
Abstract
Depression, anxiety and substance abuse/dependence are the most common mental disorders, and have their peak incidence during adolescence and young adulthood [1, 2]. Co-occurrence of these disorders among young people is substantial, and has been associated with significantly higher rates of academic problems, disability and professional help-seeking [2, 3]. While heavy drinking alone is associated with a depressive syndrome that is difficult to distinguish from major depression [4], epidemiological studies consistently report high rates of depressive disorders among young people with problem drinking [5, 6]. Of particular concern is the consistent association between alcohol, depression and youth suicide [7–9]. Together, these findings highlight the importance of screening for both alcohol (acute and chronic use) and depressive symptoms in young people presenting for treatment.
However, detection rates for co-occurring substance use and mental health problems among Australian youth have been traditionally poor, particularly within services in which such problems are not the primary focus of treatment [10, 11]. Within primary care settings, detection rates have typically been low, with general practitioners (GPs) correctly identifying <70% of patients with high-risk alcohol use [12, 13] and only 44% of those with mental disorder [14]. In recent years there has been increasing recognition of the importance of screening for mental disorders and alcohol/drug use within clinical settings across Australia [15–18]. As a result, a number of national programmes have been developed that specifically focus on improving the detection and management of mental disorders (e.g. beyondblue; Better Outcomes in Mental Health Care, BOiMHC), alcohol and other drug (AOD) issues (e.g. National Training Package for Medical Practitioners on Illicit Drug Issues [19]), as well as co-occurring mental health and alcohol problems (Managing the Mix [20]) by GPs. While several state-based comorbidity initiatives (e.g. Victorian Dual Diagnosis Initiative) have offered training to mental health and AOD workers related to managing co-occurring disorders, these have been widely variable in their coverage and intensity and have tended to be limited to clinicians within the public health sector. Opportunities for on-the-job drug and alcohol training and supervision have been limited [11], and there has been no training directly targeted at clinicians within private or community settings.
Although studies examining detection rates for co-occurring substance use and mental health problems have typically been conducted within the public health sector, most mental health treatment within Australia is provided by GPs, psychiatrists or allied health professionals working within primary care settings or private practices [21]. Recent increases in funding to the Australian BOiMHC programme will mean that a greater number of individuals will be able to gain access to allied health professionals, mental health nurses and psychiatrists for mental health treatment. However, limited data are available regarding the training needs of these professional groups in terms of managing co-occurring disorders, particularly among youth. In the present study we examined whether health professionals who commonly deal with mental disorder are able to detect co-occurring alcohol misuse in young people presenting with depression. We did this by presenting case vignettes of a depressed young person with or without co-occurring alcohol misuse. We assessed how commonly substance misuse and depression were explicitly mentioned when professionals were asked what was wrong with the young person.
Methods
Between September 2006 and January 2007 a survey examining beliefs regarding appropriate interventions for mental disorder in youth was sent to all 1710 psychiatrists listed on the Australian Medicare Provider File who had provided at least one service between 1 March and 30 June 2006; a sample of 2000 GPs from approximately 21 500 listed on the Medicare Provider File who had provided at least 375 services during the same period; all 1628 Australian members of the Australian and New Zealand College of Mental Health Nurses; and a sample of 2000 psychologists from 4812 fully registered psychologists (with a valid Australian address) listed on the Psychologists Registration Board of Victoria's online database. The GPs and psychologists were selected using the RAND function in Microsoft Excel. GPs, psychiatrists and psychologists were each sent a reminder letter (with questionnaire) if they had not responded to the survey within 4 weeks.
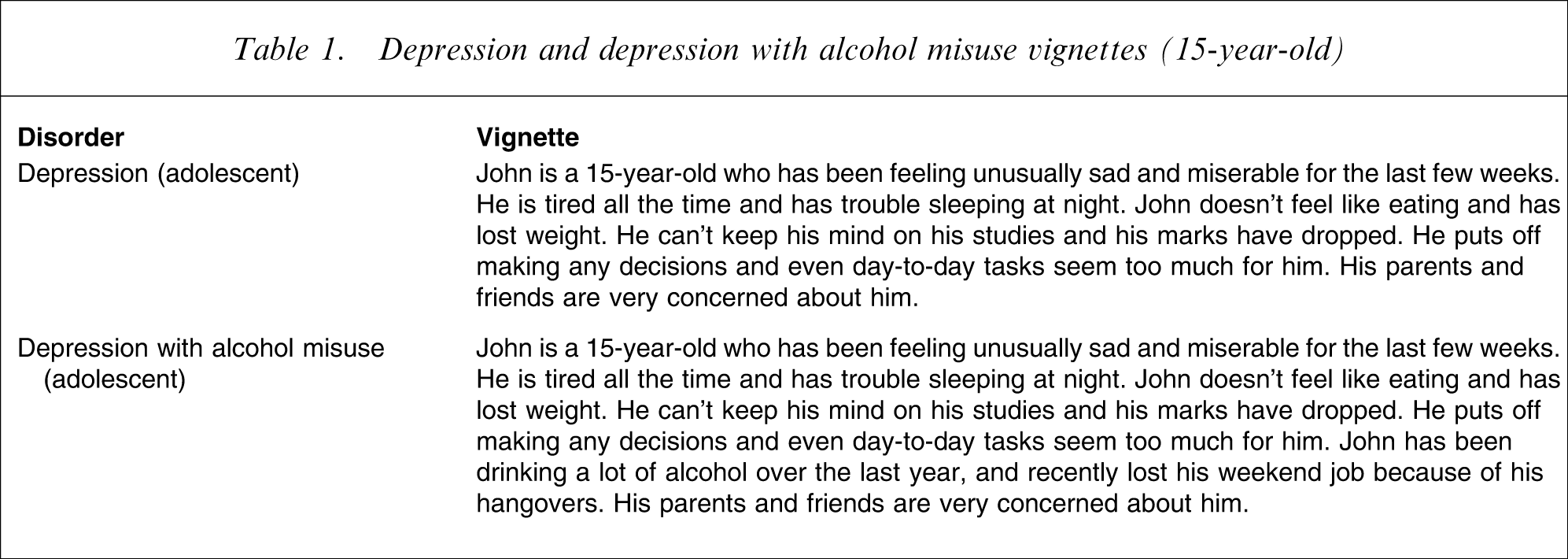
The survey was based on a vignette of a young person (John) with a DSM-IV mental disorder. Participants within each professional group were randomly given one of four vignettes: depression, psychosis (schizophrenia), social phobia or depression with alcohol misuse [22]. The vignettes were developed from previous work [23–25], and were reviewed by clinical researchers for face validity and conformity with diagnostic criteria. The age of the person in the vignette was randomly varied to be either 15 years or 21 years. Respondents were asked a wide range of questions, including ‘What, if anything, do you think is wrong with John?’. Two lines were provided to write an open-ended response to this query. For simplicity we report only data from the depression and depression with alcohol misuse vignettes (Table 1). Participants’ responses were coded by DSM-IV chapter according to whether they mentioned the presence of a mood and/or substance-related problem for each vignette.
Depression and depression with alcohol misuse vignettes (15-year-old)
Data on mood and substance use disorders are presented as percent frequencies and 95% confidence intervals (CIs). χ2 tests were used to assess statistically significant differences between professions at the p < 0.05 level. Predictors of reporting the presence of co-occurring depression and a substance use disorder (SUD) for the depression with alcohol misuse vignette were examined using simultaneous logistic regressions.
Results
The response rate for returned surveys was 24% for GPs, 35.4% for psychiatrists, 32.3% for mental health nurses and 40.3% for psychologists, and all were included for analysis. A total of 305 psychiatrists, 258 GPs, 292 mental health nurses and 375 psychologists completed one of the depression vignettes. The age, gender and experience of the different professional groups are presented in Table 2.
Age and experience of each professional group
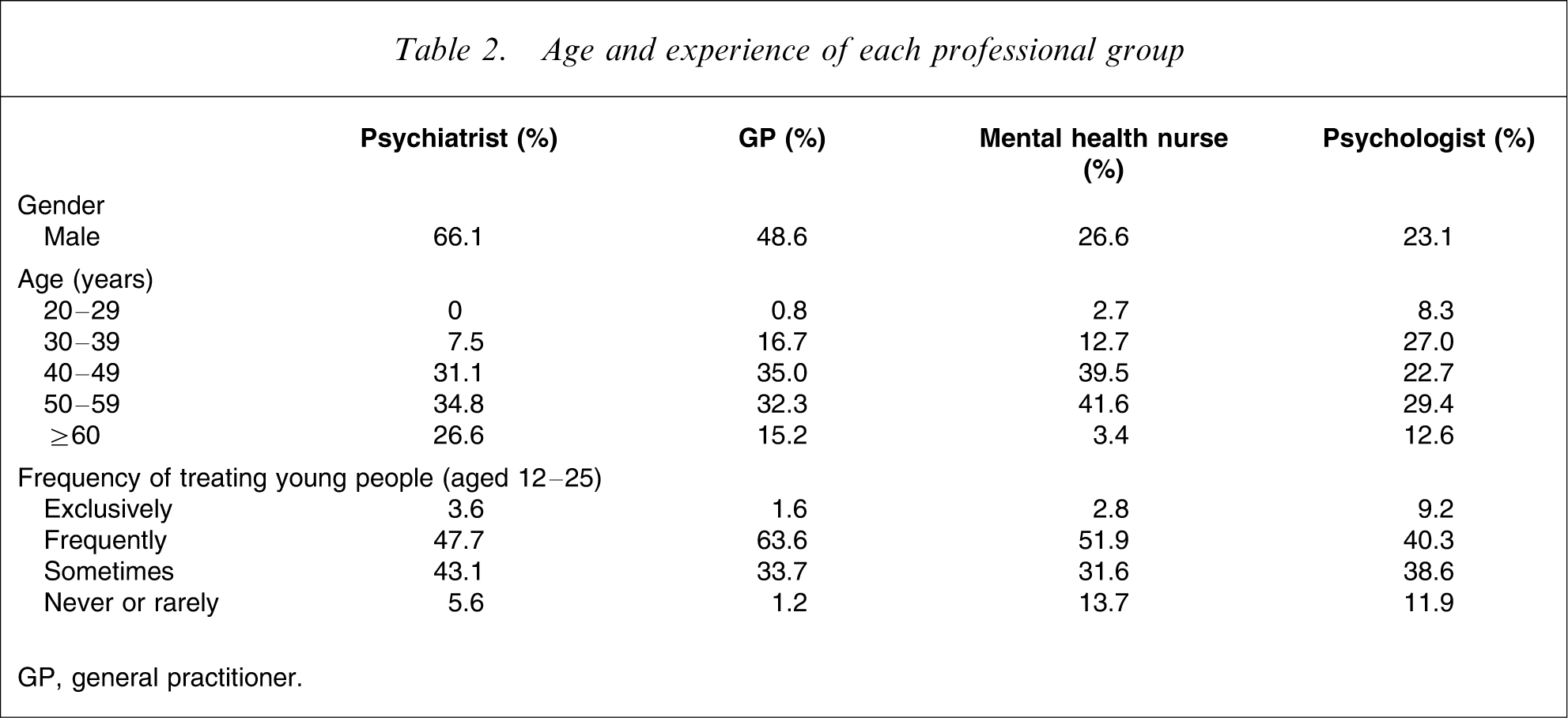
GP, general practitioner.
Percent frequencies and 95%CIs of reported diagnoses for each case (coded by DSM-IV chapters) are presented in Table 3, separated by professional group. Rates of reported SUD were almost identical to the rates of co-occurring SUD and are therefore not presented. A diagnosis of mood disorder was identified by at least 83.8% of professionals, and there were no significant differences between professions for any of the depression vignettes. Rates of reported co-occurring SUDs were substantially lower (between 29.1% and 60.0% for the depression with alcohol misuse vignette), and there were significant differences between professions for the 15-year-old depression vignette (p = 0.029) and the 21-year-old depression and alcohol misuse vignette (p < 0.001). For the 15-year-old depression case, GPs reported significantly higher rates of both disorders compared with psychologists and mental health nurses. For the 21-year-old depression and alcohol misuse case, psychologists were significantly less likely to identify both disorders compared with all other professions, and psychiatrists were more likely to identify both disorders than GPs.
Diagnoses of vignettes (coded by DSM-IV chapters) for each professional group
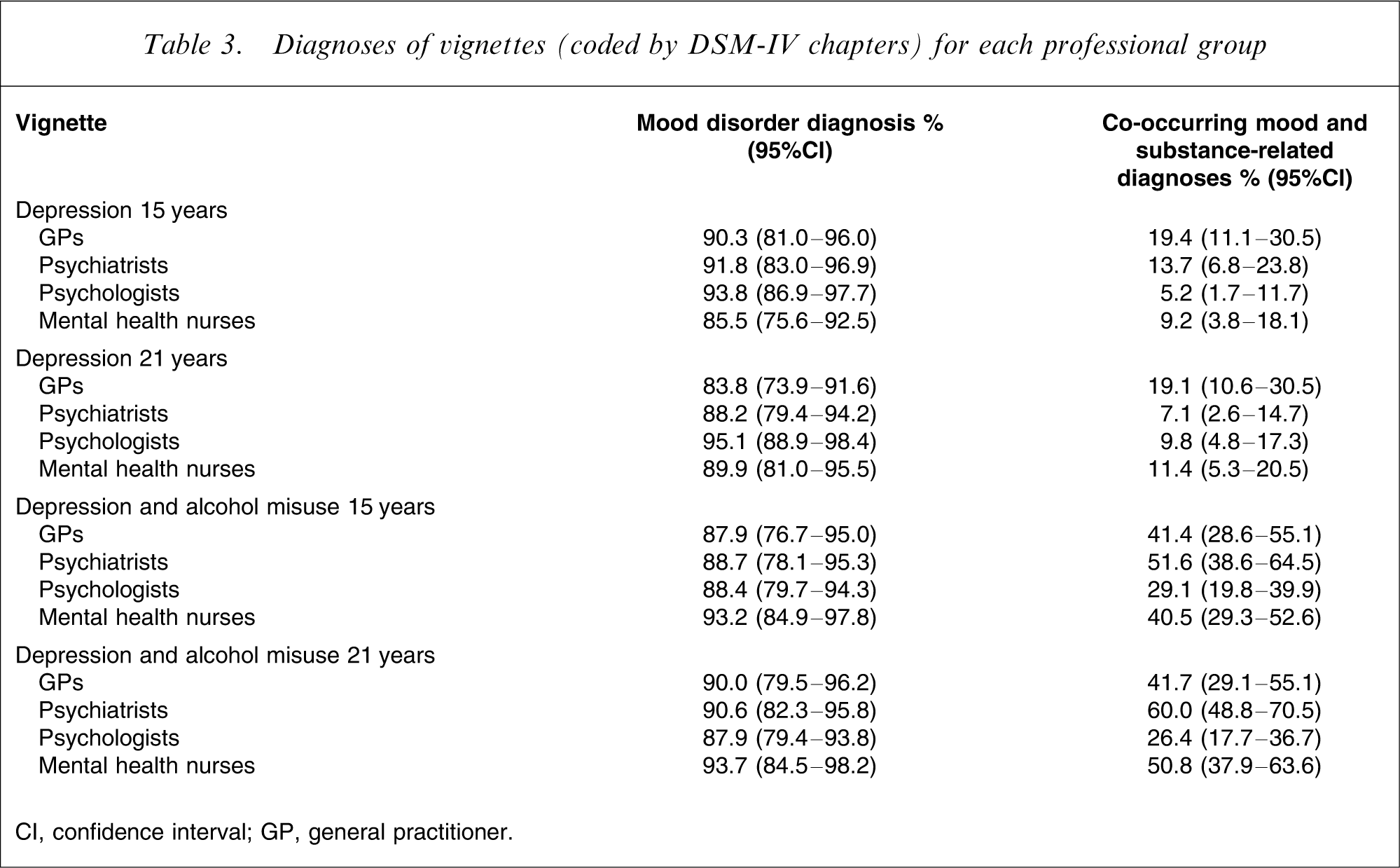
CI, confidence interval; GP, general practitioner.
In terms of major predictors of reporting a co-occurring depression and SUD diagnosis, professional group and age of the professional were significant factors (Table 4). Younger professionals were more likely to report co-occurring disorders, whereas experience with youth was of marginal significance.
Predictors of reporting a comorbid diagnosis for the depression with alcohol misuse vignette
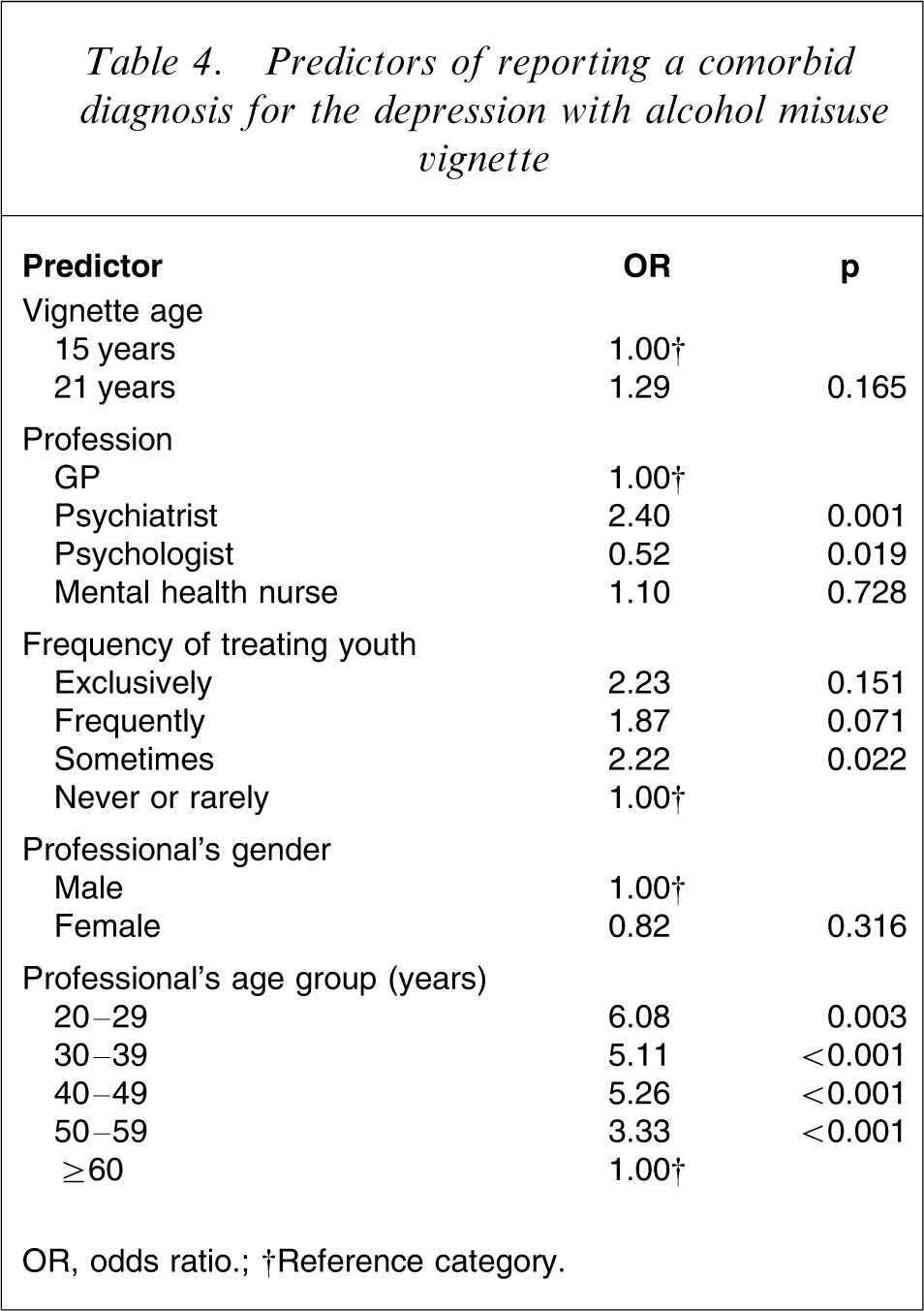
OR, odds ratio.
†Reference category.
Discussion
Health professionals identified similarly high rates of mood disorder across all the depression vignettes, regardless of the presence or absence of alcohol use within the history. Rates of reported co-occurring alcohol misuse were much lower and significantly differed across professional groups. Indeed, for the depression and alcohol misuse vignette, a co-occurring substance use issue was recorded by only approximately 56% of psychiatrists, 46% of mental health nurses, 42% of GPs and 28% of psychologists. These figures are in stark contrast with the rates of reported mood disorder, and suggest that GPs, psychologists and mental health professionals are less likely to identify alcohol misuse as an issue among young people with depression. This difference in reported rates may reflect a deficit in knowledge (e.g. the aetiological importance of heavy drinking when someone is presenting with low mood), an attitudinal deficit (e.g. viewing heavy use as normative for this age group), or a treatment deficit (e.g. professionals feel they lack relevant skills or are not mandated to treat SUD within their practice/service).
GPs were more likely to identify substance use as a potential issue within the depression vignette, which may reflect their increased exposure to targeted AOD training over recent years, as well as their focus on general health. In contrast, psychologists were consistently poorer at identifying co-occurring alcohol misuse across both age groups. It is important to note that the psychologists in the present study were recruited from a random sample of registered psychologists in Victoria, and included clinical, health, educational, organizational and neuropsychologists. While this group is likely to encompass a broad range of qualifications, training, experience and expertise, the majority of registered psychologists work in settings in which alcohol may play an important contributory role to a range of presentations. Nonetheless, the low rates of reported alcohol misuse across professional groups suggest that all health professionals require further training in the detection of primary and co-occurring alcohol disorders in youth, particularly given the associated morbidity and effect on treatment outcomes.
The overall poor rates of reported alcohol disorders in the current study are consistent with previous studies documenting low detection rates for SUD within primary care and mental health settings [11, 26]. However, despite acknowledgment of the need for GPs and mental health workers to undertake training in the assessment and management of SUD, there has been limited exposure to primary and co-occurring substance use problems at both undergraduate and postgraduate levels, as well as limited access to AOD rotations during GP, psychiatry, nursing and psychology training [16, 27–29]. Segregation of mental health from AOD services within Australia, and the associated lack of opportunities available for on-the-job AOD training and supervision across health-care professions further compounds this skills deficit [11, 30].
Recent comorbidity initiatives are to be commended, but the present findings highlight the need for GP, nursing, psychology and psychiatry training programmes to develop and expand their drug and alcohol curricula as well as access to AOD rotations during clinical training [27]. Indeed, although the Royal Australian and New Zealand College of Psychiatrists (RANZCP) now require all their trainees to undertake supervised drug and alcohol work, opportunities for trainees to work within AOD settings are limited, and few trainees are offered supervision by experienced addiction psychiatrists [31]. Further, while alcohol and drug curricula and training positions were developed in the 1990s across all medical schools in Australia (e.g. coordinators for alcohol and drug education in medical schools), most universities do not currently offer such material due to a lack of ongoing funding [16], a situation that clearly needs to be reversed. There is therefore a clear need for development of ongoing initiatives within the workplace, such as orientation, in-service and AOD-specific training programmes [27]. The present finding of greater reporting of co-occurring SUD among younger professionals is likely to be related to increased access to comorbidity training, because many will have recently worked or trained within the public health system. This suggests that national comorbidity training programmes need to particularly target older health professionals within community or private settings.
There are a number of limitations that need to be considered when reviewing the present data. The response rates were much lower than those for similar postal surveys of mental health professionals in the 1990s, which ranged from 61% for GPs to 75% for psychiatrists [24, 25]. However, it is possible that response rates of health professionals to surveys have been generally declining over this period, due to the frequency with which these groups have been surveyed. Further, despite sampling from a large pool of health professionals, responses may be biased towards participants who were particularly interested in the study's focus. Such individuals may be more aware of youth issues, and thus the reported recognition rates may be higher than expected. Nevertheless, the use of case vignettes within the survey, as well as a non-stringent coding of participant responses into DSM-IV chapters, suggests that rates of detection of co-occurring SUD within real-world clinical settings are likely to be substantially lower than reported here.
Finally, we sampled from a broad range of psychologists within a single state, many of whom may not work directly with young people with mental health or substance use issues. We were also not able to directly compare clinical psychologists with other health professionals, although it is likely that their responses may be more in keeping with the other groups because they receive more mental health-specific training than other types of psychologists. Further work in this area is clearly warranted, particularly because general psychologists and other professional groups with limited mental health training, such as occupational therapists and social workers, are now able to access BOiMHC funding.
Substance use and mental health problems are common among young people who present for treatment [1, 2, 32, 33]. It is therefore essential that GPs and other health professionals are well versed in the assessment and management of these conditions. Given the substantially negative impact of co-occurring disorders in young people, it is imperative that health-care professionals are appropriately trained to detect such disorders promptly, to ensure access to effective, early intervention.
Footnotes
Acknowledgements
Funding was provided by the National Health and Medical Research Council, the Colonial Foundation and beyondblue: the national depression initiative.