
Abstract
Objective:
Insomnia and anxiety commonly co-occur, yet the mechanisms underlying this remain unclear. The current paper describes the impact of an Internet-based intervention for insomnia on anxiety, and explores the influence of two cognitive-behavioural constructs – dysfunctional beliefs about sleep and sleep-threat monitoring.
Methods:
A large-scale, 9-week, two-arm randomised controlled trial (N = 1149) of community-dwelling Australian adults with insomnia and elevated yet subclinical depression symptoms was conducted, comparing a cognitive behavioural therapy–based online intervention for insomnia (Sleep Healthy Using The Internet) with an attention-matched online control intervention (HealthWatch). Symptoms of anxiety were assessed at pretest, posttest, and 6-month follow-up. Dysfunctional beliefs about sleep and sleep threat monitoring were assessed only at pretest.
Results:
Sleep Healthy Using The Internet led to a greater reduction in anxiety symptoms at both posttest (t724.27 = –6.77, p < 0.001) and at 6-month follow-up (t700.67 = –4.27, p < 0.001) than HealthWatch. At posttest and follow-up, this effect was found to moderated by sleep-threat monitoring (t713.69 = –2.39, p < 0.05 and t694.77 = –2.98, p < 0.01 respectively) but not by dysfunctional beliefs about sleep at either posttest or follow-up (t717.53 = –0.61, p = 0.55 and t683.79 = 0.22, p = 0.83 respectively). Participants in the Sleep Healthy Using The Internet condition with higher levels of sleep-threat monitoring showed a greater reduction in anxiety than those with lower levels from pretest to posttest, (t724.27 = –6.77, p < 0.001) and through to 6-month follow-up (t700.67 = –4.27, p < 0.001). This result remained after controlling for baseline anxiety levels.
Conclusion:
The findings suggest that online cognitive behavioral therapy interventions for insomnia are beneficial for reducing anxiety regardless of people’s beliefs about their sleep and insomnia, and this is particularly the case for those with high sleep-threat monitoring. This study also provides further evidence for cognitive models of insomnia.
Introduction
Insomnia, estimated to have a prevalence of 10–15% of the adult population (Drake et al., 2003), has a substantial impact on quality of life and productivity. When experienced in isolation, insomnia accounts for as many as 3.5 disability days per month in typical sufferers, a level comparable to non-comorbid generalised anxiety disorder and somatoform disorders (Simon and Vonkorff, 1997). Moreover, there is considerable comorbidity between many physical illnesses and insomnia, including gastroesophageal reflux disorder, neurodegenerative disease, and pain conditions (Roth, 2007). The most common comorbidities with insomnia, however, are psychiatric conditions, with approximately 20–40% of people with insomnia experiencing a co-occurring psychiatric illness (Benca et al., 1992; Ford and Kamerow, 1989; Ohayon, 2002). Depression is the single most common comorbidity with insomnia, with 35–47% of insomnia sufferers experiencing significant depression and 60–84% of people with major depressive disorder (MDD) also having significant insomnia symptoms (Taylor et al., 2005). However, anxiety disorders as a cluster are the most commonly diagnosed group of disorders in people with insomnia (Ohayon, 2002). People with insomnia are 17.4 times more likely than the general population to have clinically significant anxiety, compared to 9.8 times more likely to have clinically significant depression (Taylor et al., 2005). In all, 70–90% of people with anxiety disorders have sleep difficulties (Mellman, 2006; Papadimitrou and Linkowski, 2005; Uhde et al., 2009). Insomnia is also a strong predictive risk factor for the development of depression and anxiety disorders (Batterham et al., 2012; Neckelmann et al., 2007).
A substantial body of research has been conducted on the relationship between depression and insomnia. As indicated by Belleville et al. (2011), insomnia increases depression risk (Breslau et al., 1996; Ford and Kamerow, 1989) complicates depression treatment (Dew et al., 1997; Thase et al., 1997), and increases suicide risk in depressed patients (Thase, 1998). The relationship between insomnia and anxiety has received less attention, although, in contrast to depression, it has not been found to be confounded by neuroticism or rumination (Batterham et al., 2012). Cognitive models of insomnia closely resemble cognitive models of anxiety, with an emphasis on worry/ anxiety about the consequences of insomnia, dysfunctional beliefs about sleep, the use of safety behaviours, and selective attention to sleep-threat cues (sleep-threat monitoring) (Espie, 2007; Gosling et al., 2012; Harvey, 2002a; Lundh and Broman, 2000; Morin, 1993). Dysfunctional beliefs about sleep are a major factor in cognitive models of sleep disturbance and insomnia due to increasing worry and arousal, which are antithetical to sleep (Harvey, 2002a; Morin, 2002). Sleep-threat monitoring is also central to cognitive models of sleep disturbance, and is a more active/behavioural process referring to the tendency of people with insomnia to actively and selectively attend to cues, both internal (i.e. bodily sensations) and external (i.e. the immediate environment), that might indicate a threat to getting adequate sleep. In this sense, while dysfunctional beliefs about sleep represents a purely cognitive, or attitudinal, factor in the maintenance of insomnia, sleep-threat monitoring is something that the person is actively doing, albeit a largely mental process, and thus plays a slightly different role in maintaining a person’s insomnia and might plausibly differ from dysfunctional beliefs when it comes to moderating treatment outcomes. An example of this is scanning bodily/somatic cues for signs of relaxation or arousal, such as heart-rate, heaviness, feelings of ‘drifting off’, muscles getting weaker and so on. This has the unwanted outcome of increasing arousal and delaying sleep (Harvey, 2002a; Semler and Harvey, 2004a). Between cognitive models of anxiety and cognitive models of insomnia suggest an important relationship between insomnia and anxiety and potentially shared underlying mechanisms.
The current analysis examines anxiety symptoms as a secondary outcome in the context of a randomised controlled trial (RCT) which tested a web-based intervention for insomnia as a means of reducing depression. While the RCT demonstrated the intervention to be effective in reducing anxiety symptoms. Recruiting 1149 Australian adults aged 18–64 with subclinical depression symptoms and insomnia, GoodNight assigned participants to either a 9-week insomnia treatment programme (Sleep Health Using The Internet [SHUTi]; Ritterband et al., 2009), or an attention-matched control placebo (HealthWatch). SHUTi provides automated cognitive behavioural therapy for insomnia that is tailored and interactive, and does so through a web-based programme. The RCT’s primary focus was prevention of depression, aiming to reduce depressive symptoms and prevent depressive episodes in those at risk of developing depression via treatment of insomnia; a strong, independent risk factor for depression (Nowell and Buysse, 2001). Participants were selected based on elevated (but subclinical) depression symptoms on the Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001), and insomnia on the Bergen Insomnia Scale (BIS; Pallesen et al., 2008). Selection and exclusion were not based on anxiety symptomatology or meeting criteria for an anxiety disorder, but participants had an elevated risk of anxiety by virtue of the fact that they had both insomnia and subclinical depressive symptoms. Full details of the study design (Gosling et al., 2014) and primary outcomes (Christensen et al., 2016) are reported elsewhere. As has recently been published (Christensen et al., 2016), the intervention was effective in reducing depression symptoms (PHQ-9), suicidal ideation Psychiatric Symptom Frequency scale (PSF), anxiety (Generalised Anxiety Disorder-7 [GAD-7]), sleep (Insomnia Severity Index Scale [ISI]) and disability (WHO Disability Assessment Schedule-12).
The current paper aims to explore the intervention’s effect on anxiety, testing the moderating influence of two cognitive-behavioural factors: (1) a cognitive factor, dysfunctional beliefs about sleep and (2) a more active/behavioural factor, sleep-threat monitoring. These were both measured at pretest. We tested the hypothesis that participants with higher levels of dysfunctional beliefs about sleep and sleep-threat monitoring would show greater treatment effects with respect to anxiety. To the authors’ knowledge, no insomnia treatment trials to date have measured both cognitive and behavioural maintenance factors prior to treatment in order to elucidate their relative influences on treatment effectiveness.
Methods
Study design
The GoodNight Study is an RCT with intervention and attention-matched control arms. The current paper reports on data from the baseline, post-test, and 6 months assessments. The study was approved by the Australian National University (ANU) Human Ethics Committee (Protocol 2011/041). Recruitment commenced in April 2013 and completed in June 2014.
Participants
Participants were 1149 community-dwelling Australian adults aged 18–64. Participants were recruited largely via a dedicated Facebook page for the study, but also via advertisements placed on websites and in newsletters of Australian sleep and mental health associations and foundations, and via print and radio media publicity following media releases.
Screening and eligibility
Screening for eligibility took place online, and consisted of the BIS (Pallesen et al., 2008) and PHQ-9 (Kroenke et al., 2001). If a participant met criteria for insomnia on the BIS (a score of ⩾3 on at least one of the first four items and ⩾3 on at least one of the last two items), and subclinical depression on the PHQ-9 (>4 and <20), they completed secondary eligibility online criteria questions. This section excluded respondents who were shift workers, carers whose sleep was likely to be interrupted, pregnant women, people with no reliable Internet connection, people who could not comfortably read English, those who reported they had been diagnosed with psychosis, schizophrenia or bipolar mood disorder, and those currently receiving a non-drug treatment for insomnia from a health professional.
Eligible participants then underwent a telephone-based assessment including the Mini International Neuropsychiatric Interview (Sheehan et al., 1998) to exclude those meeting criteria for current MDD, lifetime bipolar mood disorder criteria, and/or those who had planned or attempted suicide in the previous fortnight. This interview also included Morin’s modified diagnostic insomnia interview (Thorndike et al., 2008) to confirm a diagnosis of insomnia, to exclude people with another, untreated, sleep disorder or a medical illness accounting for their sleep disturbance, and to exclude anyone whose medication had changed in the previous 3 months.
Eligible participants were then randomised to the study, completed baseline surveys online, and completed 2 weeks of daily sleep diaries, after which they began their allocated programme.
Randomisation
Participants were stratified by age and gender, and allocation was randomised using an automated procedure built into the trial management software. Telephone-based interviewers delivering the MINI and telephone reminders, statisticians and chief investigators were all blind to allocation. No unmasking occurred during the trial.
Interventions
The active intervention was SHUTi, an online insomnia programme based on Cognitive Behaviour Therapy. SHUTi delivers six modules: overview, two behaviourally focused modules that included sleep restriction and stimulus control, cognitive restructuring, sleep hygiene and relapse prevention. Participants were encouraged to complete a daily sleep diary throughout their use of SHUTi. The diaries were mandatory between the first and second module, but not required following this period. The sleep diary data were used by SHUTi to calculate sleep efficiency and identify the optimal sleep windows for the participant. The attention-matched placebo control website delivered a 9-week version of HealthWatch, an online, interactive lifestyle website with no specific mental health or sleep-related content (Griffiths et al., 2010). Modules were comprised of information about environmental health, nutrition, heart health, activity, medication, oral health, blood pressure and cholesterol, calcium and back pain, as well as weekly surveys on these topics.
Measures
The outcome of interest in this analysis was anxiety symptoms, measured using the GAD-7 scale (Spitzer et al., 2006). This assesses anxiety symptoms over the previous 2-week period and has been validated as a community anxiety screener (Lowe et al., 2008). The inventory comprises seven items reflecting core symptoms of generalised anxiety, rated on a scale from 0 ‘not at all’ to 3 ‘nearly every day’, with total scores potentially ranging from 0 to 21. The GAD-7 shows good internal consistency (α = 0.89), and convergent validity with relevant scales in community samples (Lowe et al., 2008). It has a sensitivity of 89% and a specificity of 82% for Diagnostic and Statistical Manual of Mental Disorders (4th edition; DSM-IV) GAD (Spitzer et al., 2006).
Cognitive-behavioural factors assessed in the trial were dysfunctional beliefs about sleep and sleep-threat monitoring. Dysfunctional beliefs about sleep were measured using the Dysfunctional Beliefs About Sleep-16 Scale (DBAS-16) (Morin et al., 2007), which is a reliable (α = 0.77 and 0.79 for clinical and research samples) and temporally stable scale (r = 0.83) for assessing maladaptive cognitions about sleep (Morin et al., 2007).
Sleep-threat monitoring was measured using three items taken from the Sleep-Associated Monitoring Index (SAMI; Semler and Harvey, 2004b), chosen to reflect three critical components of sleep-threat monitoring: attention to somatic sensations (an internal cue), attention to noises in the immediate environment (an external cue), and attention to the time it is taking to fall asleep (an additional major component of sleep-threat monitoring). The full-length SAMI has demonstrated good reliability and validity both before and after treatment for sleep disturbance (Semler and Harvey, 2004b).
Analyses
Analyses were conducted on an Intent to Treat (ITT) basis. Mixed model repeated measures (MMRM) analyses were used to account for missing data, with all available data included in the models. This approach yields unbiased estimates of intervention effects under the assumption that data were missing at random. An unstructured matrix was used and degrees of freedom were estimated using Satterthwaite’s correction.
Three analyses were undertaken: (1) a base model testing the effectiveness of the intervention on anxiety symptoms by comparing the two intervention groups across the three measurement time-points; (2) the addition into the model of the DBAS as an effect crossed with condition and time, to assess moderation of intervention effects by dysfunctional beliefs about sleep; and (3) the analogous addition of the SAMI to the base model, to assess moderation by initial levels of sleep associated monitoring. To illustrate the effects of dysfunctional beliefs and sleep-threat monitoring, marginal means were estimated based from these models, at two levels of DBAS-16 and SAMI scores to examine trajectories for low- and high-scoring participants using a median split.
Results
The majority of the sample was female (73.5%), well-educated (88.2% having completed post-secondary education), middle-aged, mean age = 42.7, standard deviation (SD) = 12.2, and living in urban areas (80%). More than half were employed fulltime (51.6%) and were either married or living in a defacto relationship (62.3%). Reflecting inclusion criteria, insomnia symptoms were high (mean ISI = 16.08) and anxiety/depression symptoms were elevated (mean PHQ-9 = 7.94; GAD7 = 5.8). Details of baseline characteristics are in Table 1. Further description of the sample is provided elsewhere (Christensen et al., 2015). Figure 1 shows the
Descriptive statistics based on experimental condition (N = 1149).
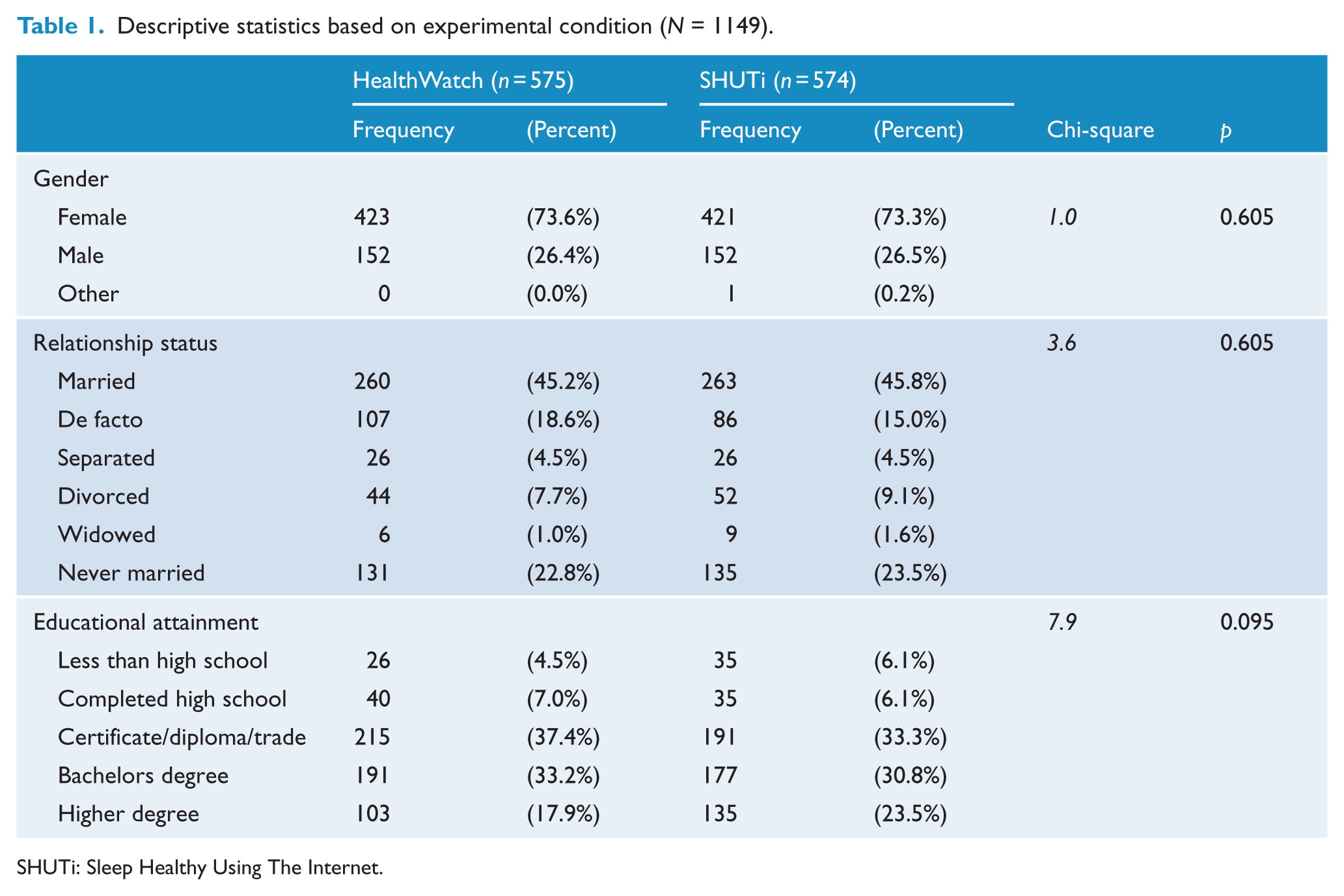
SHUTi: Sleep Healthy Using The Internet.
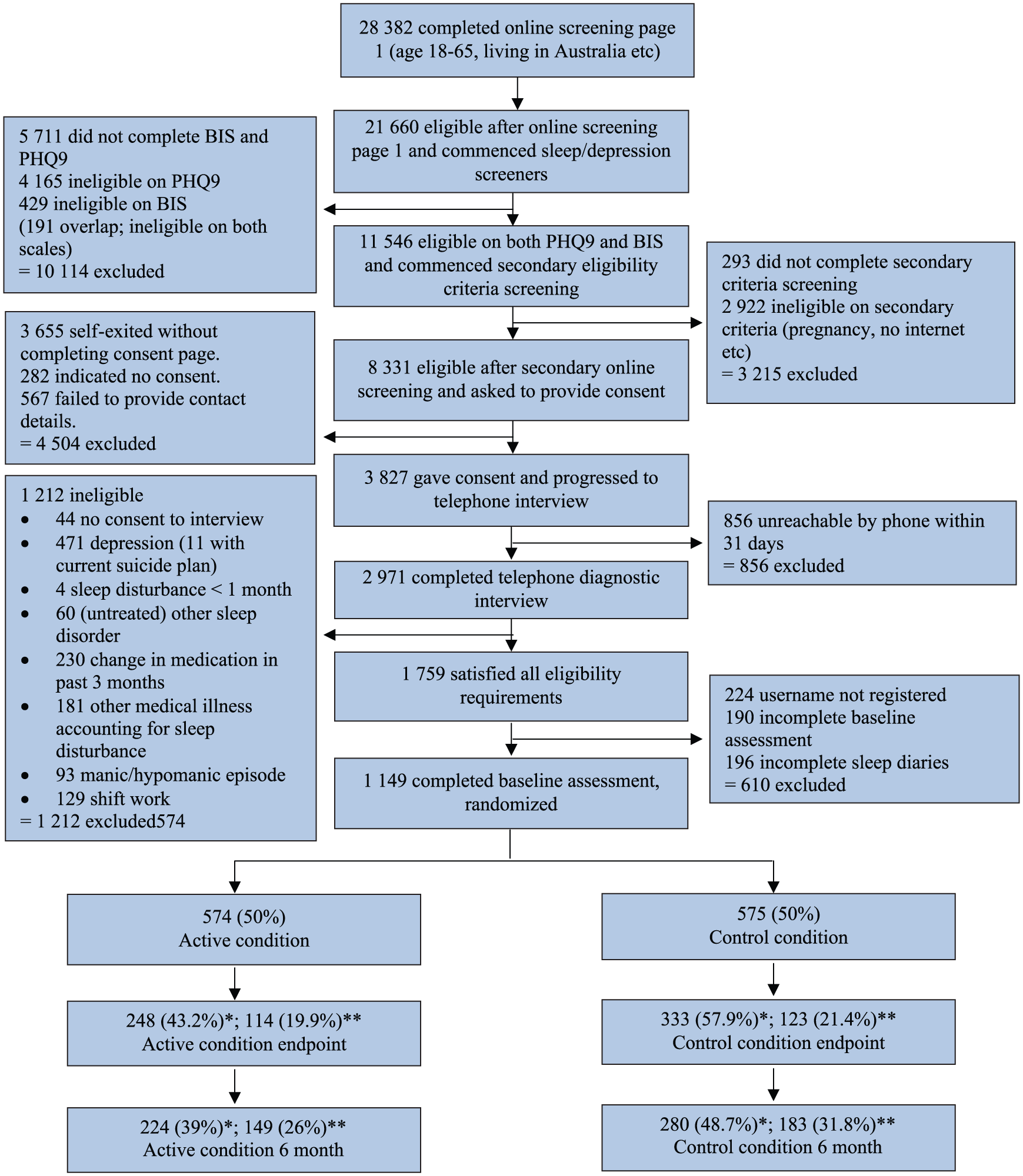
Consort diagram.
Based on GAD-7 scores at baseline, 45.3% of participants had minimal anxiety (0–4), 35.5% had mild anxiety (5–9), 13.8% had moderate anxiety (10–14) and 5.4% had severe anxiety (15–21). The previously reported fixed effects from the MMRM analyses, demonstrating that the SHUTi condition was significantly effective in reducing anxiety symptoms, are shown in Table 2 (Christensen et al., 2016). Specifically, anxiety symptoms were significantly reduced in the SHUTi condition relative to the HealthWatch condition: (F2, 624.46 = 23, p < 0.001), which was significant at both post-test (t724.27 = –6.77, p < 0.001) and 6-month follow-up (t700.67 = –4.27, p < 0.001). Both the intervention and control groups initially had estimated marginal mean scores in the ‘mild anxiety’ range (5.83 and 5.77, respectively; a score of 5 and above indicating ‘mild anxiety’ (Lowe et al., 2008)). At posttest, mean scores for intervention participants had decreased to ‘minimal anxiety’ (3.16) while control participants remained just below the ‘mild anxiety’ range (4.98). The effect size for the mean between-group difference at posttest was d = 0.37 (95% confidence interval [CI] = [0.25, 0.48]) and at 6-month follow-up was d = 0.24 (95% CI = [0.13, 0.36]). Figure 2 displays the means of GAD-7 scores for the two conditions at each timepoint.
Mixed-methods repeated measures analysis of GAD-7 outcome, with condition (SHUTi, control) and timepoint (pretest, posttest, 6-month follow-up) as predictors.
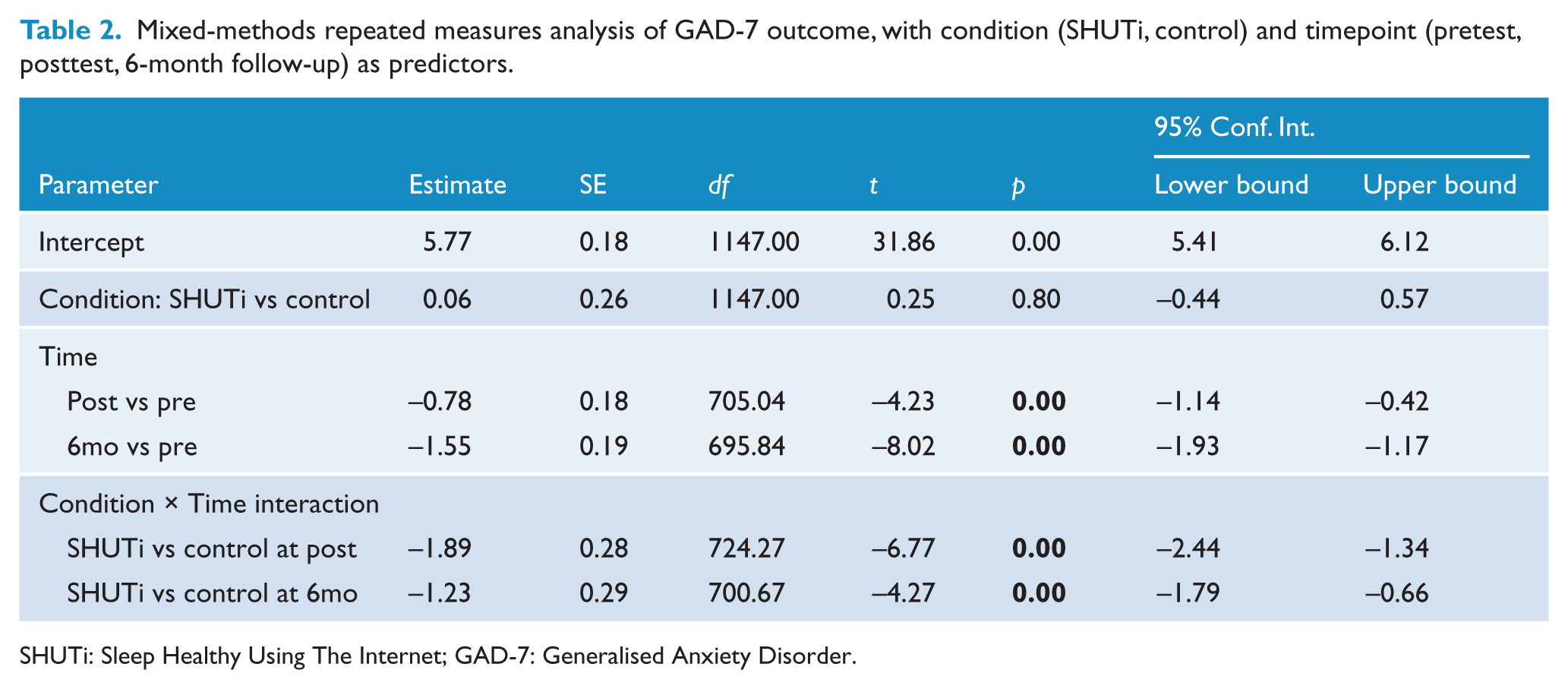
SHUTi: Sleep Healthy Using The Internet; GAD-7: Generalised Anxiety Disorder.
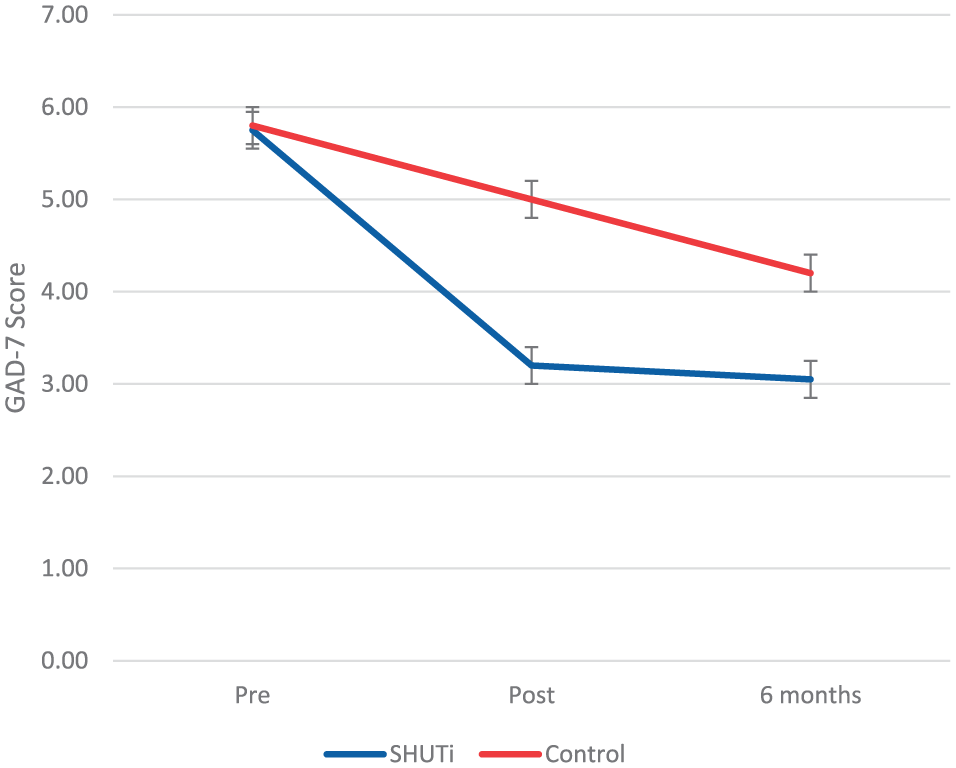
Mean GAD-7 scores for intervention (SHUTi) and control (HealthWatch) participants at pretest, posttest and 6-month follow up. Error bars indicate standard error.
Pre-test DBAS score significantly predicted GAD-7 outcome (F1, 959.99 = 117.99, p < 0.001), and the interaction of timepoint and DBAS score was significant (F2, 615.01 = 10.28, p < 0.001). The three-way interaction between dysfunctional beliefs about sleep, condition, and assessment was not significant (F2, 615.08 = .428, p = 0.65). Table 3 reports the estimates of fixed effects, and Figure 3 presents estimated marginal means for the two conditions across the three time points, assessed at two values of DBAS scores corresponding to a median split for illustrative purposes. Although Figure 3 suggests a difference at 6 months for the high DBAS group only, the overall three-way interaction effect based on the continuous DBAS measure (Table 3) was not significant, indicating no significant moderation.
Mixed-methods repeated measures analysis of GAD-7 outcome, with condition (SHUTi, control) timepoint (pretest, posttest, 6 month follow-up) and Dysfunctional Beliefs About Sleep score (high vs low) as predictors, including 2 and 3-way interactions.
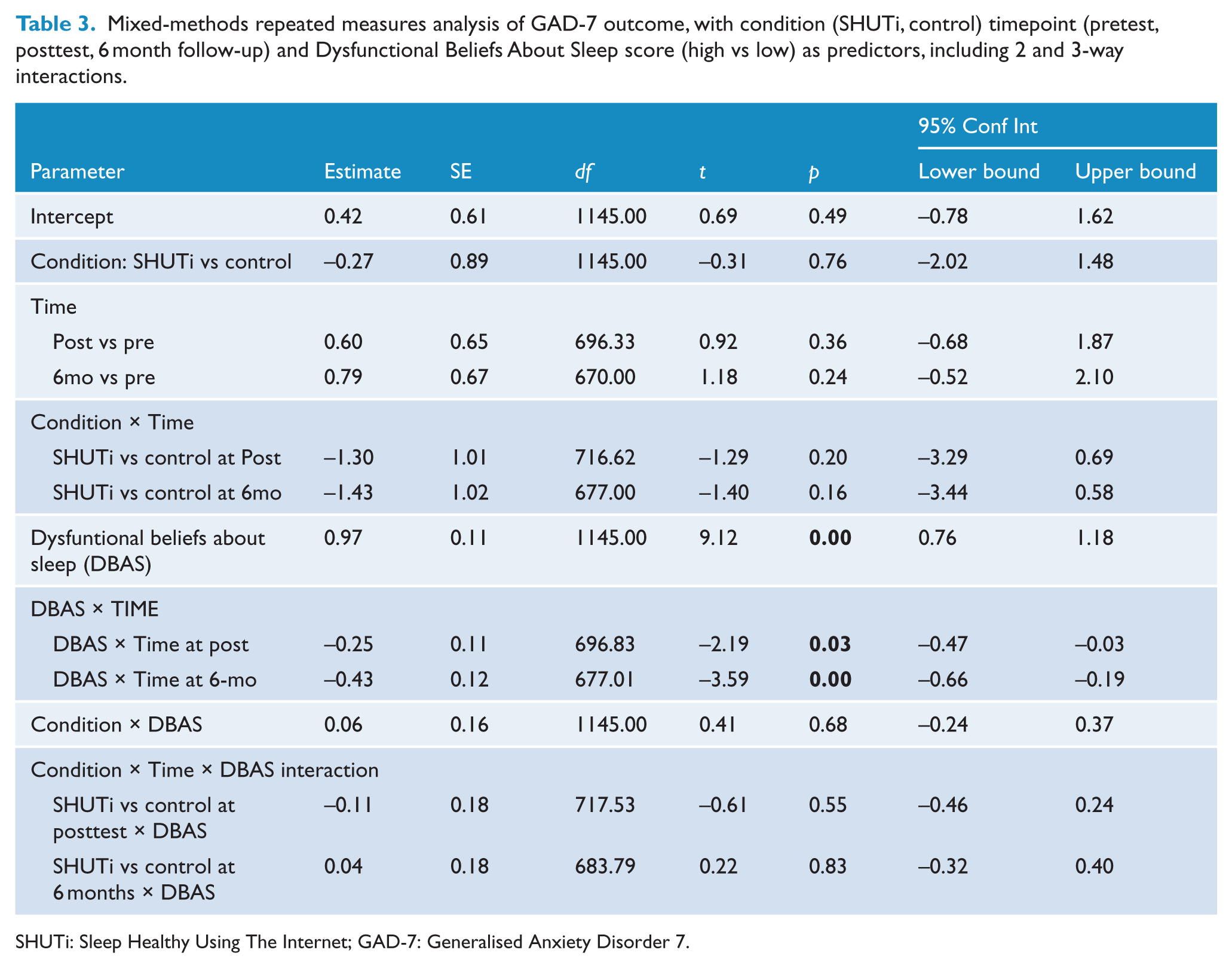
SHUTi: Sleep Healthy Using The Internet; GAD-7: Generalised Anxiety Disorder 7.
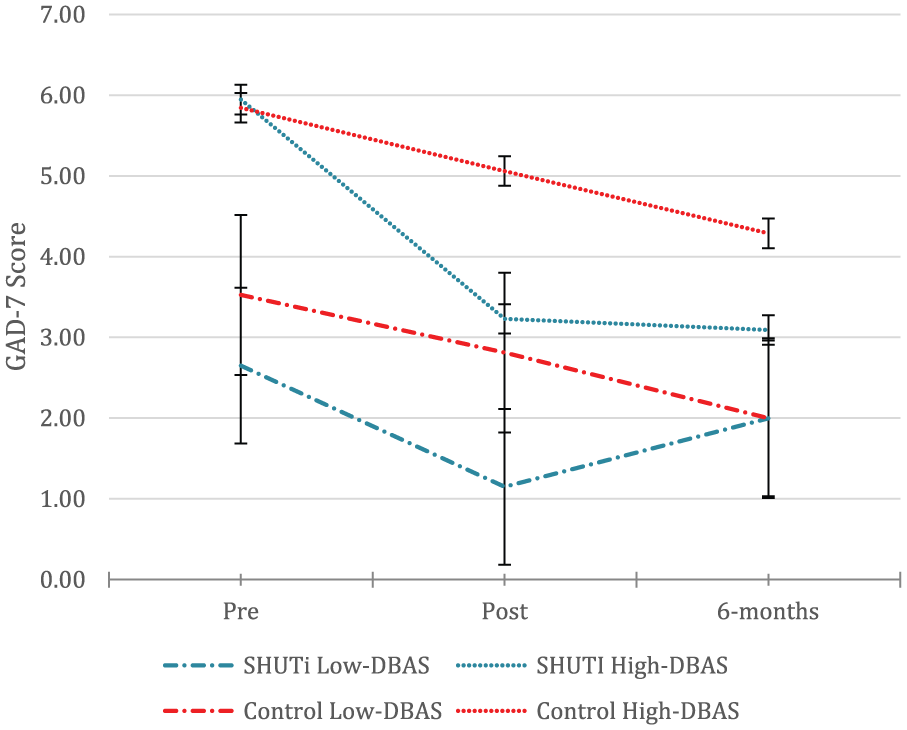
Three-way interaction between condition, time and Dysfunctional Beliefs About Sleep (DBAS) score (high vs low) on GAD-7 score. Error bars indicate standard error.
SAMI score significantly predicted GAD-7 outcome (F1, 995.84 = 42.14, p < 0.001), and the interaction between SAMI score and timepoint was significant (F2, 619.51 = 9.04, p < 0.001). The interaction between pre-test SAMI score, condition, and assessment was also significant (F2, 619.51 = 4.78, p < 0.01). Participants with higher initial SAMI scores in the intervention group showed a steeper reduction in anxiety than low-SAMI intervention-group participants from pretest to posttest (t713.69 = –2.39, p < 0.05) and through to 6 months (t694.77 = –2.98, p < 0.01). Table 4 displays the estimates of fixed effects, and Figure 4 represents estimated marginal means, assessed at two levels of SAMI score based on median split for illustrative purposes. This model was rerun controlling for baseline anxiety level. Baseline GAD-7 scores were dichotomised as high (10 or above) vs low (9 or below), and this factor was introduced as a main effect in order to test the possibility that this effect was driven primarily by presenting anxiety levels. The above three-way interaction remained significant, however (F2, 592.39 = 3.35, p < 0.05). The correlation between SAMI score and GAD-7 score at baseline was also low (r = 0.25), indicating that these are relatively independent.
Mixed-methods repeated measures analysis of GAD-7 outcome, with condition (SHUTi, control) timepoint (pretest, posttest, 6 month follow-up) and Sleep-Associated Monitoring Index score (high vs low) as predictors, including 2 and 3-way interactions.
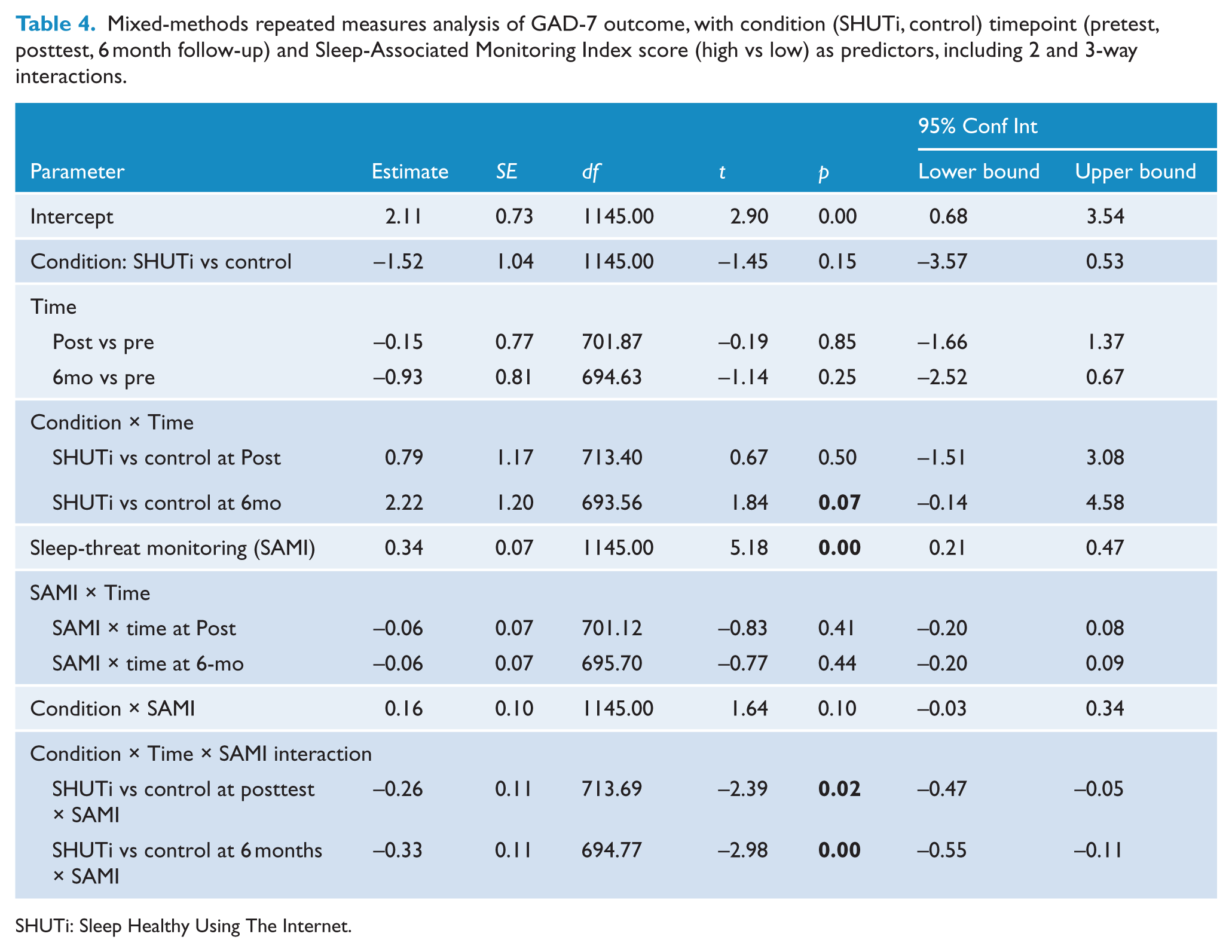
SHUTi: Sleep Healthy Using The Internet.
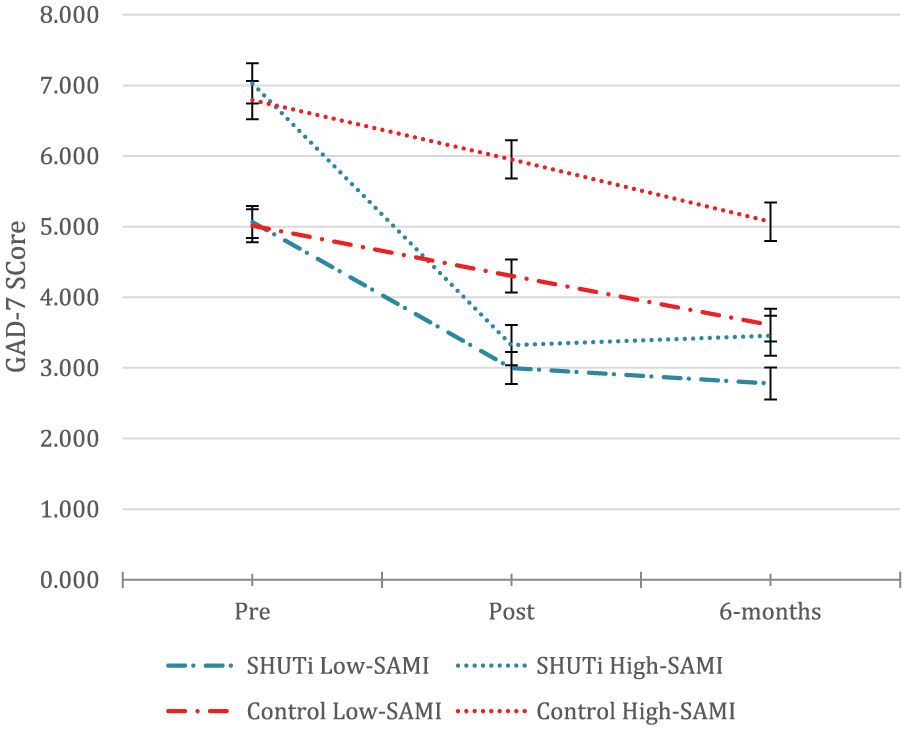
Three-way interaction between condition, time and SAMI score (high vs low) on GAD-7 score. Error bars indicate standard error.
Discussion
This study demonstrates that in treating sleep disturbance and insomnia, especially when anxiety is a concern, it is important to consider the moderating effects of cognitive-behavioural factors. In particular, pre-test level of sleep-threat monitoring, a cognitive-behavioural factor implicated in the maintenance of insomnia, is an important consideration. People who experienced higher levels of sleep-threat monitoring responded more strongly to the intervention than those with lower levels of pretest sleep-threat monitoring. Specifically, these participants’ anxiety levels showed a significantly greater reduction from pretest to posttest. This effect remained significant when baseline levels of anxiety were controlled, indicating that this finding cannot be simply attributed to anxiety. Furthermore, the correlation between SAMI and GAD-7 score at baseline was low, making it unlikely that the SAMI was simply a proxy measure of anxiety. Levels of pretest Dysfunctional Beliefs about Sleep, on the other hand, had no such impact on treatment outcome. In other words, participants receiving the CBT intervention showed a consistent reduction in anxiety across the study period irrespective of pretest levels of dysfunctional beliefs. This is also an important finding when it comes to considering the implementation of online CBTi, as it suggests that regardless of what people believe about their sleep and insomnia, this type of intervention can be effective.
The findings suggest that online CBT interventions for insomnia might be particularly useful for reducing anxiety among people whose insomnia is being maintained more strongly by active/behavioural factors, in this case sleep-threat monitoring, than by cognitive factors, such as dysfunctional beliefs about sleep. Further research is required to test this interpretation of the findings, specifically by identifying whether subtypes of insomnia might drive the development or maintenance of anxiety. If this were the case, it would be interesting in the context of Batterham et al. (2012) findings that rumination and neuroticism account for why sleep disturbance leads to depression but not why it leads to anxiety. It might be the case that while in people with sleep disturbance driven more by cognitive factors, such as rumination, depressive symptoms are more likely, those with more behavioural factors at play will display greater anxiety. This could inform more focused prevention for depression and anxiety. In terms of insomnia treatment, it is possible that approaches to treatment that are less intensive than a full course of CBTi might be sufficient for people with lower levels of sleep-threat monitoring. Knowledge of a person’s sleep-threat monitoring level might also allow tailoring of intervention content such that behavioural content is retained for high sleep-threat monitoring individuals, with others delivered a more cognitively focused package. As noted above, however, further research is needed before such conclusions are reached with any certainty.
In terms of cognitive models of sleep and insomnia, these findings regarding dysfunctional beliefs about sleep and sleep-threat monitoring provide important validation of the cognitive model proposed by Harvey (2002a), which has not previously been undertaken in the context of an intervention trial. For future exploration of the role of cognitive-behavioural factors in the association between insomnia and anxiety, the addition of a measure of safety behaviours in insomnia may provide further insight into the mechanisms driving reductions in anxiety (Harvey, 2002b; Ree and Harvey, 2004; Woodley and Smith, 2006). Sleep-related safety behaviours such as drinking alcohol to aid sleep, napping during the day or sleeping in – which were targeted through the intervention – would have been useful to systematically assess using a measure such as the Sleep-related Behaviour Questionnaire (SRBQ), and would be beneficial to include in further research. In either case, these findings suggest that screening for the cognitive-behavioural factors that are likely to be maintaining, or perpetuating, a person’s insomnia might be beneficial in predicting persons who will benefit most from intervention and potentially tailoring intervention content. Further investigation of the intervention elements that are most effective would be required to better enable tailoring of content to individual characteristics.
Strengths and limitations
This is the first test of whether treating insomnia using an online programme reduces anxiety symptoms in the context of a RCT. A large sample was recruited from the general population. As this online intervention is automated, it is highly scalable and therefore amenable to broad dissemination in the community.
Nevertheless, some limitations to the findings should be noted. In the context of this RCT focusing on depression prevention, the sample may have been somewhat truncated with respect to anxiety levels. Participants were selected based on scoring above a certain point on the PHQ-9, and were excluded if they met criteria of MDD in a telephone-administered clinical interview. Although selection and exclusion were not based on anxiety symptoms/disorders, the fact that depression and anxiety are often comorbid raises the possibility that some people with either low or markedly elevated anxiety symptoms were excluded from the study. However, GAD-7 scores at baseline indicated higher anxiety levels than would be expected in a community sample, with 13.8% and 5.4% reporting moderate or severe anxiety compared to population levels of 5% and 1%, respectively (Lowe et al., 2008). This, combined with the fact that 45.3% of participants fell in the minimal anxiety range suggests that the anxiety range was not markedly truncated. It was also the case that the current sample had a higher proportion of women. This is not unexpected given the higher prevalence of insomnia among women. There is a possibility that gender-based cognitive-behavioural differences exist, and although this study was not powered to examine gender interactions with cognitive-behavioural factors, further research exploring this issue may be warranted.
Sleep-threat monitoring was measured using three items taken from the SAMI, which have not been validated as a measure in isolation. Although these were selected to reflect central elements of sleep-threat, interpretation of results associated with sleep-threat monitoring must be undertaken with due caution. Dysfunctional beliefs about sleep and sleep-threat monitoring were measured for both experimental conditions only at baseline, precluding analysis of whether the intervention impacted differentially on these factors. It would be particularly interesting in future research to measure these factors throughout intervention, allowing lagged or dual change analyses, which could answer the question of whether cognitive or behavioural factors respond to intervention first, and thus to suggest a causal chain. It has been previously found that reductions in dysfunctional beliefs about sleep correlate significantly with reductions in insomnia as a result of CBT or combined CBT and pharmacotherapy (Morin et al., 2002), but future research that also targets, and measures, behavioural maintaining factors both at pre- and post-intervention would be beneficial. Despite the recruitment of a large sample, the larger targeted sample of 1,600 (Gosling et al., 2014) may have enabled greater power to examine response to the intervention, particularly given the need to investigate moderation using three-way or potentially four-way interaction terms. The current analysis looked at moderation by the above two cognitive-behavioural factors in isolation, and it is likely that there are multiple other moderators, including unmeasured ones. Power to isolate and detect these simultaneously, however, was limited.
This study found that online CBTi can be effective for reducing anxiety regardless of dysfunctional beliefs about sleep, but sleep-threat monitoring has a significant moderating effect. These findings have important implications for better targeting of insomnia treatment and anxiety prevention.
Footnotes
Acknowledgements
Ms Kanupriya Hehir, Ms Marina Talevski and Ms Jade Chan provided research assistance. Kylie Bennett and Anthony Bennett helped design the flow of the trial, and the software for the assessment and administration components. Dr Fiona Shand offered clinical support services to participants in the trial who sought more treatment. Professor John Cunningham facilitated trial communication. Helen Christensen is supported by National Health and Medical Research Council Fellowship Fellowship 1056964. Philip Batterham is supported by National Health and Medical Research Council Fellowship Fellowship 1083311. Kathleen Griffiths was supported by National Health and Medical Research Council Fellowship 1059620. The trial is registered with the Australian New Zealand Clinical Trials Registry (ANZCTR), registration number: ACTRN12611000121965.
Declaration of Conflicting Interests
Drs. Ritterband and Thorndike have equity ownership in BeHealth Solutions, LLC, a company developing and making available products related to the research reported in this publication. Specifically, BeHealth Solutions, LLC, has licenced the SHUTi programme and the software platform on which it was built from the University of Virginia. The terms of this arrangement have been reviewed and approved by the University of Virginia in accordance with its conflict of interest policy. The premise for the current research, including measures to include and how to analyse the data, was devised by Mr Gosling in line with his ongoing PhD research. Drs Ritterband and Thorndike provided input regarding design of the RCT, access to the intervention, theoretical interpretations of findings and accuracy of statements about the intervention. However, they were not involved in the day-to-day management of the RCT and were not involved in the statistical analyses.
Funding
The trial was funded by Australian NHMRC Project Grant 1005867.