
Abstract
Objectives:
The taxi industry relies on a male-dominated, predominately immigrant workforce who face multiple risk factors for poor mental health including shift work, low pay and threats of violence. Despite these risk factors, no previous study has documented the prevalence of psychological distress in the taxi industry. We investigated psychological distress among urban taxi drivers and explored the factors associated with high levels of distress.
Method:
A total of 380 taxi drivers were surveyed at the Melbourne Airport holding yard between September 2016 and March 2017. Psychological distress was measured using the K10. Logistic regression models were used to estimate the association between high levels of psychological distress and migration, work patterns, potentially traumatic events, health care use and social connectedness.
Results:
A third (33%) of drivers had very high (K10 ⩾ 30) levels of distress and 28% had high (K10 = 22–29) levels of distress. Trauma was significantly associated with high levels of psychological distress, and rates of trauma were much higher among drivers than among the Australian population. Despite high levels of distress, drivers were no more likely than other Australian men to visit a health professional.
Conclusion:
Urban taxi drivers are at very high risk for mental health problems, yet the mental health needs of this largely immigrant workforce has gone largely unnoticed. Interventions tailored to the unique characteristics of the job and the demographic composition of the workforce are urgently needed.
Background
Taxi driving is a heavily male-dominated industry, and in countries like Canada, Australia and the United States, the majority of drivers are immigrants (KPMG, 2011; Schaller Consulting, 2004; Xu, 2012). Taxi drivers face many challenges to good mental health, including long hours and shift work combined with a low and unreliable income which is lowered further by fare evasion (Facey, 2010; Machin and De Souza, 2004; Nieuwenhuijsen et al., 2010). Drivers frequently experience verbal abuse, which is often racist in nature, and they are at significant risk of physical assault (Burgel et al., 2012; Gany et al., 2013; Mayhew, 2000; Ministry of Transport, 2007). Compared to workers in other high-risk occupations (e.g. policing and firefighting), taxi drivers are more likely to experience workplace violence and homicide (Mayhew, 2000; Wang and Delp, 2014). Recently, drivers in many countries have also experienced increasing competition, and often a reduction in income, from ride-sharing services which, in many jurisdictions, have not been bound by the same regulations that govern taxi drivers (Dosen, 2016).
There are almost 300,000 taxi drivers in the United Kingdom, over 230,000 in the United States and 68,000 in Australia (Australian Taxi Industry Association, 2014; Bureau of Labor Satatistics, United States Department of Labor, 2016–2017; Department for Transport, 2015). Despite the substantial workforce, and the many threats to good mental health they face, few studies have examined mental health among taxi drivers and none have documented rates of psychological distress in this population. Currently, the best available evidence on the psychological wellbeing of drivers is from studies primarily investigating physical health and safety. In a study of cardiovascular risk factors among San Francisco drivers, 14% reported that they had ever been diagnosed by a doctor with depression. However, given that only 46% of participants had a regular health care provider and only 42% had medical insurance, opportunities for doctors to detect psychological problems were relatively rare and the real rate of psychological distress is likely to be much higher (Elshatarat and Burgel, 2016). In a study of Los Angeles taxi drivers, 54% of participants reported high job stress; however, a validated measure of psychological distress was not used and it is unclear to what extent job-related stress represents overall psychological wellbeing (Wang and Delp, 2014).
It is possible that the numerous risk factors associated with taxi driving are buffered by factors known to be protective against psychological distress. For example, two meta-analyses have found strong evidence of a beneficial effect of social support from co-workers and having control over work (i.e. high decision latitude) on workers’ mental health (Nieuwenhuijsen et al., 2010; Stansfeld and Candy, 2006). Qualitative studies report that drivers enjoy a high level of camaraderie with their colleagues and that they value being their own boss (Luedke, 2010). Drivers who are immigrants also report that they appreciate the flexibility of being able to return to the job after taking extended breaks while visiting their home country (Luedke, 2010). The taxi workforce may also benefit from the ‘healthy migrant effect’ which is observed in many countries due to the stringent health checks immigrants must pass before settling in their new country and because people in poor health are less likely to migrate (Anikeeva et al., 2010; Slade et al., 2009).
Prevalence data on the psychological wellbeing of taxi drivers will help to assess the level of need for mental health support in the industry. Identifying factors associated with psychological distress can also inform the development of appropriate workplace interventions. The aim of this study was to estimate the prevalence of psychological distress among urban taxi drivers and identify the factors associated with distress.
Methods
Design, setting and recruitment
A cross-sectional survey of taxi drivers recruited from the Melbourne Airport taxi holding yard was conducted between September 2016 and March 2017. The holding yard comprises over 300 parking spaces where drivers wait until it is their turn to enter the rank at the arrivals terminal to collect passengers. Waiting times range from 15 minutes to several hours. During this time, drivers socialise with colleagues, walk the perimeter of the yard, buy food from the café or use the non-denominational prayer room. Almost 100% of active taxi drivers in the Melbourne metropolitan area attend the holding yard during their working week because fares from the airport are potentially the most lucrative. Researchers visited the holding yard at different times of the day and evening on different days of the week over the survey period. Non-probability convenience sampling was used to recruit drivers who were approached by researchers at the holding yard or, more commonly, when drivers approached the researchers to enquire about the project. Drivers who provided verbal consent either completed the 10-minute survey themselves or with the assistance of one of the researchers. This study was approved by the Human Research Ethics Committee of the University of Melbourne (ID: 1545951).
Variables
Main outcome measure
We used the Kessler Psychological Distress Scale (K10) to measure psychological distress as it is a brief, easy to use, validated self-report measure (Kessler et al., 2003). The K10 has reasonable ability to discriminate between cases and non-cases of depression and anxiety disorders in the general population (Furukawa et al., 2003; Kessler et al., 2003) and has been used in the US National Comorbidity Survey Replication and in the national surveys that comprise the World Health Organization’s World Mental Health Initiative, including the Australian National Survey of Mental Health and Wellbeing (Andrews and Slade, 2001; Furukawa et al., 2003). The scale comprises 10 questions asking about the frequency of depression and anxiety symptoms over the past 4 weeks. Respondents rate each item on a five-point scale ranging from ‘none of the time’ (value = 1) to ‘all of the time’ (value = 5) and scores are summed with a possible range of 10–50. A score of 10–15 represents low psychological distress, 16–21 represents moderate psychological distress, 22–29 represents high psychological distress and 30–50 represents very high psychological distress (Andrews and Slade, 2001). In the inferential analysis, the K10 was treated as a binary variable with scores ranging from 10 to 21 coded as ‘0’ and scores ranging from 22 to 50 coded as ‘1’.
Predictor variables
Five categories of predictor variables were selected on the basis that they have previously been found to be associated with psychological wellbeing and because they have particular relevance to the taxi industry (Anikeeva et al., 2010; KPMG., 2011; Mayhew, 2000; Nieuwenhuijsen et al., 2010).
Immigration status
Participants recorded their country of birth and, if relevant, the year they settled in Australia. Country of birth was grouped into seven categories with Australia as a stand-alone category and the remaining countries grouped into six regions as defined by the United Nations (www.internetworldstats.com/list1.htm). For the analysis, participants were classified as Australian-born or non-Australian born. Participants who were born outside Australia were further classified as a recent immigrant (arriving in Australia within the last 10 years) or a longer-settled immigrant (arriving more than 10 years previously). Year of immigration was the final question on the survey and this item had a high level of missing data (15%) as some drivers were required to return to their car before finishing the survey. Therefore, only the binary variable (Australian born cf. non-Australian born) was used in the inferential analysis.
Work patterns
We asked participants whether they currently worked night shift (yes/no), the number of hours they typically worked each week and the number of years they had worked as a taxi driver.
Trauma
Lifetime exposure to seven potentially traumatic events (PTEs) was drawn from the list of PTEs used in the Australian 2007 National Survey of Mental Health and Wellbeing (NSMHWB; Mills et al., 2011). Participants were asked whether they had ever seen someone badly injured or killed or unexpectedly seen a dead body; been in a life-threatening car accident; been in another life-threatening accident; been mugged, held up or threatened with a weapon; been beaten up badly; done something that accidentally led to the serious injury or death of another person and experienced any other PTE. These PTEs were selected on the basis that they may have been experienced while driving a taxi. We asked about lifetime exposure so that we could compare our results with that from the national survey which means that these events were not necessarily experienced while working as a taxi driver.
Social contact
Social contact was measured using two questions from the Australian Bureau of Statistics General Social Survey (Australian Bureau of Statistics, 2015a). Participants were asked how often they are in contact with members of their family, including face-to-face visits, phone calls, letters or electronic communication. The same question was asked in relation to contact with friends. Responses were scored on a six-point response scale ranging from ‘never’ to ‘nearly every day’. Drivers who reported that their combined contact with friends and family was less than 3 days a month were classified as socially isolated.
Health service use
Two questions on health service use were drawn from the National Health Survey to assess frequency of health service use (Australian Bureau of Statistics, 2012). Participants were asked how often in the last 12 months they had visited (1) a primary care doctor and (2) a medical specialist.
Covariates
Participants were asked their age, highest level of education and marital status. Age was grouped into three categories: 20–29 years, 30–49 years and ⩾50 years. For the analysis, marital status was treated as a binary variable (married/unmarried).
Sample size
There are approximately 12,000 active taxi drivers in the Melbourne metropolitan area (Taxi Services Commission, 2015). Because no previous surveys on the mental health of taxi drivers exist, the expected proportion of drivers with psychological distress was unknown, therefore we used a conservative (i.e. 50%) estimate of variance to calculate the sample size. Allowing for a ±0.05% margin of error and a 95% confidence level, we calculated that the required sample size was 373.
Statistical methods
Analysis was performed using complete case analysis. The data were described using frequencies and percentages. Logistic regression models were used to estimate unadjusted associations between high psychological distress and migration; work patterns; PTEs; social contact and health service use. Multivariate logistic regression models were used to estimate these associations when adjusted for age, education and marital status. Results are reported as odds ratios (ORs) with 95% confidence intervals (CIs) and p values (p). Analysis was conducted using STATA version 13.1.
Results
Participants
A total of 380 taxi drivers completed a survey. Missing data ranged from 0.0% to 6.1% across all survey items except ‘Time since settling in Australia’ which had 15% missing data; 98% of participants were male and the average age was 40.7 years (standard deviation [SD] = 12.12 years; Table 1). Overall, 92.8% of participants were immigrants and 45.9% of those had settled in Australia within the last 10 years. Drivers were most likely to have been born in India (36.6%), Pakistan (17.6%) or Somalia (8.7%). Just under three-quarters (74.4%) of participants were married and most (69.1%) lived with family members. The higher proportion of married drivers than drivers who lived with family members is explained by anecdotal reports from drivers that their spouse was currently living in another country while awaiting an Australian visa. More than half (53.7%) of the sample had a bachelor degree or higher.
Characteristics and work patterns of study participants (n = 380).
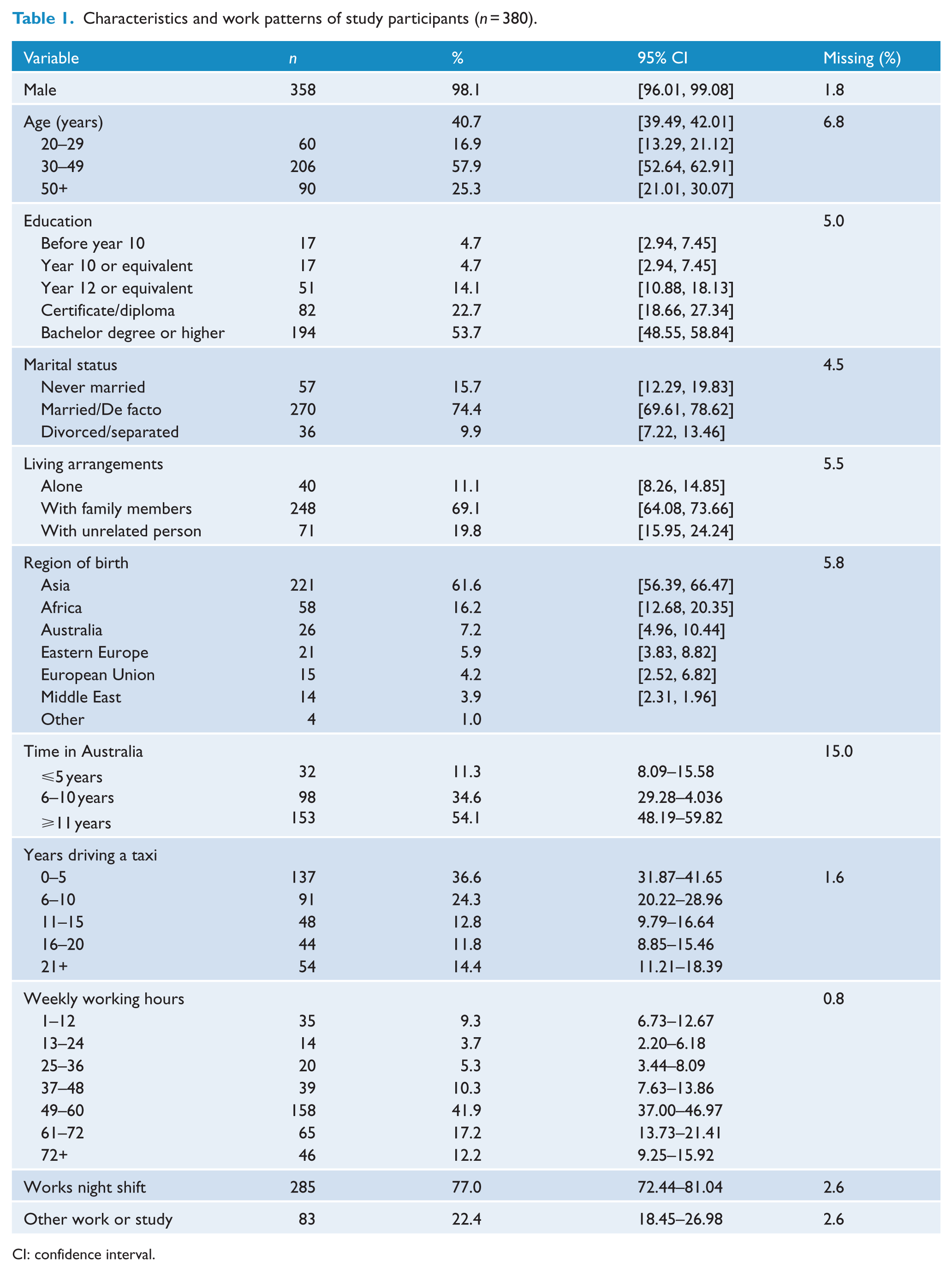
CI: confidence interval.
Driving patterns
Participants reported they had driven taxis for an average of 10.7 years (SD = 8.67 years) with a range of 3 months to 38 years. More than a third (36.6%) reported they had driven taxis for 5 years or less, while 26.2% reported driving taxis for 16 years or more (Table 1). Weekly working hours were typically long with an average of 51.6 hours (SD = 19.6 hours; range: 5–84 hours). Most participants (77.0%) worked night shift at least occasionally and 22.4% were also undertaking other work or study.
Psychological distress
The mean K10 score was 24.73 (SD = 8.04) with a range of 10–46. One-third (33.3%) of the participants had high levels of psychological distress and 28.3% had very high levels of psychological distress. Only 14.6% of participants scored in the low range (Table 2).
Psychological distress, self-rated health and trauma among taxi drivers (n = 380).
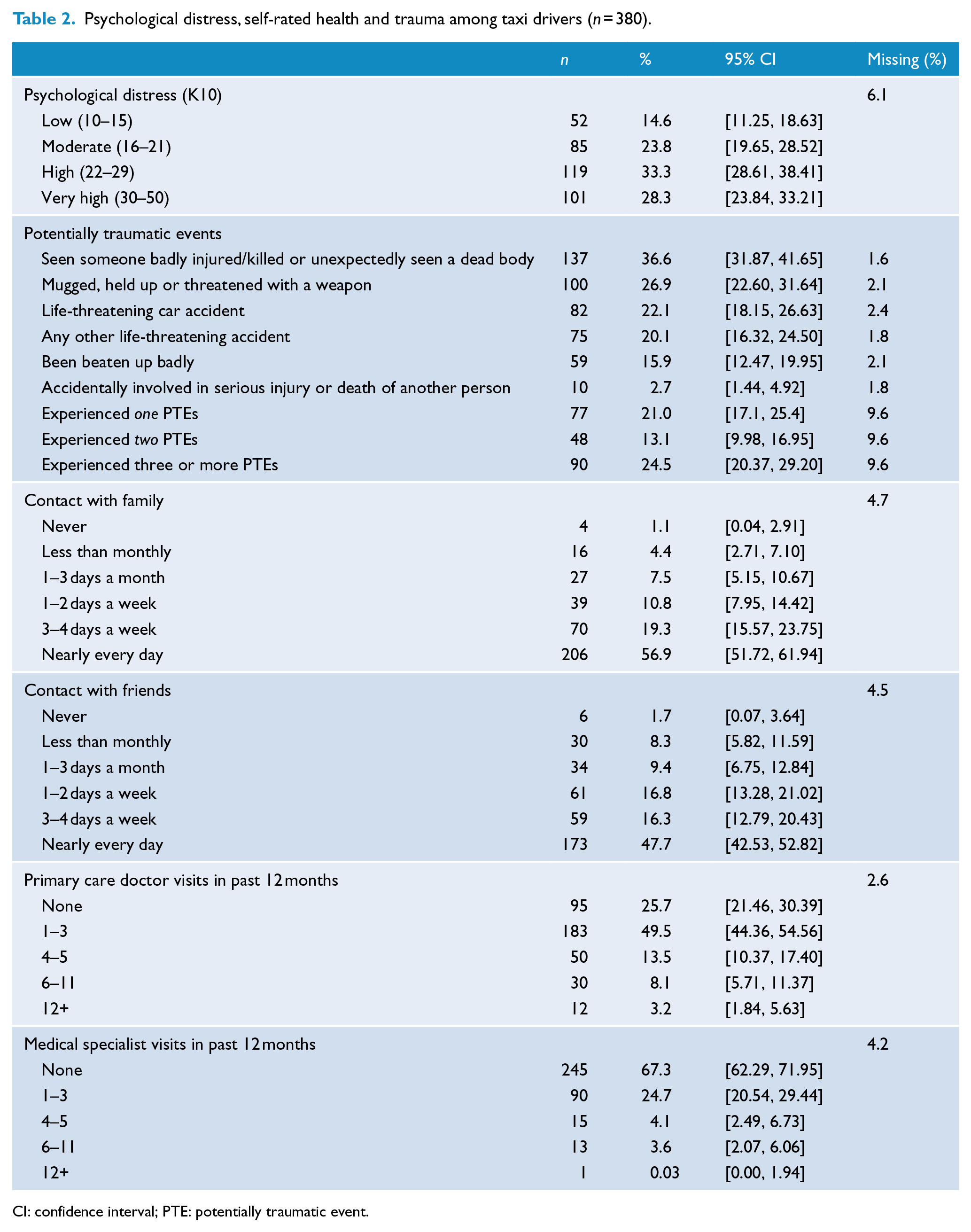
CI: confidence interval; PTE: potentially traumatic event.
Experience of trauma
Overall, 58.6% of participants reported experiencing at least one PTE. Just over a fifth (21.0%) reported one PTE, 13.1% reported two PTEs and 24.5% reported three or more PTEs (Table 2). More than a quarter (26.9%) of participants reported having been mugged, held up or threatened with a weapon at least once in their life and 15.9% reported having ever been beaten up badly. A life-threatening car accident had been experienced by 22.1% of participants and another life-threatening accident had been experienced by 20.1%.
Social contact
Levels of social contact were generally high (Table 2). Over three-quarters (76.2%) of participants were in contact with their family three times a week or more and 64.0% were in contact with friends at least 3–4 days a week. However, a small proportion (7.7%) of drivers reported that they had contact with friends and family less than three times a month and can be considered socially isolated.
Health service use
A quarter (25.7%) of participants had not seen a primary care doctor in the past 12 months and two-thirds (67.3%) had not seen a medical specialist. Of those who had seen a general practitioner (GP) at least once, the average number of visits was 3.4 (SD = 3.32; range = 1–24), and of those who had seen a specialist at least once, the average number of visits was 2.5 (SD = 2.1; range = 1–12).
Characteristics associated with psychological distress
Six of the seven PTEs we measured were significantly associated with high to very high psychological distress in both the unadjusted and adjusted analysis (Table 3). The strongest individual predictors of distress were having been in a non-vehicular, life-threatening accident (OR = 5.13, 95% CI = [2.44, 10.77], p = 0.001); having been badly beaten up (OR = 3.09, 95% CI = [1.50, 6.35], p = 0.002) and having been mugged or threatened with a weapon (OR = 2.44, 95% CI = [1.40, 4.25], p = 0.002). The likelihood of high or very high psychological distress increased significantly if a participant reported experiencing three or more PTEs in their life (OR = 5.24, 95% CI = [2.68–10.28], p = <0.001).
Unadjusted and adjusted logistic regression models estimating the predictors of psychological distress among taxi drivers.
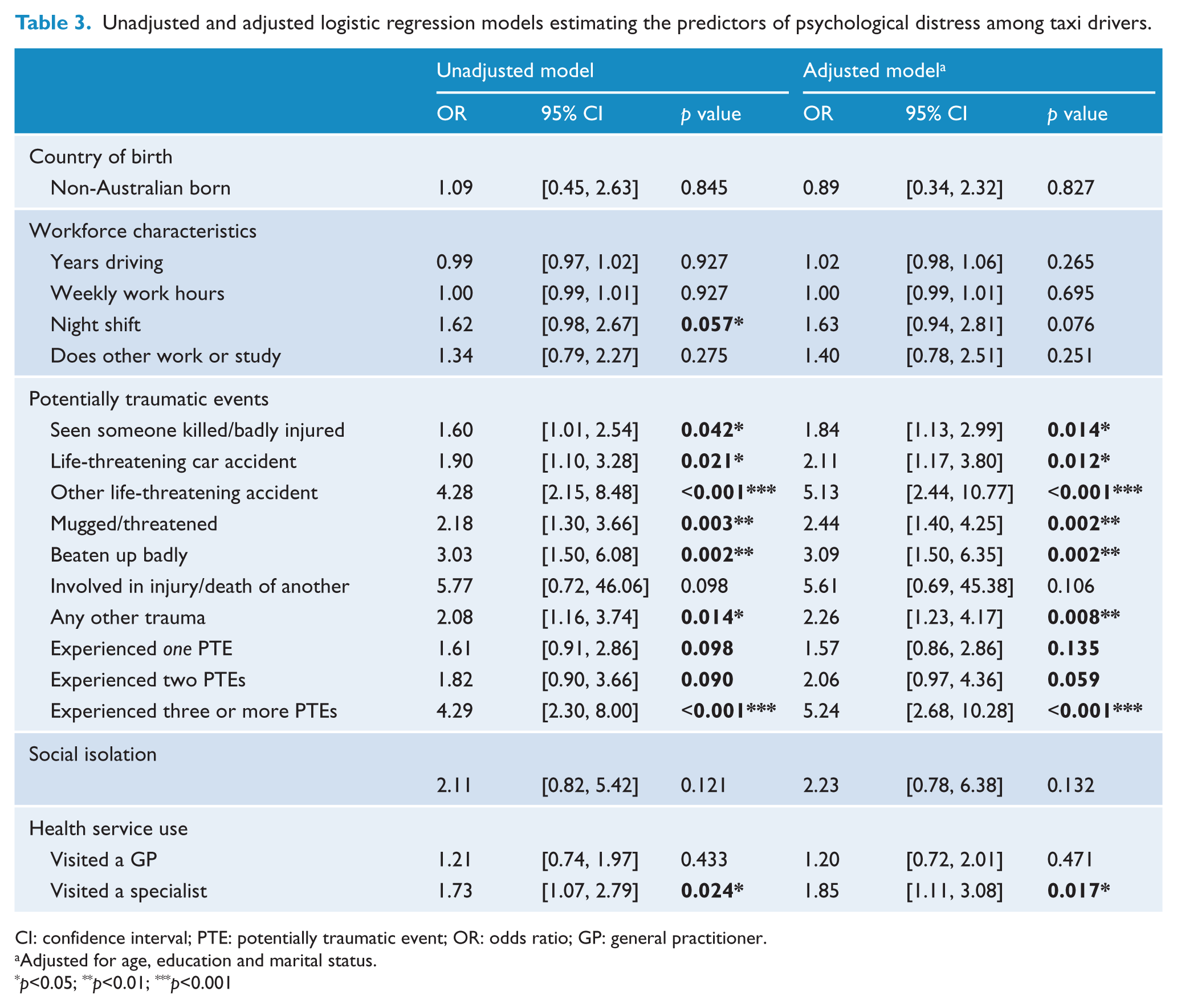
CI: confidence interval; PTE: potentially traumatic event; OR: odds ratio; GP: general practitioner.
Adjusted for age, education and marital status.
p<0.05; **p<0.01; ***p<0.001
Visiting a medical specialist in the past 12 months was a significant predictor of high to very high psychological distress in both the unadjusted and adjusted analysis (OR = 1.85, 95% CI = [1.11, 3.08], p = 0.01).
Of the workforce characteristics examined, only night shift was significantly associated with psychological distress in the unadjusted analysis (OR = 1.62, 95% CI = [0.98, 2.67], p = 0.05), and no workforce variables (i.e. night shift, hours worked per week, years working as a taxi driver and other work or study) were significant in the adjusted analysis. Immigration and social isolation were not associated with high psychological distress.
Discussion
This is the first study to investigate rates of psychological distress among the male-dominated, predominately immigrant workforce of urban taxi drivers and it provides important baseline information about mental health in the taxi industry. We found extremely high levels of psychological distress with a third (33%) of drivers scoring in the high range, 28% scoring in the very high range and only 15% scoring in the low range. The pattern of psychological distress in our sample is the reverse of the pattern found among men in Australia’s national statistics which show that 68% of the male population score in the low range, 8% score in the high range and only 4% score in the very high range (Australian Bureau of Statistics, 2015b). The pattern of distress among taxi drivers is also unlike that found in other male-dominated industries, which tend to follow the same overall pattern as the general population (Roche et al., 2016) and unlike that of the wider population of immigrants in Australia who have slightly lower rates of mental health problems compared to the Australian-born population (Slade et al., 2009). The distribution of psychological distress scores we found among urban taxi drivers is comparable to the distribution reported in studies focusing on migrant groups from high conflict countries. For example, Nguyen et al. (2016) found that 44% of Vietnamese adults attending Vietnamese-speaking primary care clinics in Sydney had high to very high distress on the K10, while Slewa-Younan et al. (2015) found that 59% of resettled Iraqi refugees in Australia scored in this range (Nguyen et al., 2016).
Taxi drivers were twice as likely as other Australian men to have been in a life-threatening accident (20% cf. 9%), they were almost a third more likely to have been threatened or assaulted with a weapon (27% cf. 17%), a third more likely to have been badly beaten up (16% cf. 10%) and a fifth more likely to have been in a life-threatening car accident (22% cf. 17%; Mills et al., 2011). Importantly, a quarter of all drivers (41% of those with any PTE exposure) reported they had experienced three or more PTEs in their life. The cumulative effect of repeated PTE exposure is well known, with evidence suggesting that the number of events experienced is more strongly associated with psychological distress than the nature of the events themselves (Dobson et al., 2012). Given that we assessed only a handful of PTEs the true rate of experiencing multiple PTEs may be much higher than reported here.
Consistent with previous studies, trauma was a significant predictor of psychological distress (Nguyen et al., 2016; Williams et al., 2007). Unfortunately, we cannot clarify whether these PTEs occurred while working as a taxi driver or whether they occurred in another setting, and we do not know how recently they occurred. Many drivers come from countries with high rates of conflict and it is highly likely that some participants’ exposure to PTEs occurred prior to immigration. However, at the same time, our findings are consistent with what is known about high rates of assault and violence directed towards taxi drivers and is supported by anecdotal evidence provided by drivers in this study (Ministry of Transport, 2007). Furthermore, our approach to assessing PTE exposure, which does not distinguish between work-related trauma and non-work-related trauma, is consistent with that taken in other organisational settings such as the military (McFarlane et al., 2010).
Increasing safety and reducing the rate of assault and violence experienced by taxi drivers is likely to make a significant impact on the psychological wellbeing of taxi drivers of the future. However, drivers who are currently experiencing high rates of psychological distress, either due to past trauma or due to their work as a driver, have a need for immediate mental health support. Only 15% of drivers could be classified as experiencing good mental health (Andrews and Slade, 2001). Just under a quarter of drivers had moderate levels of distress indicating they are experiencing symptoms of depression or anxiety, and which are likely to respond to self-help or low-intensity strategies (Andrews and Slade, 2001; National Institute for Health & Clinical Excellence, 2010). A third of drivers scored in the high range which indicates they are likely to be experiencing symptoms of depression or anxiety for which low-intensity treatments may provide some benefit. Just over a quarter scored in the very high range which indicates that they are likely to be experiencing depression or anxiety, and which evidence suggests they would benefit from pharmacological and/or psychological treatments (Andrews and Slade, 2001; National Institute for Health & Clinical Excellence, 2010).
However, our results suggest that taxi drivers are not seeking help for their mental health at the level they need. Although drivers were just as likely as other men in Australia to have visited a primary care doctor or medical specialist (primary care doctor = 74% drivers cf. 75% Australian men; medical specialist: 34% drivers cf. 33% Australian men; Australian Bureau of Statistics, 2016), the much higher rate of distress among drivers suggests that there is a substantial unmet need for professional help in this population. By way of comparison, an Australian population study by Andrews and Slade (2001) found that people with very high distress had an average of eight consultations in the past year specifically for their mental health, whereas we found that drivers with very high distress had an average of 4.5 consultations for any reason in the same time period. The lower rate of health care use among taxi drivers is consistent with a cardiovascular risk factor study of New York cab drivers (Gany et al., 2014) as well as a systematic review showing that immigrants generally use health services less often than the native-born population (Sarría-Santamera et al., 2016). Multiple factors contribute to low levels of help seeking among men who are from culturally and linguistically diverse backgrounds (CALD). Many are reluctant to talk about their mental health due to stigma (Reavley and Jorm, 2011), many do not have the tools or confidence to start a conversation about how they are feeling and some have difficulty recognising their symptoms as a mental health issue (Hughs, 2012). Additionally, men from CALD backgrounds may face barriers in understanding and navigating the Australian health system and may have a cultural framing of mental health inconsistent with available pathways to help (Hughs, 2012; Kokanovic et al., 2008).
Strengths and limitations
A limitation of this study is the convenience sampling methodology which means we were not able to calculate a response rate for the survey and the sample may not be representative of all Melbourne taxi drivers. It is possible that some ethnic or cultural groups were not adequately represented, especially those with weaker English language skills. Of note, most respondents were from India and Pakistan, countries in which English is widely spoken. It is also important to note that these findings are not generalisable to drivers working in regional and rural areas which are known to have a higher proportion of female drivers and Australian-born drivers and where drivers may have stronger links with the local community.
Another limitation is that we did not ask participants about their migration status (e.g. temporary visa holder, permanent resident or citizen) or whether they were humanitarian refugees. As such, we cannot disentangle how much of the psychological distress and trauma we found among taxi drivers was associated with their work as a taxi driver and how much was associated with their immigration and pre-immigration experiences. As stated previously, many drivers have immigrated from countries with a high rate of current or recent conflict, and it is highly likely that many of the reported PTEs occurred prior to settling in Australia and beginning working as a taxi driver in Melbourne.
We also relied on self-report measures. The local taxi industry and the government department responsible for their regulation are currently engaged in a heated political debate over the regulation of ride-sharing services and the separate issue of de-valuing taxi licence plates. It is possible that participants exaggerated their reports of distress to express their frustration with the situation.
Finally, when we compared rates of psychological distress between our sample of urban taxi drivers and Australian men, we did not control for age or socioeconomic status, both of which may be associated with levels of distress. Therefore, direct comparisons between rates of psychological distress among drivers and Australian male norms should be made with caution.
Conclusion
Taxis are essential for a functional transportation system in cities across the world. Although the industry is changing with the emergence of ride-sharing companies, whether someone is driving for a traditional taxi company or a new service, the nature of the job is essentially the same, characterised by long hours, sedentary behaviour, low pay and a predominately immigrant workforce. While some of the technological tracking features of ride-sharing services may increase safety for drivers, the unregulated status of the service places them at risk of exploitation (Warren, 2016). It is likely that the high rates of psychological distress we found among urban taxi drivers would also be found among drivers of ride-sharing services.
Our finding that people working as taxi drivers are much more likely than the general male population to have high levels of psychological distress yet have comparatively low health service use suggests that there are substantial unmet mental health needs in this large workforce. Although the study has limitations, in that we could not establish the degree to which workforce factors, trauma and immigration and/or resettlement contributed to the high rate of distress, it clearly identifies a population of predominately men and immigrants in need of targeted mental health interventions. It is important that the mental health needs of this population are recognised and acted upon, not only for the individuals themselves but also for their families and the public with whom they interact on a daily basis.
It can be difficult to identify and improve men’s mental health in a way that is non-stigmatising. Using work-based approaches to improve men’s mental health has some evidence of effectiveness although definitive randomised controlled trials are lacking (Lee et al., 2014). Therefore, designing an intervention specifically for taxi drivers is worth considering and testing. The finding that many taxi drivers are immigrants, and that they have a higher rate of PTEs, suggests that interventions should be trauma informed. In conclusion, taxi drivers are a vulnerable, hard-to-reach, immigrant population for whom mental health interventions that are tailored to the unique characteristics of the job and the demographic composition of the workforce are urgently needed.
Footnotes
Acknowledgements
The researchers would like to thank all the drivers who participated in the survey and those who shared their stories. They also thank Michael Carollo and his staff for allowing them to conduct the survey in front of their café and to Georgia Halliday and Georgia Nichols from the Victorian Taxi Association for organising access to the holding yard. They also thank Melbourne Airport Transport Management for allowing access to the holding yard. The researchers would also like to acknowledge Ms Teresa Soderlund who assisted with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by the National Health and Medical Council (S. Davidson, Early Career Fellowship ID: 1071629N; N. Reavley, Career Development Fellowship ID: 1083394) and with seed funding from the Melbourne Networked Society Institute at the University of Melbourne.