
Abstract
Background:
Evidence maps are a method of systematically characterising the range of research activity in broad topic areas and are a tool for guiding research priorities.
Aims:
‘Evidence-mapping’ methodology was used to quantify the nature and distribution of recent peer-reviewed research into the mental health and wellbeing of Australian emergency services personnel.
Methods:
A search of the PsycINFO, EMBASE and Cochrane Library databases was performed for primary research articles that were published between January 2011 and July 2016.
Results:
In all, 43 studies of primary research were identified and mapped. The majority of the research focused on organisational and individual/social factors and how they relate to mental health problems/wellbeing. There were several areas of research where very few studies were detected through the mapping process, including suicide, personality, stigma and pre-employment factors that may contribute to mental health outcomes and the use of e-health. No studies were detected which examined the prevalence of self-harm and/or harm to others, bullying, alcohol/substance use, barriers to care or experience of families of emergency services personnel. In addition, there was no comprehensive national study that had investigated all sectors of emergency services personnel.
Conclusion:
This evidence map highlights the need for future research to address the current gaps in mental health and wellbeing research among Australian emergency services personnel. Improved understanding of the mental health and wellbeing of emergency services personnel, and the factors that contribute, should guide organisations’ wellbeing policies and procedures.
Introduction
There are currently over 80,000 paid Australian emergency services personnel comprising paramedics, firefighters, police officers and state emergency services workers (Black Dog Institute, 2015). These personnel work alongside approximately 420,000 emergency volunteers (Australian Bureau of Statistics, 2010). For these emergency services personnel, exposure to traumatic events and other stressors is an integral part of the role (McFarlane et al., 2009). Recent changes to Criterion A, the stressor criteria for post-traumatic stress disorder (PTSD) in The Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013), are of particular relevance for emergency services personnel. Criterion A was broadened to include repeated or extreme exposure to aversive details of traumatic events. This includes, for example, attending the aftermath of accidents or disasters and repeated viewing of objectionable material such as child pornography and terrorism-related images. In addition, the requirement for the individual to respond at the time of the trauma with intense fear, helplessness or horror has been dropped from Criterion A. These changes reflect an increase in our understanding of how trauma is experienced in the workplace and affects employees, particularly emergency service personnel (Levin et al., 2014). Not only do emergency services personnel experience a range of different types of trauma, they may also experience different trauma reactions compared to members of the general population who are exposed to single, unexpected trauma. Specifically, reactions such as anger and guilt are often reported, rather than the typical reactions of fear or horror (Black Dog Institute 2015).
It is important to note that in most instances, as with other trauma-exposed populations, the majority of emergency services personnel are expected to react to traumatic experiences with mild, transient distress that ultimately results in return to normal function (Benedek et al., 2007). However, the risk of developing PTSD increases with the number of exposures to traumatic events (Brewin et al., 2000). Emergency services personnel rarely develop PTSD following initial exposure to a single traumatic incident. More commonly, in those who develop PTSD, it follows repeated exposures over many years. This can be understood as a process of sensitisation and kindling, whereby repeated experiences of traumatic incidents result in progressively more severe reactions over time such that events that would not previously have affected the individual begin to trigger adverse psychological reactions (McFarlane, 2010). As the risk of PTSD increases with cumulative trauma, the rates of disorder may be expected to be higher among long-term emergency services employees than new recruits (Phoenix Australia, 2013). This was borne out in a recent study of the mental health of current and retired firefighters (Harvey et al., 2016).
Importantly, the mental health challenges that can face emergency services personnel go beyond PTSD. Depression rates after experiencing a traumatic event in Japanese and US emergency services personnel are thought to be between 16% and 26% (Kleim and Westphal, 2011). The Australian media in recent years has described Australian emergency services personnel in a state of crisis, with annualised suicide rates increasing by between 450% and 800% over the past few years, in contrast to more stable rates of suicide in other Australian samples (Koubaridis, 2015; May, 2016). Furthermore, the full range of mental health problems experienced by emergency services personnel is not necessarily trauma related. Factors such as working conditions and employment-related stressors have been linked to wellbeing (Hart and Cotton, 2003). For example, several studies have found that police officers consider general organisational experiences–for example, management practices, career opportunities, decision-making, clarity of role and performance feedback – to be more stressful than operational pressures such as danger, threats and attending the aftermath of incidents with fatalities (Hart et al. 1994). Similarly, low morale has been found to be a stronger determinant of withdrawal behaviours (e.g. stress-related absenteeism and intention to submit a stress-related workers’ compensation claim) in police than overt psychological distress (Cotton and Hart, 2003). Research has also shown that beyond the context of traumatic events, other mental health disorders are highly prevalent in emergency services personnel. For example, alcohol use disorders were present in 30–36% of US firefighters (Murphy et al., 1999) and 37% of Australian police officers (Davey et al., 2001). There is, however, an absence in the literature of reported prevalence rates of other mental health problems such as PTSD, depression and anxiety in Australian emergency services personnel.
Evidence maps are a relatively new method for identifying, organising and summarising scientific evidence on a broad topic (Bragge et al., 2011; Miake-Lye et al., 2016). Although systematic reviews are more methodologically sound and comprehensive, they are highly targeted and less well suited to heterogeneous groups (Callahan et al., 2012). Maps are designed to collate and summarise studies rather than provide synthesis or aggregate data, and quality appraisal is not always included (Callahan et al., 2012). The capacity for breadth in evidence mapping allows it to identify evidence gaps in order to guide future research efforts. Evidence maps are based on an explicit research question in relation to the field of enquiry, which may vary in depth, but should be informed by end users (Callahan et al., 2012). The end user may be researchers or research funding bodies who can identify gaps in the evidence, which in turn will create opportunities for new research. The research question drives the search for, and collection of, appropriate studies using explicit and reproducible methods at each stage (Arksey and O’Malley, 2005; Katz et al., 2003). Because the scope of this research question is so broad, it is well suited to an evidence map.
This paper presents the results of an evidence map that we conducted on recent mental health and wellbeing research in Australian emergency services personnel. It is the first synthesis of research into emergency services personnel health and wellbeing. To date, there has been no collation or summary of the current literature on Australian emergency services personnel, in relation to mental health and wellbeing. The extent, range and nature of peer-reviewed research is summarised in the current paper. This process of taking stock of the evidence is an essential first step in obtaining an overview of the breadth of research activities related to the mental health and wellbeing of Australian emergency services personnel.
Method
The Australian emergency services personnel mental health and wellbeing evidence mapping project was undertaken by the researchers as part of a larger project being conducted by beyondblue, a national organisation that provides information and support to help Australians affected by depression, anxiety and suicide. After consulting with experts in the area of emergency services personnel mental health and wellbeing, the questions and scope of the evidence map were defined. This process revealed two areas of focus for the map, namely
What current evidence exists regarding the mental health and wellbeing of Australian emergency services personnel?
What areas are, and are not, well researched?
Search strategy
To identify relevant literature, a broad search of relevant databases was conducted: the PsycINFO, EMBASE and the Cochrane Library databases were searched for relevant peer-reviewed literature. The search was not constrained by methodology, outcome, intervention or topic of investigation, in order to make the search broad and inclusive. In order to capture current literature and keep pace with the changing landscape of research in this area, the search period was constrained from January 2011 to July 2016. The search terms were determined after consultations with experts in the area of the mental health and wellbeing of Australian emergency services personnel. The following search terms were used: ‘police officer’ OR ‘police’ OR ‘policem*n’ OR ‘policewom*n’ OR ‘law enforcement’ OR ‘fire*fighter*’ OR ‘fire service personnel’ OR ‘firem*n’ OR ‘firewom*n’ OR ‘fire officer’ OR ‘first*responder*’ OR ‘response worker’ OR ‘emergency worker’ OR ‘emergency service* worker’ OR ‘emergency service* personnel’ OR ‘emergency response service personnel’ OR ‘emergency service*’ OR ‘paramedic*’ OR ‘emergency medical service*’ OR ‘ambulance worker’ OR ‘ambulance service worker’ OR ‘ambulance personnel’ OR ‘ambulance officer’ OR ‘ambulance’ OR ‘ambulance service*’ OR ‘disaster worker*’ OR ‘post-disaster worker’ OR ‘rescue worker’ OR ‘rescuer*’ OR ‘high*risk occupation’ OR ‘high*risk job*’ OR ‘state emergency service’ OR ‘SES’ OR ‘search and rescue’ AND Australia or Australian or NSW or ‘New South Wales’ or Victorian or Queensland or QLD or ‘Northern Territory’ or ‘South Australia’ or ‘Western Australia’.
Inclusion and exclusion criteria
Studies were eligible for inclusion if the population of interest was Australian emergency services personnel, the focus of the study was mental health or wellbeing, the study presented original research (i.e. the study was not solely an opinion piece, review or editorial), the study had been published since 2011 in a peer-reviewed journal and the study was published in English. Studies were excluded if the area of mental health related solely to the emergency services personnel’s interactions with the public (e.g. police restraints of mentally ill individuals; empathy levels in paramedics for their patients) rather than the emergency services personnel’s own mental health. Studies were also excluded if they solely investigated aspects of emergency services personnel as they relate to the operation of the organisation (e.g. factors that contribute to retention of volunteer firefighters; preparedness of paramedic personnel based on quality of clinical placement). A single study can often have multiple publications and as such, the primary reference for each study was established. This process prevented counting one study multiple times and misrepresenting the number of studies in a particular area. The authors took a conservative approach and unless the study clearly indicated it was a secondary study, it was considered unique in order to avoid under-representing the research field.
Screening and positioning the relevant evidence in the map (i.e. charting)
The titles and abstracts of all potentially relevant papers identified by the searches of the databases were collated. Where a title or abstract reported a trial that appeared to be eligible for inclusion, the full article was obtained. The full text was then assessed against the inclusion and exclusion criteria. Information extracted from the studies included sample size and participants, data sources/methodology, aims/objectives and key findings. Given that the purpose of the evidence map is to simply provide an overview of the extent, range and nature of the research activity, it is not necessary to appraise or describe research findings in detail (Hetrick et al., 2010). An evidence map is not meant to drill into the detail of individual articles to the same extent as systematic reviews.
Studies that met the inclusion criteria were then categorised according to the focus of the research described at the abstract level. Seven research foci were identified: (1) interventions related to mental health and/or wellbeing; (2) potentially traumatic event (PTE)/PTSD-related; (3) prevalence/incidence of mental health and/or wellbeing; (4) psychological factors relating to work-related injury; (5) sleep and fatigue; (6) organisational factors relating to mental health and/or wellbeing and (7) social/individual factors relating to mental health and/or wellbeing. Studies were also categorised by the location that the sample was obtained from, in terms of what Australian state(s) or territory, and by the service participants worked in (e.g. Police, State Emergency Service, Paramedic, etc.)
Results
The initial searches identified 2200 potentially relevant studies. After deleting 224 duplicates, 1976 studies were retained to be screened on the title and abstract. Based on the title and abstract screening, full texts were retrieved for 124 studies. Based on the information provided by the full text of the retrieved publications, 43 studies were deemed eligible for inclusion in the final map, and a further 6 studies were secondary publications (a flowchart of the search is presented in Figure 1). A map of recent research examining the mental health and wellbeing of Australian emergency services personnel was produced (see Table 1). In Table 2, an overview of the characteristics of these studies is provided. Please note that a study can have more than one outcome and therefore can be counted more than once in the table count. A list of citations for all studies included in the map is available on request.
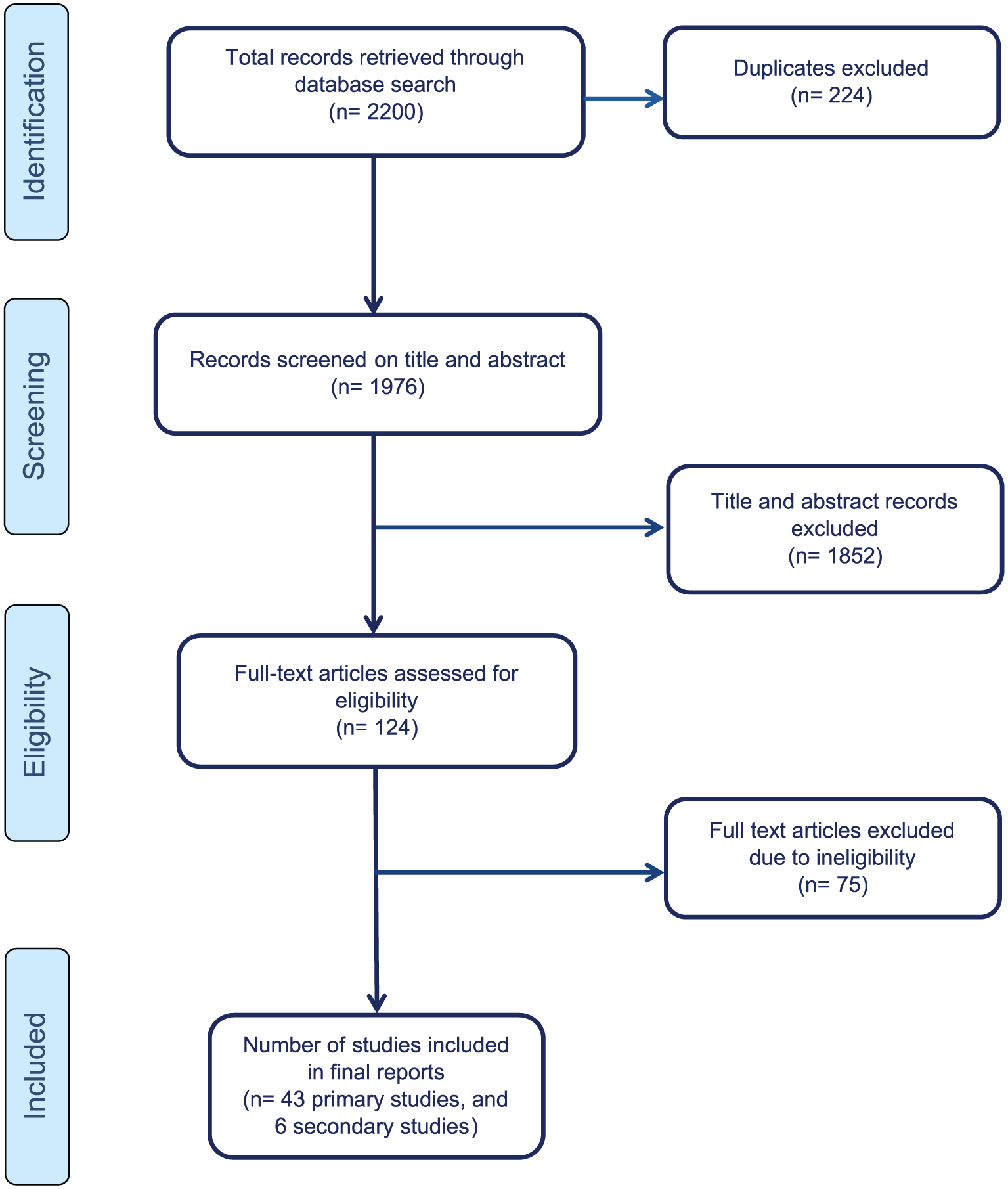
Flowchart of search for studies.
Evidence map of number of publications examining the mental health and wellbeing of Australian emergency services workers.
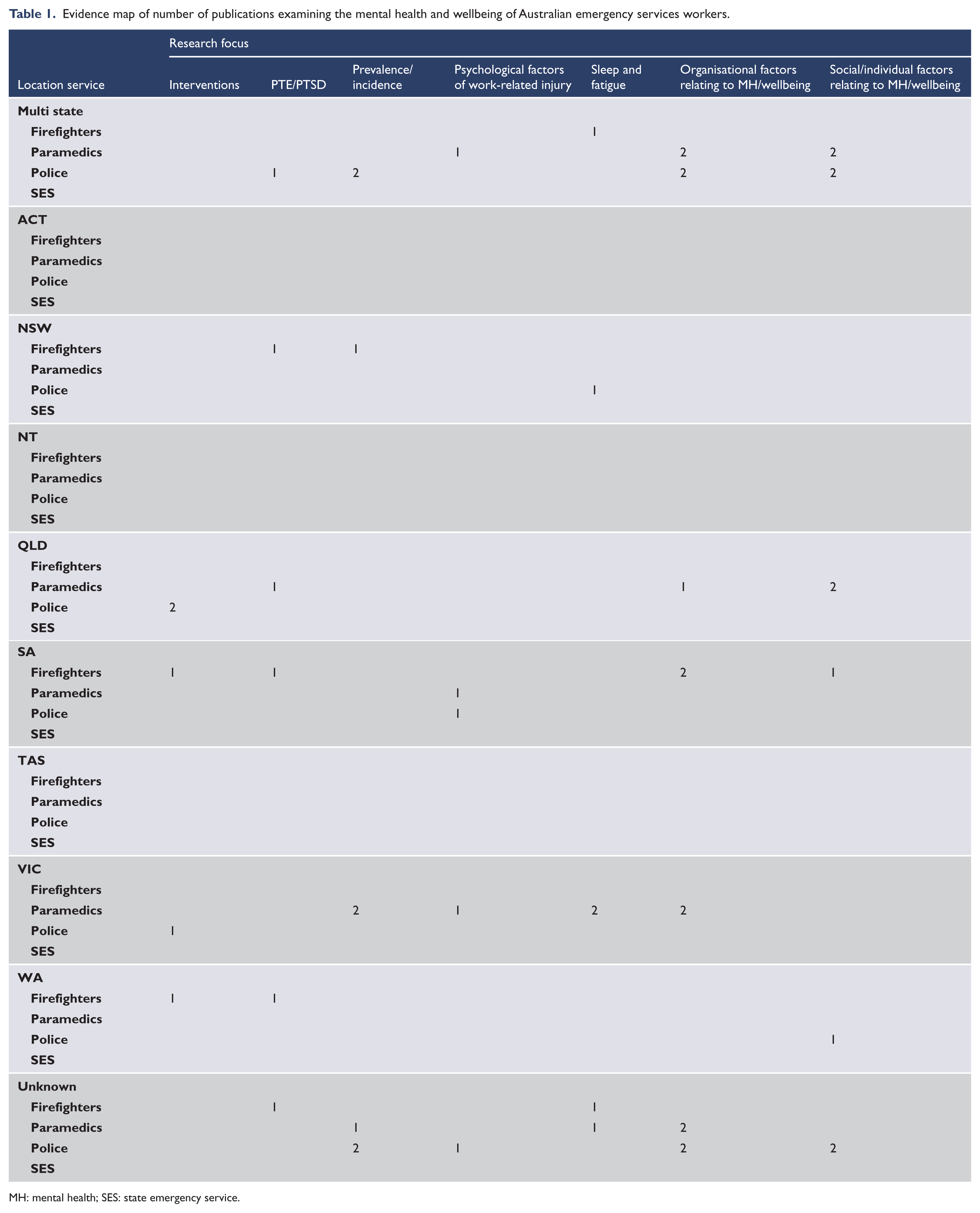
MH: mental health; SES: state emergency service.
Characteristics of studies included in the evidence map.

CISD: Critical Incident Stress Debriefing; EI: emotional intelligence; ICE: Internet child exploitation; NSW: New South Wales; PFA: psychological first aid; PTE: potentially traumatic event; PTSD: post-traumatic stress disorder; QLD: Queensland; RCT: randomised controlled trial; SA: South Australia; WA: Western Australia.
Service
The emergency services populations with the largest number of studies were paramedics (45% of the studies), followed by police (33% of the studies) and firefighters (21%). No studies were conducted with a multi-service population (i.e. more than one service in the one study). On the basis of the study title, a number of other studies appeared to have involved a multi-service population, but at the full-text assessment stage, it was found the majority included a single-service population. Of interest, there was a significant amount of research on sub-groups of emergency services personnel, such as volunteer firefighters, police investigators of child abuse and emergency medical dispatchers.
Location
Studies were conducted with emergency services personnel from Queensland (14%), South Australia (12%), Victoria (10%), Western Australia (7%) and New South Wales (5%). No studies were conducted with samples that were predominately from the ACT, NT or Tasmania, although personnel from these states may have been included in some of the multi-state studies (this was not specified). Around 35% of studies did not list the state(s) that their sample was recruited from. While 17% of the studies were multi-state, there were no studies that representatively sampled all Australian emergency services personnel populations at the national level. The few multi-state studies were narrow in their scope, with one study investigating injured paramedics who reported to Safe Work Australia (Maguire et al., 2014), three studies investigating paramedic students enrolled in degrees at Australian universities (McManamny et al., 2013; Williams et al., 2012, 2015), two studies investigating Internet child exploitation investigators (Powell et al., 2013, 2014) and a final study investigating crime scene investigators from around Australia (Kelty and Gordon, 2015). No studies were both multi-service and national in focus.
Research focus
As can be seen from the map (Table 1), the most commonly investigated area of research was organisational factors as they relate to mental health problems and/or wellbeing (13 studies: Adams et al., 2015; Armstrong et al., 2014; Dollard et al., 2012; Gayton and Lovell, 2012; Huynh et al., 2014; McManamny et al., 2013; Noblet et al., 2012; Powell et al., 2013; Powell and Tomyn, 2011; Shakespeare-Finch and Daley, 2016; Smith et al., 2011; Tuckey et al., 2012; Tuckey and Hayward, 2011). This includes factors such as operational aspects (e.g. shift work, potential occupational risks, job demands); aspects of the individual’s career (e.g. student compared to later career workers) and aspects related to emotional resources, or lack thereof, within the workplace (feelings of workplace belongingness; perceived workplace support and sense of camaraderie and bullying). The least researched areas were psychological factors relating to work injury (five studies: Broniecki et al., 2011; Larsen et al., 2016; Maguire et al., 2014; Roberts et al., 2015; Tuckey et al., 2012) and intervention studies targeting mental health or wellbeing (five studies: Burke and Shakespeare-Finch, 2011; LaMontagne et al., 2016; Lewis et al., 2014; Skeffington et al., 2016; Tuckey and Scott, 2014).
Overwhelmingly, the research investigated the impact of mental health on the individual emergency services personnel. Only one study included both current serving and retired personnel, while six studies involved student paramedic samples. Similarly, few studies involved non-operational personnel. Two studies involved emergency medical dispatchers, and one study involved fire and emergency services personnel and support personnel.
There were several areas of research where very few studies were detected through the mapping process. These include suicide, personality, stigma, pre-employment factors that may contribute to mental health outcomes and the use of e-health. No studies were detected which examined the prevalence of self-harm and/or harm to others, bullying, substance use and barriers to care.
Discussion
This investigation set out to answer two questions: how much research has been undertaken into the mental health and wellbeing of emergency services personnel and what areas are well-researched or conversely under-researched? The resulting evidence map is the first to summarise and describe the characteristics of primary research studies examining the mental health and wellbeing of Australian emergency services personnel, allowing us to identify priorities for future research.
The evidence map shows that a substantial amount of research into the mental health and wellbeing of Australian emergency services personnel has been undertaken in the past 5 years. Specifically, a number of studies have investigated the organisational factors that impact emergency services workers’ mental health and wellbeing, as well as individual and social factors that impact mental health and wellbeing. However, there are several gaps within this broad area of research. In particular, there was little investigation of suicide/self-harm or alcohol or substance use disorders. Both of these domains are critical to our understanding of mental health and wellbeing among emergency services personnel and warrant further research. With respect to suicidality in particular, the findings of higher rates of suicidal ideation than the Australian average among military personnel (McFarlane and Hodson, 2011), a population that shares repeated exposure to PTEs, highlight the need for further research into suicidality among emergency services personnel.
No studies focused on the experiences of families of emergency services personnel and the potential for ‘spillover’ or how emergency services personnel work both positively or negatively affects the lives of Australian families and loved ones. Again, drawing from military populations, there is evidence that a military career can dramatically impact the lives of family members and loved ones (Australian Centre for Posttraumatic Mental Health, 2012), and early research (Alexander and Walker, 1998; Cowlishaw et al., 2010; Murphy et al., 1999; Thompson et al., 2001) suggests that the same may be true in emergency services families.
Unfortunately, the sum of research to date does not permit a comprehensive understanding of the mental health and wellbeing of emergency services personnel. Systematic study with consistency in design and measurement across each sector of the emergency services and a broad focus on the full range of mental health and wellbeing outcomes would provide an important population-based estimate of the prevalence of mental health disorders across each of the Australian emergency services, as well as critical information on risk and protective factors. This information is required in order to develop evidence-based strategies to promote the wellbeing of emergency services personnel through prevention and early intervention at the individual and organisational levels and targeted strategies for high-risk sub-groups.
Limitations
Evidence mapping is a means of systematically identifying, organising and summarising the evidence pertaining to a broad topic. Defining the boundaries of this or any other evidence map is a somewhat subjective step. However, in this instance, we were guided by expert advice and by the end users, beyondblue. Evidence maps differ from other types of systematic reviews in that they provide a snapshot of the existing literature without quality assessment or extensive data synthesis. As such, no assessment of the quality of the studies, or bias in their methodologies was made for the current study, meaning that it is not possible to make judgments about the quality of research that has been conducted within this area. Given that the primary question of interest was what current evidence exists regarding the mental health and wellbeing of Australian emergency services personnel, the search period was constrained to the past 5 years.
Conclusion
The mental health of Australian emergency services personnel is in the spotlight with the increasing recognition of the potential impact of repeated workplace trauma and the stressors associated with these occupations. Although research has been conducted in Australian emergency services personnel in the past 5 years, it has been uncoordinated and piecemeal. Significantly less is known about the mental health and wellbeing of emergency services personnel compared to other trauma-exposed populations in Australia. In the first instance, systematic study with consistency in design and measurement across each sector of the emergency services that addresses prevalence of mental health disorders is needed. This research is critical to establish the nature and size of the problem as well as allow comparisons between service types. On the basis of this research, a host of other research questions follow, including attitudes towards help-seeking and barriers to care, the availability and uptake of mental health supports, the provision of evidence-based care and the effectiveness of return-to-work rehabilitation programmes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This evidence mapping project was funded by beyondblue as part of its Police and Emergency Services Program. The study sponsor had no role in the study design, data collection, analysis, interpretation or writing of this report.