
Abstract
Objectives:
This study investigated whether there were differences in coping strategies and self-esteem between offspring of parents with bipolar disorder (high-risk) and offspring of unaffected parents (control), and whether these psychological factors predicted the onset and recurrence of mood episodes.
Methods:
High-risk and control offspring were followed longitudinally as part of the Flourish Canadian high-risk bipolar offspring cohort study. Offspring were clinically assessed annually by a psychiatrist using semi-structured interviews and completed a measure of coping strategies and self-esteem.
Results:
In high-risk offspring, avoidant coping strategies significantly increased the hazard of a new onset Diagnostic and Statistical Manual of Mental Disorders, 4th Edition twice revised mood episode or recurrence (hazard ratio: 1.89, p = 0.04), while higher self-esteem significantly decreased this hazard (hazard ratio: 2.50, p < 0.01). Self-esteem and avoidant coping significantly interacted with one another (p < 0.05), where the risk of a Diagnostic and Statistical Manual of Mental Disorders, 4th Edition twice revised new onset mood episode or recurrence was only significantly increased among high-risk offspring with both high avoidant coping and low self-esteem.
Conclusion:
A reduction of avoidant coping strategies in response to stress and improvement of self-esteem may be useful intervention targets for preventing the new onset or recurrence of a clinically significant mood disorder among individuals at high familial risk.
Introduction
Bipolar disorder (BD) refers to a heterogeneous group of heritable, persistent or recurrent, psychiatric illnesses associated with substantial individual and familial burden (Judd et al., 2005). BD represents a diagnostic challenge, with accurate identification occurring on average 10 years after first contact with primary care (Hirschfeld et al., 2003). Findings from high-risk offspring studies have enriched our understanding of the clinical trajectory of emerging BD and the early course after the first hypomanic or manic episode (Duffy et al., 2014; Hafeman et al., 2016; Mesman et al., 2013; Preisig et al., 2016). Yet, specific early intervention targets have not been identified, and uncertainty remains as to why some individuals at high familial risk develop mood disorders, while others do not (Duffy et al., 2016b; Mcgorry and Nelson, 2016; Rice, 2010).
BD tends to onset in adolescence and early adulthood, an important period of biological, social and psychological development (Angst and Gamma, 2008; Paus et al., 2008), underscoring the importance of studying antecedent risk factors predicting the onset of illness (Duffy, 2015; Kapczinski and Streb, 2014). BD is likely the result of multiple susceptibility genes interacting with other vulnerability factors to determine illness onset (Heim, 2012). Psychological risk factors have been studied extensively in clinical populations with unipolar depression and adults with BD and have proven useful as targets for intervention (Alloy et al., 1988; Bentall et al., 2005; Bortolotti et al., 2008; Duffy et al., 2016a; Hammen, 2003; Jones, 2004). In comparison to the unipolar depression literature, there has been little investigation into how psychological constructs modify the association between genetic susceptibility and the subsequent development of mood disorders. Yet, these constructs may be of similarly high clinical utility in populations of offspring at familial risk of bipolar mood disorders.
Offspring of parents with mood disorders appear to be more sensitive to stress, as evidenced by a high emotionally reactive temperament (Doucette et al., 2013; Ostiguy et al., 2009). As a result of this vulnerability, it is plausible that high-risk individuals cope with stress differently or less effectively compared to individuals at lower familial risk, increasing the likelihood of developing mood psychopathology. Indeed, there is evidence from cross-sectional studies, supporting that offspring of BD parents (high-risk offspring) use more distraction and ruminative coping strategies than controls, and among high-risk offspring with a lifetime history of mood disorder, these coping strategies are more pronounced relative to unaffected high-risk offspring (Jones et al., 2006; Nijjar et al., 2014). Furthermore, self-esteem has been found to be less stable in high-risk offspring compared to controls (Jones et al., 2006) while, in offspring of depressed mothers, higher self-esteem is a robust predictor of resilience and high functioning into adulthood (Lewandowski et al., 2014). In a recent experience sampling study, it was found that decreases in self-esteem predicted excessive risk-taking in the offspring of BD parents and that these children had reduced ability to use active (adaptive) coping strategies when experiencing negative affect (Pavlickova et al., 2015). However, these processes have yet to be studied using long-term longitudinal designs appropriate for investigating causality.
In this paper, we report findings from a longitudinal high-risk dynamic cohort study of the offspring of well-characterized bipolar parents, investigating whether there were differences in coping strategies and self-esteem between high-risk offspring and controls, and whether these psychological factors predicted the subsequent onset of diagnosable mood episodes in offspring of parents with confirmed BD.
Materials and methods
Recruitment of participants
High-risk and control offspring were participants of the Flourish Canadian high-risk bipolar offspring cohort study, described in detail elsewhere (Duffy et al., 2010, 2014). Briefly, high-risk offspring were recruited from parents confirmed to meet Diagnostic and Statistical Manual for Mental Disorders (4th ed. twice revised; DSM-IV) criteria for lifetime BD I or II based on a wealth of prospective clinical information and Schedule for Affective Disorders–Lifetime (SADS-L; Endicott and Spitzer, 1978) format research assessments confirmed by a best estimate diagnostic procedure involving at least two additional research psychiatrists. The other biological parent was confirmed to have no DSM-IV Axis I or II psychiatric disorder (i.e. no psychotic, mood, substance use or personality disorder) based on SADS-L interview at baseline. Affected parents typically derived from multiplex families participating in neurobiological and genetic studies were recruited from a specialty mood disorder program in Ottawa. Control offspring were recruited from local schools in Ottawa from parents confirmed to have no Axis I DSM-IV lifetime psychiatric disorder at baseline as determined by semi-structured SADS-L (Endicott and Spitzer, 1978) format research interviews by a psychiatrist and blind consensus review again by a panel including at least two research psychiatrists.
Procedure
High-risk and control offspring who completed the psychological measures of interest were selected for this study. Offspring were recruited as identified and were between the ages of 5 and 25 years at baseline. This study is an open, dynamic cohort design, where participants enter at different ages and times. All consenting/assenting offspring were clinically assessed on average annually by a child and adolescent psychiatrist using the Kiddie SADS-present (P)L (Axelson et al., 2003)/SADS-L (Endicott and Spitzer, 1978) (depending on age) format semi-structured research interviews. DSM-IV diagnoses were confirmed through a blind consensus review involving two additional research psychiatrists. During the annual research visits, when well or in clinical remission, offspring completed a measure of coping strategies and self-esteem. Socio-economic status (SES) was collected in parents at baseline using the Hollingshead SES scale (Hollingshead, 1970), a validated composite measure of education and occupation in both working spouses. This study was approved by the local Independent Research Ethics Board in Ottawa, Ontario and funded by a grant from the Canadian Institutes of Health Research (MOP 102761).
For this study, we used a subset of data from participants who completed the psychological self-report measures of coping strategies and self-esteem (n = 224). This subset represented 63% of the original sample (n = 356) at the time of this analysis. Sensitivity analyses were conducted to determine if those not completing these specific measures were different on important characteristics compared to those completing them. All high-risk and control offspring were in clinical remission from major mood episode and other psychiatric comorbidities when completing these psychological measures confirmed on clinical research assessment by a psychiatrist and Beck Depression Inventory-II (BDI-II) score (Beck et al., 1996).
Measures
Coping strategies were measured using the Children’s Coping Strategies Checklist–Revised (CCSC-R; Ayers and Sandler, 1999). The CCSC-R is a 54-item self-report measure of coping strategies where respondents were asked to rate on a scale from 1 (never) to 4 (most of the time) how they coped with a stressful event that occurred in the past 12 months. For this analysis, the four subscales: active coping (problem-solving and positive thinking), distraction (distraction actions and physical release of emotions [e.g. exercise]), avoidance (avoidant actions, repression and wishful thinking) and support seeking (seeking support for actions and feelings) were used. Higher scores indicate higher levels of each of these coping strategies. This measure has demonstrated good internal consistency and validity on all subscales (α = 0.72–0.88) in children and adolescents (Ayers and Sandler, 1999).
Self-esteem was measured using the Rosenberg Self-Esteem Scale (RSES) (Rosenberg, 1965) which is a 10-item self-report measure of positive and negative feelings toward the self. Respondents were asked to rate how much they agree with each statement using a 4-point Likert scale. Higher scores indicate higher self-esteem. The RSES has established acceptable reliability and validity (α = 0.77–0.88; Rosenberg, 1986).
Clinical assessments were conducted using the Kiddie (KSADS-PL; Axelson et al., 2003) and the SADS-PL (Endicott and Spitzer, 1978) semi-structured interviews depending on the age of the offspring. The BDI-II (Beck et al., 1996) was used as a supplementary clinician-rated measure to confirm clinical remission between episodes during measure completion. The BDI-II is a 21-item, well-validated and reliable measure of depressive symptoms which rates the severity of current depressive symptoms on a scale ranging from 0 (least severe) to 3 (most severe) in accordance with DSM-IV diagnostic criteria. Cronbach’s alpha are typically >0.90 (Beck et al., 1996).
Outcome
The outcome was defined as a first mood episode onset meeting full DSM-IV criteria (major depression, mania, hypomania, BD not otherwise specified [NOS], depression NOS, dysthymia, cyclothymia) or a recurrence of a mood episode among offspring who already had experienced an index episode but were in clinical remission. Temporality was ensured by excluding any cases in which the psychological measures were completed after the onset or recurrence of mood episodes.
Data analysis
Descriptive characteristics were estimated using chi-square tests, Fisher’s exact tests and t-tests where appropriate. To estimate differences in psychological scores between high-risk and control offspring, linear mixed regression models were used to account for potential clustering within families. All regression models were adjusted for sex and age at first interview. To estimate the association between the psychological factors and first onset mood episode or recurrence, separate Cox Proportional Hazard models were calculated producing hazard ratios (HR) and corresponding 95% confidence intervals (CI). Date of birth to the date of mood episode onset was used as the time period owing to the open, dynamic design of this prospective cohort study, where, participants enter at different ages. Participants were censored at date of last assessment. All Cox models were adjusted for sex and sibling correlation (Lin and Wei, 1989) to account for potential clustering within families. Interaction between factors was tested by adding statistical interaction terms to models, and effect modification was explored through estimating stratum-specific HR using the ‘ESTIMATE’ command which produces group specific HR while accounting for the other covariates in the model. A final model of risk was estimated using a manual backward selection approach. Predictors were removed one at a time starting with the largest p-value and their contribution to the model was tested using the likelihood ratio test. All model assumptions were verified using graphical techniques and all analyses were performed using SAS software (Version 9.4).
Results
Descriptive characteristics
The subset sample included 224 offspring (144 high-risk and 80 control). While 224 offspring completed the CCSC-R, 185 completed the self-esteem measure. There were no significant differences (all p > 0.05) in Table 1 characteristics in these subset samples compared to each other, as well as compared to the original cohort (data not shown). The mean age in years when completing the CCSC-R and RSES in high-risk offspring was 20.5 (standard deviation [SD] = 5.2) and 24.9 (SD = 5.8), and in control offspring was 15.8 (SD = 2.1) and 21.1 (SD = 5.8), respectively. Among those completing the CCSC-R, the age in years at last assessment in high-risk offspring was 26.9 (SD = 6.0) and in controls was 20.6 (SD = 3.9), and among those completing the RSES, the age in years at last assessment in high-risk offspring was 26.9 (SD = 6.0) and 23.0 (SD = 2.7) in controls.
Descriptive characteristics of the cohort.
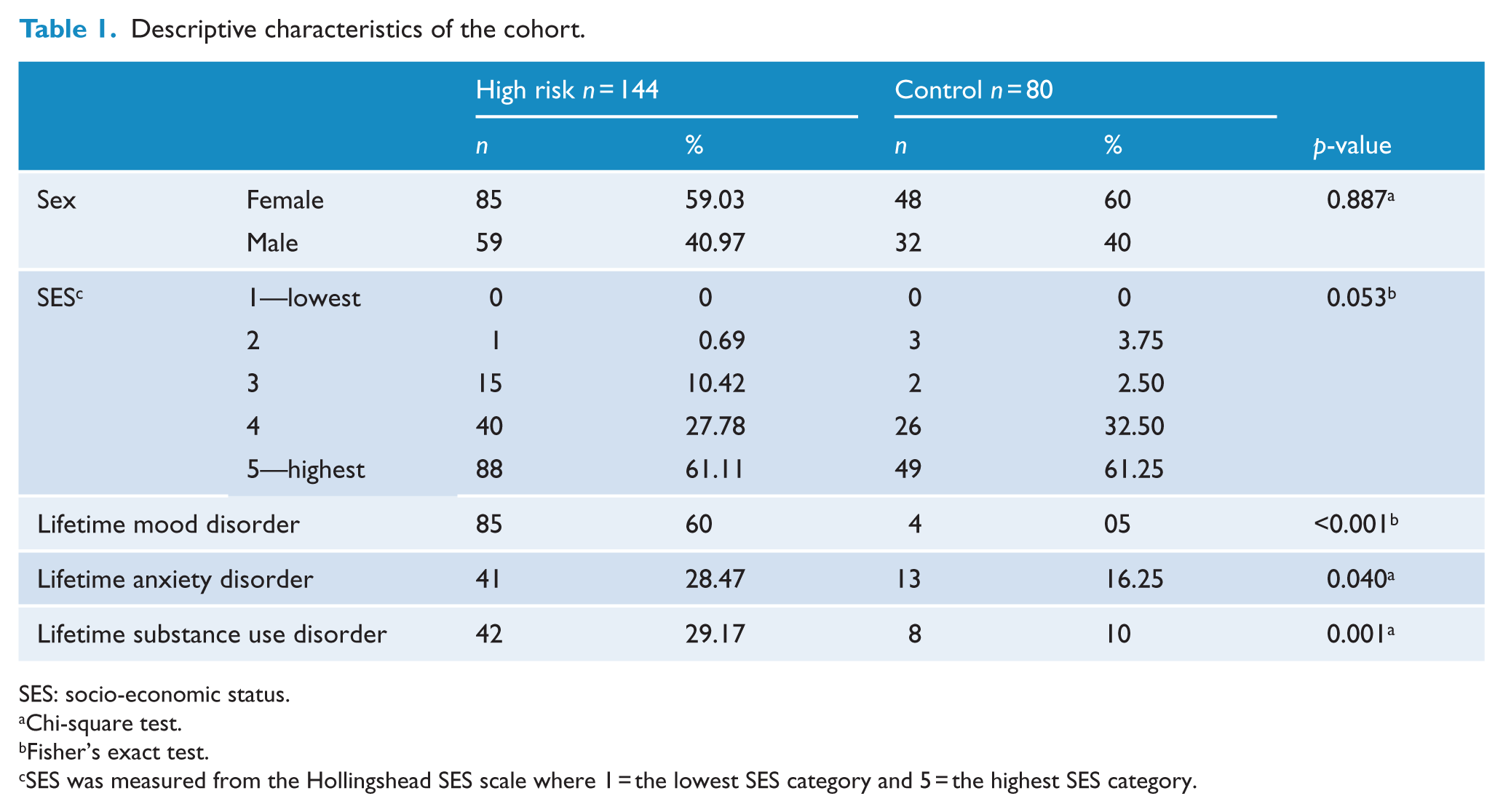
SES: socio-economic status.
Chi-square test.
Fisher’s exact test.
SES was measured from the Hollingshead SES scale where 1 = the lowest SES category and 5 = the highest SES category.
Approximately 60% were female in both high-risk and control offspring groups. There were no significant differences in SES (p = 0.05) between the groups. A lifetime diagnosable mood disorder was present in 60% of high-risk offspring compared to 5% of control offspring (p < 0.001), at last assessment. At last assessment, DSM-IV anxiety and substance use disorders were present in 28% and 30% of high-risk offspring, respectively; the majority of which were comorbid to mood disorder (Table 1). Rates of other comorbid lifetime diagnoses including attention-deficit hyperactivity disorder, oppositional defiant disorders and learning disorders are low in both high-risk and control offspring (Duffy et al., 2014). There were 50 and 24 cases of new onset mood episode/recurrences that occurred after the completion of the CCSC-R and RSES, respectively. Average total BDI-II score was less than 7.5 in both high-risk and control offspring at the time of completing the CCSC-R and RSES.
Psychological factors in high-risk and control offspring
There were no differences in active, distraction or avoidance coping strategy scores between well or remitted high-risk offspring compared to controls; however, support seeking coping scores were significantly higher in high-risk compared to control offspring (p = 0.04). Self-esteem scores were not significantly different between the high-risk and control groups (p = 0.23; Table 2).
Coping strategies and self-esteem scores in high-risk compared to control offspring.
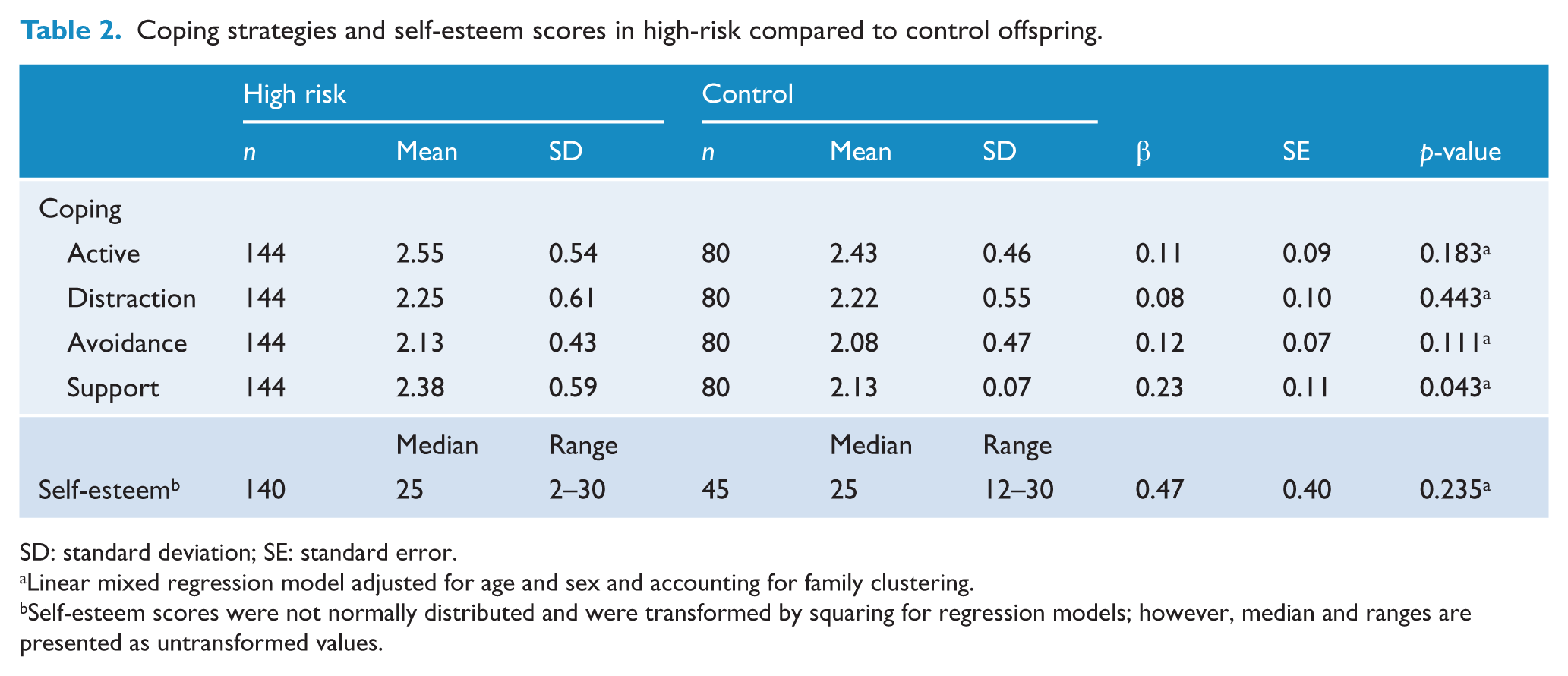
SD: standard deviation; SE: standard error.
Linear mixed regression model adjusted for age and sex and accounting for family clustering.
Self-esteem scores were not normally distributed and were transformed by squaring for regression models; however, median and ranges are presented as untransformed values.
Psychological factors predicting mood disorder in high-risk offspring
Higher avoidant coping was significantly associated with the hazard of developing a subsequent mood episode onset or recurrence (HR: 1.89, 95% CI: [1.02, 3.41]), while lower self-esteem scores were associated with a significant increase in the hazard of developing a mood episode (new onset or recurrence; HR: 2.50, 95% CI: [1.39, 4.54]; Table 3).
Coping and self-esteem total scores predicting the hazard of a new onset mood episode or recurrence.
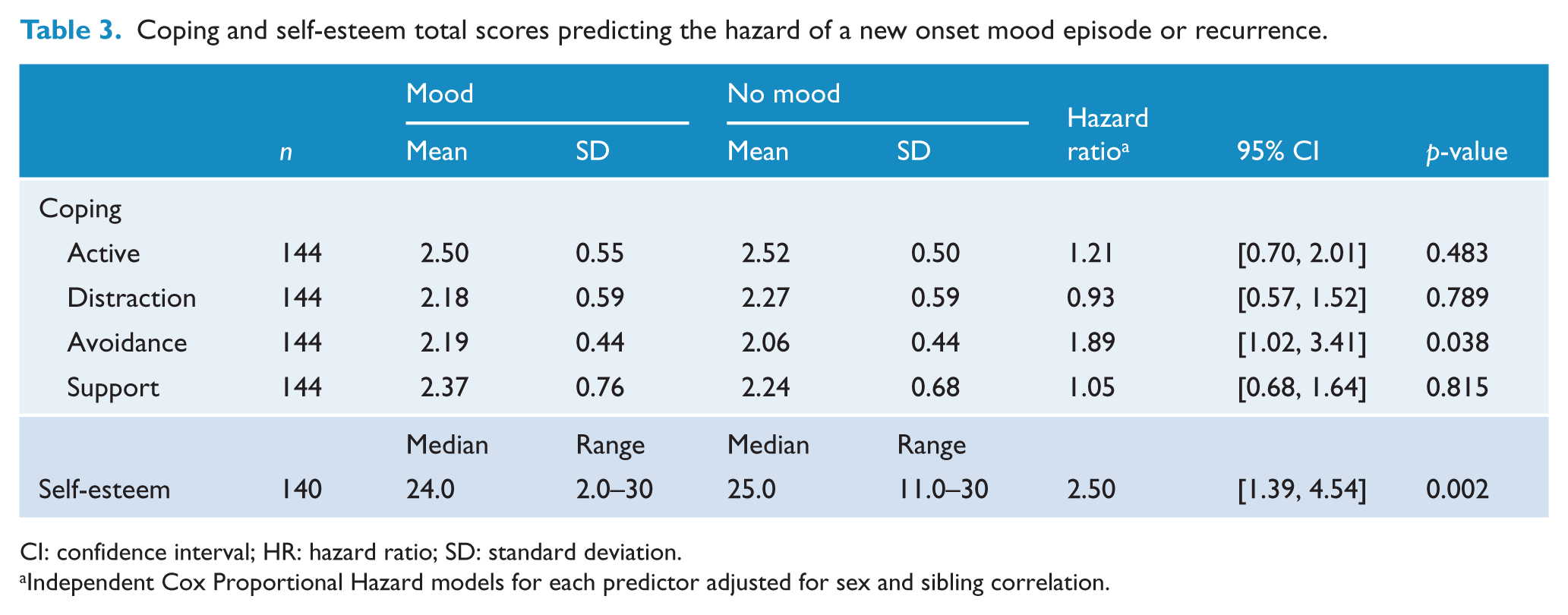
CI: confidence interval; HR: hazard ratio; SD: standard deviation.
Independent Cox Proportional Hazard models for each predictor adjusted for sex and sibling correlation.
Multivariable model
The resulting model, following the manual backwards selection procedure, included offspring sex, self-esteem, avoidant coping and an interaction between self-esteem and avoidant coping. Self-esteem, and the interaction between self-esteem and avoidant coping, were the only covariates that remained statistically significant (p = 0.02, and p < 0.05, respectively).
The interaction between self-esteem and avoidant coping was explored by testing for effect modification. The stratum-specific HR of a new mood episode/recurrence in high-risk offspring indicated an increased risk among those endorsing low self-esteem and high avoidant coping strategies (HR: 2.42, 95% CI: [1.10, 5.30]), a decreased risk among those endorsing high self-esteem coupled with low avoidant coping (HR: 0.38, 95% CI: [0.17, 0.86]), while the stratum-specific HR among those reporting low self-esteem together with low avoidant coping was non-significant (HR: 0.73, 95% CI: [0.41, 1.30]; Figure 1).
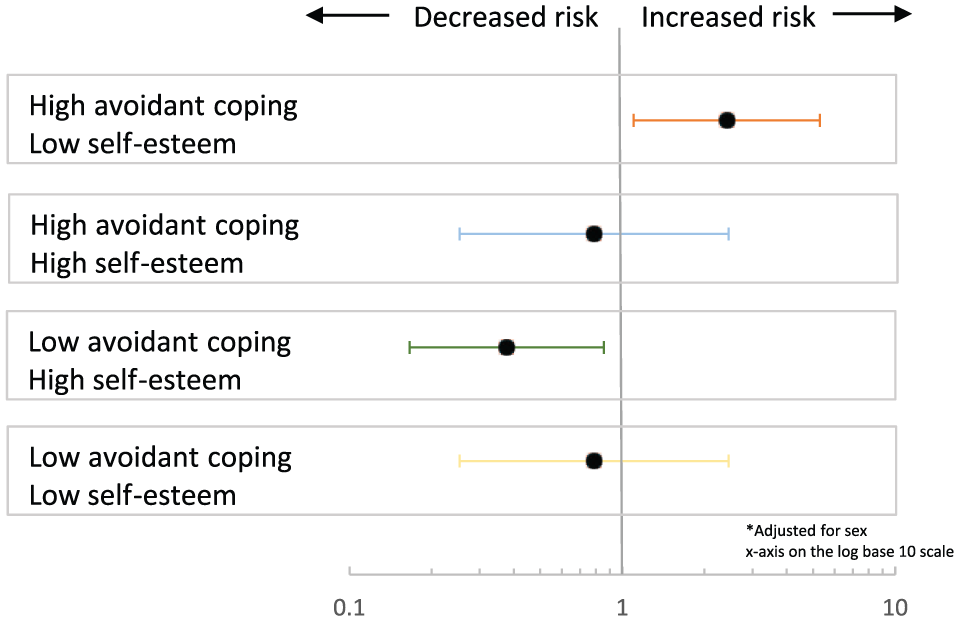
Stratum-specific hazard ratios and corresponding 95% confidence intervals of high and low self-esteem and avoidant coping predicting mood episode first onset or recurrence.
Discussion
In this longitudinal study of psychological risk factors in offspring of bipolar parents, we found evidence that self-esteem and avoidant coping style play an important role in the development of diagnosable mood disorder episodes. These findings are in agreement with and confirm prior cross-sectional reports. In particular, high-risk offspring with lower self-esteem and those relying more on avoidant coping styles in response to a stressful event were 2.5 and 2.0 times more likely to develop a first onset mood episode or recurrence, respectively. There was also significant evidence of interaction and effect modification, where the association between lower self-esteem and higher likelihood of mood episode onset or recurrence was significant only among offspring endorsing high levels of avoidant coping. The risk of mood episode onset or recurrence was increased by 2.4 times among high-risk offspring endorsing low compared to high self-esteem, while also reporting use of avoidant coping strategies. This suggests that in high-risk offspring with low levels of self-esteem, having low levels or an absence of avoidant coping in response to stress could be protective against the risk of developing mood episodes or recurrences.
In this cohort, high-risk offspring were found to endorse higher support seeking coping styles compared to control offspring. Plausible explanations for high-risk offspring adopting higher support seeking coping strategies include that (1) high-risk offspring were either well or in good clinical remission early in the course of a mood disorder when completing these measures, and, in this cohort, 80% of high-risk offspring were exposed to their parents’ BD illness in childhood (Goodday et al., 2015), therefore, were possibly more aware of their own risk; (2) a potential bias toward help-seeking through parental modeling may be present; (3) our research families are relatively highly functioning and well educated. Support seeking coping strategies may be adaptive in the high-risk offspring from this cohort given the lack of relationship with future mood episodes. In support of this, there is evidence that adult remitted patients with BD compared to patients with unipolar depression report more extraversion and adaptive coping involving accessing social support (Coulston et al., 2013).
Other studies have reported differences in cognitive and coping styles predicting onset of mood episodes of a specific polarity, as well as between bipolar subtypes (I vs II) in adults with BD (Fletcher et al., 2014). In this high-risk population, our findings suggest that low self-esteem could act as a potential target for prevention of subsequent mood episode onset. We did not have enough numbers to examine differential effects by bipolar subtype (I vs II), or polarity.
The following study limitations should be considered. Although all offspring were in clinical remission when completing the measures confirmed by semi-structured clinical interview and BDI-II score, there were some cases where offspring had a mood episode prior to completing the psychological measures. In these cases, the outcome was a new recurrence of mood episode, occurring after the completion of the self-report measures. Prior mood episodes may have influenced the participants perceptions of the psychological constructs examined and it is unclear if these constructs reflect a scar of previous illness. We did not have enough cases of new mood disorder onset; therefore, to increase statistical power, we combined first onset and recurrent mood episodes together as a single outcome. Future research with larger numbers should determine how these psychological constructs are associated with the development of a mood disorder, compared to subsequent recurrences and chronicity. Finally, the age when completing these measures was variable; however, age was adjusted for in all statistical models.
In summary, findings from this high-risk offspring study suggest that improvement of self-esteem and a reduction in avoidance as a coping strategy could serve as important salient targets for prevention and early intervention strategies in youth and young adults at high familial risk for developing mood disorders. More research with larger numbers, repeatedly measuring these constructs over the emerging illness course, is needed to determine how these risk factors act as potential mood episode triggers and to determine timing of mood episode onset in relation to the occurrence of these potential targets.
Supplemental Material
Supplementary_table_1 – Supplemental material for Coping Strategies and self-esteem in the high-risk offspring of bipolar parents
Supplemental material, Supplementary_table_1 for Coping Strategies and self-esteem in the high-risk offspring of bipolar parents by Sarah M Goodday, Richard Bentall, Steven Jones, Arielle Weir and Anne Duffy in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research was supported by a Canadian Institutes for Health Research Operating Grant (MOP # 102761). This research would not be possible without the ongoing support of our research families.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.