
Abstract
Objective:
Over the past decade, cognitive behavioral therapy has been applied to an increasingly wider range of disorders and problems in Chinese societies. However, no meta-analysis has been conducted to synthesize the studies on cognitive behavioral therapy for Chinese clients. The purpose of this meta-analytic study was to examine the overall efficacy of cognitive behavioral therapy for Chinese people.
Method:
A literature search was conducted using electronic databases, including Web of Science, PsycINFO and PubMed. Pooled mean effect sizes were calculated using the random-effects model.
Results:
The literature search identified 55 studies with 6763 Chinese participants. The overall short-term effect of cognitive behavioral therapy on the primary outcome was medium in size. Effect sizes were medium for anxiety, depression/well-being and caregiving stress and small for psychotic symptoms and addictive behaviors. The effects of cognitive behavioral therapy on process variables, dysfunctional thoughts and coping, were in the small range. The overall longer-term effect of cognitive behavioral therapy on the primary outcome was medium in size. Moderator analyses showed that the short-term effect was stronger for culturally adapted cognitive behavioral therapy than for unadapted cognitive behavioral therapy. Type of primary outcome, type of control group, recruitment method, study design, the format of delivery and region were found to moderate the efficacy of cognitive behavioral therapy.
Conclusion:
The findings of this study provide evidence for the overall efficacy of cognitive behavioral therapy for Chinese people and the benefit of cultural adaptation of cognitive behavioral therapy to Chinese culture.
Introduction
Cognitive behavioral therapy (CBT) is one of the most widely used and extensively studied forms of psychotherapy (Butler et al., 2006; Hofmann et al., 2012). CBT refers to an array of interventions that are premised on the fundamental notion that individuals’ cognitions and thoughts influence their emotions and behaviors (Chu and Harrison, 2007; Kendall and Braswell, 1993). According to Beck (1970), psychological distress and behavioral problems are maintained by dysfunctional cognitions, which encompass general beliefs or schemas about the self, the world and the future, leading to automatic thoughts in specific circumstances. CBT assumes that reductions in dysfunctional cognitions through cognitive and behavioral techniques (e.g. cognitive restructuring, behavioral experiments, relaxation, social skills training) lead to reductions in mental health symptoms and behavioral problems (Hofmann, 2011).
Research has provided support for the efficacy of CBT for a wide range of psychological disorders and problems (Butler et al., 2006; Hofmann et al., 2012). A recent review identified 269 meta-analytic studies examining the efficacy of CBT for various disorders (Hofmann et al., 2012). Meta-analyses have found large effect sizes for CBT for adult depression (Gloaguen et al., 1998), adolescent depression (Reinecke et al., 1998), childhood depression (Grossman and Hughes, 1992), generalized anxiety disorder (Gould et al., 1997b), social phobia (Gould et al., 1997a), panic disorder with or without agoraphobia (Gould et al., 1995), and childhood anxiety (Grossman and Hughes, 1992), medium effect sizes for chronic pain (Morley et al., 1999), anger (Beck and Fernandez, 1998), and criminal behaviors (Illescas et al., 2001; Lösel and Schmucker, 2005), and small effect sizes for caregiving stress (Pinquart and Sorensen, 2006; Singer et al., 2007), psychotic symptoms (Jauhar et al., 2014) and addictive behaviors (Powers et al., 2008). Besides, several meta-analyses have investigated the effects of CBT on process variables (e.g. cognitive processes such as dysfunctional thoughts and threat interpretations, coping such as problem-solving skills and stress management skills) that mediate the treatment effect. One meta-analytic study found medium effect sizes for cognitive processes and coping (Chu and Harrison, 2007).
Scholars have postulated that the extent to which a form of psychotherapy is effective depends on its compatibility with clients’ cultural values and beliefs (Benish et al., 2011; Xu and Tracey, 2016). As most forms of psychotherapy have originated from Western societies emphasizing Western cultural values, such as individualism and future orientation (Griner and Smith, 2006; Lin, 2002), they might be less culturally appropriate for people from other cultural groups (Benish et al., 2011; Chowdhary et al., 2014). However, prior meta-analytic studies have rarely examined the efficacy of psychotherapy in non-Western cultures (Xu and Tracey, 2016). Therefore, more systematic studies are needed to understand the applicability of different forms of psychotherapy, such as CBT in non-Western contexts.
Over the past decade, CBT has become an increasingly popular formal practice in Chinese societies. Lin (2002) posited that CBT is compatible with Chinese culture because the intervention is structured and solution focused. This suggestion is based on the understanding that Asian clients (including Chinese clients) tend to have a lower tolerance for ambiguity and prefer structured therapy sessions with immediate and practical solutions to their problems (Leong, 1986). Moreover, Chinese people prefer therapists who adopt a directive rather than a non-directive approach. Therapists are perceived as effective by Chinese clients when they take partial responsibility for the process and play an active role in providing suggestions and advice (Lin, 2002). Although a growing body of research has investigated the effects of CBT on an increasingly diverse range of disorders and problems in Chinese populations, the overall efficacy of CBT for Chinese people remains unclear.
Scholars have proposed that because of the high degree of compatibility between CBT and Chinese values and beliefs, CBT will be an efficacious intervention for Chinese clients with appropriate cultural adaptations (Chen and Davenport, 2005; Hodges and Oei, 2007). Cultural adaptation of psychotherapy is defined as the systematic modification of intervention protocol to consider language, culture and context aimed at improving the compatibility of the treatment with clients’ cultural values, meanings and patterns (Bernal et al., 2009). Scholars have identified various types of cultural adaptations of psychotherapy, including explicit incorporation of cultural values and beliefs into the treatment, matching of the race or ethnicity between clients and therapists, provision of services in clients’ native language, consultation with people familiar with clients’ culture and cultural sensitivity training for staff (Benish et al., 2011; Chowdhary et al., 2014; Griner and Smith, 2006). In a meta-analysis of 21 studies, Benish et al. (2011) found that culturally adapted psychotherapy for ethnic and racial minorities in the United States was more effective than unadapted, conventional psychotherapy. Although a number of recent studies have examined the efficacy of culturally adapted CBT for Chinese clients (Wong, 2008a, 2008b; Wong and Poon, 2010; Wong and Sun, 2006; Wong et al., 2007, 2015, 2016a, 2016b), the relative efficacy of culturally adapted CBT versus unadapted CBT for Chinese clients has not yet been investigated.
This study endeavored to contribute to the literature by meta-analyzing studies on CBT for Chinese people. The purpose of this study was fourfold. First, we examined the overall efficacy of CBT for the primary outcome variable for Chinese people. Second, we performed a series of moderator analyses to investigate whether the effect of CBT for Chinese people was moderated by specific characteristics (outcome type, cultural adaptation, type of control group, study design, recruitment method, the format of delivery and region) of the included studies. These moderator analyses provide the basis to understand for which type of clients and under which conditions the treatment is efficacious (Driessen et al., 2010). Third, to understand the overall sustainability of the efficacy of CBT for Chinese people, the longer-term effects (follow-up of 3 months or longer) of CBT for Chinese people were examined. Fourth, we also examined the overall efficacy of CBT for two process variables, dysfunctional thoughts and coping, for Chinese people. This study was of theoretical significance because it represented an initial attempt to investigate the overall efficacy of CBT for Chinese people and examine whether cultural adaptation of CBT to Chinese culture can enhance treatment efficacy. Based on the past findings mentioned above, we hypothesized that the overall short-term and long-term effects of CBT on the primary outcome for Chinese people would be significant. We also hypothesized that the overall effect of CBT on two process variables, dysfunctional thoughts and coping, would be significant. Moreover, we expected that the efficacy of CBT for Chinese people would differ across different types of primary outcome variables. Furthermore, we predicted that culturally adapted CBT for Chinese people would be more effective than unadapted CBT. Additionally, the moderating roles of the type of control group, study design, recruitment method, the format of delivery and region in the efficacy of CBT for Chinese people were explored.
Method
Identification and selection of studies
To identify relevant studies, titles and abstracts were searched in electronic databases including Web of Science, PsycINFO and PubMed. We combined search terms indicative of CBT and Chinese clients. Specifically, the following search terms were used: (a) cognitive behavio* therap* OR CBT and (b) Chinese OR China. The search was performed from the inception of database to January 2017. Additional records were identified by manually searching the reference lists of the included studies and personal bibliographies.
Studies were included if they (a) were published in peer-reviewed journals in English, (b) evaluated the efficacy of CBT, (c) used a sample of Chinese clients, (d) included at least one CBT condition and one control condition, (e) were either randomized or non-randomized controlled trials, (d) included at least 10 participants in the CBT condition and the control condition and (e) reported sufficient data to calculate the effect size.
Extraction of data
The study characteristics that were coded included type of primary outcome variable (addictive behaviors, anxiety, caregiving stress, psychotic symptoms, depression/well-being, others), type of process variable (dysfunctional thoughts, coping, nil), cultural adaptation (culturally adapted, not culturally adapted), type of control group (wait list or no treatment, alternative treatment), study design (randomized design, non-randomized design), recruitment method (clinical, community), format of delivery (group, individual, self-help, mixed) and region (China, Hong Kong, others). Moreover, treatment effects were coded as short-term (posttest or follow-up at less than 3 months) or longer-term effects (follow-up at 3 months or longer). The coding was done independently by two coders. Any disagreements in coding were discussed until consensus was reached.
Meta-analyses
All meta-analyses were conducted using RevMan 5.3 (The Cochrane Collaboration, 2014). For each comparison between a CBT condition and a control condition, the effect size Hedges’ g indicating the difference between two conditions at posttest or follow-up was computed. This effect size is computed as the difference in posttest or follow-up scores between the CBT condition and the control condition, divided by the pooled standard deviation of the two conditions. Hedges’ g is a variation of Cohen’s d that corrects for small sample bias (Hedges and Olkin, 1985). According to Cohen (1988), effect sizes of 0.2, 0.5 and 0.8 represent small, medium and large effects, respectively. The effect sizes for process variables were also calculated.
In the calculation of effect sizes, instruments that explicitly measure the outcome of interest were used. If a study used more than one measure, the mean of the effect sizes was computed (Borenstein et al., 2009). If a study contained more than one CBT condition or more than one non-CBT control condition, the weighted mean and standard deviation by sample size across groups are used to compute a combined effect size as suggested by Borenstein et al. (2009). Therefore, each study provided only one effect size for each meta-analysis.
We conducted separate meta-analyses to examine the short-term and longer-term effects of CBT, so that a study measuring both short-term and longer-term effects provided one effect size for each analysis. If a study contained more than one follow-up test assessing the longer-term effect, the mean of the effect sizes was calculated so that there was only one longer-term effect size for each study (Borenstein et al., 2009).
Because considerable heterogeneity among the included studies was expected, pooled mean effect sizes were calculated using the random-effects model. To assess the heterogeneity of studies, the Q statistic was used (Borenstein et al., 2009). The Q statistic approximates a chi-square distribution. A significant Q value rejects the null hypothesis of homogeneity. An I2 statistic was computed as an indicator of heterogeneity in percentage. A higher I2 value represents greater heterogeneity, with a value of 0% indicating no observed heterogeneity, 25% indicating low heterogeneity, 50% indicating medium heterogeneity and 75% indicating high heterogeneity (Higgins et al., 2003).
Also, to investigate potential moderator effects, we conducted a series of subgroup analyses. The Q statistic was computed to examine differences in pooled effect sizes across different subgroups (Borenstein et al., 2009). The Q statistic follows a chi-square distribution. A significant Q value suggests that the effect sizes differ across subgroups.
Results
Selection of studies
The selection process used to gather the studies is shown in Figure 1. The literature search produced a total of 887 records, and 6 additional records were identified from other sources (748 after removal of duplicates). We removed 632 irrelevant records based on title and abstract. Full-text articles of the remaining 116 articles were retrieved. A total of 61 studies were excluded for reasons presented in Figure 1. Finally, 55 studies met the inclusion criteria for this meta-analysis.
Flow chart of the selection process.
Characteristics of included studies
The 55 included studies involved a total of 6763 participants (3571 in the CBT conditions and 3192 in the control conditions). The characteristics of the included studies are presented in Table 1. Regarding the type of primary outcome, 18 (32.7%) studies focused on depression/well-being, 7 (12.7%) on caregiving stress, 6 (10.9%) on anxiety, 5 (9.1%) on psychotic symptoms, 5 (9.1%) on addictive behaviors and 14 (25.5%) on other outcomes (e.g. aggression, child behavior problem, insomnia). In 24 (43.6%) studies, the CBT was reported to be culturally adapted, and in 31 (56.4%) studies, no cultural adaptation of CBT was reported. In all, 26 (47.3%) studies used wait list or no treatment control groups, and 29 (52.7%) studies used alternative treatment control groups. In all, 44 (80.0%) studies used a randomized design and 11 (20.0%) used a non-randomized design. In all, 25 (45.5%) studies used a clinical sample, 30 (54.5%) studies used a community sample. The CBT was delivered in a group format in 33 (60.0%) studies, in an individual format in 11 (20.0%) studies, in a self-help format in 4 (7.3%) studies and 7 (12.7%) studies used a mixed format. In all, 28 (50.9%) studies were conducted in Hong Kong, 20 (36.4%) in Mainland China and 7 (12.7%) in other countries (Taiwan, Australia and the United States). In 53 (96.4%) studies, the short-term effect of CBT was examined. Specifically, CBT conditions were compared with control conditions at posttest in 50 (90.9%) studies. Among the five (9.1%) remaining studies, three studies (5.5%) included a follow-up test at less than 3 months, one (1.8%) study only included follow-up tests at 3 and 6 months after treatment (Leung et al., 2016) and one (1.8%) study only included a follow-up test at 4.5 months after treatment (Wang et al., 2013). The longer-term effect of CBT was examined in 21 (38.2%) studies. These studies investigated the differences between CBT and control conditions at follow-up of 3 months or longer.
Characteristics of the studies included in the meta-analysis.
CBT: cognitive behavioral therapy; HK: Hong Kong.
The short-term effect of CBT on the primary outcome
We used 53 studies to examine the short-term effect of CBT on the primary outcome for Chinese people. Figure 2 presents a forest plot of the effect sizes of these short-term effects. It was revealed that the overall short-term effect of CBT on the primary outcome for Chinese people was in the hypothesized direction and medium in size (g = 0.61, 95% confidence interval [CI] = [0.46, 0.76], Z = 7.98, p < 0.001). The heterogeneity across the studies was high (Q = 402.53, p < 0.001, I2 = 87%).
Forest plot of the effect sizes indicating the short-term effects of CBT on the primary outcome for Chinese people.
Moderator analyses of the short-term effect of CBT
A series of subgroup analyses were conducted to assess whether the short-term effect of CBT on the primary outcome for Chinese people was moderated by factors including outcome type, cultural adaptation, type of control group, the format of delivery, region, study design and recruitment method. The results of moderator analyses are summarized in Table 2.
Moderator analyses of the short-term effect of CBT on the primary outcome for Chinese people.
p < 0.05; **p < 0.01; ***p < 0.001.
Consistent with our expectation, we found that the type of primary outcome significantly moderated the short-term effect of CBT (Q = 17.12, p = 0.004). The short-term effect of CBT was medium in size for anxiety (g = 0.78), depression/well-being (g = 0.53) and caregiving stress (g = 0.51) and was small in size for psychotic symptoms (g = 0.42) and addictive behaviors (g = 0.23). For other primary outcomes, the short-term effect of CBT was medium in size (g = 0.52). Post hoc comparisons with Bonferroni correction showed that the effect size for anxiety was significantly larger than that for addictive behaviors (Q = 14.19, p = 0.003), and the effect size for depression/well-being was significantly larger than that for addictive behaviors (Q = 9.54, p = 0.030).
As predicted, we found that cultural adaptation had a significant moderating effect on the short-term effect of CBT on the primary outcome (Q = 8.05, p = 0.005). The effect was stronger when the CBT treatment was culturally adapted (g = 0.60) than when the CBT treatment was not culturally adapted (g = 0.44).
The type of control group was found to significantly moderate the short-term effect of CBT on the primary outcome (Q = 4.55, p = 0.03). The effect was stronger when a wait list or no treatment control group was used (g = 0.57) than when an alternative treatment control group was used (g = 0.45).
The study design was shown to be a significant moderator of the short-term effect of CBT on the primary outcome (Q = 13.18, p < 0.001). The effect was greater when a randomized design was used (g = 0.54) than when a non-randomized design was used (g = 0.28).
The recruitment method showed a significant moderating effect on the short-term effect of CBT on the primary outcome (Q = 4.92, p = 0.005). The effect was stronger for clinical samples (g = 0.56) than for community samples (g = 0.45).
However, format of delivery (Q = 3.40, p = 0.33) and region (Q = 3.70, p = 0.16) did not significantly moderate the short-term effect of CBT on the primary outcome.
The longer-term effect of CBT on the primary outcome
There were 21 studies investigating the differences between CBT and control conditions at follow-up of 3 months or longer. These studies were used to assess the longer-term effects of CBT on the primary outcome. The effect sizes of these longer-term effects are summarized in Figure 3. We found that the overall longer-term effect of CBT on the primary outcome for Chinese people was in the hypothesized direction and medium in size (g = 0.63, 95% CI = [0.37, 0.89], Z = 4.80, p < 0.001). The heterogeneity across the studies was high (Q = 215.73, p < 0.001, I2 = 91%).
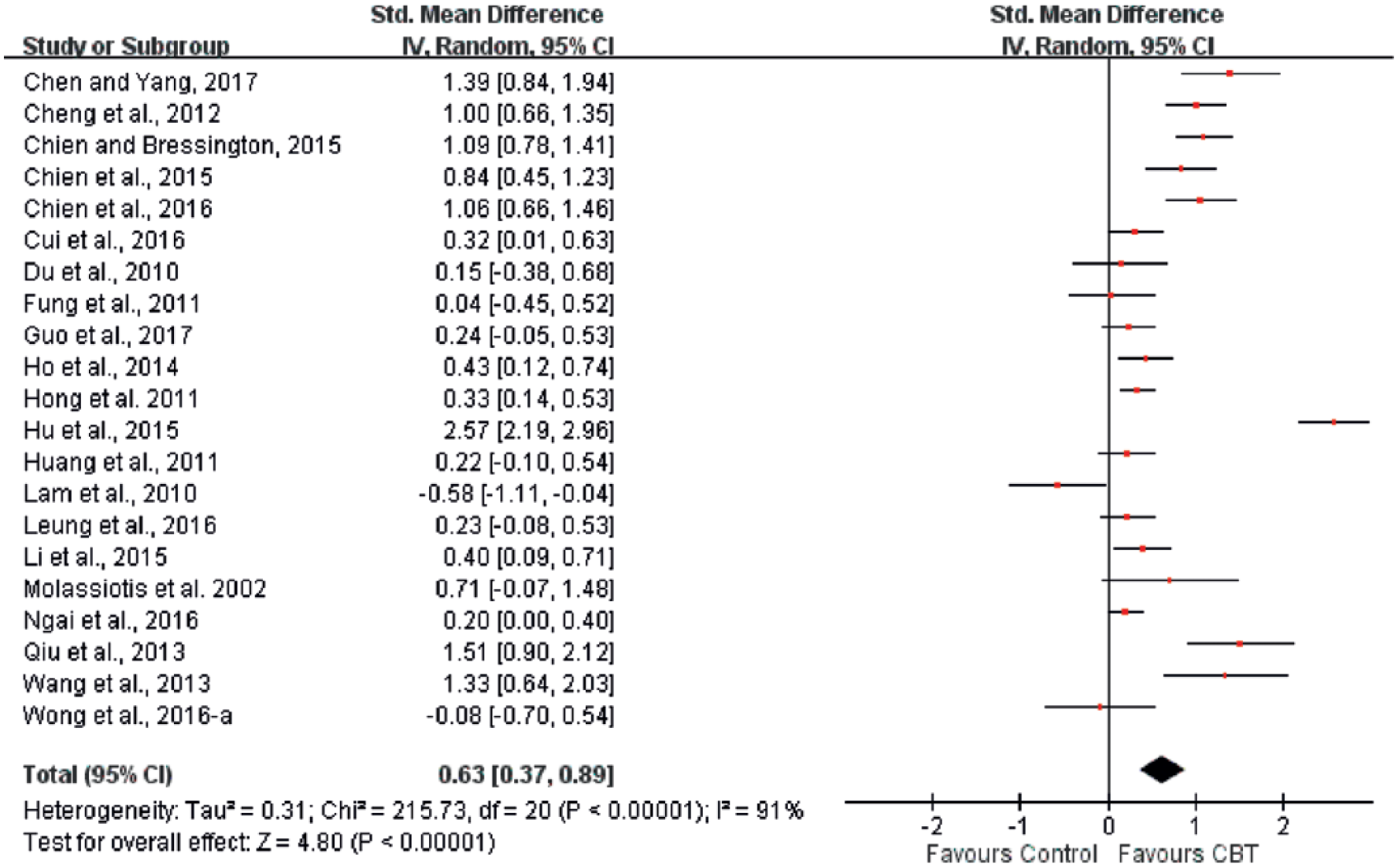
Forest plot of the effect sizes indicating the longer-term effects of CBT on the primary outcome for Chinese people.
The short-term effects of CBT on process variables
There were 16 studies examining the short-term effect of CBT versus control condition on at least a process variable. Among these studies, 12 studies included dysfunctional thoughts and 9 studies included coping. The effect sizes indicating the short-term effects of CBT on dysfunctional thoughts and coping are shown in Figures 4 and 5, respectively. We found that the overall short-term effect of CBT on dysfunctional thoughts was in the predicted direction and in the small range (g = 0.43, 95% CI = [0.19, 0.67], Z = 3.49, p < 0.001). Medium heterogeneity across the studies was detected (Q = 39.69, p < 0.001, I2 = 72%). Similarly, the overall short-term effect of CBT on coping was in the predicted direction and in the small range (g = 0.31, 95% CI = [0.02, 0.60], Z = 2.10, p = 0.04). High heterogeneity across the studies was observed (Q = 41.60, p < 0.001, I2 = 81%).
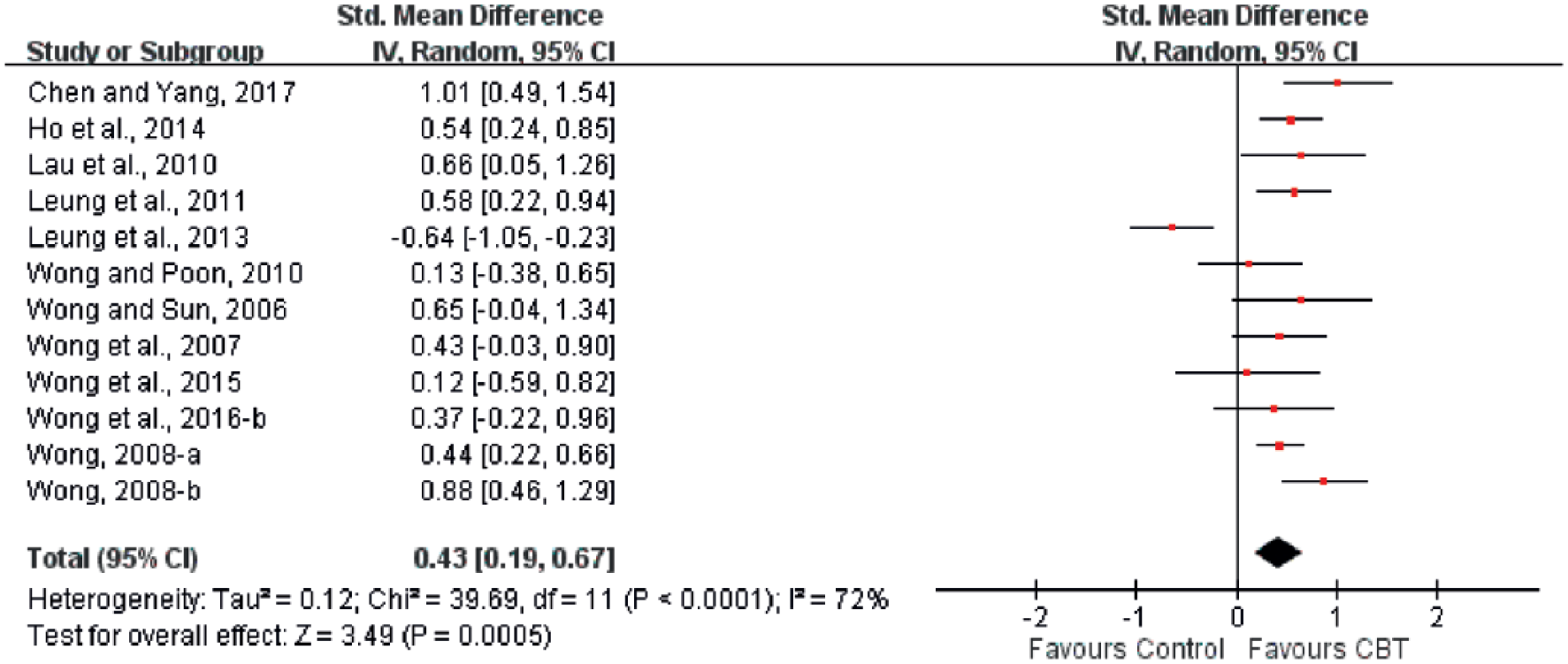
Forest plot of the effect sizes indicating the short-term effects of CBT on dysfunctional thoughts for Chinese people.
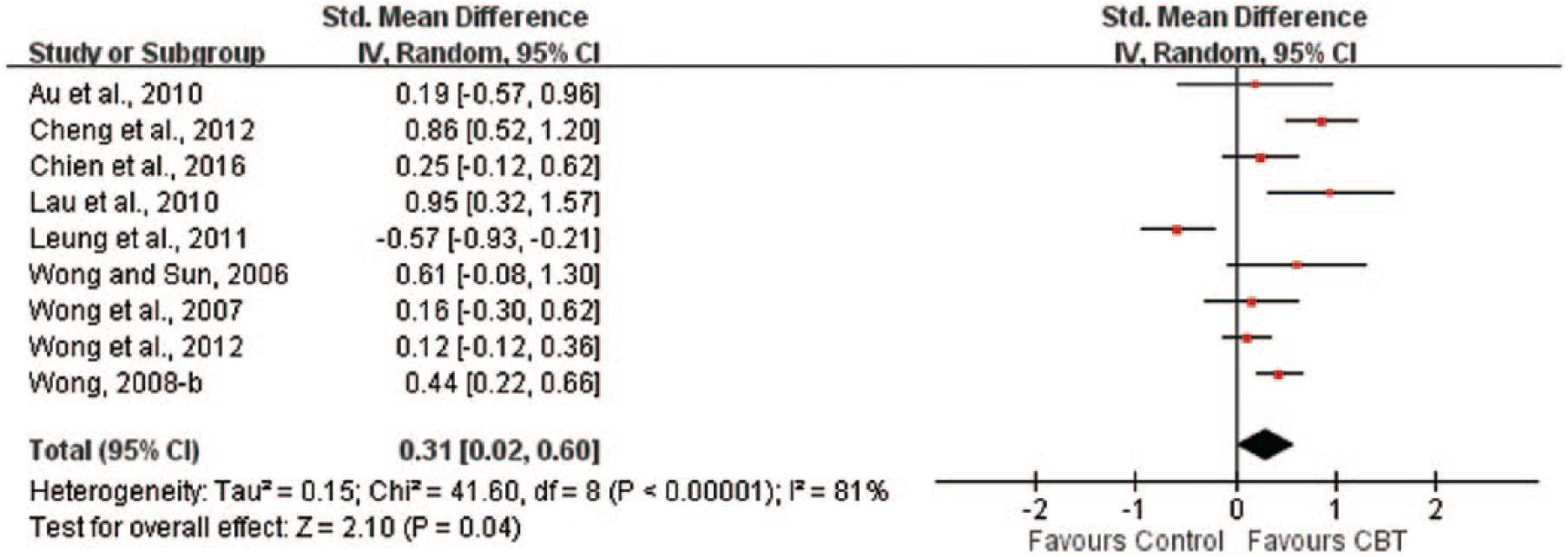
Forest plot of the effect sizes indicating the short-term effects of CBT on coping for Chinese people.
Since there were only three and two studies investigating the longer-term effects of CBT on dysfunctional thoughts and coping, respectively, we did not perform meta-analyses to examine these effects.
Discussion
This study attempted to advance the research on CBT by investigating the overall efficacy of CBT for Chinese people. To our best knowledge, this is the first meta-analytic study to review CBT studies using Chinese samples. Our results indicate that the overall short-term and longer-term effects of CBT for Chinese people were in the medium range. While it has been postulated that CBT is compatible with Chinese cultural values and beliefs (Chen and Davenport, 2005; Hodges and Oei, 2007; Leong, 1986; Lin, 2002), the current findings provide support that CBT is an effective psychotherapeutic approach for Chinese clients in general. The longer-term effect of CBT was similar to the short-term effect, suggesting that the efficacy of CBT is sustainable for Chinese clients.
The current results demonstrate differential effects of CBT on different primary outcomes for Chinese clients. CBT was most efficacious in treating anxiety and depression/well-being for Chinese clients, yielding effect sizes in the medium range. These findings are consistent with previous studies conducted in other populations, which have shown that CBT is an efficacious form of psychotherapy for anxiety and depression (Butler et al., 2006). However, past meta-analyses have revealed large effect sizes for CBT for anxiety (Gould et al., 1995, 1997a, 1997b; Grossman and Hughes, 1992; Reinecke et al., 1998) and depression (Gloaguen et al., 1998; Grossman and Hughes, 1992; Reinecke et al., 1998). There are multiple potential explanations for the weaker effects detected for Chinese people. First, while scholars have proposed that CBT will be an effective treatment for Chinese clients with appropriate cultural adaptations (Chen and Davenport, 2005; Hodges and Oei, 2007; Lin, 2002), only less than half of the studies included in this meta-analysis used culturally adapted CBT. Moreover, this study found that unadapted CBT had significantly weaker efficacy than culturally adapted CBT. Therefore, the inclusion of studies using unadapted CBT might have resulted in a smaller effect size. Second, compared with Westerners, Asian and Chinese people have lower anxiety and depression literacy (Kim and Zane, 2016; Wong et al., 2017). Such a lower level of mental health literacy might lead to a lowering of expectation that psychotherapy, including CBT, can be helpful, and this negative view toward psychotherapy might, in turn, affect the treatment effects, resulting in a weaker effect size (Jorm, 2012; Kim and Zane, 2016).
Moreover, the present results produced small effect sizes for CBT for psychotic symptoms and addictive behaviors for Chinese clients. These findings are in line with past meta-analyses that have also found small effects of CBT on psychotic symptoms (Jauhar et al., 2014) and addictive behaviors (Powers et al., 2008). Furthermore, while prior meta-analyses have shown a small effect of CBT on caregiving stress (Pinquart and Sorensen, 2006; Singer et al., 2007), this study found a medium effect size for CBT for caregiving stress for Chinese clients. One plausible explanation is that Asian caregivers tend to experience a higher level of distress than do Western caregivers (Pinquart and Sorensen, 2005). As a result, Asian caregivers might have more room for improvement from CBT. Future research is needed to verify this claim.
Consistent with our prediction, this study revealed that cultural adaptation of CBT to Chinese culture resulted in better therapeutic efficacy. The effect of culturally adapted CBT was in the medium range, while the effect of unadapted CBT was small. This finding concurs with the recent meta-analytic study by Benish et al. (2011), which supported that culturally adapted psychotherapy for ethnic and racial minorities in the United States showed greater short-term and longer-term efficacy than unadapted, conventional psychotherapy. Although researchers have advocated that CBT should be culturally adapted to meet Chinese clients’ needs (Chen and Davenport, 2005; Hodges and Oei, 2007; Lin, 2002), no prior work has compared the efficacy of culturally adapted CBT for Chinese people with that of unadapted CBT. This study provides initial evidence for the benefit of cultural adaptation of CBT to Chinese people.
We found that type of control group significantly moderated the effect of CBT for Chinese people. The effect of CBT relative to a wait list or no treatment control group was in the medium range, whereas the effect of CBT relative to an alternative treatment control group was small. This finding suggests the superiority of CBT over other treatments for Chinese clients. Moreover, it was revealed that the effect of CBT was stronger for clinical samples than for community samples. This finding is reasonable because compared with community samples, clinical samples generally have more severe problems at baseline and, therefore, tend to benefit more from treatments (Weisz et al., 2005).
We detected small effects of CBT on two process variables, dysfunctional thoughts and coping, for Chinese clients. However, a previous meta-analytic study found medium effect sizes for CBT for cognitive processes and coping (Chu and Harrison, 2007). A potential reason for the weaker effect of CBT on dysfunctional thoughts for Chinese clients is that Chinese culture is beset with strong traditional cultural beliefs, such as the hierarchy of relationships and relational harmony (Chen and Davenport, 2005). These beliefs, which are strongly held by some Chinese people, might take longer to be modified and changed. On the other hand, a possible explanation for the weaker effect of CBT on enhancing coping for Chinese clients is that Chinese people prefer to seek immediate and practical solutions from external sources to resolve their difficulties and, therefore, might be less inclined to devote their time to developing their inner coping and problem-solving capacities (Leong, 1986; Lin, 2002). Underlying these explanations is the need to design CBT programs that will allow sufficient time to modify dysfunctional beliefs and to enhance the development of inner coping capabilities. However, future research is needed to better understand the mechanisms through which CBT works for Chinese clients.
The findings of this study have several important implications. First, this study offers some evidence for the short-term and longer-term efficacy of CBT for a range of disorders and problems for Chinese clients. However, the application of different forms of psychotherapy including CBT is relatively recent in Chinese societies (Xu and Tracey, 2016), and there is a need to increase its application in Chinese societies so that a clearer picture of its efficacy can be ascertained. Second, this study shows that cultural adaptation of CBT to Chinese culture can improve treatment efficacy. However, culturally adapted CBT was used in less than half of the studies included in this study. Therapists in Chinese societies should make more effort to develop culturally attuned CBT, thereby maximizing its effects on Chinese clients. Third, the current findings echo the notion that it is relatively difficult for Chinese clients to change their dysfunctional beliefs (Chen and Davenport, 2005). According to Chen and Davenport (2005), it might be easier to help Chinese clients reframe their beliefs in a less absolute and more positive way than to help them refute those beliefs. Moreover, it might be necessary to allow more time for modifying culturally entrenched dysfunctional beliefs when designing CBT intervention for Chinese people.
Despite its contributions, this meta-analytic study is not without limitations. First, although the present findings show that CBT is effective in treating anxiety, depression/well-being, caregiving stress, psychotic symptoms, addictive behaviors and some other disorders for Chinese people, we could not identify any studies examining the effects of CBT on problems such as chronic pain, eating disorders, personality disorders and somatoform disorders. While previous meta-analyses have supported the efficacy of CBT for these problems for Western clients (Butler et al., 2006; Hofmann et al., 2012), future research is needed to investigate whether CBT is effective in treating these mental health issues among Chinese people. Second, we could not perform reliable moderator analyses of the longer-term effect of CBT because of the small number of studies in some subgroups. For example, there was only a single study focusing on anxiety, one study focusing on addictive behavior, two studies focusing on caregiving stress, one study using non-randomized design, two studies using a self-help CBT, two studies using a mixed format and one study conducted in a region other than Mainland China and Hong Kong (Taiwan). Future studies are required to better understand the longer-term effect of CBT for Chinese clients. Third, although our results found stronger efficacy for the culturally adapted CBT than for the unadapted CBT, we were unable to examine the moderating effects of different types of cultural adaptations because some studies did not provide detailed descriptions of the modifications made. Previous meta-analyses have examined the moderating effects of various types of cultural adaptations, including explicit incorporation of cultural values and beliefs into the intervention, matching of the race or ethnicity between clients and therapists, provision of services in clients’ native language and adaptation of illness myth on the effect of psychotherapy for ethnic minorities in Western countries (Benish et al., 2011; Chowdhary et al., 2014; Griner and Smith, 2006) and people in non-Western countries (Chowdhary et al., 2014). Further studies are needed to understand how different types of cultural adaptations influence the treatment effect of CBT for Chinese people. Fourth, our study only included studies published in peer-reviewed journals in English, which had undergone rigorous peer review processes by international experts. However, the efficacy of CBT for Chinese people reported in Chinese articles was not addressed. Future meta-analyses are recommended to include studies written in Chinese using Chinese databases such as Wanfang, Chongqing VIP (CQVIP), and China National Knowledge Infrastructure (CNKI).
Conclusion
In conclusion, this meta-analytic study advances the current literature by synthesizing studies on CBT for Chinese people. The overall short-term effect of CBT on the primary outcome was in the medium range. Medium effect sizes were found for anxiety, depression/well-being and caregiving stress, and small effect sizes were found for psychotic symptoms and addictive behaviors. The effects of CBT on process variables (dysfunctional thoughts and coping) were small. The overall longer-term effect of CBT on the primary outcome was in the medium range. Culturally adapted CBT has a stronger effect than unadapted CBT. The effect of CBT was moderated by the type of primary outcome, type of control group, recruitment method, study design, the format of delivery and region. The findings of this study suggest that CBT is an effective intervention for Chinese people, and cultural adaptation of CBT to Chinese culture leads to higher efficacy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.