et al. (2012) report, many participants complete the prescribed intervention activities but ‘simply closed their Internet browsers’ when required to complete questionnaires. This again highlights the necessity of analysing usage vs outcomes in order to really assess how users interacted with the intervention and what patterns of interaction, if any, are associated with positive outcomes. Furthermore, this suggests that simple measures of minutes spent online or at each login might not be an accurate measurement of intensity of use. Retention predictor models were reported by Christensen et al. (2017), and Schaub et al. (2012) in comparing attrition rates with baseline characteristics, and Deady et al. (2016) reported retention against number of modules completed. While these analyses help understand which users need to be targeted in order to increase engagement, and general engagement patterns, they do not necessarily assist with understanding the design features required to improve retention.
Several studies used qualitative methods to measure user satisfaction with the intervention, however most suffered from low participation rates. These methods are useful in highlighting design features users liked or disliked but are often only completed by those who have remained engaged in the intervention.
Behaviour change
Despite the different target lifestyle behaviours of the analysed studies, there were several common behaviour change techniques employed across the interventions and similar ways of implementation of these techniques. Self-monitoring of the behaviour was the most popular technique and employed by all the interventions that achieved significant improvements in both the lifestyle behaviour target and depression symptoms. Self-monitoring is aimed at improving a person’s self-regulatory skills, which is seen as key construct in achieving behaviour change according to social cognitive theory (Middleton et al., 2013). In the studies reviewed, self-monitoring activities involved either the completion of a diary documenting the lifestyle behaviour over a retrospective time period or an assigned homework activity related to the behaviour or behaviour change that required the user to report on or reflect on their performance.
Information about the behaviour and its health consequences also featured prominently in the interventions reviewed and particularly those that achieved significant outcomes. This is another key construct in social cognitive theory; that in order to initiate behaviour change, a person needs awareness of how their behaviours affect their health. This technique was implemented through the delivery of module content and also reinforced via online quizzes or homework exercises in some of the interventions (Blom et al., 2015; Deady et al., 2016).
Some techniques were common across several studies but not all of these achieved significant outcomes. Instruction on how to perform the technique, was employed by both sleep studies that reported significant outcomes. Goal setting, was used by Deady et al. (2016) and Mailey et al. (2010) to achieve reduction in alcohol use and increased physical activity, respectively.
Of the techniques employed and ways of implementation, none of the studies explicitly discussed which activities were best received or thought to contribute to behaviour change. In most cases, the implementation techniques are driven by the theoretical framework the intervention is based on, as opposed to the target audience. Jones et al. (2015) discussed the theoretical approach used in their intervention and how it might be beneficial for depressed populations in their analysis, but not specific intervention features. In addition, their study was a post hoc analysis of a depressed subset and not an intervention specifically designed for depressed populations.
Limitations
The focus on engagement and adherence measures in the quality criteria resulted in a wide range of quality scores. The disparity of measurement and reporting of engagement and adherence in these kinds of interventions makes the comparison of outcomes and the identification of design elements that promote engagement difficult. Many important lifestyle behaviours associated with depression were not captured in the available studies, including diet, increasing social networks and activity scheduling. It was not possible to compute the relative weighting of these lifestyle factors in terms of impact on depression outcomes.
Since lifestyle medicine is a fairly new proposition for the treatment of depression, there were few online examples of these kinds of treatments targeted for this population. It is promising however that, as shown in the PRISMA flowchart, during the course of the systematic search, several protocol design papers were also retrieved, highlighting that more lifestyle interventions targeted at depressed populations are currently underway.
Recommendations for future research
In order for online lifestyle interventions for depression to be supported as viable treatment options for improving depressive symptoms, comparison of the lifestyle intervention with online interventions that have demonstrated efficacy for depression would be optimal. This approach was employed by Blom et al. (2015) in their comparison of online CBT for insomnia vs an online CBT intervention for depression; however, this study did not explicitly report on between group effect sizes and the statistical analysis was underpowered due to the low sample size.
In designing future interventions targeting depressed populations, it is important to consider the levels of participation required and ways to actively encourage participation. Intervention designs that employ several behaviour change techniques, particularly self-monitoring and action planning, and that require consistent participation in interactive exercises over moderate intervention lengths appear to be more successful in achieving behaviour change in this population. Prompting participation with regular communication, which can be automated to facilitate scalability, and minimising participant burden, by limiting the number and length of measures required to be completed, are also advantageous for interventions targeting this population.
Conclusion
The results of this review highlight the potential of online lifestyle interventions as adjunctive treatments for depression, and the possibility of achieving significant improvement in depressive symptoms when targeting lifestyle behaviour change. While only a limited number of studies have been published to date, the systematic search results indicate this is a growing area of interest. Further analysis of engagement patterns will give a better understanding of what intervention designs can assist more users to achieve significant lifestyle behaviour changes and associated improvements in their depression symptoms can be achieved.
Supplemental Material
Efficacy_of_Online_Lifestyle_Interventions_targeting_lifestyle_behaviour_change_in_Depressed_Populations_Young_2018_v1.0_Appendix_1 – Supplemental material for Efficacy of online lifestyle interventions targeting lifestyle behaviour change in depressed populations: A systematic review
Supplemental material, Efficacy_of_Online_Lifestyle_Interventions_targeting_lifestyle_behaviour_change_in_Depressed_Populations_Young_2018_v1.0_Appendix_1 for Efficacy of online lifestyle interventions targeting lifestyle behaviour change in depressed populations: A systematic review by Claire L Young, Karen Trapani, Samantha Dawson, Adrienne O’Neil, Frances Kay-Lambkin, Michael Berk and Felice N Jacka in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Efficacy_of_Online_Lifestyle_Interventions_targeting_lifestyle_behaviour_change_in_Depressed_Populations_Young_2018_v1.0_Appendix_2 – Supplemental material for Efficacy of online lifestyle interventions targeting lifestyle behaviour change in depressed populations: A systematic review
Supplemental material, Efficacy_of_Online_Lifestyle_Interventions_targeting_lifestyle_behaviour_change_in_Depressed_Populations_Young_2018_v1.0_Appendix_2 for Efficacy of online lifestyle interventions targeting lifestyle behaviour change in depressed populations: A systematic review by Claire L Young, Karen Trapani, Samantha Dawson, Adrienne O’Neil, Frances Kay-Lambkin, Michael Berk and Felice N Jacka in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
Systematic review registration: PROSPERO CRD42017062733.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
A.O. is supported by a Future Leader Fellowship (#101160) from the Heart Foundation, Australia. F.K.L. is supported by a NHMRC Senior Research Fellowship (#1110371). M.B. is supported by a NHMRC Senior Principal Research Fellowship (APP1059660). F.N.J. is supported by an NHMRC Career Development Fellowship (2) (#1108125).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.