
Abstract
Objective:
To assess depression literacy, help-seeking and help-offering to others in members of the police force in the state of Victoria, Australia.
Methods:
All staff in police stations involved in a cluster randomised controlled trial of an integrated workplace mental health intervention were invited to participate. Survey questions covered sociodemographic and employment information, recognition of depression in a vignette, stigma, treatment beliefs, willingness to assist co-workers with mental health problems, help-giving and help-seeking behaviours, and intentions to seek help. Using the baseline dataset associated with the trial, the paper presents a descriptive analysis of mental health literacy and helping behaviours, comparing police station leaders and lower ranks.
Results:
Respondents were 806 staff, comprising 618 lower-ranked staff and 188 leaders. Almost 84% of respondents were able to correctly label the problem described in the vignette. Among those who had helped someone with a mental health problem, both lower ranks and leaders most commonly reported ‘talking to the person’ although leaders were more likely to facilitate professional help. Leaders’ willingness to assist the person and confidence in doing so was very high, and over 80% of leaders appropriately rated police psychologists, general practitioners, psychologists, talking to a peer and contacting welfare as helpful. However, among both leaders and lower ranks with mental health problems, the proportion of those unlikely to seek professional help was greater than those who were likely to seek it.
Conclusion:
Knowledge about evidence-based interventions for depression was lower in this police sample than surveys in the general population, pointing to the need for education and training to improve mental health literacy. Such education should also aim to overcome barriers to professional help-seeking. Interventions that aim to improve mental health literacy and help-seeking behaviour appear to be suitable targets for better protecting police member mental health.
Introduction
High prevalence mental disorders such as depression, anxiety and related conditions are leading causes of disability worldwide (Whiteford et al., 2013). In Australia, one in five people aged 16–85 years experiences an anxiety, affective or substance use disorder in any 12-month period (Slade et al., 2009). However, approximately two-thirds of people who meet the criteria for these disorders do not seek professional help (Burgess et al., 2009).
The majority of mental health problems occur in people of working age, and in recent years, there has been an increasing focus on the workplace as an important setting for intervention, not only to address health problems caused by work but also to address non-work-related problems that may become visible or be exacerbated within the working environment (LaMontagne et al., 2012, 2014; Martin et al., 2009; Sanders and Crowe, 1996). While workplace mental health programmes can span the spectrum from primary prevention (e.g. job stress prevention) to tertiary interventions (e.g. return-to-work programmes), promotion of help-seeking from appropriate professional sources (including workplace providers) is a key aspect. Mental health literacy is a key factor impacting on help-seeking. It incorporates the ability to recognise mental health problems; knowledge of causes, risk factors, self-treatments and available professional help, as well as attitudes that promote recognition and appropriate help-seeking (Jorm et al., 1997).
Good mental health literacy is important in all working age adults but may be particularly important in professions at greater risk of exposure to psychosocial job stressors, such as police (Burke, 2017; Johnson et al., 2005). Internationally, police have been shown to experience both operational (e.g. exposure to traumatic incidents) and organisational stressors (e.g. high job demands, low job control, poor supervisor support) (Burke, 2017), as well as a male-dominated culture that places an emphasis on denial of distress (Harris et al., 2015) and stigmatises help-seeking behaviour (Karaffa and Koch, 2016). High levels of job stressors in police have been linked to burnout (Houdmont, 2017), work-family conflict (Hall et al., 2010), depression (Lawson et al., 2012), intimate partner violence (Gershon et al., 2009), psychological distress (Noblet et al., 2009a, 2009b) and suicide (Loo, 2003).
While a number of studies have explored police attitudes towards community members with mental health problems, these typically pertain to the crisis situations that police might have to deal with in the course of their employment (e.g. attending to people displaying signs of suicidality or psychosis; Arensman et al., 2016; Bahora et al., 2008; Pinfold et al., 2003). Relatively few studies have explored attitudes towards common mental disorders, or help-seeking in police officers themselves or in their colleagues. Available evidence suggests that while knowledge about available services and helping intentions is reasonably high for police, rates of professional help-seeking for mental health problems are relatively low, even in cases of serious suicidal ideation (Berg et al., 2006; Mishara and Martin, 2012). To our knowledge, no previous studies have comprehensively explored mental health literacy and helping behaviours in Australian police contexts, despite this being the subject of several recommended actions raised in a 2016 independent Mental Health Review of Victoria Police (Victoria Police, 2016). The mental health of police and emergency services workers is also a priority of the Australian national depression initiative’s (beyondblue) Police & Emergency Services Program, first launched in 2014 (beyondblue, 2014). To inform mental health literacy intervention efforts in the Australian policing context, and to contribute to the international literature in this area, the aim of this study was to assess depression literacy and helping behaviours within Victoria Police, a statewide police force in Australia.
Methods
Data reported in this study were collected in the pre-randomisation baseline assessment for a two-arm cluster randomised controlled trial (RCT) of an integrated workplace mental health intervention (Current Controlled Trials: ISRCTN82041334; Registered 24 July, 2014). Victoria Police is a statewide organisation consisting of over 15,300 sworn police members and around 3600 civilian employees. There are an estimated 329 police stations across Victoria. Full details on the trial protocol have been previously published and are summarised below (LaMontagne et al., 2016). Ethical approval was granted by the Human Ethics Sub-Committee at the University of Melbourne (Application number: 1340429), the Human Ethics Committee at Deakin University (Melbourne, Australia) (Application number: 2014–132) as well by Victoria Police.
Study population and data collection
Recruitment of clusters
For feasibility reasons, recruitment was restricted to divisions of Victoria Police located in geographical regions that were within 2 hours’ travel time by car from the researchers’ university base; this corresponds to a large proportion of the state’s population. These divisions were selected in consultation with welfare-related departments within Victoria Police (e.g. Policy Psychology, OH&S, HR) and a project steering group. The Eastern and North West police districts (compass direction relative to the Melbourne central business district) were chosen to obtain some variation in setting and population base. The selected areas include a mix of predominantly suburban stations, with some urban and regional stations also included. In addition to being in the selected areas, station inclusion/eligibility criteria included 24-hour operation and a minimum size of 40 or more sworn police members working in each station. In all, 24 police stations enrolled in the trial and participated in baseline surveys.
Recruitment of participants within stations
All sworn Victoria Police members within participating police stations were invited to take part in assessments and intervention activities, including early career officers (Probationary Constables and Constables), mid-tier ranks (Senior Constables and Leading Senior Constables) and station leaders (Sergeants and Senior Sergeants). There were no exclusion criteria at the individual level. Information regarding the project activities was distributed in hard-copy leaflet and poster format at participating stations. Information sessions were also held for station leaders and general staff. This session explained the goals of the study, outlined what the baseline survey involved and emphasised that participation in the survey was voluntary and anonymous. Due to the surveys including information on mental health, Victoria Police key informants requested the survey be anonymous with no possibility of responses being seen by the employer; hence, the survey remained anonymous and was accessed via direct web-link to Deakin University, with no data collected or transferred on Victoria Police computer systems. The introduction to the questionnaire reiterated the voluntary and anonymous nature of the survey, hence completion of the questionnaire signified informed consent.
Excluding a small number of unsworn public servants working at the police stations included in the study, as well as ‘survey responses’ with only a few fields completed, the total N included in this analysis was 806, comprising 618 lower ranks and 188 leaders at Sergeant rank or above. The overall survey response rate was 70.3% of sworn police members at the 24 participating police stations, based on census of all eligible police members at the participating stations. During the baseline data collection period, station sizes ranged from 24 to 102 sworn police members.
Measures
Two surveys were implemented: one for lower ranks and one for station leaders (Acting Sergeant or higher rank). The survey for station leaders included a few additional manager-specific questions, but in most respects was the same as the survey for lower ranks. Both surveys contained the following questions relating to sociodemographic information and measures of mental health literacy used in previous national surveys of mental health literacy and stigma (Jorm et al., 1997; Reavley and Jorm, 2011a) and adapted for use in police:
Sociodemographic and employment information
All respondents were asked to report their age group (categorical), sex and highest educational attainment. They were also asked to report their current job title and rank, time in current position, length of employment in Victoria Police and full- or part-time working status.
Depression recognition
Depression recognition was measured using a written vignette featuring a 30-year-old man named ‘John’ (Jorm et al., 1997; Reavley and Jorm, 2011a). The vignette covers common symptoms of major depression with suicidal features and meets both Diagnostic and Statistical Manual for Mental Disorders (4th ed.; DSM-IV) and International Classification of Disorders, 10th edition (ICD-10) criteria for this condition (American Psychiatric Association, 1994; World Health Organization, 1993). All respondents were asked for an open-ended response to identify what problem, if any, John has.
Beliefs about treatment
The vignette was also used as reference to ask the respondent (leaders only) their views on the degree to which various sources of help might be helpful or harmful to ‘John’ (e.g. seeing their general practitioner [GP] and dealing with problem on his own) (Reavley and Jorm, 2011a).
Help-seeking intentions
All respondents were asked if they were to experience a mental health issue in the future, how likely they would be to seek help from each of 13 sources (response options on 5-point Likert-type scale: very/somewhat likely, neither likely or unlikely and somewhat/very likely).
Willingness to assist
For the leader survey only, the depression vignette was followed by a question asking the respondent if they would help John if he was a co-worker (on a scale of 1 = not at all, to 7 = strongly agree). If yes, the respondent was asked what they would do to help (free text response). The respondent was then asked about their degree of confidence in having a conversation with someone at work with a problem like John’s (on a scale of 1 = not at all to 5 = extremely).
Recent helping behaviours
All respondents were asked to indicate (yes/no/don’t know) whether, over the past 6 months, they had worked with a colleague suffering from a mental health problem, and if yes, what they thought the problem was (free text), whether they tried to help that person, and if yes, in what ways (six choices, for example, suggesting they see a health professional; Kitchener and Jorm, 2004).
Recent help-seeking behaviours
All respondents were asked ‘in the past 6 months, if you had a mental health issue, did you seek professional help?’, with response options yes/no/haven’t had an issue. If yes, respondents were asked to indicate the type of help sought (seven choices, for example, a psychologist and police union).
Personal depression stigma
A measure of stigmatising attitudes towards John as a hypothetical colleague with depression was assessed using the first six items on the personal subscale of the Depression Stigma Scale (Griffiths et al., 2004). These items assess the degree to which respondents perceived that a person with depression can ‘snap out’ of the problem if they wanted, that depression is a sign of personal weakness, that depression is not a genuine medical illness, and that people with depression should be avoided as they are contagious, unpredictable or dangerous.
Coding of open-ended responses
Responses to the question of what was wrong with the person in the vignette were coded based on the pre-coded categories used in previous surveys (Jorm et al., 1997; Wright et al., 2005); responses were coded as ‘depression’ if the respondent made any mention of the condition or ‘suicide’ if the respondent mentioned this. Other free text responses were coded thematically.
Statistical analysis
The data were analysed using percent frequencies and 95% confidence intervals. All analyses were performed using Intercooled Stata 14.2 (StataCorp LP, TX, USA). Results are reported for lower ranks, leaders and both groups combined (where appropriate).
Results
Sociodemographic characteristics
Sociodemographic characteristics of the sample are given in Table 1. Respondents comprised 76.7% lower-ranked Police and 23.3% leaders. They were most likely to be male, aged between 20 and 39 years, have worked for Victoria Police for between 13 months and 6 years, to have been employed at their current rank for between 1 and 4 years and to work full time. The most commonly reported ranks were probationary constable and senior constable. Leaders were more likely to be male, older and to have longer duration of employment with Victoria Police.
Sociodemographic characteristics.
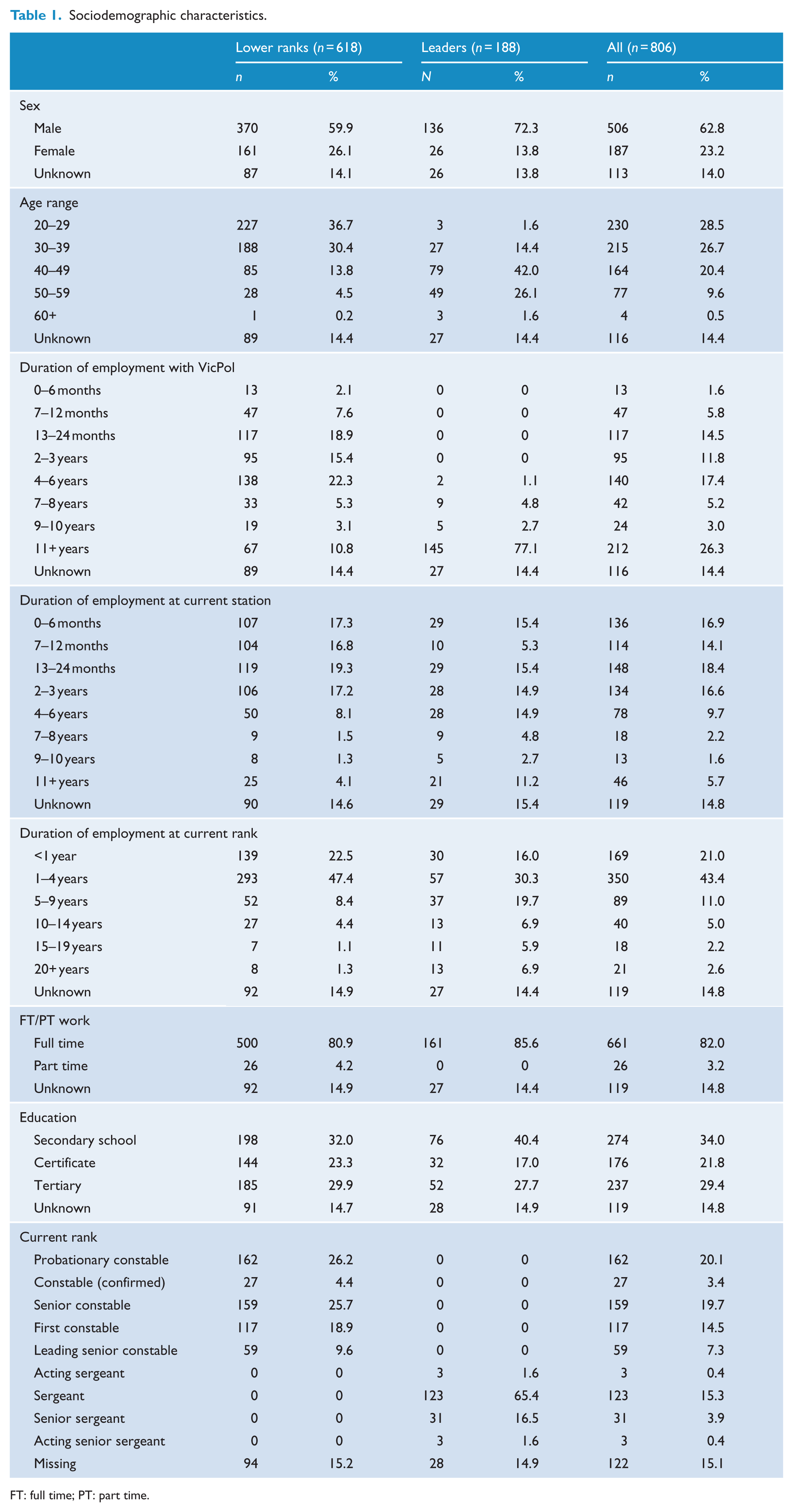
FT: full time; PT: part time.
Depression recognition
In response to the vignette, 84.3% (95% confidence interval [CI] = [81.3, 86.9]) of respondents mentioned ‘depression’ while only 12.5% (95% CI = [10.1, 15.2]) mentioned ‘suicide’. The responses with ‘depression’ were higher among leaders (89.9%, 95% CI = [84.3, 94.0]) compared to lower ranks (82.5%, 95% CI = [78.9, 85.6]), although the difference did not quite reach statistical significance. Other common responses include those related to workload pressures and ‘mental health problems’.
Beliefs about treatment
Table 2 shows leaders’ ratings of the likely helpfulness or harmfulness of specific people and interventions. Among people who could help, police psychologists, GPs, psychologists, talking to a peer and contacting welfare were considered helpful by over 80% of respondents. Among interventions, physical activity and relaxation/stress management received the highest ratings. Dealing with the problem alone, which is not recommended, was rated as harmful by 49.0% (95% CI = [40.7, 57.3]) of respondents.
Percentage (and 95% CI) of respondents rating each type of intervention as ‘helpful’, ‘harmful’ or ‘neither’ for the person described in the vignette.
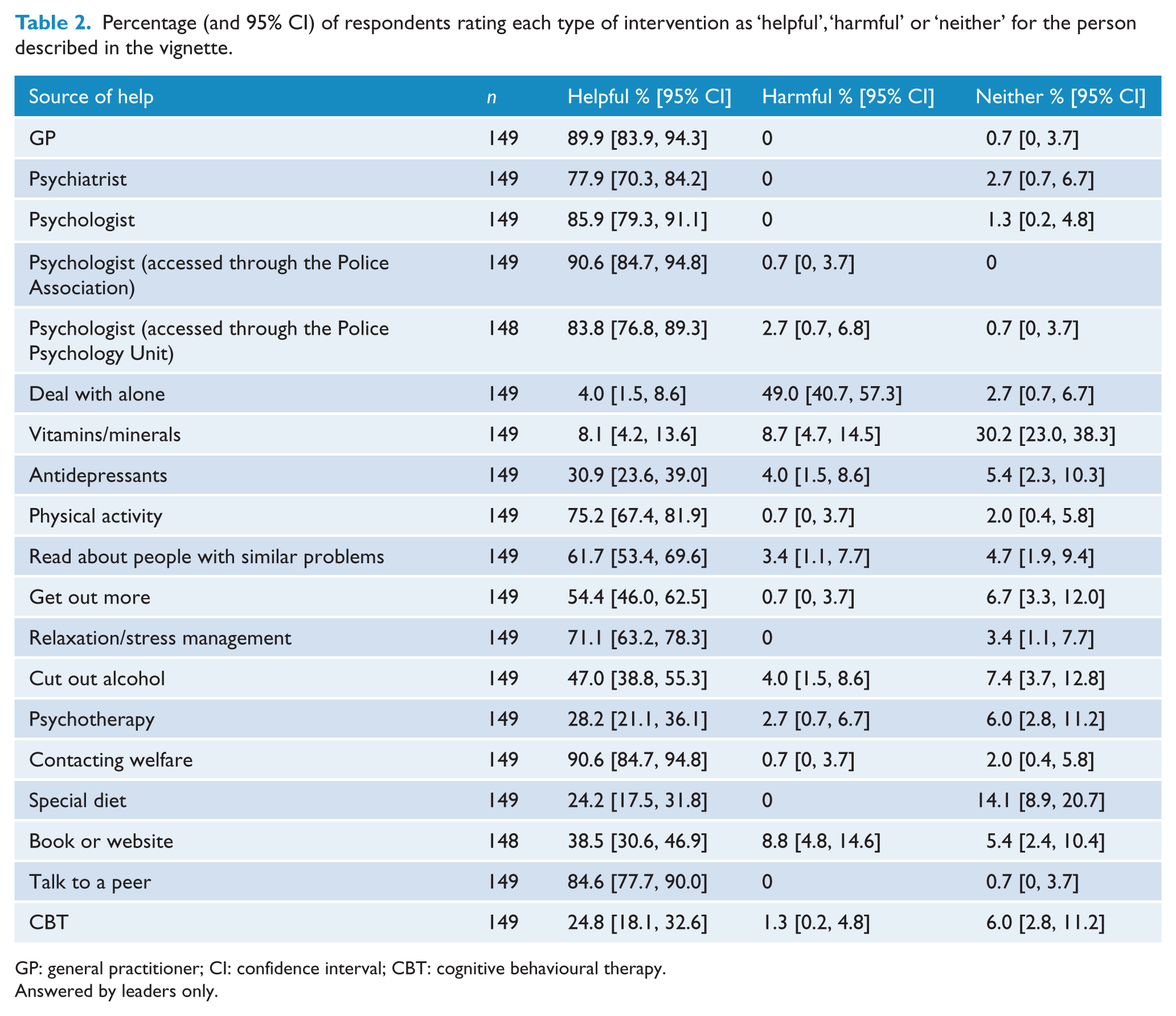
GP: general practitioner; CI: confidence interval; CBT: cognitive behavioural therapy.
Answered by leaders only.
Help-seeking intentions
When asked where they would go for help if they had a mental health problem, the most commonly nominated options were spouses, family members or friends (see Table 3). Among health professionals, GPs were the most commonly nominated options, followed by psychologists in general (without affiliation specified), which was roughly equivalent to seeking help from a psychologist through the Police Association (police union). Just under half of respondents would seek help from colleagues while roughly one-third would seek help from peer support officers.
Percentage (and 95% CI) of respondents who would seek help from various sources for a mental health problem in the future.
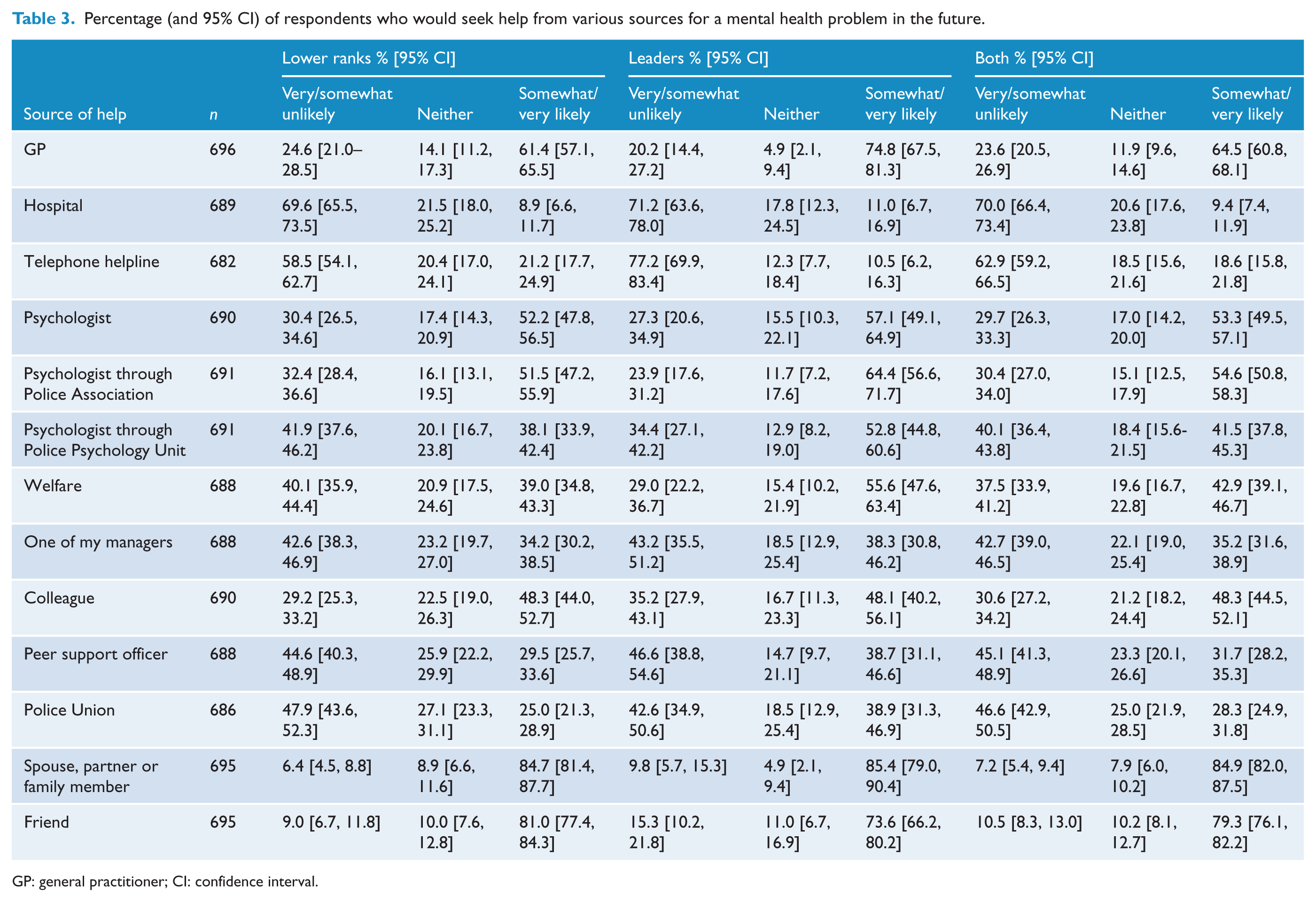
GP: general practitioner; CI: confidence interval.
When responses from lower ranks and leaders were compared, leaders were more likely to seek help from GPs, psychologists through the Police Association or Police Psychology Unit, psychologists in general and Welfare. Lower ranks were more likely to seek help from GPs, and psychologists in general or through the Police Association.
Willingness to assist
When leaders were asked if they were willing to assist (scale of 1 to 7, with 7 = strongly agree), mean (standard deviation [SD]) score was 6.70 (0.82). Mean (SD) confidence about helping (scale of 1 to 5, with 5 = extremely confident) was 4.17 (0.88). Free text responses (n = 149) describing the help they would provide fell into the following categories: talking to him or providing support (84.6%, 95% CI = [77.7, 90.0]), communicating with family (9.4%, 95% CI = [5.2, 15.3]), adjusting workload or roster and/or removing from operational duties (47.7%, 95% CI = [39.4, 56.0]), removing firearm Operational Safety Training qualification (3.4%, 95% CI = [1.1, 7.7]), advising station command or supervisors (29.5%, 95% CI = [22.3, 37.5]), encouraging help-seeking or seeking help on John’s behalf (87.9%, 95% CI = [81.6, 92.7]), and accessing peer support or police union assistance (28.2%, 95% CI = [21.1, 36.1]).
Recent helping behaviours
A substantial percentage of respondents reported having worked with someone with a mental health problem in the previous 6 months: 42.2% (95% CI = [38.6, 46.0]) overall said yes, only 15.2% (95% CI = [12.7, 18.1]) said no and 42.5% (95% CI = [38.9, 46.2]) said they did not know.
A much smaller percentage of lower ranks reported having worked with someone with a mental health problem (36.8%, 95% CI = [32.7, 41.0]) compared to leaders (60.2%, 95% CI = [52.4, 67.7]). When asked what affirmative respondents thought what the mental health problem was, a wide range of responses were reported. These included non-specific or general responses (e.g. ‘personal issues’), specified diagnoses (e.g. depression, posttraumatic stress disorder [PTSD], bipolar disorder), symptom descriptors (e.g. hopelessness, insomnia), factors external to work (e.g. relationship difficulties) and work-related factors (e.g. work pressures, inadequate performance).
Among those who reported working with someone with a mental health problem, most had offered help of some kind, 76.1% (95% CI = [64.5, 85.4]) of lower ranks had tried to help while for leaders, this proportion was 88.7% (95% CI = [80.6, 94.2]). The most commonly reported actual helping behaviour among lower ranks and leaders was that of ‘talking to the person’ (see Table 4). Leaders were more likely to facilitate professional help than lower ranks. Among leaders, 94.2% (95% CI = [87.0, 98.1]) said they recommended professional help, 77.9% (95% CI = [67.7, 86.1]) offered to help make an appointment and 84.9% (95% CI = [75.5, 91.7]) followed up with the person.
Percentage (and 95% CI) of respondents offering different types of help to fellow police members who might have had mental health problem in the previous 6 months.
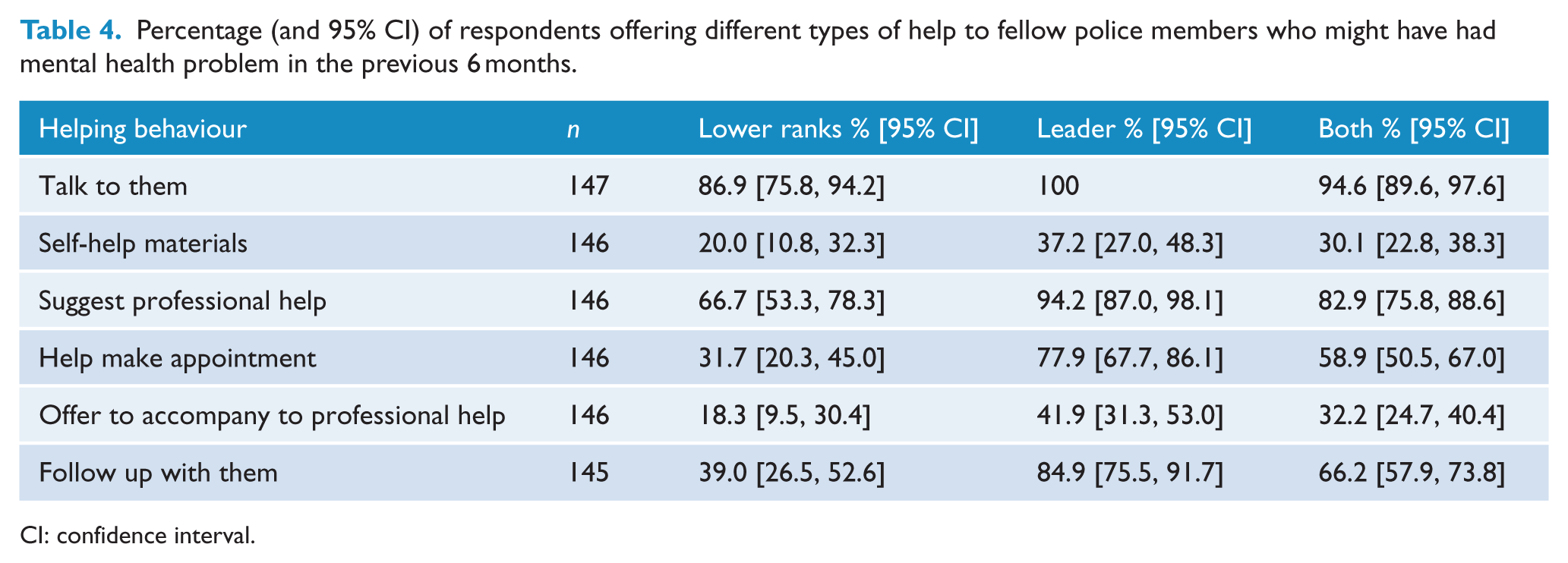
CI: confidence interval.
Recent help-seeking behaviours
When asked if they had sought professional help for a mental health problem of their own in the previous 6 months, 73.7% (95% CI = [70.3, 76.9]) of respondents said they had not had a problem. Among those reporting that they had problems, 12.1% (95% CI = [9.8, 14.7]) had sought help while 14.2% (95% CI = [11.7, 17.0]) had not sought help. Among those who had sought help, sources of help are given in Table 5. GPs were the most commonly nominated source of help.
Percentage (and 95% CI) of respondents who sought help from professional sources for a mental health problem in the previous 6 months (if they experienced a mental health problem in the previous 6 months).
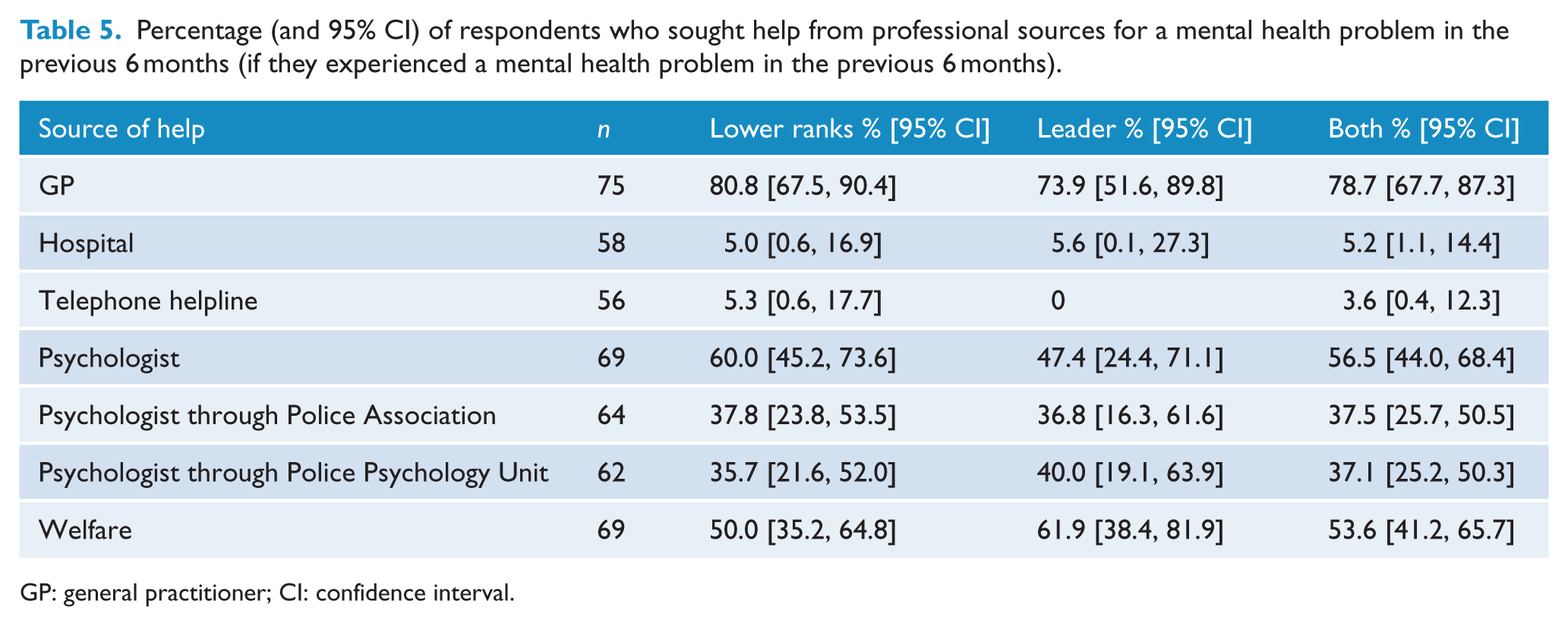
GP: general practitioner; CI: confidence interval.
Personal depression stigma
The proportions of respondents agreeing or strongly agreeing with the statements about the person described in the vignette are given in Table 6, which shows that avoiding the person was the statement with which respondents were least likely to agree. Respondents were most likely to agree that the person’s problem made him unpredictable.
Percentage (and 95% CI) of respondents who ‘agree’ or ‘strongly agree’ with statements about personal attitudes to mental disorders.
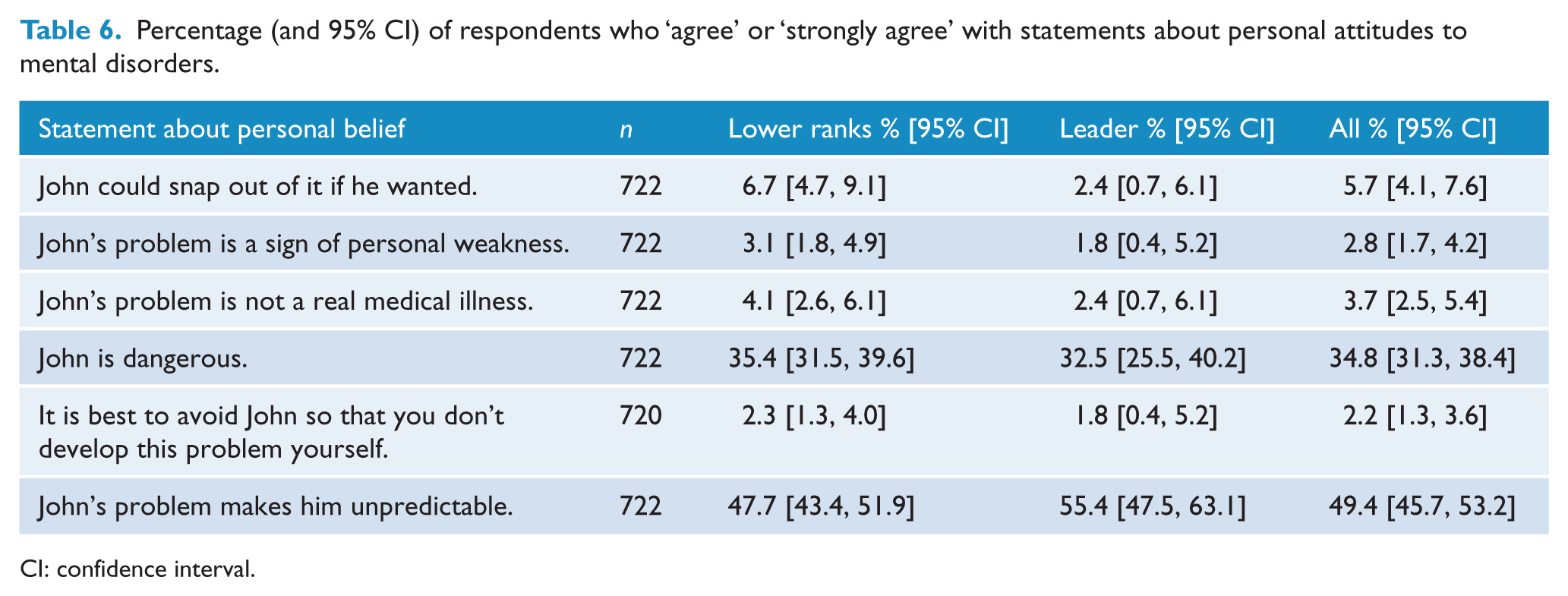
CI: confidence interval.
Discussion
This study, the first to comprehensively explore mental health literacy and helping behaviours for depression in Australian police, aimed to examine the mental health literacy profile of a sample of Australian police officers in order to inform mental health promotion strategies that may be tailored to this context.
Recognition of depression
Results showed that most police members could recognise depression in a vignette, with rates of recognition slightly higher in leaders than in lower ranks, although the difference did not reach statistical significance. When compared to surveys of the general population, rates of depression recognition were similar (Reavley and Jorm, 2011a). However, analysis of the open-ended responses showed that respondents were much more likely than those in the general population to mention workload pressures. This is possibly because of the circumstances surrounding the data collection in this study (baseline data collection for a job stress intervention) or may reflect police perceptions about their workload and the links to mental health (Houdmont, 2017). However, it may point to the need for education about the signs and symptoms of depression and suicidality among the lower ranks (Mishara and Martin, 2012). It is generally agreed that recognition of a problem is the necessary first step to seeking help from an appropriate professional, with failure to recognise signs and symptoms of mental disorder likely to delay help-seeking (Gulliver et al., 2010) and adversely impact long-term outcomes (McGorry et al., 2007; Wang et al., 2003). The use of correct psychiatric labels may facilitate communication with health professionals, and it has been shown that GPs are more likely to detect a mental disorder if the patient conceptualises their problem as such (Haller et al., 2009).
Beliefs about treatment
Beliefs about the helpfulness of interventions also impact on help-seeking and treatment compliance. When compared to beliefs in general population studies, leaders’ beliefs about the helpfulness of GPs, psychologists and psychiatrists were similar (Reavley and Jorm, 2011a). Police psychology services also received high ratings of helpfulness. Beliefs about the helpfulness of antidepressants were considerably lower than the general population: 30% versus 64% (Reavley and Jorm, 2011a). This is concerning given the severity of the symptoms described in the vignette, as such beliefs can affect treatment outcomes. For example, it has been found that depressed patients who have negative attitudes towards antidepressants are less likely to be prescribed these medications, less likely to fill prescriptions and less likely to benefit overall (Pyne et al., 2005). Moreover, beliefs about the helpfulness of physical activity and cutting out alcohol were also lower than in the general population (75% vs 96% for physical activity and 47% vs 77% for cutting out alcohol). As there is evidence of benefit of both these self-help strategies (Berk et al., 2013; Morgan et al., 2013), these may point to the need for police mental health education to have a greater focus on evidence-based medical and self-help interventions.
Help-giving intentions and behaviours
When asked about their willingness to assist a co-worker like the person described in the vignette, leaders strongly agreed that they would and had high levels of confidence in doing so. Most reported that they would offer multiple forms of help – most commonly that they would talk to ‘John’, encourage or assist with help-seeking, and adjust workload or remove from operational duties. In contrast, very few (~3%) suggested that they would remove the officer’s firearm. All respondents were asked about their contact with people with mental health problems over the previous 6 months and whether they tried to help the person. Leaders were more likely than lower ranks to have known and helped a person with a mental health problem, possibly reflecting the higher levels of mental health literacy in leaders (arising from participation in previous training) or a greater likelihood of disclosure of mental health problems to supervisors than colleagues (Reavley and Jorm, 2014). When compared to studies in the general population (Rossetto et al., 2014) and US police (Mishara and Martin, 2012), helping behaviours were more commonly reported in both leaders and lower ranks, possibly reflecting increased attention to mental health problems in police in recent years.
Help-seeking intentions and behaviours
Among both lower ranks and leaders with mental health problems, the proportion of those unlikely to seek professional help was slightly greater than those who were likely to seek it. While interpretation of these findings does depend on the person’s definition of ‘mental health problems’, there is some evidence from the open-ended responses suggesting that respondents interpreted this question as referring mostly to depression and PTSD and that these are more likely to require professional assistance than ‘stress’. Thus, mental health education should aim to overcome barriers to early professional help-seeking for potential mental health problems. Among those who had sought help, GPs were the most common source, particularly among lower ranks. Help-seeking from GPs was also the most commonly nominated option in relation to future help-seeking. Thus, despite high ratings of helpfulness of police psychology services, respondents appeared to prefer seeking help outside the police, possibly due to concerns about confidentiality, impact on career progression or being seen as weak, cowardly or unable to perform their role effectively (Barocas and Emery, 2017). This was particularly the case for lower ranks as opposed to leaders. Just under half of respondents expressed an intention to seek help from colleagues, pointing to the complementary value of peer support programmes (Barocas and Emery, 2017; Dowling et al., 2006; Levenson and Dwyer, 2003).
Personal depression stigma
When asked about their attitudes towards ‘John’, lower ranks and leaders did not differ. The majority of police were not likely to believe that depression was a weakness rather than an illness. However, compared to the general population, attitudes relating to depression not being a real illness appear to be less of an issue in police, with percentage agreement ranging between 3% and 5%, compared to 10–18% in the general population (Reavley and Jorm, 2011b). However, belief in the dangerousness of John was higher in the police (35% vs 28% in the general population). This may be because police work can involve exposure to extreme situations with very distressed people presenting with mental health problems. In addition, when a mental health problem affects a fellow police member, that person may be seen as dangerous if armed. However, beliefs about unpredictability were lower than in the general population 49% versus 59%. This requires further investigation to fully understand.
Strengths and limitations
Study strengths include the use of established measures with benchmarks for comparison, and the large sample and strong response rate (70%). We would acknowledge, however, that our results may also be affected by response bias (such as those with mental health concerns or experiences being more likely to respond to the surveys) and that, strictly speaking, our results generalise only to station-based general duty police members.
Implications for policy and practice
Beliefs about evidence-based interventions were lower in this sample of police officers than in the general population, pointing to the need for increased evidence-based education and training to improve mental health literacy in these areas. Such programmes should also aim to reduce stigma and to overcome other barriers to professional help-seeking, given that the proportion of police with mental health problems who would not seek help is greater than the proportion who would. These results can help to inform growing efforts to protect and promote the mental health of police and emergency service workers in Australia and internationally. Locally, these results provide specific information to inform the development of mental health literacy programmes in Victoria Police, and nationally, these findings can inform the ongoing police and emergency services mental health initiative (beyondblue, 2014).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The study was funded by Partnership Project funding (APP1055333) from the Australian National Health and Medical Research Council, including contributions from the Victorian Health Promotion Foundation (Melbourne), WorkSafe Victoria and Victoria Police.