
Abstract
The DSM-IV diagnosis of major depressive episode (MDE) requires the presence of at least one of the two key symptoms of depressed mood and loss of interest, together with at least three associated symptoms to give a total of five or more of nine depressive symptoms [1]. This categorical, polythetic view of depression assumes, first, that a diagnostic threshold definitely exists and, second, that all depressive symptoms, with the exception of depressed mood and loss of interest, should be equally weighted in determining the diagnosis. This study tests the empirical evidence behind these two assumptions.
Choosing a symptom threshold to diagnose depression is a contentious topic [2, 3]. It is commonly reported that the number of depressive symptoms is positively related to measures of disability and impairment [4–6]. However, the exact nature of this relationship remains unclear. The implicit assumption behind the DSM-IV threshold of five depressive symptoms is that there is something qualitatively different between those who have four symptoms and those who have five symptoms and that this difference is greater than at any other point along the continuum. However, the extent to which the rise from four to five depressive symptoms is associated with a greater increase in impairment than at any other point along the continuum is not known. Comparing the gradients of increases in impairment with each additional depressive symptom may help to derive an empirically based threshold for the diagnosis of MDE.
In arriving at a diagnosis of DSM-IV MDE the two symptoms of depressed mood and loss of interest or pleasure are considered core symptoms. Without endorsing one of these core symptoms a diagnosis of MDE, according to DSM-IV, is not warranted. However, the assumption in DSM-IV is that the remaining seven non-core symptoms are of equal importance in determining a diagnosis of MDE. It is possible that certain symptoms may be more significant predictors of impairment than others. If such a situation exists, the degree of impairment is not best explained by a simple additive model in which each symptom contributes equally to the ascertainment of MDE. Instead, a model in which certain criteria receive more weight in the diagnosis may be warranted [7, 8].
The current study investigates, using data from the Australian National Survey of Mental Health and Wellbeing, whether a clear threshold can be found in the number of depressive symptoms and whether each of the seven non-core symptoms of DSM-IV MDE makes a similar contribution to impairment. Analysis of a large epidemiological study of mental disorders in the general population allows for the relationship between depressive symptoms and impairment to be investigated across the full spectrum of symptomatology.
Methods
Sample and diagnostic interview
The data were obtained from the Australian National Survey of Mental Health and Wellbeing, a nationwide household survey of adults. The details of the survey methods can be found elsewhere [9]. The prevalence of mental disorders according to DSM-IV diagnostic rules was determined through the Composite International Diagnostic Interview (CIDI) [10], for 10 641 persons aged 18 and above. The interview was administered from a laptop computer by trained interviewers from the Australian Bureau of Statistics, a statutory body responsible for conducting such surveys using ethical protocols. The sample represents 78.1% of those approached through a stratified multistage sampling process. The CIDI contains questions that address each of the nine DSM-IV MDE criterion A symptoms. While many of the nine symptoms are assessed through a number of individual questions and are thus more accurately called ‘symptom clusters’, for the purposes of the current study each of the nine will be referred to as a ‘symptom’ of MDE. Those who endorsed ‘depressed mood’ (n = 598), or ‘loss of interest’ (n = 604), or both (n = 935) nearly every day for at least 2 weeks in the past 12 months were assessed for the presence of the other seven depressive symptoms. This subsample (n = 2137) was used in all analyses.
Measures of impairment
Impairment was quantified using four measures: the mental component summary scale of the SF-12 Health Survey [11], the Brief Disability Questionnaire [12], the number of disability days, and the number of health professional consultations. Disability days were made up of a combination of ‘days out of role’ and ‘days cut back’. The days out of role and days cut back are, respectively, the number of days in the past 4 weeks an individual has been unable to perform, or has had to cut down on, their normal activities because of their health [13]. The summary measure, disability days, was created by summing the days out of role and 0.4 times the days cut back [14]. Health professional consultations represented the number of times the respondent had consulted a health professional for any reason in the 4 weeks prior to the interview. Given that the respondent could attribute these impairment measures to any health problems, including depression, the presence of other mental and physical problems were included as covariates in all the regression models.
Statistical analyses
To test whether there is a distinct threshold in the relationship between the number of depressive symptoms and impairment, multivariate linear regression analyses were carried out in which the number of symptoms (ranging from one to nine) predicted impairment. The gradients of increases in impairment from one through nine symptoms were determined by fitting polynomial contrast coefficients to test for linear, quadratic, and cubic trends. A significant linear trend alone indicates that each additional symptom adds a similar amount of impairment and challenges the existence of a distinct diagnostic threshold. Significant quadratic and cubic trends indicate that the rate of changes in impairment is not constant with each additional symptom. Significant linear, together with significant quadratic and/or cubic trends indicate a shift in the increasing rate of impairment at one or more points along the continuum. The exact position of this shift may provide one method of establishing an empirically based diagnostic threshold. These relationships are graphically represented in Figure 1. An adjusted significance level of α = 0.013 (0.05/4) was used to test for significant linear, quadratic and cubic trends.
Potential trends in the relationship between the number of depressive symptoms (x-axis) and measures of impairment (y-axis).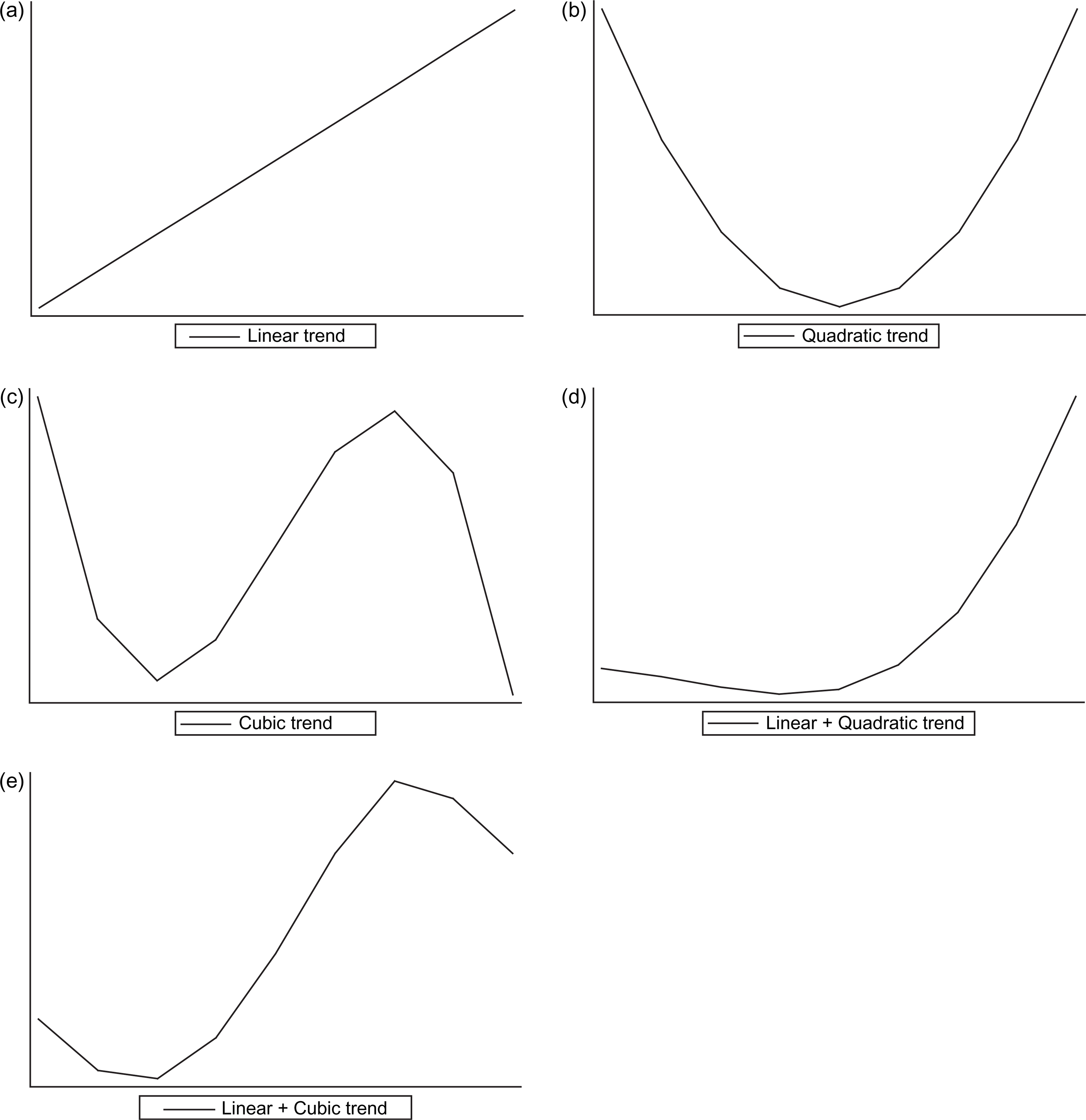
To test for the assumption of equality among the seven non-core symptoms of MDE a separate series of multivariate linear regression analyses was carried out in which all seven symptoms together predicted each measure of impairment. The resulting beta weights from these multivariate regression models provide an indication of the strength of the relationship between individual symptoms and impairment, controlling for the presence of other symptoms. Using a conservative α of 0.01 the results demonstrate which symptoms make a unique contribution to impairment that is not explained by the other symptoms.
The sample was weighted to conform to the age and sex distribution of the Australian population and to account for the probability of selection. All linear regression models analysed in the SUDAAN software package [15] controlled for age, gender, and the presence of other physical disorders (asthma, chronic bronchitis, anaemia, high blood pressure, heart trouble, arthritis, kidney disease, diabetes, cancer, stomach or duodenal ulcer, chronic gall bladder or liver trouble, hernia or rupture) and mental disorders (panic disorder, agoraphobia, social phobia, generalized anxiety disorder, obsessive–compulsive disorder, post-traumatic stress disorder, dysthymia, bipolar disorder, drug and alcohol use disorder).
Results
The relationship between the number of depressive symptoms and each of the four measures of impairment is shown in Figure 2. As can be seen in Figure 2 all four measures of impairment increase in a purely linear fashion as the number of depressive symptoms increases. This is confirmed by statistically significant linear trends together with non-significant quadratic and cubic trends.
Empirical relationship between the number of depressive symptoms and four measures of impairment.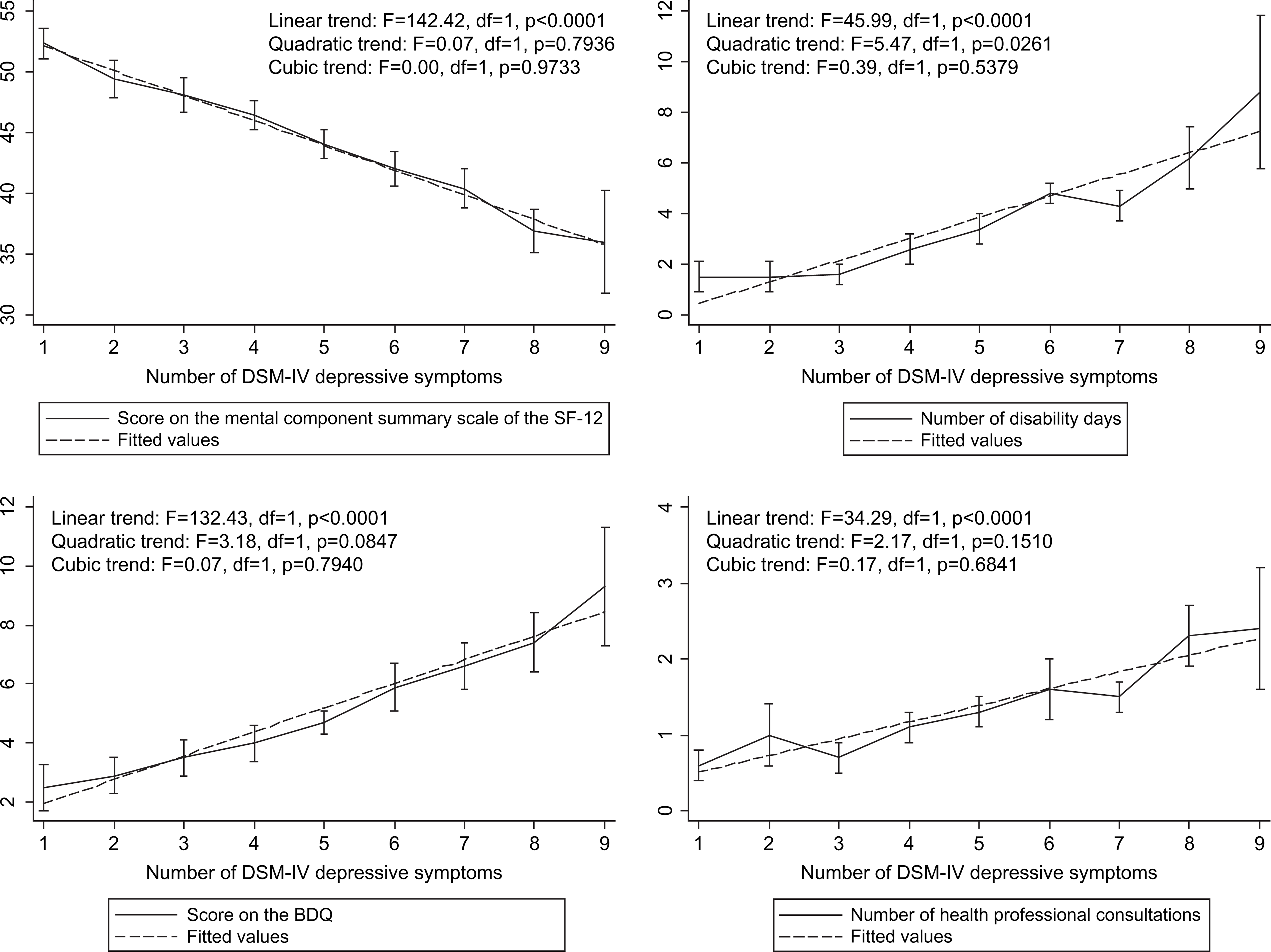
The multivariate relationship between the type of depressive symptom and each of the four measures of impairment is shown in Table 1. The beta weights represent the standardized contribution that each symptom makes to impairment, independent of all other symptoms. As can be seen in Table 1, the symptom ‘loss of energy’ is independently related to all four measures of impairment. In addition, the symptoms ‘sleep problems’ and ‘psychomotor disturbance’ are significantly related to three out of the four measures of impairment, and the symptoms ‘worthlessness or guilt’, ‘trouble thinking’ and ‘thoughts of death’ are significantly related to one out of the four measures of impairment.
multivariate linear regression analyses examining the independent relationship of depressive symptoms to four measures of impairment
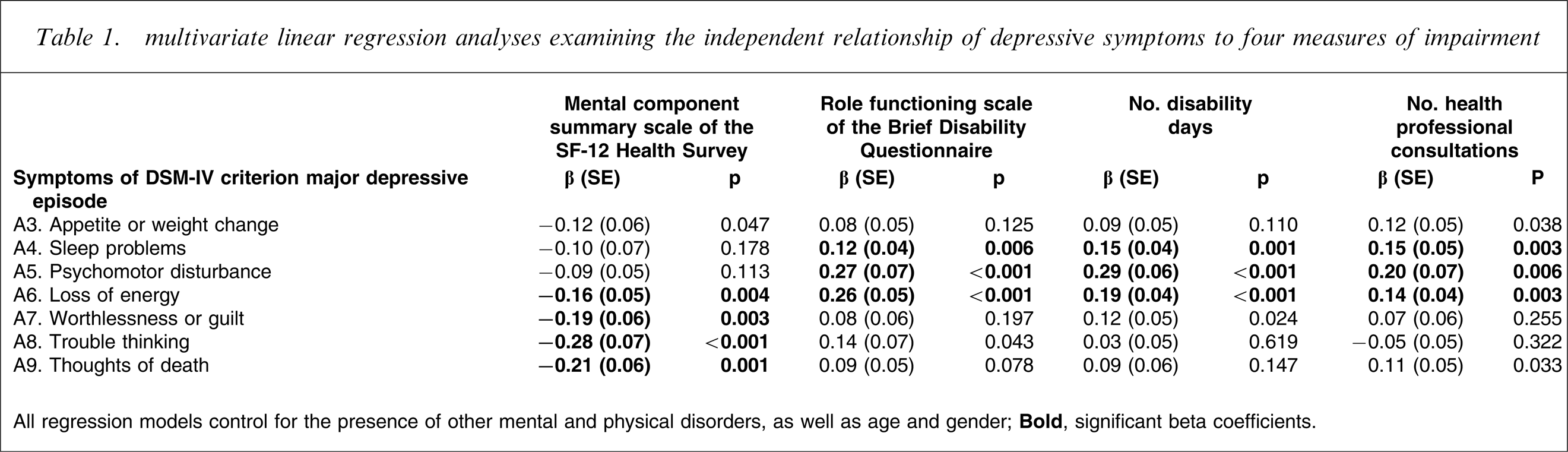
All regression models control for the presence of other mental and physical disorders, as well as age and gender.
Discussion
The current study has demonstrated that significant linear trends in the absence of significant quadratic and cubic trends exist in the relationship between the number of depressive symptoms and four independent measures of functional impairment. To the extent that functional impairment is considered an external validator of mental disorder diagnosis, these findings suggest that DSM-IV MDE does not represent a distinct diagnostic category with an empirically supported threshold of five out of nine symptoms. These findings are in accordance with previous studies that have failed to identify a clear symptom cut-off for the diagnosis of MDE [4, 5]. Furthermore, a number of studies using statistical techniques specifically designed to distinguish, at the latent level, between categorical and dimensional explanations of depression have failed to identify distinct groups of ‘depressed’ individuals [16–18].
The results of the current study lend support to the recent movement away from strictly categorical models of mental disorders, toward models that take into consideration the dimensional nature of psychopathology [19]. While the current study provides evidence in support of the dimensional nature of depression, the potential complexity of dimensional models of mental disorders means that their practical incorporation into future revisions of the classification systems and their utility in day-to-day clinical practice would need to be carefully considered. Kessler et al. have argued for the recognition that treating mild cases (i.e. cases that fall below the traditional thresholds for diagnosis) may be beneficial in the long term because this may prevent a substantial number of future serious cases [2].
The analyses examining the number of symptoms do not take into account the fact that different people with the same total number of symptoms may have endorsed completely different types of symptoms. When the specific types of symptoms are considered, important differences emerge. The results of the current study demonstrate that the non-core symptoms of ‘sleep problems’, ‘psychomotor disturbance’, and particularly ‘loss of energy’ are all significantly and independently related to impairment when the contribution of all other symptoms is taken into account. This means that endorsing any of these symptoms alone can impact on impairment (assuming either of the core symptoms of ‘depressed mood’ or ‘loss of interest’ is also endorsed). Thus, all symptoms are not equally associated with impairment.
These relationships do not reflect differences magnified to statistical significance by the large sample. Rather, the relationships are clear and substantial. In the subsample of respondents who endorsed at least one key symptom (n = 2137), the three independent symptoms of ‘sleep problems’, ‘psychomotor disturbance’, and ‘loss of energy’ (together with the covariates) explained 23% of the variance in scores on the Brief Disability Questionnaire, yet the model containing all seven non-core symptoms merely explained an additional 1% of the variance. Similarly, for the remaining three impairment measures, the addition of all seven non-core symptoms added only 2.2% (SF-12), 0.6% (disability days) and 0.7% (health professional consultations) of the variance over and above the three significant symptoms. When the entire sample (n = 10 641) is considered, and the key symptoms included, the four non-significant independent symptoms still add little to the variance explained by the three significant independent symptoms.
The differential associative relationship of the symptoms is also evident in the mean disability days and number of health consultations. In our data, those who endorsed the three most consistently significant symptoms (‘sleep problems’, ‘psychomotor disturbance’, ‘loss of energy’) in the absence of the remaining four symptoms averaged 1.5 disability days and two health consultations per month, while those who endorsed all four non-significant symptoms in the absence of the three significant symptoms averaged 0.8 disability days and 0.6 health consultations. Thus, the three significant symptoms are associated with twice as much impairment as the four non-significant symptoms. This finding may help to explain why impairment in sub-threshold cases is often substantial [20–22]. The relationship between specific symptoms and measures of impairment is consistent with past research. In the Dutch epidemiological survey of mental disorders ten Have et al. demonstrated a significant independent relationship between ‘loss of energy’ and consultation with health professionals, both in the primary care and specialist care sectors [23]. The role of psychomotor disturbance in treatment seeking and the significant relationship between psychomotor function and severity of depression attests to the critical role of psychomotor function in the diagnosis of MDE [24, 25].
The present results warrant further research on the relative importance of depressive symptoms. Although the current DSM-IV diagnosis requires one of the two core symptoms [1], their relative importance compared to the subsequent symptoms in terms of impairment is not known. In the current study, only those who endorsed at least one of the core symptoms were asked the remaining seven non-core symptom questions. Thus, the analysis was restricted to seven out of the nine symptoms of depression. Future studies should obtain data in which the presence of all the symptoms is determined for all respondents to establish the relative importance of all nine symptoms. Furthermore, investigating the differential impact of the subcomponents of individual symptoms (e.g. ‘insomnia’ versus ‘hypersomnia’ under ‘sleep problems’) may also be valuable in future studies.
The differential impact of symptoms on impairment suggests that counting symptoms alone may not give clear guidance regarding levels of impairment. Weightings of the different symptoms may be established by averaging the regression coefficients obtained by different impairment measures, assuming the different impairment measures are equal indicators of impairment. More research is required to determine the weightings of the two key symptoms and to examine the consistency of the present results across different populations. Once the weightings are established a weighted depression score (total of the weighted symptoms) can be produced. This weighted depression score would better reflect one's impairment level than the simple addition of the number of symptoms. However, the difficulties brought about by introducing complex weighting algorithms such as those suggested require careful consideration (see [8] for a discussion of the issues).
In conclusion the current study aimed to empirically examine two assumptions in the diagnosis of DSM-IV MDE. The assumption that MDE is a distinct diagnostic entity with a definitive boundary at five symptoms lacked strong empirical support. Furthermore, the assumption that all symptoms of depression are equal, at least in terms of their association with external measures of impairment, also lacked empirical support. Further research is needed to investigate the utility and applicability of diagnostic criteria that take into account the dimensionality of depression, while at the same time appreciating the differential cumulative impact of different depressive symptoms.