
Abstract
Objective:
Disruptive mood dysregulation disorder is a newly proposed childhood disorder included in Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition to describe children ⩽18 years of age with chronic irritability/temper outbursts. This study aimed to examine the prevalence of disruptive mood dysregulation disorder, severe mood dysregulation and chronic irritability in an Australian study of young people at increased familial risk of developing bipolar disorder (‘HR’ group) and controls (‘CON’ group).
Methods:
A total of 242 12- to 30-year-old HR or CON subjects were administered the severe mood dysregulation module. Of these, 42 were aged ⩽18 years at the time of assessment, with 29 subjects in the HR group and 13 in the CON group.
Results:
No subjects ⩽18 years – in either group – fulfilled current or lifetime criteria for disruptive mood dysregulation disorder or severe mood dysregulation, the precursor to disruptive mood dysregulation disorder. Similarly, no subjects in either group endorsed the severe mood dysregulation/disruptive mood dysregulation disorder criteria for irritable mood or marked excessive reactivity. One HR participant endorsed three severe mood dysregulation criteria (distractibility, physical restlessness and intrusiveness), while none of the comparison subjects endorsed any criteria. Exploratory studies of the broader 12- to 30-year-old sample similarly found no subjects with severe mood dysregulation/disruptive mood dysregulation disorder in either the HR or CON group and no increased rates of chronic irritability, although significantly more HR subjects reported at least one severe mood dysregulation/disruptive mood dysregulation disorder criterion (likelihood ratio = 6.17; p = 0.013); most of the reported criteria were severe mood dysregulation ‘chronic hyper-arousal’ symptoms.
Conclusion:
This study comprises one of the few non-US reports on the prevalence of disruptive mood dysregulation disorder and severe mood dysregulation and is the first non-US study of the prevalence of these conditions in a high-risk bipolar disorder sample. The failure to replicate the finding of higher rates of disruptive mood dysregulation disorder and chronic irritability in high-risk offspring suggests that these are not robust precursors of bipolar disorder.
Keywords
Introduction
The syndromes of severe mood dysregulation (SMD) (Leibenluft, 2011) and its Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) derivative – disruptive mood dysregulation disorder (DMDD) (American Psychiatric Association [APA], 2013) – have been proposed over the last decade to better encapsulate presentations of chronic irritability in children and adolescents without distinct episodes of mania, who were otherwise being diagnosed with paediatric bipolar disorder (BD) (Margulies et al., 2012; Roy et al., 2014; Singh et al., 2014).
DMDD is defined by persistent irritability and frequent temper outbursts, which may include either verbal or behavioural rages, with onset prior to the age of 10 years (APA, 2013). Substantial differences in prevalence in children and adolescents have been reported from post hoc analyses of existing data, varying from 0.12% to 8.2% (Althoff et al., 2016; Brotman et al., 2006; Copeland et al., 2013; Dougherty et al., 2014), with rates dependent upon age group and definitional issues – particularly use of diagnostic hierarchy and frequency of outbursts.
DMDD has a close relationship with other behavioural disorders, such as oppositional defiant disorder (ODD) and conduct disorder (CD), with one study of 706 primary school aged children finding that nearly 96% of those meeting criteria for DMDD also met criteria for either ODD or CD (Axelson et al., 2012).
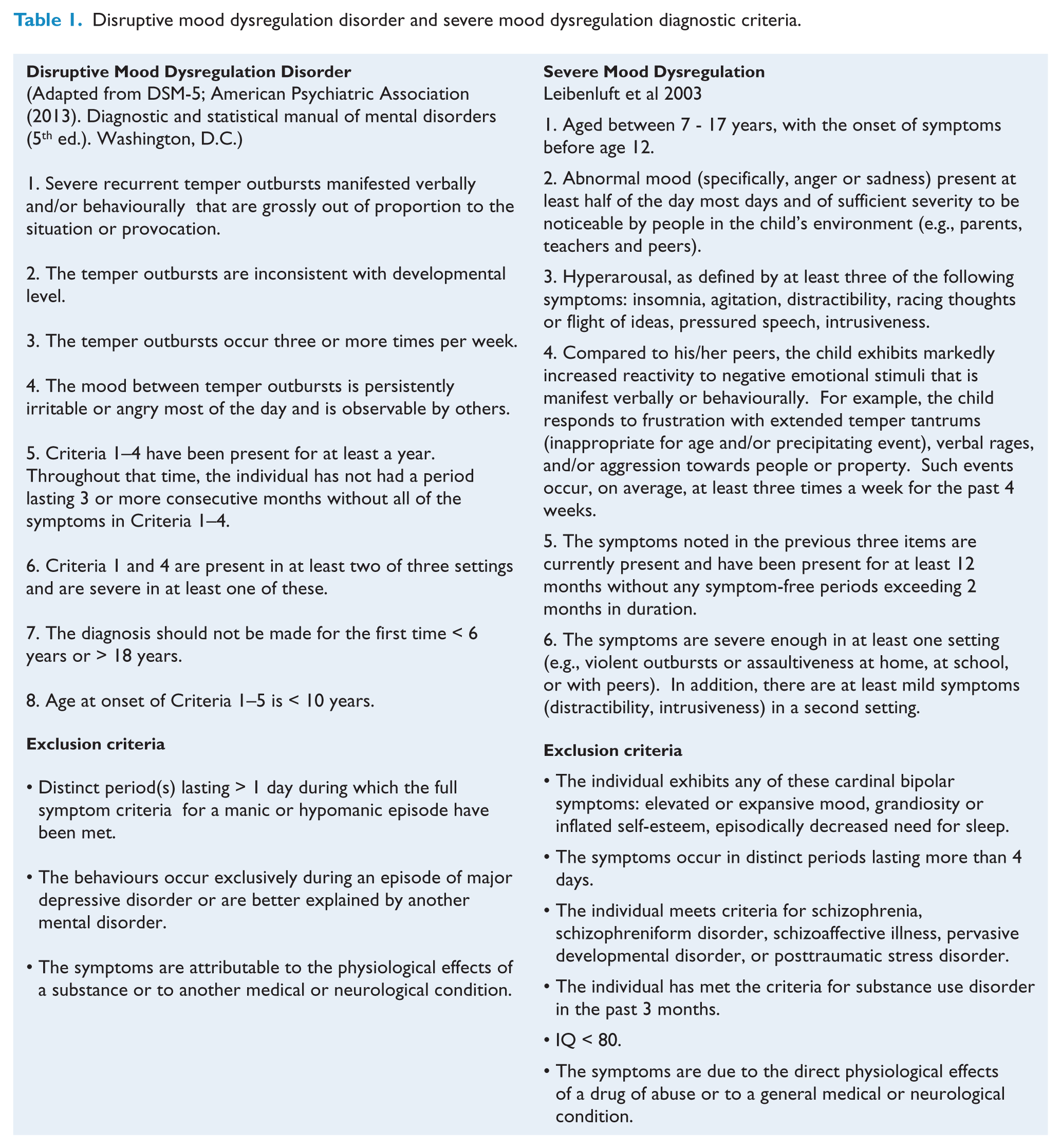
SMD was the precursor concept to DMDD, primarily defined for research purposes to facilitate the recruitment of youth with severe, chronic irritability, but without distinct manic episodes, to enable comparison against youth with BD in order to determine whether these two groups differed in course, family history and pathophysiology (Towbin et al., 2013). Differences between DMDD and SMD include the following: differences in age of onset criteria (for SMD before the age of 12 years, for DMDD before the age of 10); the abnormal mood of SMD more clearly specified as anger in DMDD; and the absence of hyper-arousal criteria in DMDD (for comparative details, see Table 1).
Disruptive mood dysregulation disorder and severe mood dysregulation diagnostic criteria.
There have been a number of studies which have examined the long-term outcome of children and adolescents with irritability, SMD and DMDD. Regarding irritability, one longitudinal study reported that chronic irritability predicted attention-deficit/hyperactivity disorder (ADHD) and major depressive disorder (MDD) at the 2- and 4-year follow-ups, respectively, while, in contrast, episodic irritability predicted simple phobia and mania (Leibenluft et al., 2006).
While SMD has been found not to be associated with either increased familial rates of BD (Brotman et al., 2007) or the later development of BD (rather being associated with depression) (Brotman et al., 2006), uncertainty remains concerning the long-term outcome of DMDD and its familial links with BD.
Copeland et al. (2014) reported from a prospective community study that young adults with a history of childhood DMDD developed increased rates of anxiety and depression, but not BD (Copeland et al., 2014). However, investigating a clinically defined high-risk sample, Sparks et al. (2014) reported that offspring of parents with BD were more likely to meet criteria for DMDD and chronic irritability than offspring of control families (Sparks et al., 2014). Specifically, this latter study reported that 6.7% of BD offspring met criteria for DMDD, compared to 0.8% in the control families. These increased rates of DMDD in the BD offspring occurred within the context of a greater prevalence of a broad range of psychopathology, with particularly high rates of DMDD being reported in those with ADHD and CD. Sparks et al. (2014) also reported higher rates of chronic irritability in their high-risk group, with 12.5% of BD offspring reporting this compared to 2.5% of controls. The report of Sparks et al. (2014) is consistent with some prior findings of higher rates of preceding CD and/or ODD in those who go on to develop mania (Kim-Cohen et al., 2003; Perich et al., 2015) and higher rates of preceding externalising disorders in first-degree relatives of probands with BD in those who go on to develop BD and/or MDD (Axelson et al., 2015; Nurnberger et al., 2011).
Recently, Mesman et al. (2016) reported a study comparing rates of psychopathology in BD offspring between the Dutch Bipolar Disorder Offspring study (Mesman et al., 2013) and the US sample described by Sparks et al. (2014). They noted higher rates of psychopathology and greater co-morbidities in the US sample compared to the Dutch sample; however, DMDD was not assessed (Mesman et al., 2016).
This study aimed to assess rates of lifetime DMDD and SMD (and associated symptoms such as chronic irritability) in an Australian sample: (1) those at high familial risk of developing BD (‘HR’) and (2) participants from control families (‘CON’). While the focus of this paper is on those ⩽18 years of age – the age range for which diagnoses of both SMD and DMDD have been validated – we also report, in exploratory analyses, lifetime rates of DMDD and SMD (and associated symptoms) in the broader study age range of 12–30 years.
Method
Participants
This report will focus on subjects aged ⩽18 years who were part of a prospective BD high-risk study of subjects aged 12–30 years. Subjects were recruited from a variety of settings including prior BD pedigree studies, BD research clinics and publicity through print and electronic media advertising and through notice boards in universities and local community centres (such as libraries and community health centres). See Perich et al. (2015) for more details. Here, we focus on two groups: (1) ‘high risk’ – subjects with a first-degree family member (parent or sibling) with Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) BD (‘HR’) and (2) ‘controls’ – those with no family history of serious mental illness (such as BD, MDD, schizophrenia or schizoaffective disorder) (‘CON’).
Procedure and measures
All participants underwent an initial screening process which involved a brief family history telephone interview. Participants (or their consenting parent if under 16) were administered the Family Interview for Genetic Studies (FIGS) (Maxwell, 1992) to determine any family history of psychiatric disorders. For those participants aged 12–21, the Kiddie-Schedule for Affective Disorders and Schizophrenia for School-Aged Children – Present and Lifetime Version (K-SADS-BP) was administered to both a participating parent and the child. The K-SADS-BP is an adapted version of the K-SADS Present and Lifetime Version (K-SADS-PL; Kaufman et al., 1997), which extends on sections on depression, mania and ADHD (Geller et al., 2001). For those aged 22–30 years of age, the Diagnostic Interview for Genetic Studies (DIGS v. 4; Nurnberger et al., 1994) was administered. The DIGS assessed lifetime depressive disorders, mania/hypomania, alcohol abuse and other drug abuse/dependence, psychosis, schizotypal personality features, anxiety disorders, eating disorders, CD, ADHD and pathological gambling.
The BD proband (parent or sibling) of all at-risk participants and the participating parent of the control group were also interviewed with the DIGS to confirm any psychiatric diagnoses (DIGS v. 4; Nurnberger et al., 1994). Using the Best Estimate Methodology (Leckman et al., 1982), lifetime diagnoses and age of onset were determined by the consensus of two independent raters (psychiatrists). For a more detailed description of the study procedures, please see Perich et al. (2015).
The SMD module – which was developed by Leibenluft (2011) to be appended to the K-SADS-PL – was administered to all subjects. While this module was originally developed to enable the diagnosis of SMD, it also covers the criteria for DMDD. It comprised questions covering the SMD domains (Leibenluft et al., 2003). This SMD module included the DSM-5 DMDD criteria (APA, 2013) in addition to the SMD-specific hyper-arousal criteria (such as insomnia, agitation, distractibility, racing thoughts or flight of ideas, pressured speech and intrusiveness).
Statistical analyses
Chi square analyses were conducted on categorical variables with the likelihood ratio being employed in cases where there was a smaller than expected numbers in the cells. Analyses of variance (ANOVAs) were conducted on dimensional variables of age.
Results
Main analysis: subjects aged ⩽18 years
Of the 242 subjects recruited to this prospective BD high-risk study who were administered the SMD module, 42 were aged < 18 years at the time of assessment. Of these, 29 were in the HR group, with 18 (62%) males and 11 (38%) females, and 13 were in the CON group, with 8 (63%) males and 5 (37%) females. The mean age of the sample of subjects was 15.59 years (standard deviation [SD] = 1.47); there were no significant differences between the groups with regard to age or gender.
No subjects in either group fulfilled current or lifetime criteria for DMDD or SMD. As detailed in Table 2, three of the HR subjects (10%) had a lifetime diagnosis of MDD compared to none of the CON subjects (not significant [NS]), while six HR subjects had an anxiety disorder (21%) compared to one (4%) of the comparison group (NS). No subjects in either the HR or CON group fulfilled criteria for a behavioural or substance use disorder.
Lifetime psychiatric disorders.
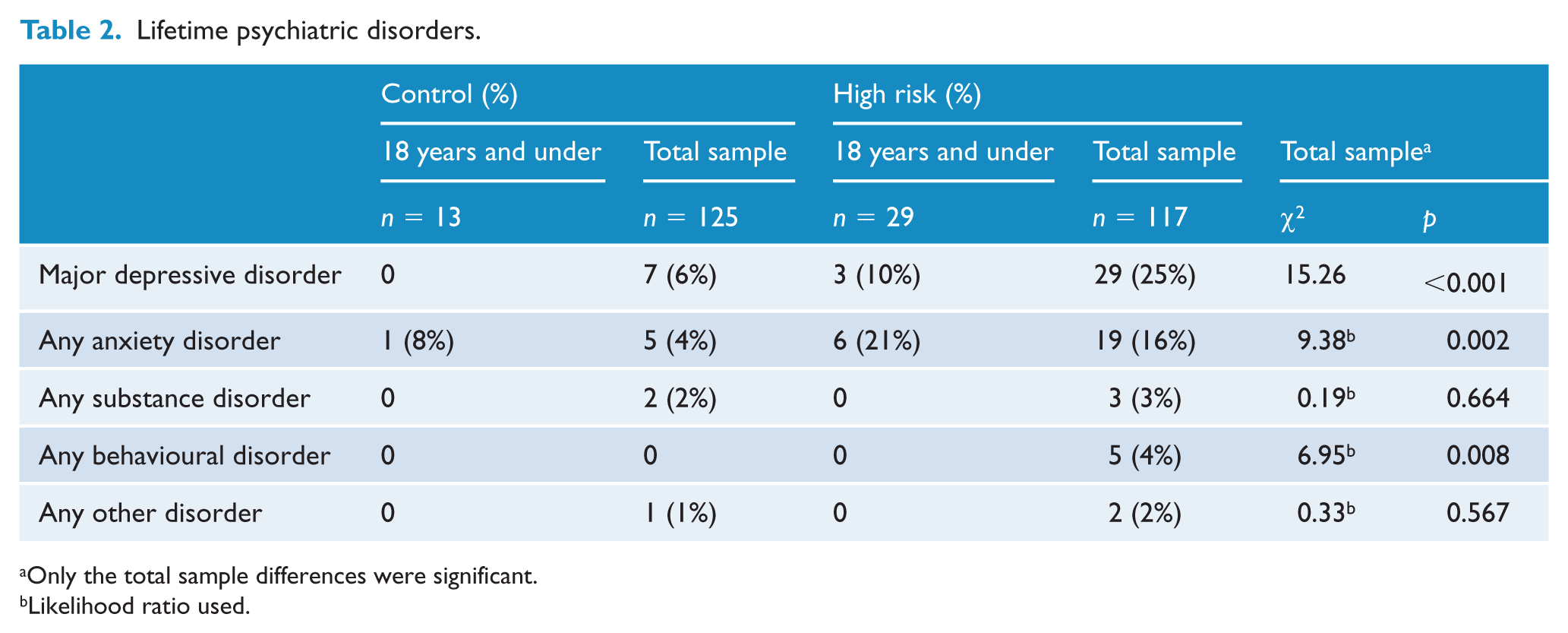
Only the total sample differences were significant.
Likelihood ratio used.
The individual DMDD and SMD criteria are detailed in Table 3. One HR participant endorsed three symptoms (distractibility, physical restlessness and intrusiveness), while none of the comparison subjects endorsed any of the criteria (NS). Specifically, no subjects in either group endorsed the criteria for chronic irritable mood or marked excessive reactivity.
Past DMDD and SMD criteria endorsed.
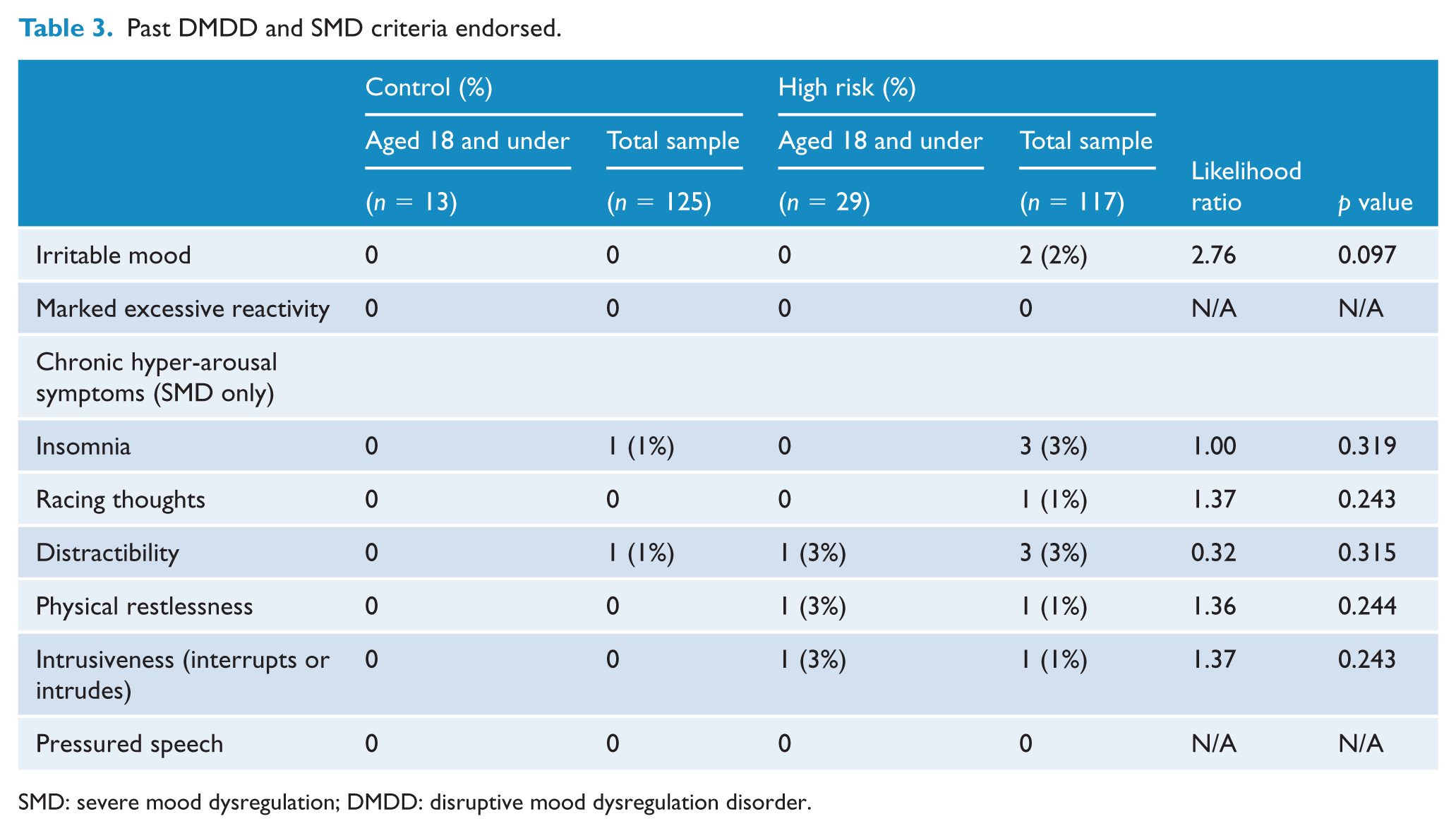
SMD: severe mood dysregulation; DMDD: disruptive mood dysregulation disorder.
Exploratory analysis: total sample (aged 12–30 years)
Of the total sample of 242 subjects, 117 were in the HR group: mean age 23.23 (SD = 6.15) years with 65 (56%) female. The CON sample consisted of 125 participants: mean age 24.81 (SD = 4.73) years with 59 (51%) female. There were no significant differences between the groups with regard to gender; however, age was significant (F(1, 230) = 4.781, p = 0.03) with the HR group being significantly younger than the CON group.
No subjects in either group fulfilled either current or lifetime criteria for SMD or DMDD. As detailed in Table 1, there were higher lifetime rates of MDD, anxiety disorders and behavioural disorders in the HR group compared to the CON group. Specifically, it should be noted that while significantly more HR subjects had a behavioural disorder, this only comprised 4% of that group.
The individual DMDD and SMD criteria are detailed in Table 3. In the total sample, 18 subjects (8%) endorsed at least one of these criteria: 9 (8%) from the HR group and 4 (3%) from the CON group, with a significant difference between the groups with a likelihood ratio of 6.17 (p = 0.013). Most of the reported criteria were those included under the SMD ‘chronic hyper-arousal’ symptoms. No other results were significant (see Table 3).
Discussion
Focusing primarily on those subjects aged ⩽18 years, there were two major findings from this study. First, it was striking that no subjects – in either the HR or CON group – fulfilled current or lifetime criteria for either SMD or DMDD. This is the first report of the prevalence of these syndromes in Australia, and similar to more recent US studies, which suggests that these are not common conditions, although it must be emphasised that we did not investigate a general community sample.
Unlike the recent report of Sparks et al. (2014) from a US ‘at-risk’ sample, this study did not find either a greater prevalence rate of DMDD or chronic irritability in the offspring of BD subjects compared to offspring from control families. With regard to irritability, Sparks et al. (2014) found a rate of 12.5% in their HR subjects compared to 2.5% among controls. No subjects in either our HR or CON group reported either chronic irritability or marked excessive reactivity. Even when we investigated the broader 12- to 30-year-old sample in an exploratory study, only 2% of the HR subjects (and none of the comparison group) reported chronic irritability, with none in either group acknowledging excessive reactivity. However, our results are consistent with the recent report of Mesman et al. (2016) who also noted lower rates of psychopathology and co-morbidities in a very similar Dutch group compared to the same US sample described by Sparks et al. (2014).
It should be noted that there were notable differences between our study sample and that of Sparks et al. (2014). First, our sample of those ⩽18 years was much smaller, comprising only 42 subjects compared to the 375 of Sparks et al. (2014). Second, there were substantial differences in the overall rates of behavioural disorders, with none of our ⩽18 years HR or control group subjects having categorical behavioural disorders (such as ADHD, ODD and CD). This is in sharp contrast to the Sparks et al. (2014) HR sample, which reported 25% with ADHD, 15% ODD and 4% CD. Even when we broadened the age range to 12–30 years, only 4% of our HR subjects fulfilled lifetime criteria for a behavioural disorder. This is a critical issue, as Sparks et al. (2014) found high rates of DMDD among those with other behavioural disorders such as ADHD and CD. Again, it should be noted that our findings were very similar to those of the Dutch group reported recently by Mesman et al. (2016).
Although the focus of our study was the ⩽18-year-old age group for which the diagnostic concepts of DMDD and SMD have been validated, it was of interest that analysis of our broader study age range (12–30 years) found that significantly more of our HR group reported at least one of the DMDD or SMD criteria compared to controls. As the reported criteria were mostly those included among the SMD ‘chronic hyper-arousal’ symptoms, it is possible that these may be indicative of either subthreshold hypomania or some affective instability.
It is also possible that the reason for the lower rates of DMDD symptoms (such as chronic irritability) in our study was that the interpretation of the criteria as used by our research team was stricter than those used by teams in other countries like the United States. Further research on such possible cross-national differences in interpretation of DMDD symptom criteria would be of considerable interest.
Two conclusions can be drawn from this study. First, no subjects with either current or lifetime SMD or DMDD were found in this Australian sample, although it must be acknowledged that we did not examine a nationally representative community population. Second, we were unable to replicate the finding of higher rates of DMDD and chronic irritability in high-risk BD offspring, suggesting that DMDD or chronic irritability is not a robust precursor of BD.
Footnotes
Acknowledgements
We are grateful to Dr Ellen Leibenluft of the National Institute of Mental Health, MD, USA, for both provision of the severe mood dysregulation module and helpful comments on an early draft of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was funded by the Australian National Health and Medical Research Council (NHMRC) through Programme Grant No. 1037196 and the Lansdowne Foundation. The funding sources played no role in the design, analysis or writing of this report.