
Abstract
Background:
It is unclear which specific symptoms of post-traumatic stress disorder are related to poor perceived quality of life.
Objective:
To investigate the influence of post-traumatic stress disorder symptomatology on quality of life in traumatic injury survivors.
Method:
Traumatic injury survivors completed questionnaires on post-traumatic stress disorder symptomatology and quality of life at 3 months (n = 987), 12 months (n = 862), 24 months (n = 830) and 6 years (n = 613) post trauma.
Results:
Low quality of life was reported by 14.5% of injury survivors at 3 months and 8% at 6 years post event. The post-traumatic stress disorder symptom clusters that contributed most to poor perceived quality of life were numbing and arousal, the individual symptoms that contributed most were anger, hypervigilance and restricted affect.
Conclusions:
There was variability in the quality of life of traumatic injury survivors in the 6 years following trauma and a consistent proportion reported low quality of life. Early intervention to reduce anger, hypervigilance and restricted affect symptoms may provide a means to improving the quality of life of traumatic injury survivors.
It is well recognised that posttraumatic stress disorder (PTSD) is associated with significant impairment in functioning and quality of life (QoL) (Magruder et al., 2004; Rona et al., 2009). Critically, these impairments are often broad rather than localised, and include reductions in relationship functioning (intimate, familial and social), occupational functioning and performance and general engagement in rewarding and productive activity (Kuhn et al., 2003; Rodriguez et al., 2012; Sayers et al., 2009; Smith et al., 2005). In addition, of particular importance is that PTSD, particularly when chronic, is associated with high levels of distress and suicidality (Sareen et al., 2007, 2005). Despite substantial research and clinical evidence to support its pervasive impact on QoL, there is a relative paucity of research investigating which PTSD symptoms, or symptom clusters, account for these functional deficits and diminished perceived QoL. A small body of research has revealed that some specific PTSD symptom groups, such as numbing, may be associated with particular functional outcomes, namely relationship dysfunction (Taft et al., 2011). But to date, there has been no systematic research examining the influence of the full range of PTSD symptomatology on perceived QoL, across the key domains. A more systematic approach is necessary because the diagnosis of PTSD involves eliciting a heterogeneous and diverse range of symptoms that affects reliability. Greater understanding of which symptoms most account for domains of reduced functioning and QoL is critical in aligning phenomenology with treatment and guiding targeted intervention to more directly improve life satisfaction and functioning. This study sought to investigate the specific effects of PTSD symptomatology on QoL profiles in traumatic injury survivors.
Method
Participants
Participants were injury patients recruited from the trauma services of four hospitals in three states of Australia (in the period April 2004-February 2006). All patients met the DSM-IV Criterion A1 for PTSD. Patients were selected randomly from a pool of injury patients using a computerised random selection procedure. Inclusion criteria for patients were as follows: (1) having experienced a severe injury being one that required admission in hospital for greater than 24 hours, (2) aged between 16 and 70 years and (3) a reasonable comprehension of English. Patients were excluded if they had a traumatic brain injury (TBI) that was more severe than mild using the American Congress of Rehabilitation Medicine definition (American Congress of Rehabilitation Medicine, 1993), or if they were currently suicidal or psychotic. Written informed consent was obtained from all participants who were recruited over an 18-month timeframe. The Human Research and Evaluation Committees (HREC) in each hospital approved the research.
Of the 1590 patients eligible for the study, 1167 participants consented to participate. At 3 months, 987 persons completed the questionnaires for this study, and this dropped successively at 12 months to 862, at 24 months to 830 and at 6 years to 613. Those who refused to participate in the current study did not differ from participants in gender, χ2(1, N = 1590) = 1.50, p > 0.05, length of hospital admission, t(1571) = .92, p > 0.05, or injury severity t(1571) = 1.46, p > 0.05.
At 3 months, those lost to follow-up were younger (M = 35.5 years) than completers (M = 38.3), t(1143) = 3.8, p = 0.01. Those lost to follow-up were also younger at 12 months (p < 0.001), 24 months (p = 0.002) and 72 months (p < 0.001). The only other difference across the demographic variables was found at 24 months where those lost to follow-up had lower Injury Severity (ISS) scores (10.0 compared with 11.4), t(1163) = 2.6, p = 0.01.
At the first assessment point (3 months post-trauma), the majority of the participants were male (n = 729, 73.9%) with 43% of participants experiencing a TBI. On average, participants spent 12.4 (SD = 12.9) days in hospital and 14% of participants had an intensive care unit (ICU) admission. The principal mechanism of injury was transport accidents (65.9%), 16.1% experienced falls, 6.3% were assaults and 6.6% ‘other’.
Measures
PTSD was assessed using the Clinician Administered PTSD Scale CAPS (Blake et al., 1995). This structured clinical interview has demonstrated excellent reliability and validity and is one of the most widely used tools for diagnosing PTSD. All CAPS assessments were conducted by telephone, digitally audio-recorded and 5% were rescored by an independent rater who was blind to the original scoring to test inter-rater reliability. Overall PTSD diagnostic percentage agreement was 99%.
QoL was measured using the WHOQoL Bref. The WHOQoL Bref assesses four domains of QoL (social, psychological, environmental and physical) specified across 24 indicators. The measure has demonstrated good discriminant validity, content validity, internal consistency and test–retest reliability (World Health Organisation Quality of Life Instrument Group, 1998). In the WHOQoL, high scores represent greater function in particular domains; accordingly lower scores represent lower QoL.
Injury severity was measured using the Injury Severity Score scale (Copes et al., 1998). Prevalence of PTSD in the sample at each time point were 9.4% (3 months), 9.5% (12 months), 10.1% (24 months) and 7.7% (6 years). Other mental disorders were assessed using the Mini International Neuropsychiatric Interview, version 5.5 (22), a brief structured diagnostic interview based on Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) and International Statistical Classification of Diseases and Related Health Problems (ICD-10) criteria. The most prevalent other mental disorders were depression and generalised anxiety disorder with rates of 16.0% and 7.8%, 16.2% and 11.1%, 15.3% and 10.8% and 11.5% and 5.9% at each time point, respectively.
Data analysis
Latent class analysis (LCA) was implemented to model QoL profiles at 3 months, 12 months, 24 months and 6 years after the trauma. All analyses were conducted in Mplus version 7.2. LCA is a statistical technique that identifies patterns of responses using binary indicators; in this study, these indicators reflected dichotomised responses to items on the WHOQoL-Bref. LCA places individuals with similar profiles into the same class, and allows the user to empirically determine the number of classes that best fit the data. Full information maximum likelihood estimation is used to adjust for missing data on the latent class indicator variables. Three analytic steps were undertaken.
First, we identified the best-fitting unconditional model at each time-point. Here, we first fit the most parsimonious (one-class) model at each time-point, followed by successive models with increasing number of classes (e.g. two classes, three classes, etc.) to determine the minimum number of classes that can account for associations between symptoms. We assessed comparative model fit using information criteria, including the Bayesian information criterion (BIC), the Sample Size Adjusted Bayesian Information Criterion (SS-BIC), and the Akaike’s information criterion (AIC). For these indices, smaller values represent relatively better fit. We also considered entropy, which is a measure of classification quality, with values approaching 1 representing superior fit. Finally, we considered the Lo-Mendell-Rubin Likelihood Ratio Test (LMR-LRT), which compares the fit of a model solution with k classes to the previous solution (k-1 classes), with a significant LMR-LRT indicating that this model evidences better fit than the previous model. When determining the optimal class solution, we also considered parsimony and interpretability.
In the second analytic step, we used the best-fitting unconditional model at each time-point to construct a conditional model, by entering covariates (PTSD symptom cluster scores) into the model at each time-point. As this study commenced prior to the release of the DSM-5 criteria, we used the re-experiencing, effortful avoidance, emotional numbing and hyperarousal symptom clusters articulated by King and colleagues (King et al., 1998).
Finally, we used multinomial logistic regression analyses to examine the relationship between class membership (in the optimal unconditional models) and (1) injury severity score at baseline, (2) PTSD symptom severity score at each time-point and (3) individual symptoms from the PTSD symptom clusters that predicted class membership in the conditional models.
Results
Unconditional model
The goodness-of-fit indices for the one to five class unconditional models at each time-point are presented in Table 1. The three-class solution evidenced the optimal model fit at each time-point. For all models, the increase from a two to three class model yielded substantial decreases in the AIC, BIC and SS-BIC. When moving from the three to four class solution, the decreases in the AIC and SS-BIC were much smaller in magnitude, and the BIC evidenced increases in the 12-month, 24-month and 6-year models. Entropy was highest for the three class models at all time-points; however, at the 3-month time-point entropy was equally strong for the four-class model. For all models, except for the 6-year model, the LM-LRT was significant when moving from the two- to three-class models (indicating that the three-class solution evidenced better fit), but not significant when moving from the four- to five-class solutions (suggesting that the four-class solution did not fit the data better than the three class solution). For the 6-year model, the LM-LRT was not significant when moving from the two- to three-class models (p = 0.10); however, the AIC and the SS-BIC decreased substantially from the two- to three-class models. Accordingly, we judged the three-class solution as the optimal model at all time-points.
Unconditional LCA analyses at each timepoint.
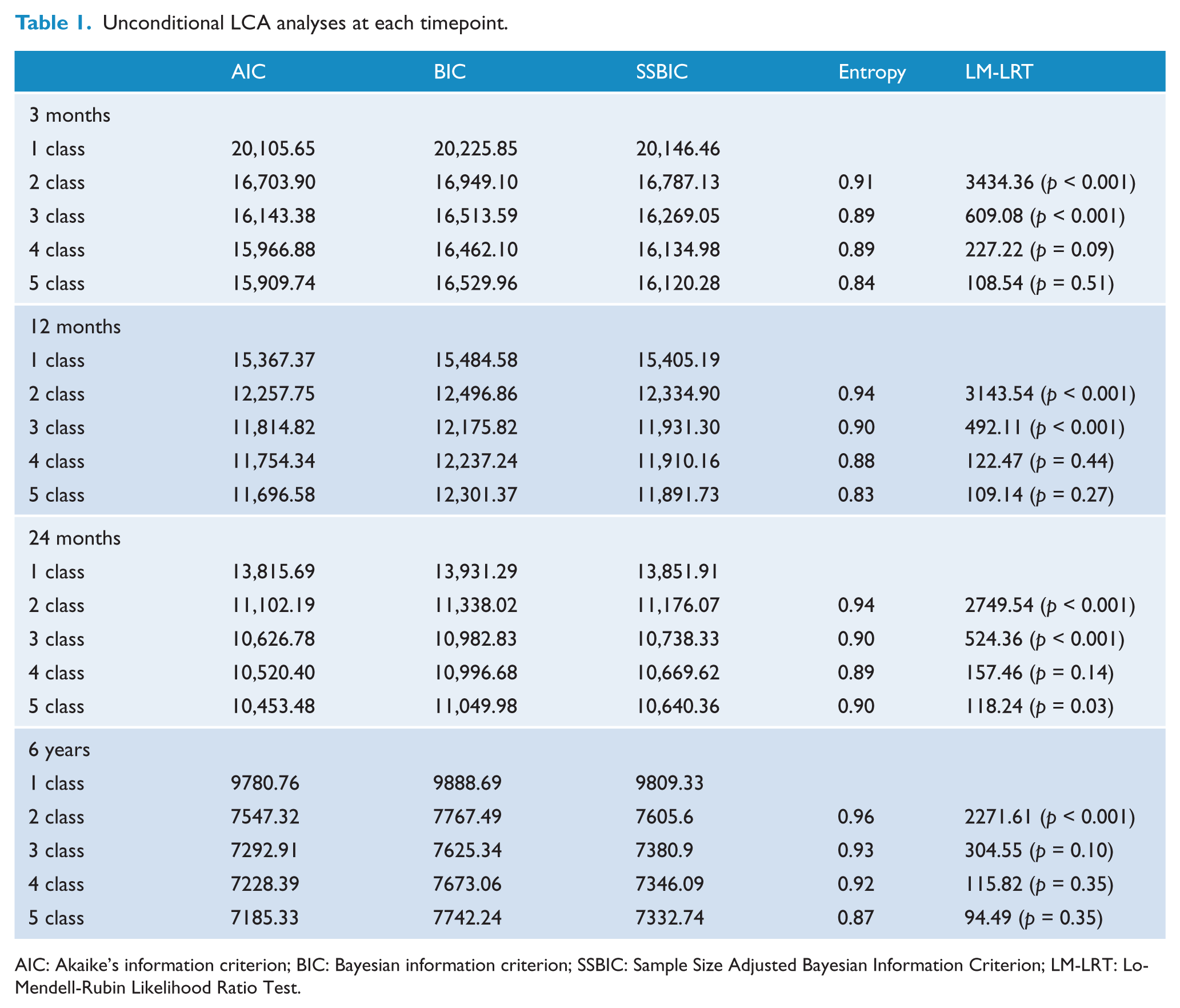
AIC: Akaike’s information criterion; BIC: Bayesian information criterion; SSBIC: Sample Size Adjusted Bayesian Information Criterion; LM-LRT: Lo-Mendell-Rubin Likelihood Ratio Test.
Final class counts at 3, 12, 24 months and 6 year were based on estimated posterior probabilities. Conditional probabilities of individual quality of life indicators for the optimal solution at each time-point are presented in Table 2, representing the proportion of individuals in each class who endorsed each indicator. We considered values of ⩾0.60 to represent a high probability that the symptom was present in this class, and probabilities of ⩽0.15 to represent a low probability that the symptom was present in this class (Burstein et al., 2012). Accordingly, we considered values ⩽0.59 and ⩾0.15 as representing a moderate probability that the symptom was present in this class.
Conditional probabilities of class membership for impairment profiles for optimal class solution at each timepoint.
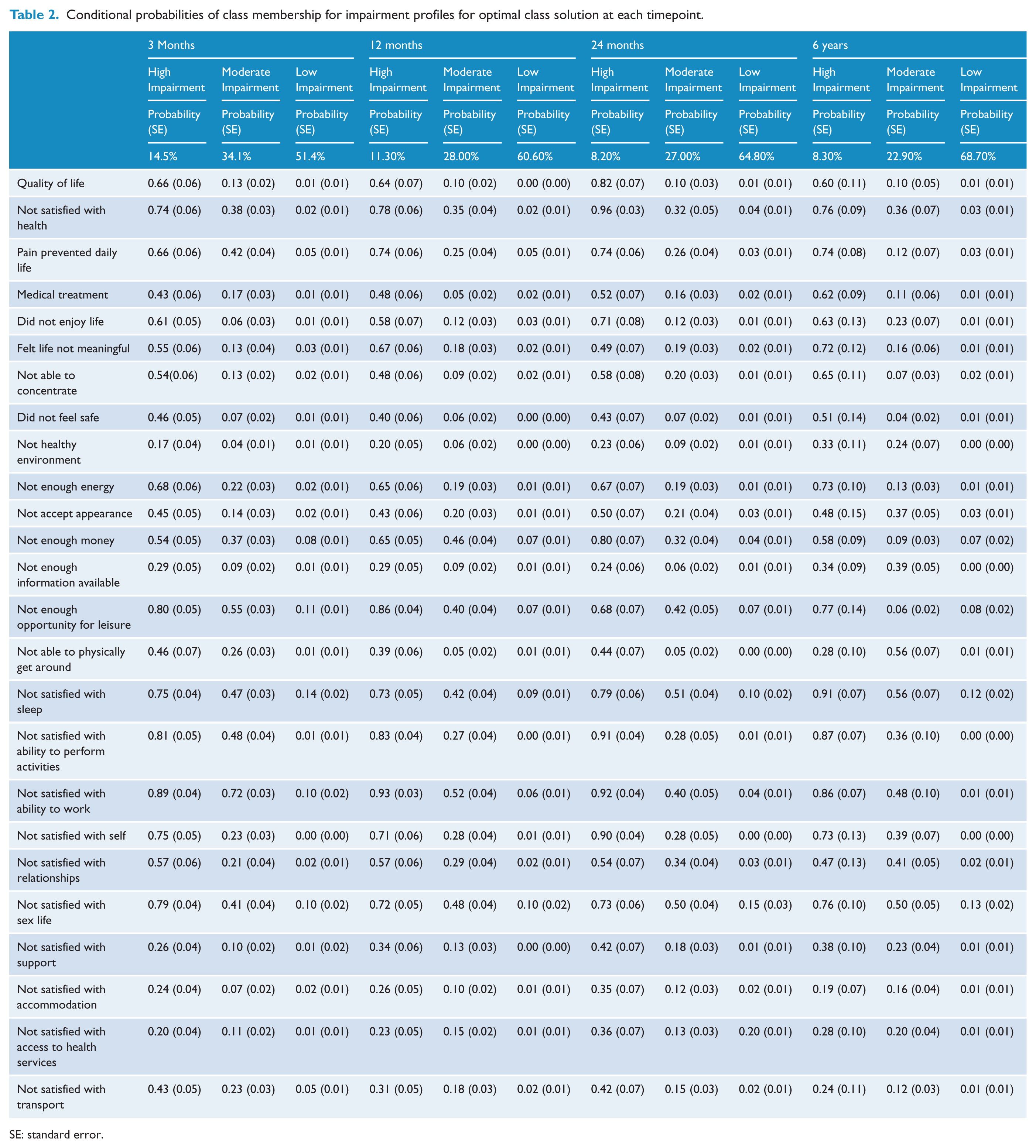
SE: standard error.
Quality of life profile in unconditional models
At 3 months, 14.5% of the sample (n = 131) comprised the Low QoL Class, 34.1% (n = 309) comprised the Moderate QoL Class, and 51.4% (n = 465) comprised the High QoL Class. Individuals in the Low QoL Class evidenced a high probability of endorsing problems in 11 of the 24 QoL indicators, and a moderate probability of endorsing problems in other QoL indicators. Key areas of perceived reduced QoL endorsed included general health, energy, leisure, performance of productive activity and capacity to work and sex life. Individuals in the Moderate QoL Class evidenced a high probability of reporting they were not satisfied with their ability to work, a moderate probability of endorsing 13 QoL indicators, and a low probability of endorsing the other 11 QoL indicators. Individuals in the High QoL Class evidenced low probability of endorsing problems in any QoL indicators.
At 12 months, 11.3% (n = 91) of the sample comprised the Low QoL Class, 28% (n = 225) comprised the Moderate QoL Class, and 60.6% (n = 487) comprised the High QoL Class. Participants in the Low QoL Class evidenced high probability of endorsing problems in 12 QoL indicators, and a moderate probability of endorsing problems in all other QoL indicators. Key areas significantly endorsed included those outlined at 3 months in addition to dissatisfaction with money and meaningfulness of life. Individuals in the Moderate QoL Class evidenced a moderate probability of endorsing problems in 15 of the QoL indicators, and a low probability of endorsing problems in the remaining 10 QoL indicators. Individuals in the High QoL Class evidenced low probability of endorsing problems in any of the QoL indicators.
At 24 months, 8.2% (n = 62) of the sample comprised the Low QoL Class, 27.0% (n = 203) made up the Moderate QoL Class and 64.8% (n = 488) comprised the High QoL Class. Individuals in the Low QoL Class evidenced high probability of endorsing problems in 12 of the QoL indicators, and a moderate probability of endorsing problems in 13 of the QoL indicators. Key areas significantly endorsed as problematic included health, pain, money, leisure, productive activity, ability to work and sex life. Individuals in the Moderate QoL Class evidenced a moderate probability of endorsing problems in 17 of the QoL indicators, and a low probability of endorsing problems in all other indicators. Participants in the High QoL Class evidenced low probability of endorsing problems in any QoL indicator.
At 6 years, 8.3% (n = 46) of the sample made up the Low QoL Class, 22.9% (n = 127) comprised the Moderate QoL Class and 68.7% (n = 381) made up the High QoL Class. Participants in the Low QoL Class evidenced high probability of endorsing problems in 14 of the QoL indicators and moderate probability of endorsing problems in 11 of the indicators. Key areas included health, pain, meaningfulness of life and sex life. Individuals in the Moderate QoL Class evidenced moderate probability of endorsing problems in 16 of the QoL indicators, and low probability of endorsing problems in nine of the indicators. Participants in the High QoL evidenced low probability of endorsing problems in any QoL indicators.
Conditional models
Results from the conditional models in which covariates (PTSD clusters) were used to predict class membership are presented in Table 3. Bonferroni corrections were used to adjust for multiple comparisons with significance, with significance set at p < 0.012. At 3, 12 and 24 months, participants in the Low QoL Class evidenced significantly more numbing and arousal symptoms compared to the High QoL Class. Participants in the Moderate QoL Class evidenced significantly more arousal symptoms at 3 and 12 months compared to those in the High QoL Class and at 24 months significantly greater numbing and arousal compared to those in the High QoL Class. At 6 years, participants in the Low and Moderate QoL Classes evidenced significantly more arousal compared to those in the High QoL Class.
Conditional models with PTSD symptom cluster scores as covariates.
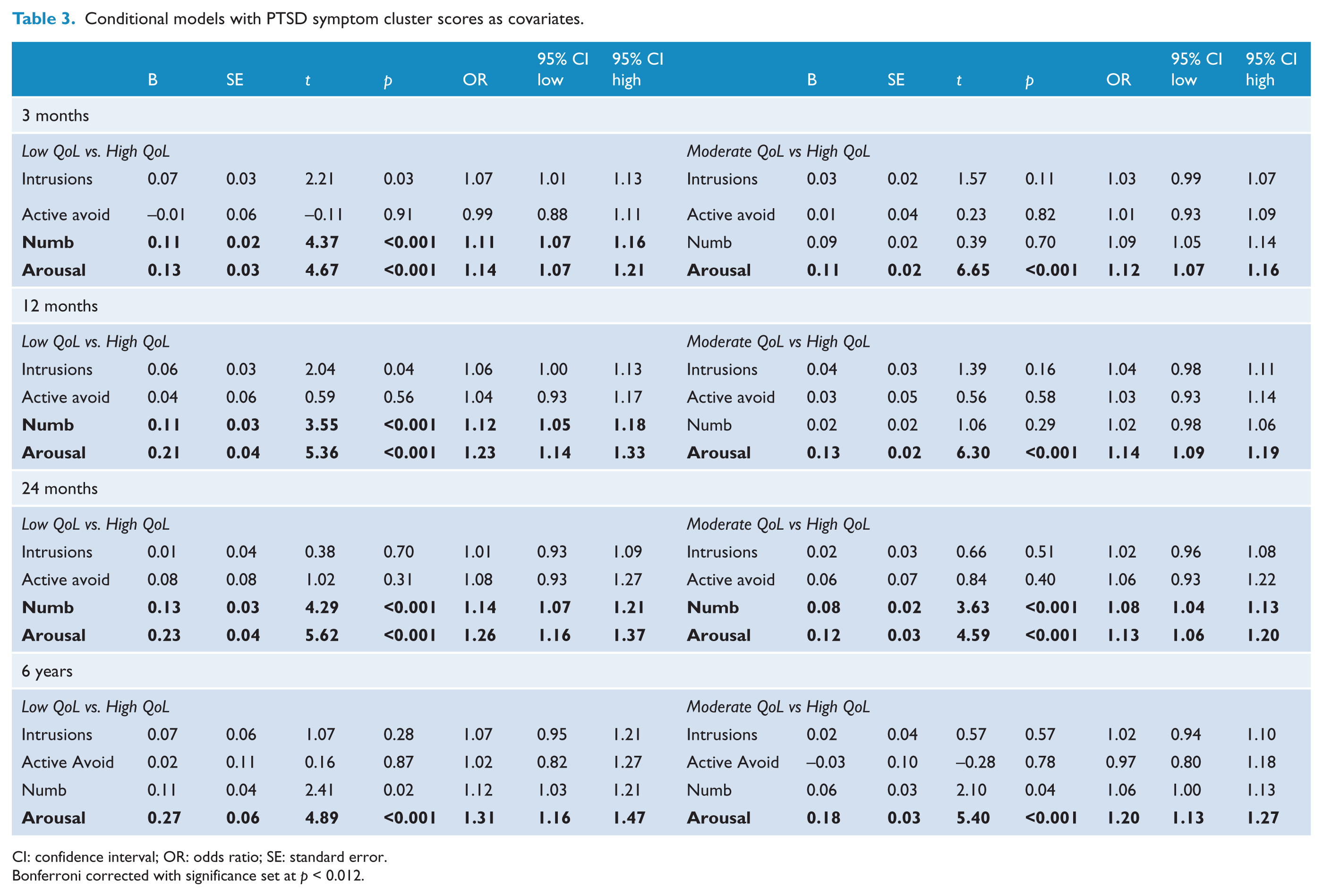
CI: confidence interval; OR: odds ratio; SE: standard error.
Bonferroni corrected with significance set at p < 0.012.
Relationship between Class Membership and Injury Severity Score
Multinomial logistic regressions were used to investigate the association between class membership at each time-point and injury severity score upon admission to hospital. Results are presented in Table 4. Findings indicated that there were no significant differences between classes in injury severity at any time-point.
Relationship between class membership and injury severity score.
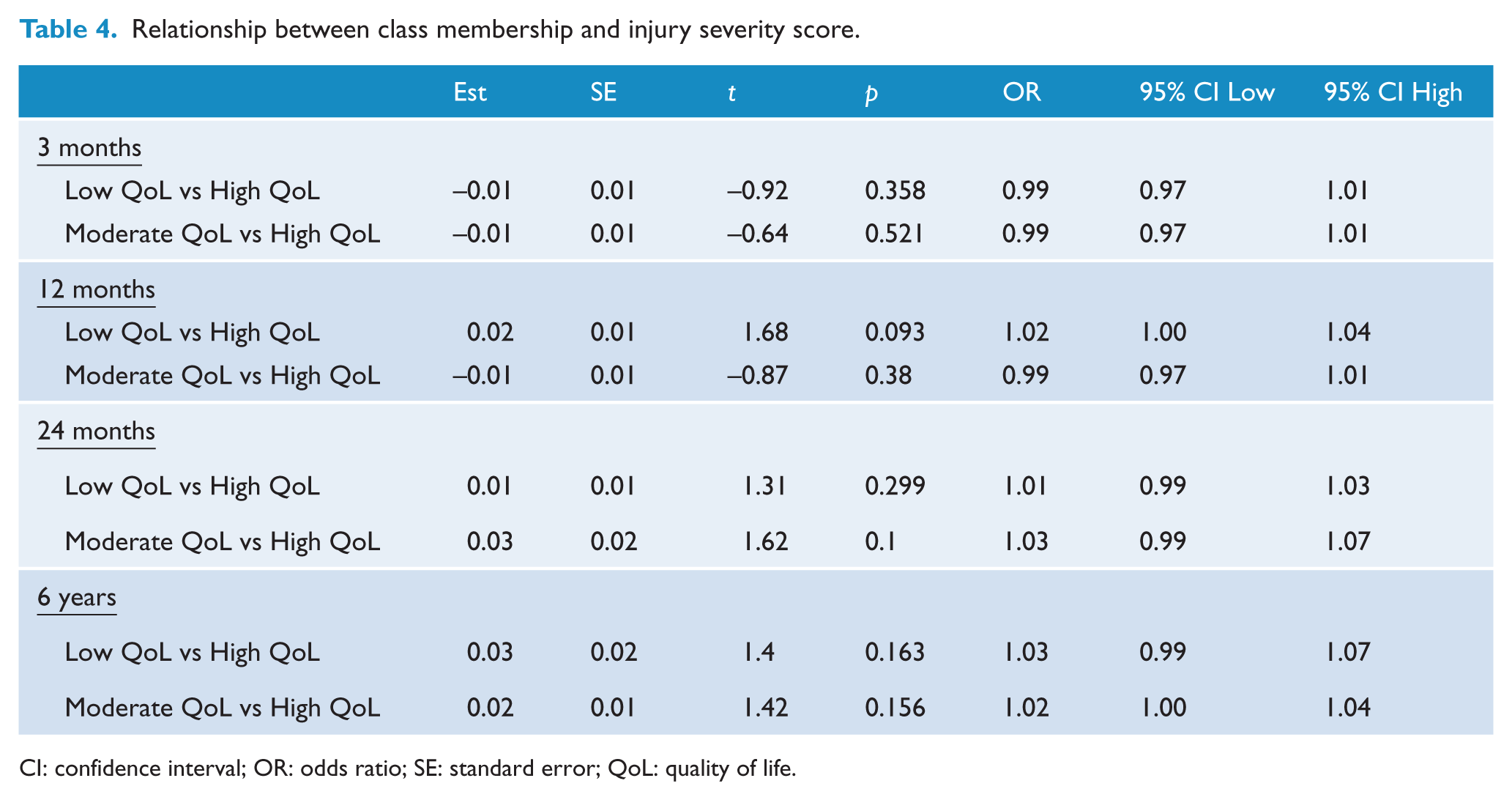
CI: confidence interval; OR: odds ratio; SE: standard error; QoL: quality of life.
Relationship between class membership, PTSD symptom severity
We used multinomial logistic regression analyses to examine the relationship between class membership at each time-point and PTSD total symptom scores at the corresponding time-point. Results are presented in Table 5. Findings revealed that, at each time-point, individuals in the Low QoL class evidenced higher levels of PTSD symptoms compared to those in the High QoL class. Similarly, individuals in the Moderate QoL class reported higher levels of PTSD symptoms compared to those in the High QoL class.
Relationship between class membership and PTSD symptom severity.
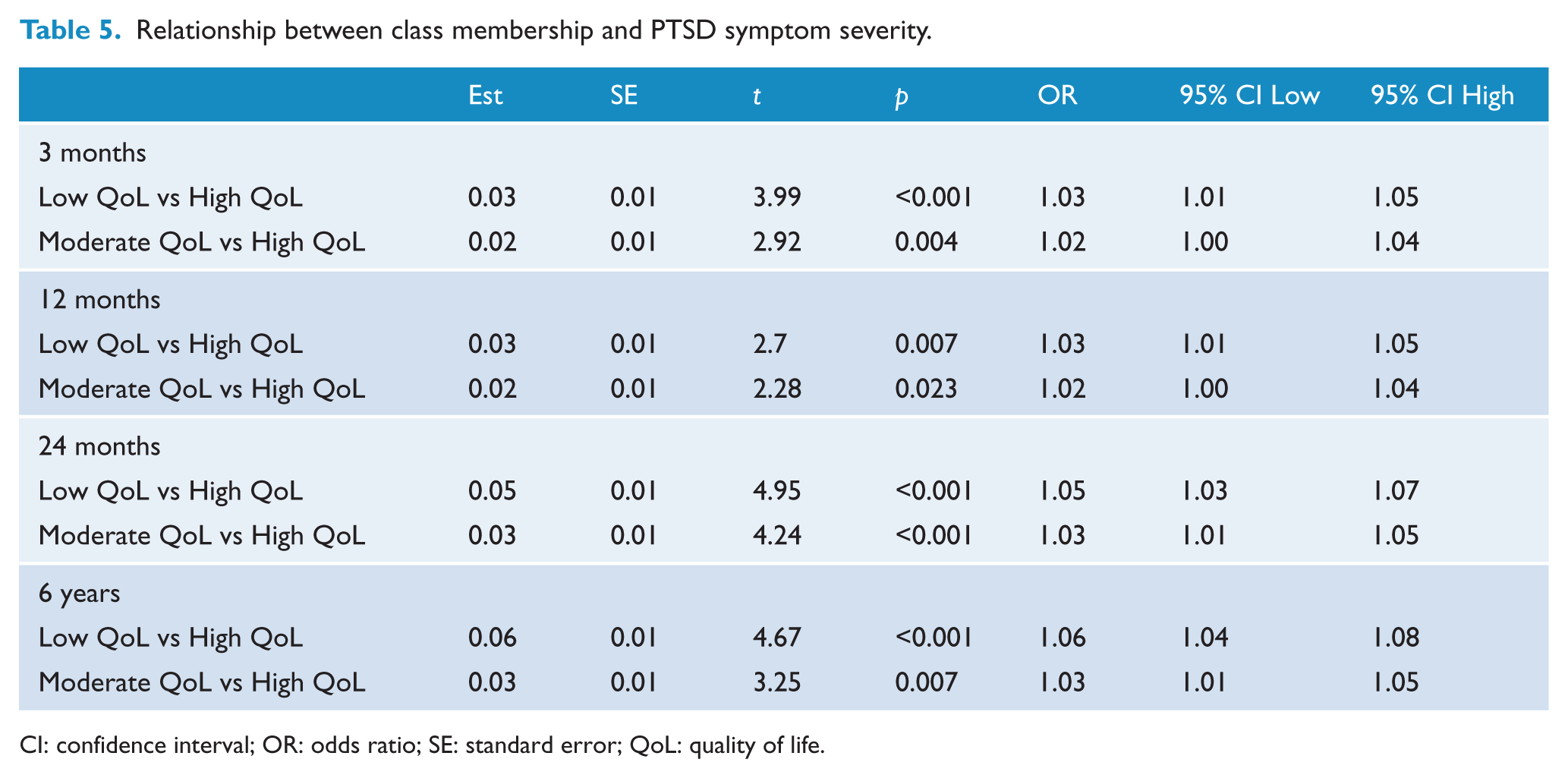
CI: confidence interval; OR: odds ratio; SE: standard error; QoL: quality of life.
Relationship between class membership and numbing and hyperarousal symptoms
Multinomial logistic regressions were conducted to examine the association between class membership at each time-point and individual numbing and hyperarousal symptoms. Results are presented in Table 6. Bonferroni corrections were used to adjust for multiple comparisons with significance, with significance set at p < 0.005. At 3 months, participants in the Low QoL Class were more likely than those in the High QoL Class to report restricted affect, anger, and concentration difficulties. Participants in the Moderate QoL Class compared to the High QoL Class reported greater anger and concentration problems.
Association between PTSD symptoms and class membership.
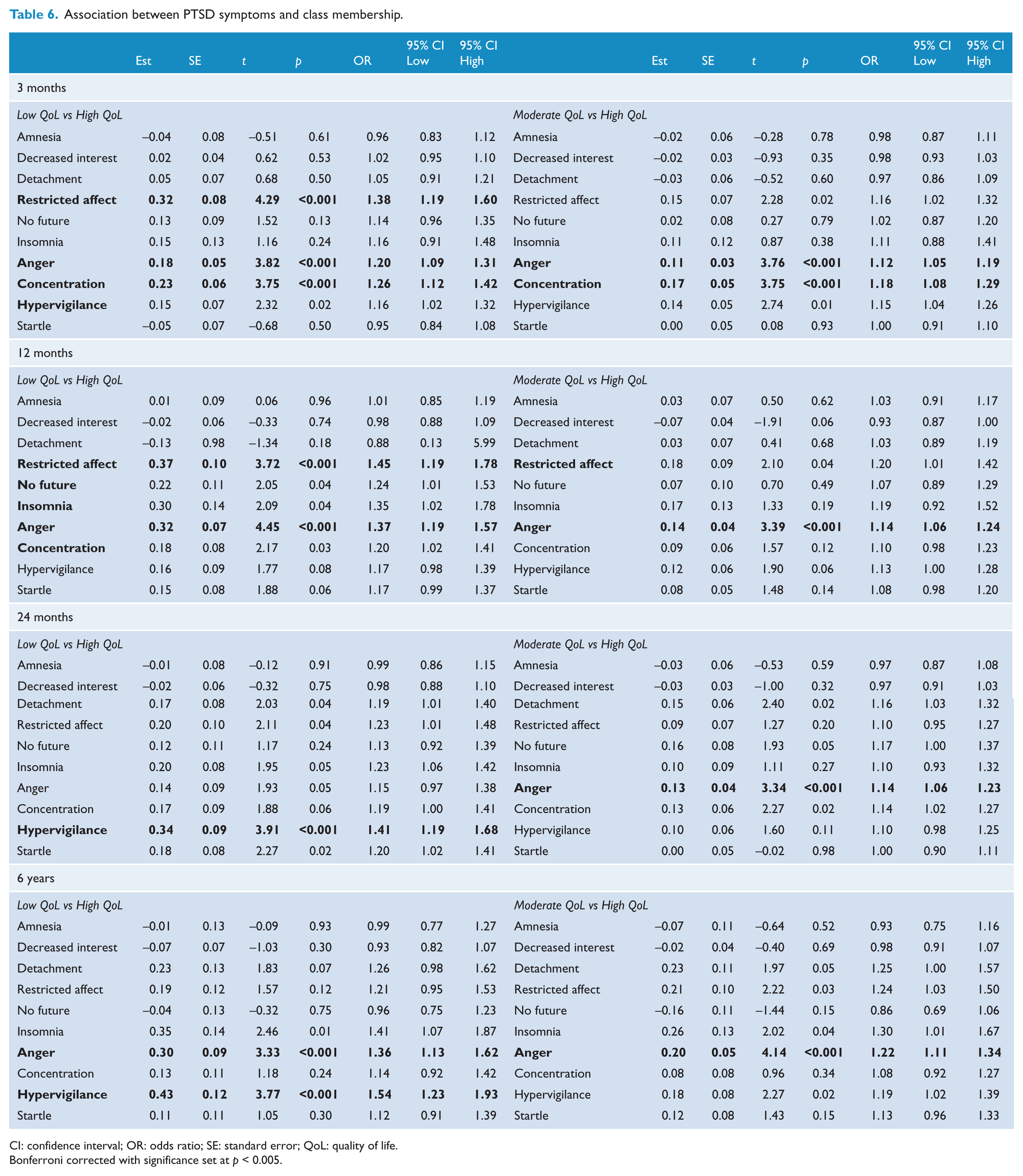
CI: confidence interval; OR: odds ratio; SE: standard error; QoL: quality of life.
Bonferroni corrected with significance set at p < 0.005.
At 12 months, participants in the Low QoL Class were more likely than those in the High QoL Class to report restricted affect and anger difficulties. Compared to those in the High QoL Class, participants in the Moderate QoL Class were more likely to report anger. At 24 months, participants in the Low QoL Class were more likely than those in the High QoL Class to report hypervigilance. Compared to those in the High QoL Class, participants in the Moderate QoL Class were more likely to report anger. At 6 years, participants in the Low QoL Class were more likely than those in the High QoL Class to report anger and hypervigilance. Compared to those in the High QoL Class, participants in the Moderate QoL Class were more likely to report anger. Figures 1 and 2 reflect the trajectories of the key predictive symptoms of anger, hypervigiliance, concentration and restricted affect.
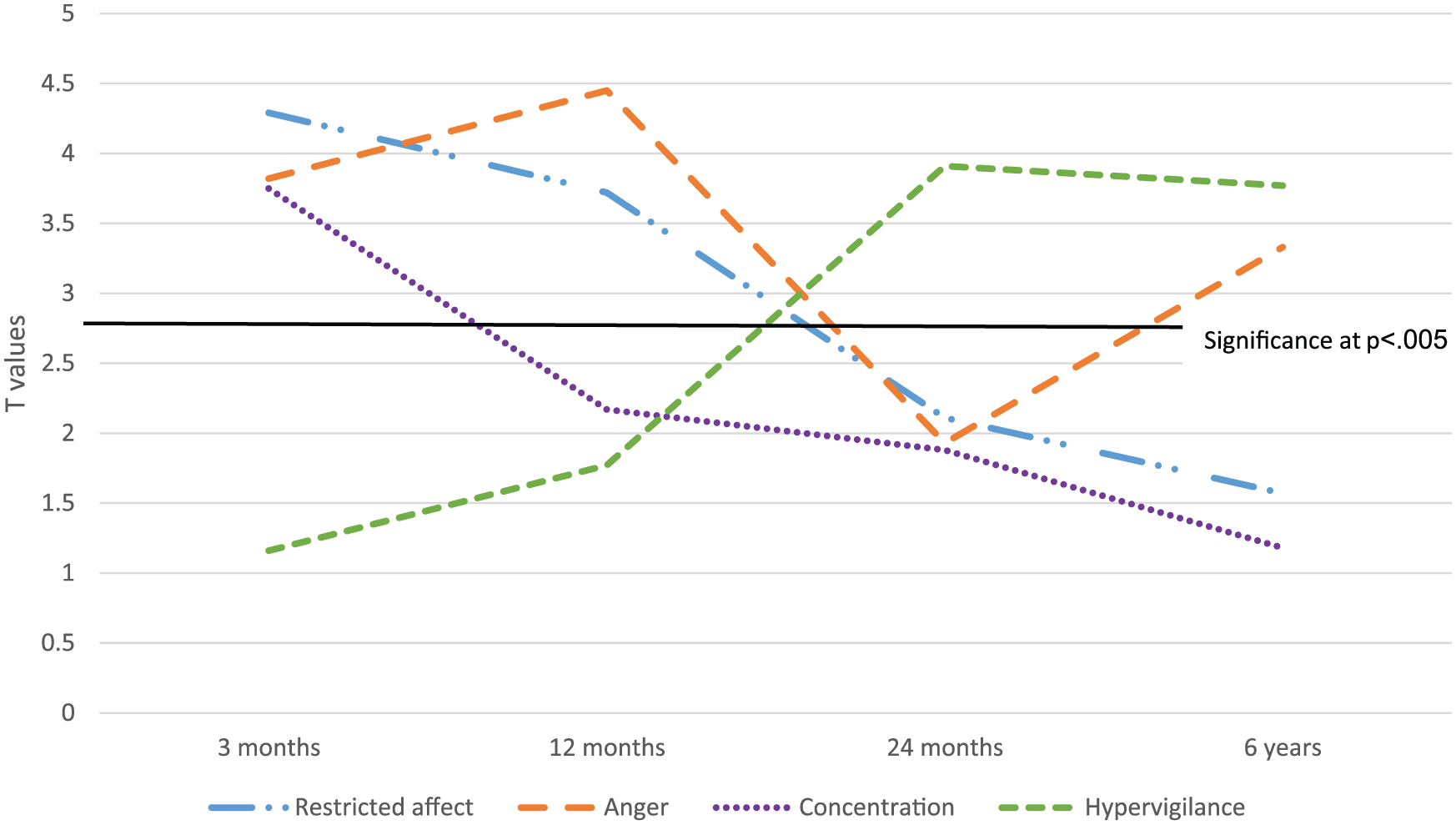
Four key PTSD symptoms associated with class membership – Low QoL vs High QoL.
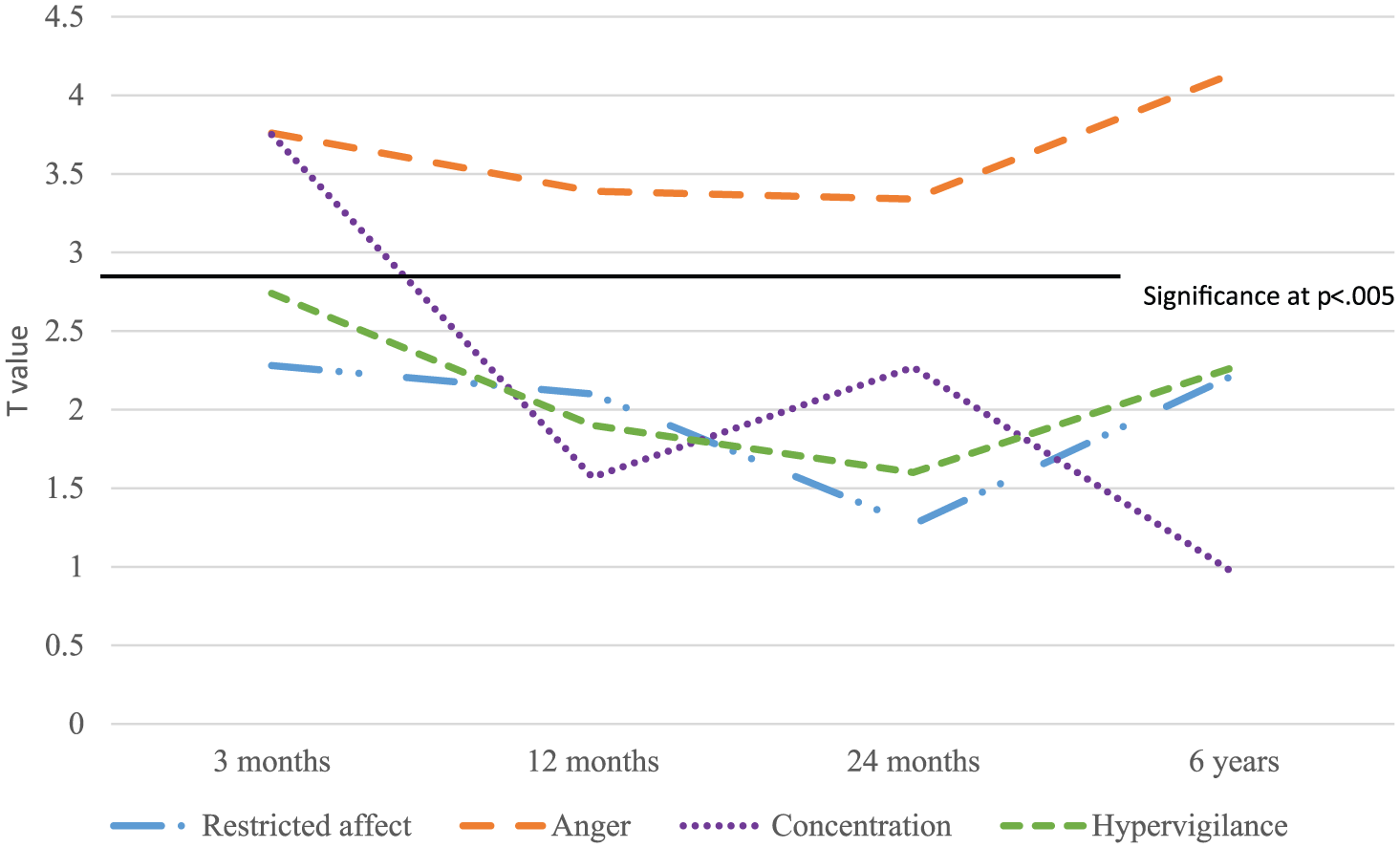
Four key PTSD symptoms associated with class membership – Moderate QoL vs High QoL.
Discussion
Prevalence of poor perceived QoL
This study highlights the variability in QoL in traumatic injury survivors. In traumatic injury survivors across both the low and moderate QoL groups, dissatisfaction with life was reflected across multiple domains of functioning. The number of injury survivors reporting the poorest QoL remained substantial from 3 months (14.5%) to 6 years (8%) post event. There was also considerable consistency in the domains of functioning highlighted as those of greatest concern over the course of the 6 years post-injury. These domains included dissatisfaction with health, productive activity, capacity to work, sex life and pain. By 12 months, those reporting the poorest QoL were also highlighting monetary concerns and loss of a perceived meaningfulness of life that also persisted to 6 years post event. Critically, these QoL classes did not differ on scores of injury severity.
PTSD symptoms related to poor QoL
In terms of understanding the relationship between PTSD and QoL, first PTSD severity was higher overall in both the Low QoL and Moderate QoL classes compared with the High QoL class. More specifically, the PTSD symptom clusters that contributed most to poor perceived QoL were interestingly not the hallmark intrusion and avoidance symptoms. Intrusions and active avoidance symptoms failed to predict class membership at any time point. Rather, numbing and hyperarousal were important predictors. Closer examination of the symptoms that most strongly accounted for perceived poorer functioning within these domains showed an important difference between those with low and moderate QoL. For those with low QoL, restricted affect from the numbing cluster and anger from the hyperarousal cluster, were influential across the first two time points, while hypervigilance emerged as influential at 24 months, and again at 72 months, alongside anger. There was a more consistent pattern for those with moderate QoL, with anger almost exclusively predicting poorer QoL at every time point from 3 months to 6 years post event.
A noteworthy feature of both anger and hypervigilance is their potential pervasiveness, negative emotional valence and influence on cognitive set. Anger and hypervigilance reflect an orientation to threat sensitivity, hostile appraisal and blame likely to also be associated with confrontational or combative behaviour (Forbes et al., 2013; Novaco and Chemtob, 2002). By contrast other hyperarousal symptoms such as sleep disturbance and concentration difficulties, while impairing function, are not necessarily associated with negative emotional states nor do they reflect hostile or threat related engagements with the world. Similarly in understanding the limited influence of intrusive symptoms or avoidance behaviours on QoL, it may be that, while generating considerable internal distress or restriction in activity they are not predicated on negative threat based interpersonal engagements. These findings are also consistent with previous research findings indicating that, in addition to being associated with the development and maintenance of PTSD, anger is also linked to poorer health outcomes post-trauma (Forbes et al., 2008; Jayasinghe et al., 2008; Koenen et al., 2003).
The impact of numbing, and more particularly, restricted affect on QoL in the first 12 months is also notable. Interestingly restricted affect ceases to feature as predicting poorer QoL by 24 months. The literature indicates that numbing, where present, tends to be a more persisting feature of traumatic stress and associated with more severe forms of the condition (Breslau and Davis, 1992). That is ceases to be a predictor of reduced QoL after 12 months is a curious finding and somewhat contrary to the authors’ expectations. It needs to be noted here that the QoL measure does not assess function, but perceptions of satisfaction with various aspects of life. Perhaps after 12 months survivors adapt to the experience of restriction of affect where it is present, accommodating it to the point where they decreasingly perceive lack of emotional reactivity as a QoL concern.
Implications for treatment
Trauma-focused psychological therapies are currently the most evidence-based approaches to the treatment of PTSD and indeed are recommended as first line interventions in international guidelines for the treatment of this disorder (Forbes et al., 2010). However, trauma-focused treatments tend to target most directly the hallmark features of the disorder, namely the re-experiencing and avoidance symptomatology. The findings of this study suggest that while this is important, it is not the re-experiencing and avoidance features that most affect perceptions of QoL across a broad range of domain indicators. While trauma-focused treatments have demonstrated effectiveness in improving quality-of-life outcomes in trauma survivors, findings indicate that a considerable proportion of PTSD sufferers do not fully respond to these treatments, with between 30–50% retaining diagnosis even after the most evidence based treatments. It may be that early intervention, targeting the features of PTSD of anger, hypervigilance and detachment directly may offer a more direct pathway into improvements in QoL, and also offer a particular focus for those who fail to gain sufficient benefit from the current approaches.
Limitations
There are a number of limitations that need to be considered when interpreting the results from this study. First, these findings are based on reports from severe injury survivors specifically and cannot necessarily be generalised to PTSD symptoms experienced in survivors of other types of traumatic events. In particular responses to interpersonal and non-interpersonal trauma are found to vary considerably (Galatzer-Levy et al., 2012). Therefore, replication of this study with survivors of interpersonal trauma is warranted. Second, anger has been identified as an important component in the differential QoL reported after a trauma across a broad timespan. However, as a single item measure, we are unable to unpack whether there are specific aspects of anger which are most important. The STAXI includes six subscales of anger which include aspects such as trait anger, anger inwards and anger outwards (Spielberger, 1996), while other measures such as the DAR-5 identify anger and its impact on social relations, the desire to express anger physically, along with intensity and duration of anger (Forbes et al., 2014). Future studies which investigate whether individual components of anger are more important would be worthwhile to inform clinical treatment approaches. Finally, we note the extent of depression and generalised anxiety in this sample and that while the focus of this study is on PTSD symptoms, this has not controlled for the impact of these other disorders on QoL. There would be benefit in future studies widening the lens of investigation to include the impact of symptoms of other disorders such as depression and generalized anxiety disorders on QoL.
In conclusion, we found variability in the QoL of traumatic injury survivors over a 6 year period, with a significant proportion reporting low QoL 3, 12, and 24 months and 6 years after the trauma. Anger, hypervigilance and detachment contributed most to poor perceived QoL, potentially via their negative impact on behaviour and interpersonal engagements. Interventions, which specifically target these symptoms may have the greatest potential to improve the QoL of traumatic injury survivors.
Footnotes
Acknowledgements
The authors gratefully acknowledge all the participants involved in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was financially supported by a National Health and Medical Research Council Program Grant (568970). The National Health and Medical Research Council were not involved in the design or completion of the study.