
Abstract
Background:
The few studies of the recidivism by people with psychotic illness and cognitive disorder who are convicted of serious violent offences and sentenced by the courts.
Method:
Re-imprisonment data were obtained for 661 individuals convicted of serious non-lethal violent offences in the District Courts of New South Wales in the years 2006 and 2007. Rates of re-imprisonment of offenders known to psychotic illness or cognitive disorder (intellectual disability or acquired brain injury) was compared to those not known to have those conditions. A survival analysis was performed controlling for the effects of male sex, having a report by a mental health professional at the initial sentencing and receiving a custodial sentence for the initial offence.
Results:
There was no significant difference in the overall likelihood of further imprisonment between those with psychotic disorder (53.7%), those with cognitive disorder (50.7%) or among those with neither condition (45.2%; χ2 = 2.22, p = 0.33). A Kaplan–Meier analysis found that people with a psychotic disorder were returned to custody earlier than those not known to have psychosis (p = 0.002). People with psychosis spent a non-significantly greater time in custody (mean 477 days) than those with a cognitive disorder (mean 334 days) or among those with neither condition (mean 348 days) (Mann–Whitney Z-score = 1.5, η2 = 0.003, p value = 0.13). For the entire sample of 661 offenders, those who received non-custodial sentences for their initial offences had a lower likelihood of spending any time in custody in the follow-up period.
Conclusion:
The likelihood of returning to custody of sentenced violent offenders with psychotic illness or cognitive disorder is higher than that of released forensic patients in New South Wales followed up for a similar period. The results suggest an opportunity to improve the outcome of offenders with psychosis by better treatment and rehabilitation.
Introduction
It has been estimated that between 5% and 7% of prisoners in New South Wales (NSW) have schizophrenia (Nielssen and Misrachi, 2005), which is between 10 and 15 times greater than the estimated prevalence of schizophrenia among adults in the community of 0.46% (Saha et al., 2005). The proportion of serious violent offenders with schizophrenia is even higher. The rate of psychotic illness, mainly schizophrenia, among homicide offenders in NSW has been estimated to be 8.8% (Nielssen et al., 2007), and in a previous study of serious non-lethal violent offenders, charged with attempted murder, wounding and assaults resulting in serious injury, the proportion of the sample with a psychotic illness was 11% (Yee et al., 2011). Offenders with schizophrenia may also have a higher rate of re-offending, including violent reoffending (Grann et al., 2008), possibly because substance use and non-adherence to treatment increase the probability of violence among people with schizophrenia (Igoumenou et al., 2015). However, other studies have noted the similarities in the criminal histories, patterns of substance use and social disadvantage between offenders with schizophrenia and other offenders and that only a minority of offenders with psychosis had active symptoms at the time of the offence (Peterson et al., 2010).
The rates of reoffending among those found not guilty of an offence on the grounds of mental illness (NGMI), or to have reduced criminal responsibility in order to be rehabilitated to the community via secure psychiatric hospitals, are generally lower than those of other prisoners (Fazel et al., 2016; Hayes et al., 2014; Ong et al., 2009; Skipworth et al., 2006). In a previous study of violent recidivism among NSW forensic patients followed up for an average of 6 years after release, rates of recidivism were 3.1% among those granted conditional release and 4.7% among those granted unconditional release. None of the unconditionally released patients received a further not guilty due to mental illness (NGMI) verdict or were sentenced to a term of imprisonment (Hayes et al., 2014).
In contrast, the overall rate of reoffending after release from NSW prisons is very high, as about 45% of released prisoners return to prison within 2 years of release (Pauley and Holmes, 2015). While recidivism rate for forensic patients released from secure hospitals is known to be low, the comparable rate for serious violent offenders with psychotic disorder who were found guilty of an offence and rehabilitated through the NSW correctional system is not known.
In a previous study, we examined the rate of psychotic illness among a sample of 661 people charged with serious non-lethal violent offences and dealt with in the District Courts of NSW in the years 2006 and 2007 (Yee et al., 2011). The serious non-lethal violence was chosen as the subject of the original study because although there are numerous studies of homicide offenders with psychotic disorder, and also many studies reporting aggression and violence by people with psychotic illness in clinical settings, the role of psychotic illness in serious but not lethal violence is not well studied. These offences involved fall between homicide and the often minor assaults reported in clinical samples (Large and Nielssen, 2011). In our earlier study, a report by a mental health professional was found in the court files of more than half of the offenders in the sample. Based on the findings of those reports, 74 of the 661 (11%) had a diagnosis psychotic disorder, mostly schizophrenia. Of the 74, 7 (10% of those with psychosis or 1% of the total sample) were found to be NGMI, while the remaining 67 were sentenced, in most cases to terms of imprisonment. There were also 73 offenders diagnosed with a cognitive disorder (defined as an acquired brain injury or intellectual disability).
In this study, we conduct a survival analysis to examine re-imprisonment and the amount of time spent in custody after release among those diagnosed with a psychotic disorder and a cognitive disorder and among those without either condition over a period of follow-up of between 8 and 10 years. We controlled for male sex, receiving a custodial sentence for the initial offence and whether a report was prepared by a mental health professional for the initial offence, on the likelihood of re-imprisonment.
Methods
Recidivism data
The methods for selecting and analysing the sample are described in detail in the original paper (Yee et al., 2011). The seven offenders found NGMI were excluded. The Bureau of Crime Statistics and Research (BoCSaR) has a comprehensive re-offender database (ROD) that records, among other information, the sentences imposed and the dates of release and return to custody of convicted offenders. ROD entries for the original sample of 661 were provided up to 31 December 2015 or between 8 and 10 years after the court verdicts for the serious violent offences that led to inclusion in the original study. For the purpose of this study, we only considered return to custody and the time spent in custody and did not consider convictions that resulted in non-custodial sentences or whether the period in custody was followed by an acquittal.
The diagnoses made in the original reports were recorded by N.Y. and O.N., and the data sheets from the original study were re-examined by O.N., to include the diagnoses of brain injury and intellectual disability. For the purpose of the analyses, 12 offenders with overlapping diagnoses were included in both groups. The difference between the date of release following any sentence imposed for the index offence and first return to prison were subtracted to calculate time at liberty, and the total number of days spent in custody was recorded for those who returned to custody.
Approval to conduct the follow-up study was obtained from Human Research and Ethics Committee of the University of Sydney (Ref. No. 2015/917).
Statistical analysis
The likelihood of a further custodial sentence following release with a diagnosis of psychotic disorder, cognitive disorder, and those without a psychotic or cognitive disorder was examined using chi-square distribution tests and Kaplan–Meier survival methods. The likelihood of later custody and the subsequent days in custody among people with psychotic disorder, cognitive disorder and those without a psychotic or cognitive disorder who received or did not receive an initial custodial sentence was examined in those using chi-square and Mann–Whitney statistics. A Cox proportional-hazard survival analysis was performed to examine the independence of psychotic disorder and cognitive disorder on re-imprisonment, controlling for male sex and the presence of a report by a mental health professional and an initial custodial sentence.
Time spent in custody after returning to custody was examined among those with a psychotic disorder, those with a cognitive disorder and those with neither disorder was not normally distributed and was examined with a Mann–Whitney U test. Those with both a psychotic disorder and a cognitive disorder were double counted in both chi-square tests and Mann–Whitney tests with the conservative effect of lessening the statistical power to discern differences according to these two diagnoses. People who did not return to custody were scored as having zero days in custody.
Results
Among the 661 people convicted of a serious non-lethal violent offence in the NSW District Courts in 2006 and 2007, 67 (10.1%) were known to have a psychotic illness. Of these, 49 received a custodial sentence and 18 received non-custodial sentences ranging from periodic detention (available as a sentencing option at that time), suspended sentences, good behaviour bonds with and without conditions, community service orders and fines.
Over the whole period of follow-up, there were no significant differences in rates of further imprisonment between those with psychotic disorder (53.7%), those with cognitive disorder (50.7%) or among those with neither condition (45.2%) as assessed as chi-square distribution (χ2 = 2.22, p = 0.33). Once returned to custody, people with psychosis spent non-significantly more days in prison than those without psychosis (Table 1, η2 = 0.003, p value = 0.13). An initial custodial sentence was associated with more days in further custody among people with psychosis, with cognitive disorder and among those without these diagnoses, and was associated with an increased risk of further custody among those without psychosis and those with a psychotic or cognitive disorder (Table 1).
Comparison of subsequent custody within diagnostic groups for those with and without an initial custodial sentence.
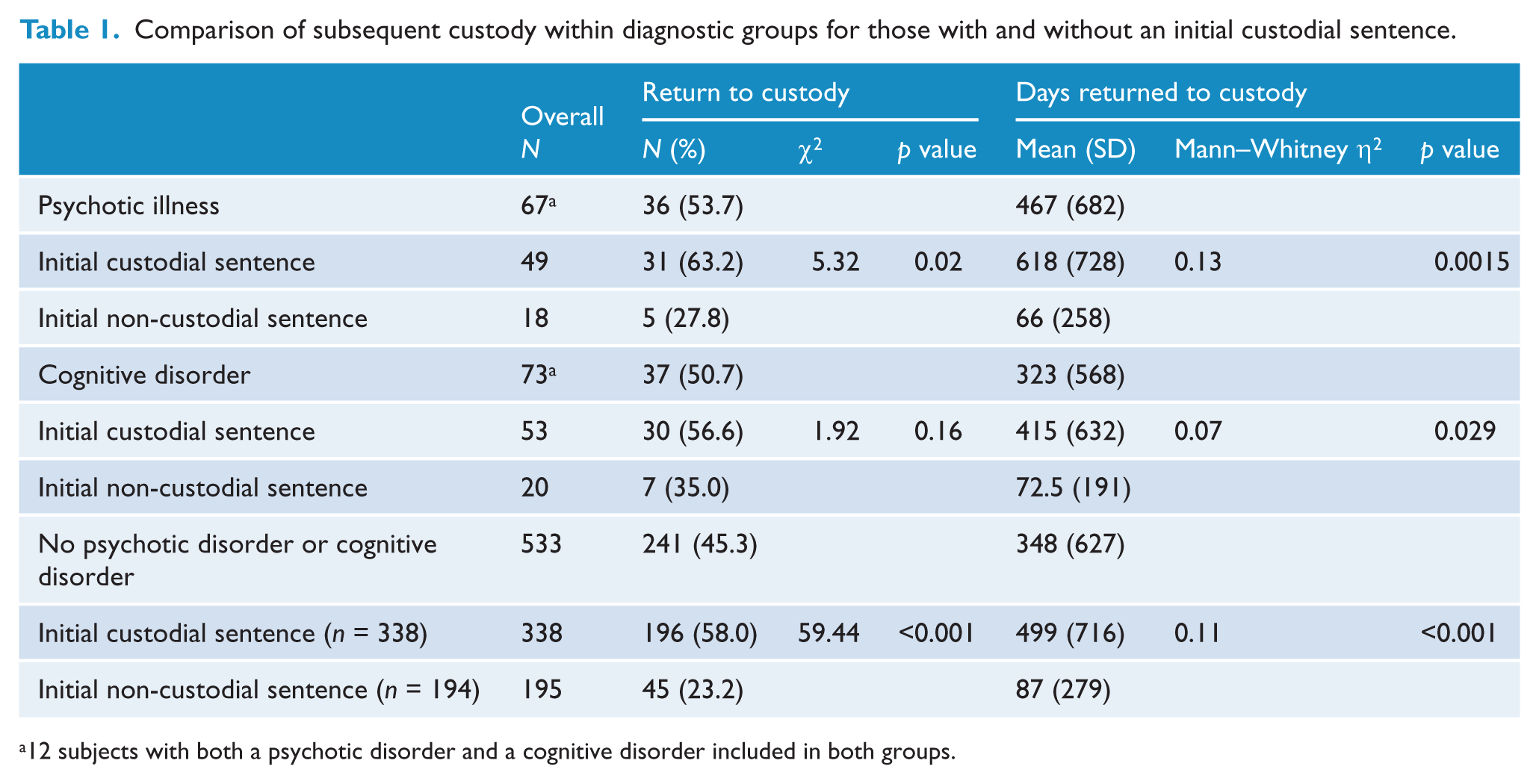
12 subjects with both a psychotic disorder and a cognitive disorder included in both groups.
Although people with psychosis did not have significantly increased risk of return to custody over the whole period of follow-up, Kaplan–Meier estimates of survival found that people with psychosis returned to custody sooner (mean 1554 days, 95% confidence interval [CI] = [1237, 1867], median 958) than those without psychosis (mean 1926 days, 95% CI = [1816, 2036], median 2372, χ2 = 9.2, p = 0.002; Figure 1).
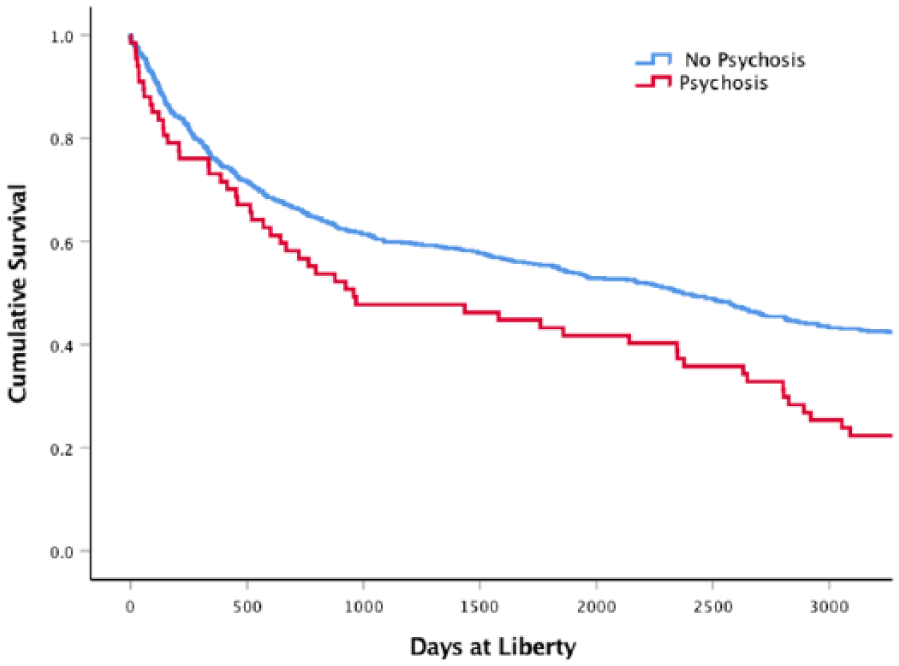
Survival analyses comparing offenders with psychotic illness and other offenders.
Kaplan–Meier estimates found that people with intellectual disability or brain damage were not more likely to be returned to custody sooner (mean 1734 days, 95% CI = [1408, 2060], median 1428) than those without these disorders (mean 1907 days, 95% CI = [1799, 2017], median 2324, χ2 = 0.33, p = 0.56; Figure 2).
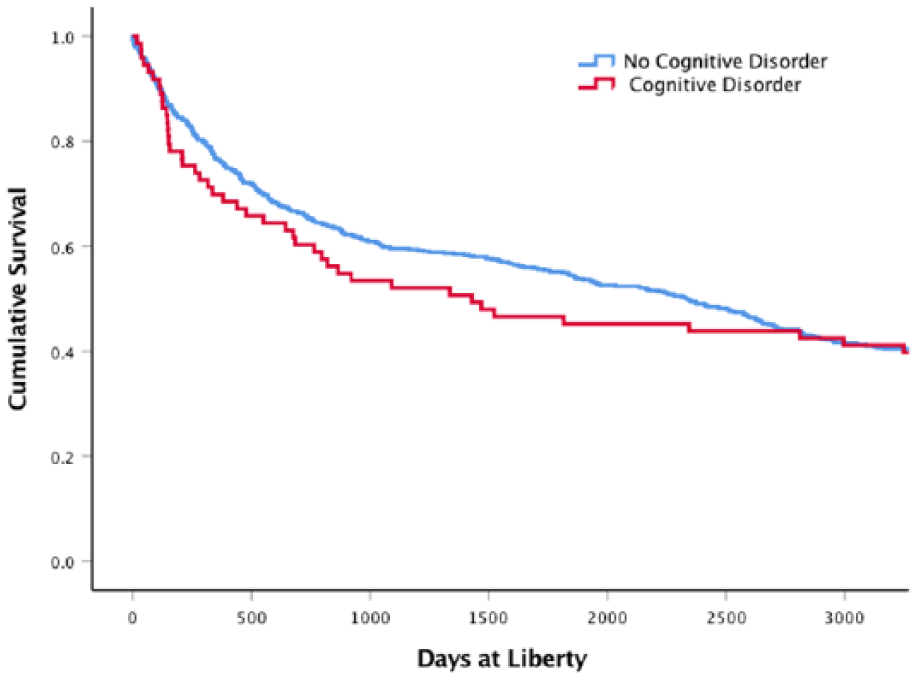
Survival analyses comparing offenders with cognitive disorder and other offenders.
People who had an initial custodial sentence were significantly more likely to return to custody sooner (mean 1462 days, 95% CI = [1334, 1548], median 890) than who did not receive a custodial sentence (mean 2689 days, 95% CI = [2546, 2831], median 3285, χ2 = 153, p < 0.001; Figure 3).
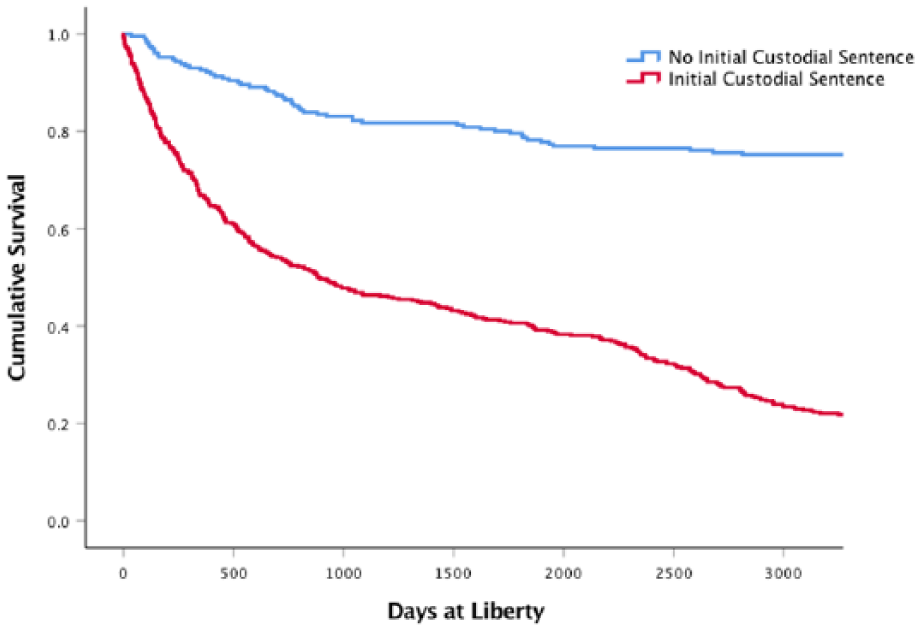
Survival analyses comparing offenders who received an initial custodial sentence and those who received a non-custodial sentence.
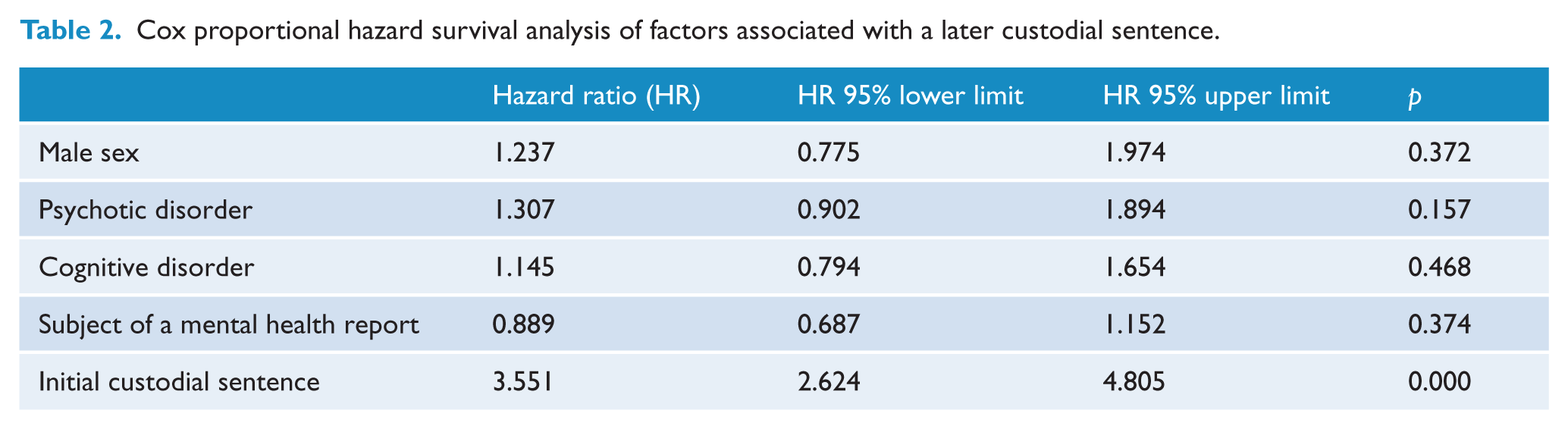
A multivariate Cox proportional-hazard survival analysis examined the hazards of psychosis, a cognitive disorder, controlling for effect of an initial custodial sentence, male sex and the presence of a report by a mental health professional, suggested that having had an initial custodial sentence was the only independent hazard for a further return to custody (Table 2).
Cox proportional hazard survival analysis of factors associated with a later custodial sentence.
Discussion
Serious non-lethal violent offenders with either a psychotic illness or a cognitive disorder at the time they were sentenced by the District Court in NSW were very likely to return to prison after release and spent long periods in prison. Prisoners known to have a psychotic illness were no more likely to be re-imprisoned, but were returned to custody sooner and spent a non-significantly greater number of days in custody. The similarity in the overall rates of recidivism are not entirely surprising, because the demographic and criminological characteristics of the sample of offenders with psychotic disorder were similar to those of offenders without psychotic illness (Yee et al., 2011), and the arrangements for ensuring adherence to parole conditions, which generally include adherence to treatment, abstinence from substances and leading a law abiding lifestyle, are not especially successful (Pauley and Holmes, 2015). The overlap in the criminological characteristics of the psychotic and non-psychotic offenders included a high proportion of males, a high rate of previous convictions, more offenders of indigenous heritage and a high rate of comorbid substance use disorder and intoxication at the time of the original offence than that of Forensic Patients (Hayes et al., 2014; Yee et al., 2011). In the original study by Yee et al., 58 (78.4%) were reported to have acute symptoms of psychosis that contributed to the offending. However, other studies have reported that acute symptoms were not present at the time of most offences committed by released prisoners with serious mental illness, and the majority of recidivist offences appeared to be due to combinations of other criminogenic factors (Peterson et al., 2010, 2014).
The offenders who received non-custodial sentences at the time of the initial sentence were significantly less likely to return to custody and spent less time in custody on average. The most likely reason for this difference is that the those sentenced to a term of imprisonment were already repeat offenders, or had committed more serious offences and were hence more likely to reoffend. It is also likely that the judicial officers were good at assessing the probability of reoffending in much the same way as the decisions regarding conditional release of Forensic Patients have been shown to be sound (Hayes et al., 2014; Skipworth et al., 2006). The absence of a significant difference for those with psychosis and cognitive disorder might have been because the presence of those conditions reduced their likelihood of receiving an initial custodial sentence. Nevertheless, these explanations do not exclude the possibility that being sentenced to prison itself increased the likelihood of returning to custody.
The over-representation of people with schizophrenia in the prison population, the high probability of return to custody, their earlier return to custody and the longer time spent in custody raises the important question as to whether better systems of care might reduce all of these figures. The low rates of recidivism by Forensic Patients suggest that the elements of rehabilitation could be successfully applied to mentally ill offenders sent to prison. The first element would be improved systems of ensuring adherence to treatment with antipsychotic medication after release from prison. A recent study from Canada showed that lack of adherence to treatment was associated with violent recidivism by released prisoners with schizophrenia (Rezansoff et al., 2017), and a population-based study from Sweden showed a similar association between collecting prescriptions for antipsychotic medication and the likelihood of further violent offences (Chang et al., 2016). At present, mentally ill offenders are often released from low security prisons in remote locations with a social security payment and a few days supply of medication, without clear arrangement for accommodation or further mental health care. In the original study, only 16% of the offenders with an established diagnosis of psychosis were adherent to treatment and not surprisingly most reported active psychotic symptoms at the time of their offences (Yee et al., 2011).
Another element of the successful rehabilitation of forensic patients is close monitoring of abstinence from illegal drugs and alcohol, as part of the conditions of release. There are very high rates of comorbid substance use and all forms of mental disorder among NSW prisoners (Butler et al., 2011), and substance use is known to be associated with an increased probability of violent recidivism in people with schizophrenia (Igoumenou et al., 2015). The circumstances of supervision of abstinence from substance use among released prisoners is different to those of Forensic Patients, as the requirement for drug testing can only be enforced for the duration of parole, which can often be quite short.
A third element of the successful rehabilitation of Forensic Patients is graded release and the careful consideration of the circumstances into which those patients will live in the community, whereas many mentally ill prisoners are released with no fixed abode. More than a quarter of homeless hostel clinic attenders had been released from prison to homelessness, a half of whom had psychotic illness (Nielssen et al., 2018). Having a place to live greatly improves the likelihood of engaging with a local mental health service, and stable housing has been shown to improve adherence to treatment (Rezansoff et al., 2016). The interface between prison and the community is an area that is difficult to accommodate within the security requirements of the prison system. A model that might meet with some success is the Compulsory Drug Treatment Correctional Centre (CDTCC; Birgden and Grant, 2010), which includes a pre-release focus on optimal treatment for substance use, supervision of abstinence and graded release during the last stage of the programme, which could be easily applied to making accommodation and follow-up arrangements for mentally ill offenders.
In some ways, the cost of imprisonment at an average of AUD301 per night (Productivity Commission, 2017) can be viewed as an inexpensive form of institutional care when compared to the cost of a secure hospital bed of AUD1073 per night (Mental Health Services Australia, 2017). However, the 31 offenders with psychotic illness spent a total of 16,812 further days in custody during the follow-up period at a cost of around AUD160,000 per offender for imprisonment alone, matched by the roughly equivalent amount for police investigation, legal representation and court costs (Lin et al., 2015). The very low rate of recidivism of conditionally released forensic patients suggests that applying some of the elements of successful rehabilitation of those patients to mentally ill offenders would be both more humane and cost-effective.
Limitations
There are a number of limitations to this study. The most obvious is that nothing is known about the nearly half of the offenders who did not have an assessment by a mental health professional prior to their sentencing. It is likely that this group included offenders with significant psychiatric disorders, based on the low sensitivity of initial screening for psychiatric disorder (Nielssen and Misrachi, 2005). It is also likely that a number of offenders developed psychotic illness or sustained a brain injury during the 8–10 years of follow-up. A further limitation is that we did not consider the amount of time spent on remand prior to the initial sentencing date, as about a third of prisoners in NSW are yet to be sentenced. Moreover, we only examined return to custody, which included some periods as short as 1 day, despite the long mean figures, rather than reconviction, or the nature of the further charges. The data provided by BoCSaR included reconviction, which showed that a number of those who returned to custody were convicted of offences that did not result in a term of imprisonment, and some of those who returned to custody did not have a further conviction. Another limitation is that the sample sizes for the groups diagnosed with psychotic illness and cognitive impairment was small, and the study may have lacked the statistical power to demonstrate significant differences between the groups. A further consideration is the differences in the symptoms and circumstances of the psychotic offenders found NGMI and psychotic offenders dealt with by the courts, who are more like other offenders, and hence might not be as responsive to attempts to reduce recidivism through better systems of care.
Implications
The main implication of the study is that investment in the long-term treatment, supervision and rehabilitation of violent offenders with psychotic illnesses may be warranted, given the very high rate of reoffending and the high cost of recidivism in this group and the comparatively low rates of recidivism by forensic patients who receive that kind of care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.